


Case presentation
A 14-year-old girl who had undergone pulmonary artery banding in the neonatal period and a corrective surgical repair of a ventricular septal defect at 2 years of age presented with a complaint of a heartbeat sensation in the neck. The patient’s physical examination showed a thrill at the jugular notch and aortic pulsation. The femoral pulses were robust and pulsatile. Cervical aortic arch was suspected, and CT revealed a Zhong’s B2 type and Haughton’s B type cervical arch, associated with a Kommerell diverticulum (Figure 1, Video 1). Conventional angiography revealed no gradient suggestive of either true or pseudo-coarctation (Figure 2, Video 2). Since our patient’s imaging revealed no respiratory compression or coarctation/stenosis gradient, we decided on clinical follow-up. This will involve monitoring symptoms and blood pressure, performing an annual echocardiogram to check the gradient, and conducting a repeat CT scan in 5 years.
( a ) Posterior–anterior chest X-ray of the patient shows a high-positioned and elongated aortic arch. (b ) 3D reconstruction of CT shows the aortic arch above the sternum, the origin of the right common carotid artery (RCCA), and the course of the left common carotid artery (LCCA). ( c ) 3D CT reconstruction shows isolated cardiac structures and large vessels, the aberrant right subclavian artery (aRScA), the course of the left subclavian artery (LScA), and the Kommerell diverticulum (KmD) in anterior (C1), left-anterior (C2), and left-posterior (C3) positions.

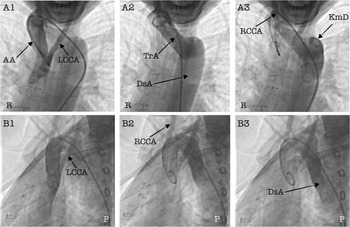
Conventional angiography images: ( a ) series showing temporal contrast filling in the anteroposterior position; ( b ) series showing temporal contrast filling in the lateral position. It was observed that the left common carotid artery (LCCA) arises proximal to the ascending aorta (AA), the right common carotid artery (RCCA) arises distal to the AA, near the junction of the transverse arch (TrA), and the transverse arch turns posterior to the trachea. The descending aorta (DsA) runs dilated after the Kommerell diverticulum (KmD).

Cervical aortic arch is an exceedingly rare congenital anomaly characterised by an abnormally high aortic arch, frequently positioned above the clavicle. The cervical aortic arch is thought to have developed from the persistence of the third embryonic aortic arch and the regression of the normal fourth aortic arch, limiting the typical caudal migration of the aorta into the thorax. It exhibits significant anatomical heterogeneity in laterality and branching patterns. Many paediatric patients are diagnosed incidentally, while others present with a pulsatile supraclavicular or neck mass, upper-airway or oesophageal compressive symptoms (vascular ring physiology), differential upper-limb blood pressures, or complications associated with related lesions (kinking/pseudocoarctation). Vascular anomalies, such as the cervical aortic arch or incomplete vascular rings, can remain undetected during routine intracardiac procedures, including ventricular septal defect repair or pulmonary artery banding, because these conditions extend superiorly into the extrapericardial space, beyond the reach of standard surgical exposure. Cross-sectional imaging is essential for defining the arch framework, head-and-neck vascular branching, and related aneurysmal alterations. Surgical management is individualised and generally reserved for symptomatic vascular ring physiology, significant obstruction, or the presence or risk of aneurysm or pseudoaneurysm. Paediatric outcomes are generally favourable when the anatomy is thoroughly delineated preoperatively. Reference Baudo, Varrica and Reali1
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951126111792
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare no conflict of interest to disclose.
Ethical standards
Written informed consent was obtained from a legally authorised representative for anonymised patient information to be published in this article.




 Open access
Open access