


Compulsive buying behaviour (CBB), defined as a repetitive purchasing behaviour with a lack of control, is often associated with negative repercussions such as legal and financial problems, psychological difficulties and interpersonal conflicts.Reference Lejoyeux and Weinstein1 Specifically, CBB fosters higher credit card debt,Reference Joireman, Kees and Sprott2 reinforces low self-esteem,Reference Lejoyeux and Weinstein1 reduces happiness,Reference Moulding, Duong, Nedeljkovic and Kyrios3 leads to an increase in criminal problems and increases feelings of guilt.Reference Christenson, Faber, de Zwaan, Raymond, Specker and Ekern4 It is estimated in a meta-analysis that 4.9% of the population displays CBB, with university students standing out with a nearly 9% prevalence rate.Reference Maraz, Griffiths and Demetrovics5 In recent years, an expansion of CBB on online platforms has been observed owing to technological advancements, increasing accessibility and convenience, and reduced barriers to purchasing goods, all of which magnify the risk of CBB.Reference Müller, Joshi and Thomas6
Conceptualisations of CBB
Theoretical conceptualisations of CBB are mixed. CBB exhibits elements of impulsive–compulsive-spectrum disorders, as impulsively, compulsive buyers are inclined to the urge to purchase, while compulsively, CBB is a way of reducing anxiety.Reference Ridgway, Kukar-Kinney and Monroe7 However, it is still debated whether CBB should be categorised as an addictive, impulsive or obsessive–compulsive feature in psychopathology, although overall the literature tends to agree that CBB aligns more with impulsive characteristics.Reference Filomensky, Almeida, Castro Nogueira, Diniz, Lafer and Borcato8 This mixed opinion is reflected in the major diagnostic guidelines, as ICD-11 recognises compulsive buying–shopping disorder (CBSD) as an impulse control disorder, whereas DSM-5 does not acknowledge CBB as a diagnostic criterion. Since CBB can be explained by several psychopathological components, compulsive buyers often experience difficulties with their mental health.
Gender differences in CBB
Besides differences in classifications and conceptualisation, the literature also shows mixed results for gender differences in CBB. Women are more commonly reported to be at risk of CBB compared with men, although some studies found that this gender difference is non-significant.Reference Biolcati9 A deeper investigation into shopping motivation reveals that women tend to be influenced by gratification-seeking when online shopping, compared with information-seeking (‘idea shopping’) in men.Reference Wang, Fayaz, Zubair, Qilin and Ahsan10 Additionally, CBB might be a form of maladaptive coping strategy that is more prevalent among women.Reference Otero-López, Santiago and Castro11 It is suggested that women tend to purchase appearance-based objects to help with emotion regulation, social approval and expression of an idealised self,Reference Biolcati9 aligning with an emotion-based coping approach that is evidently prevalent in women.Reference Meléndez, Mayordomo, Sancho and Tomás12 The link between emotional coping strategies and CBB in women is further emphasised in a study reporting that mood compensation appeared to be a female-specific cognitive pathway that mediates CBB severity.Reference Ching, Tang, Wu and Yan13 Therefore, females with CBB tend also to experience higher rates of mood disorders, specifically major depression, and anxiety disorders. Despite the clear gender differences, limited research has examined the relationships between mental health and CBB in females separately.
The present study
CBB is consistently linked to symptoms and factors related to mental disorders, including depression and anxiety.Reference Koh, Tang, Gan and Kwon14 Furthermore, a meta-analysis found that studies using correlative examinations have shown a positive association between general perceived stress and the severity of CBB symptoms, with these correlations observed across both online and offline shopping contexts, different age groups and various countries,Reference Maraz, Griffiths and Demetrovics5 supporting the notion that CBB is among the behavioural manifestations of heightened depression, anxiety or stress.
Similarly to stress, the relationship between subjective well-being and compulsive buying is complex and inconsistently documented in the literature. A clear distinction between impulsive and compulsive buying is identified when examining its relationship with well-being,Reference Olsen, Khoi and Tuu16 suggesting the potential role of well-being in mediating the development of CBB as a maladaptive coping strategy during periods of worsening mental health.
Despite substantial research globally, studies in Vietnamese populations are limited. Furthermore, multiple mixed results have been identified in the literature, indicating the need to investigate CBB in specific subgroups of the population. However, to the best of our knowledge, no research has been published investigating the mediating effect of well-being on the relationship between mental disorders and CBB in a specific population of female urban office workers in Vietnam. Additionally, identifying specific subgroups to study the relationship between mental health and CBB can contribute to both cross-cultural understandings of the relationship and insights into potential psychological mechanisms of CBB when strictly controlling for demographic variables.
This study aims to explore the effects of different mental health domains, in particular depression, anxiety and stress, on CBB in office-working females. Specifically, we will evaluate (a) the direct relationships between these three mental health domains, as well as general mental well-being, and CBB, and (b) the mediating role of mental well-being on those direct relationships. Based on a literature review, the study proposes the following hypotheses: hypothesis 1, that mental disorders including stress, anxiety and depression, along with subjective well-being, will directly have, respectively, a positive and a negative influence on CBB; hypothesis 2, that mental well-being mediates the impact of mental disorders on CBB.
Method
Procedure and participants
This study employed a cross-sectional design, utilising Google Form as the platform for survey distribution. Convenience sampling was used to ensure a sufficient sample size in a timely manner. Thus, government, international and private organisations were contacted for data collection, where surveys were sent to participants individually via either emails or personal social media accounts.
The study aimed to gather data from approximately 300 female urban office workers, as a sample size of 200–300 is suggested for mediation analysis.Reference Fritz and MacKinnon17 The inclusion criteria were: (a) being in the age range of 20–50 years, (b) being female and (c) currently living and working in Ho Chi Minh City, Vietnam. Individuals who did not meet one of these criteria were excluded from the study. Other exclusion criteria included fixed-pattern and inconsistent responses.
This study received approval from the Vietnam Academy of Social Sciences (Decision No. 3763, signed 10 December 2021). The study ensured adherence to ethical standards outlined in the Declaration of Helsinki, revised in 2013,18 as well as compliance with the American Psychological Association’s Ethical Principles and Code of Conduct.19 Before inclusion in the study, all participants were required to provide written informed consent, affirming their voluntary participation and understanding of the study’s procedures and objectives.
Measures
Demographic information
We collected demographic information regarding age range, marital status and occupational setting.
The Compulsive-Buying Index (CBI)
The Compulsive-Buying Index (CBI), composed by Ridgway et al (2008), is consists of six items rated on a 7-point Likert scale, with a score of 1 being ‘strongly disagree’ and 7 being ‘strongly agree’.Reference Ridgway, Kukar-Kinney and Monroe7 All items of the scale are indicators of compulsive buying tendencies among consumers, for example ‘I buy things I don’t need’. A total score >25 (calculated by the sum of all item scores) is considered the cut-off point for compulsive buying. The Vietnamese version used in this study was translated in a study by Tran et al (2024).Reference Tran, Vo, Nguyen and Nguyen20
The Depression, Anxiety and Stress Scale (DASS-21)
The mental health components in this study were measured using the 21-item Depression, Anxiety and Stress Scale (DASS-21), developed by Lovibond & Lovibond (1995) and translated into Vietnamese by Tran et al (2013).Reference Tran, Tran and Fisher21 This measure contains three subscales evaluating levels of depression, anxiety and stress within the past week using seven items for each subscale. The DASS-21 uses a 4-point Likert scale, ranging from 0 (‘Did not apply to me’) to 3 (‘Applied to me very much or most of the time’). An example item on the scale is ‘I found it hard to wind down’. The total score for each subscale was calculated by multiplying the sum of its item scores by two, making the scores consistent with the original 42-item scale, with three 14-item subscales.Reference Lovibond and Lovibond22
World Health Organization-Five Well-being Index (WHO-5)
The World Health Organization-Five Well-Being Index (WHO-5) is a measure of subjective well-being over the past 2 weeks.Reference Do, Baker, Van Vo, Luong-Thanh, Nguyen and Valdebenito23 Its five items are rated on a 6-point Likert scale, ranging from 0 (‘At no time’) to 5 (‘All of the time’). Example items are ‘I have felt calm and relaxed’ and ‘I have felt active and vigorous’. The scale has shown good internal consistency when adapted to Vietnamese culture.Reference Do, Baker, Van Vo, Luong-Thanh, Nguyen and Valdebenito23
Data analysis
Data collected in this study were stored on an encrypted computer to which only the study’s authors are allowed access. Data aggregation, verification and cleaning were performed after completing data gathering. Data analysis was carried out using IBM SPSS 25.0 for Windows for descriptive statistics and SmartPLS 4 for Windows (SmartPLS, Monheim am Rhein, Germany; www.smartpls.com/) for evaluation of causal/predictive relationships in a complex model.
First, descriptive analysis was performed using SPSS, to provide an overview of demographic data and the distribution of the sample size. No missing data were recorded in our sample. Next, the reliability of the three scales was evaluated using Cronbach’s alpha and Spearman’s rho (SmartPLS 4’s rho_a and rho_c). Correlations between all variables were also examined. After that, based on a CBI cut-off score of 25,Reference Ridgway, Kukar-Kinney and Monroe7 participants were divided into either compulsive or non-compulsive buying groups to compare levels of depression, anxiety, stress and mental well-being, allowing deeper understanding of differences in mental health and mental well-being between the two groups. Finally, partial least squares structural equation modelling was performed using SmartPLS to examine the relationships among CBB, well-being and mental health variables, providing exploratory insights into the causal/predictive relationships between mental health and mental well-being and compulsive buying.
Results
Demographic characteristics and descriptive statistics
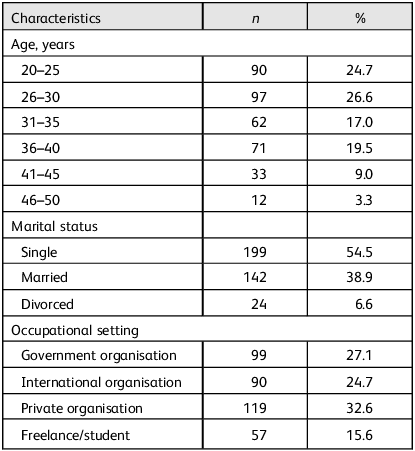
This study included 369 female urban office workers who resided and were currently working in Ho Chi Minh City, aged between 20 and 50 years. More than half of the participants (51.3%) were aged 20–30, 36.5% were between 30 and 40 years old, and only 12.3% were above 40 years old. Regarding marital status, the majority of participants were single (54.5%) and the rest were either married (38.9%) or divorced (6.6%). The distribution of occupational activities showed a relatively balanced spread among government organisations, international organisations, private organisations and freelance/student status. Further details on sociodemographic information are presented in Table 1.
Sociodemographic of participants (n = 369)

Table 2 gives descriptive statistics for the variables and evaluations of scale reliability. Generally, the sample exhibited normal levels of depression (mean M = 5.67; s.d. = 4.61), anxiety (M = 6.63; s.d. = 4.19) and stress (M = 8.90; s.d. = 4.30), below the common cut-off points for mental disorders among Vietnamese women suggested by Tran et al (2013).Reference Tran, Tran and Fisher21 All variables assessed in the study show acceptable to good internal consistency and are significantly correlated, except for compulsive buying and well-being. The correlations between depression, anxiety and stress are strongly positive (r > 0.7). Additionally, these three variables present weak positive relationships to compulsive buying and moderate negative connections to mental well-being. All variables show good internal consistency and composite reliability, with acceptable construct validity, expect for mental well-being, which shows good construct validity.
Means, standard deviations and correlations between variablesa

a. Spearman’s rho is shown as rho_a and rho_c, calculated using SmartPLS 4.
CBI, Compulsive-Buying Index.
** Correlation is significant at the 0.01 level (2-tailed).
Based on the CBI’s cut-off point of 25 to classify compulsive and non-compulsive buyers, Table 3 demonstrates the mean differences in dependent and mediating variables between the two groups. Specifically, statistically significant differences in anxiety (t(363) = 2.93, p = 0.004) and stress (t(363) = 3.27, p = 0.001) between compulsive and non-compulsive buyers were found, whereas the differences in depression and mental well-being were susceptible to chance.
Means, mean differences and standard deviations for depression, anxiety, stress and mental well-being based on compulsive buying groupsa

a. A CBI score ≥25 indicates compulsive buying.
CBI, Compulsive-Buying Index.
*** Correlation is significant at the 0.01 level (2-tailed).
Effects of mental health on compulsive buying
First, analysis utilising partial least squares structural equation modelling identified significant direct effects of stress and mental well-being on compulsive buying (Fig. 1). Specifically, standardised regression weights indicate a positive direct effect of stress (β = 0.427, p < 0.001) and well-being (β = 0.148, p = 0.010) on compulsive buying. This suggests that compulsive buying increases as either stress, or mental well-being or both rise. Furthermore, depression and anxiety exert no significant direct effects on compulsive buying. Additionally, a significant negative direct effect of depression on mental well-being is observed (β = 0.15, p = 0.010), whereas anxiety and stress have no direct effects on mental well-being.
Structural model of mental health and compulsive buying. Data appearing on the paths show standardised regression coefficients, with p-values in parentheses. Numbers appearing after the scale names indicate the scale items, with D denoting depression and A denoting anxiety. WHO-5, World Health Organization-Five Well-being Index; DASS, 21-item Depression, Anxiety and Stress Scale; CBI, Compulsive-Buying Index.

Second, depression is the only variable showing a significant indirect effect on compulsive buying, with mental well-being as a mediator (β = −0.077, t = 2.37, p = 0.018; Table 4). This means that depression indirectly leads to a decrease in compulsive buying behaviour due to a reduction in mental well-being.
Specific indirect effects of mental health on compulsive buying

CBI, Compulsive-Buying Index.
Last, in our study, 23.3% of variance in mental well-being is explained by stress, depression and anxiety (adjusted R 2 = 0.233), and 12.9% of variance in compulsive buying is predicted by stress, depression, anxiety and mental well-being (adjusted R 2 = 0.129).
Discussion
This study aimed to explore the influence of mental health on CBB among female urban officer workers, as well as the mediating role of subjective well-being on the relationships. Overall, participants who met the compulsive buying cut-off experienced significantly higher stress and anxiety levels, but differences in depression and subjective well-being were not statistically significant. This aligns with the literature on CBB and mental health,Reference Koh, Tang, Gan and Kwon14,Reference Thomas, Schmid, Kessling, Wolf, Brand and Steins-Loeber15 further suggesting that CBB is potentially a maladaptive coping strategy for heightened anxiety and stress among women.Reference Otero-López, Santiago and Castro11 More importantly, the findings support our hypotheses, as (a) stress and subjective well-being show significant direct effects on CBB and (b) depression influences CBB indirectly via subjective well-being.
How stress and well-being simultaneously affect CBB
A positive direct effect of stress on CBB is observed in our study, meaning that female urban office workers were more inclined to purchase compulsively when their stress levels rose. Our result aligns with the stress–CBB relationship reported across different populationsReference Koh, Tang, Gan and Kwon14 and various shopping contexts.Reference Albrecht, Hattula and Lehmann24 Although stress is not incorporated into theoretical models explaining CBB, two pathways have been proposed justifying the role of stress in reinforcing CBB: stress (a) as a vulnerability factor or (b) as a trigger.Reference Thomas, Schmid, Kessling, Wolf, Brand and Steins-Loeber15 As a vulnerability factor, stress activates CBB-related components such as materialistic value orientationReference Dittmar, Long and Bond25 or genetic predisposition,Reference Brand, Wegmann, Stark, Müller, Wölfling, Robbins and Potenza26 facilitating CBB. From the pathway of a trigger, stress has a more situational influence on CBB, as it fosters craving and affective responses, supporting the theoretical framework viewing CBB as an addiction.Reference Thomas, Schmid, Kessling, Wolf, Brand and Steins-Loeber15 Despite that, the overall evidence for this pathway is mixed and needs more investigation.
Besides stress, our study observed a positive direct effect of subjective well-being on CBB, meaning that CBB increased when subjective well-being was enhanced, which contradicts findings of a negative connection in other studies.Reference Villardefrancos and Otero-López27 One explanation might be that CBB is used as a coping mechanism and a protective factor against distress to maintain mental well-being,Reference Lins, Koch, Aquino, Costa and Melo28 and therefore a growth in subjective well-being might be an indicator of increasing CBB. Furthermore, the literature often explains the negative well-being–CBB connection by negatively linking well-being to materialism. However, similarly to how CBB is measured, conceptualisation of materialism is often mixed and negatively biased. Shrum et al (2013) proposed that engaging in purchasing behaviours might be a form of autonomy exploration,Reference Shrum, Wong, Arif, Chugani, Gunz and Lowrey29 indicating that individuals high in subjective well-being are more likely to engage in CBB as their identity pursuit is facilitated, which is highly prevalent among females.Reference Nepomuceno, de Aguiar Pastore and Stenstrom30 Given that well-being increases when identity is validated,Reference Burke, Cerven, Stets and Serpe31 individuals with higher well-being may engage in CBB as a means of status signalling or identity verification. This aligns with the contribution of identity-related components in reinforcing CBB in theoretical models.Reference Dittmar, Long and Bond25,Reference Kyrios, Frost and Steketee32 This suggests a highly complex relationship between well-being and CBB, with multiple perspectives due to a diverse proposed underpinning mental mechanism of CBB.
It is interesting that an increase in both stress and well-being contributed to compulsive buying. A hybrid model separately investigating mechanisms of impulsive and compulsive buying proposed that impulsive buying is more influenced by positive affect, whereas compulsive buying is encouraged by negative affect.Reference Darrat, Darrat and Amyx33 As stress and well-being are negative and positive affects respectively, and CBB is conceptualised as a combination of both impulsive–controlled and obsessive–compulsive behaviours in the current study, this model supports our findings, explaining the observed significant influence of both stress and well-being. Furthermore, our results highlight the importance of a unified conceptualisation of CBB in achieving a comprehensive understanding of the mental mechanisms underlying it and its connections to mental health.
Well-being as a mediator of mental health and CBB
Examining the mediating role of subjective well-being, depression is the only mental health variable in our study demonstrating an inverse indirect effect on CBB with statistical significance. This means that our study found that an increase in depression led to a reduction in well-being, simultaneously facilitating a slight decrease in CBB, whereas stress and anxiety had no indirect influence on CBB. This finding, despite challenging the literature, provides more nuance to the connection between mental health and CBB, highlighting the complexity of the mood–well-being–CBB relationship. First, when considering subjective well-being as a mediator, our finding challenges previous evidence directly linking depression positively to CBB,Reference Kyrios, Frost and Steketee32,Reference Müller, Claes, Georgiadou, Möllenkamp, Voth and Faber34 suggesting a more multifaceted relationship between CBB and mood. Differences in conceptualising CBB might influence these differences in results. It is agreed that CBB contains traits of addiction, poor impulse control and obsession–compulsion, although which factor influences CBB more is still debated.Reference Thomas, Schmid, Kessling, Wolf, Brand and Steins-Loeber15 Particularly, our study measures CBB using the Compulsive-Buying Index by Ridgway et al (2008),Reference Ridgway, Kukar-Kinney and Monroe7 defining CBB as a combination of poor impulse control and obsession–compulsion, whereas others mainly utilised the Compulsive Buying Scale developed by Faber & O’Guinn (1992), which views CBB as solely a poor impulse-control behaviour. Thus, such a fundamental difference potentially influences the disparity in observations. Further investigating different CBB conceptualisations, Lawrence et al (2014) found that, compared with depressive symptoms, CBB is more closely related to reward sensitivity.Reference Lawrence, Ciorciari and Kyrios35 This partially explains the observed mediating effect of well-being on the depression–CBB relationship in our study, since reward sensitivity is often positively linked to subjective well-being and inversely connected to negative affects, including depression. Furthermore, the indirect effect of depression on CBB can infer the role of CBB as a coping mechanism among individuals with lower depression levels. Extreme changes from negative to positive moods between pre-shopping and shopping have been documented among compulsive buyers,Reference Faber and Christenson36 indicating that when reaching a certain threshold of negative affect, a pattern of reverting to shopping to improve their mood, manage their depression and maintain a sense of well-being, is prevalent among people with high CBB. Thus, this reinforcement loop justifies our observation, suggesting a multivariate composition of the depression–well-being–CBB relationship.
Implications
This study offers several critical insights into the intricate interplay between mental health and CBB among female urban office workers. The identification of stress and subjective well-being as direct predictors of CBB emphasises the role of both negative and positive affective states in driving compulsive consumption. These findings challenge the conventional understanding of CBB as purely a maladaptive response to negative emotional statesReference Ridgway, Kukar-Kinney and Monroe7–Reference Koh, Tang, Gan and Kwon14 and suggest that heightened subjective well-being may also foster CBB, possibly through mechanisms of identity expressionReference Shrum, Wong, Arif, Chugani, Gunz and Lowrey29–Reference Kyrios, Frost and Steketee32 and emotion regulation.Reference Biolcati9,Reference Meléndez, Mayordomo, Sancho and Tomás12 Therefore, future research should focus on exploring CBB from a neutral perspective to fully understand the complex relationship between CBB and different mental health aspects.
Additionally, the current study reinforces the importance of moving towards integrated models of CBB that incorporate both affective and identity-based motivations. The observation that depression influences CBB indirectly via subjective well-being, while anxiety exerts no direct or indirect influence, further supports a multifactorial and dynamic model of CBB rather than a linear psychopathological account. This distinction is critical for refining existing frameworks, particularly those rooted in addiction theory,Reference Thomas, Schmid, Kessling, Wolf, Brand and Steins-Loeber15 impulse-control disordersReference Hudders and Pandelaere37 and compulsive pathology.Reference Ridgway, Kukar-Kinney and Monroe7
Last, these findings inform the interventions for CBB, highlighting a person-specific approach, as the influence of both stress and well-being on CBB reflects the difference in mental mechanisms among individuals. Traditional frameworks emphasising negative mood and distorted beliefs may be insufficient in certain cases. Interventions should also recognise that enhanced well-being does not necessarily equate to resilience and may, paradoxically, coincide with increased risk for CBB in contexts where material consumption becomes a tool for self-verification or identity construction.Reference Nepomuceno, de Aguiar Pastore and Stenstrom30,Reference Hudders and Pandelaere37 Particularly, the findings of this study advocate psychologists and other healthcare professionals to approach CBB as a behavioural manifestation of various possible psychological mechanisms. Thus, interventions for individuals with CBB should explore and consider these underlying within-person mechanisms to enhance intervention effectiveness and appropriateness.
Limitations
Despite its valuable insights, this study has several limitations. Its cross-sectional design prevents causal inference. The use of convenience sampling limits generalisability to the entire female population,Reference Andrade38 especially as our study exclusively targeted those who are urban office workers. The reliance on self-report measures introduces potential biases, such as interpretation bias.Reference Hill, Mogle, Whitaker, Gilmore-Bykovskyi, Bhargava and Bhang39 Additionally, it should be noted that our study assessed anxiety as a state variable, and there is evidence that state and trait anxiety influence CBB differently.Reference Weinstein, Mezig, Mizrachi and Lejoyeux40 This further limits the nuanced understanding of how anxiety contributes to compulsive buying tendencies and whether CBB is only manifested during elevated short-term anxiety in Vietnamese female urban office workers. Thus, future studies incorporating multi-method approaches, such as combining with behaviour tracking or qualitative interviews, could provide a richer and more accurate understanding of the directional relationship between CBB and mental health, as well as how CBB emerges in female populations. Last, since this study defined CBB as a behaviour on the impulsive–compulsive spectrum,Reference Ridgway, Kukar-Kinney and Monroe7 the findings might be interpreted through a relatively narrow conceptual lens.
Data availability
The data-set generated during and/or analysed during the current study will be available from the corresponding author, H.K.N., on reasonable request after the authors have fully exploited it.
Author contributions
Conceptualisation: H.A.N.V., V.H.A.N., H.M.P.; data collection: H.A.N.V., G.T.N.N.; formal analysis: H.A.N.V., H.K.N., V.H.A.N.; methodology: H.A.N.V., H.M.P.; writing – original draft: H.K.N, H.A.N.V.; writing – review and editing: G.T.N.N., H.M.P. All authors reviewed and agreed on the final version of the article.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.





 Open access
Open access
eLetters
No eLetters have been published for this article.