


Introduction
CHD impacts approximately 1% of the population. Reference Park1 Several congenital heart lesions require surgical intervention at age 3–6 months, including single ventricle patients undergoing bidirectional Glenn (BDG), ventricular septal defect closure, and repair of tetralogy of Fallot. Anecdotally, bedside staff and providers have noted that patients who have undergone a bidirectional Glenn palliation have increased discomfort and require additional sedation and analgesia medications post-operatively than those patients who undergo cardiac surgery at a similar age. This is often attributed to a “Glenn headache”; however, this anecdotal experience of increased sedation and analgesia needs postoperatively has, to our knowledge, never been officially assessed.
The bidirectional Glenn is part of the palliation sequence for children with anatomic or functional single ventricle physiology. Reference Park1,Reference Ungerleider, Meliones and McMillan2 The bidirectional Glenn, also called a cavopulmonary shunt, involves anastomosis of the superior vena cava directly to the pulmonary artery and each superior vena cava is anastomosed to their respective pulmonary artery for patients with bilateral superior vena cavas (bilateral bidirectional Glenn). Reference Park1–Reference Shuler, Statile and Heydarian3 These surgical interventions result in passive pulmonary blood flow, improved oxygenation, and volume unloading of the systemic ventricle. Reference Ungerleider, Meliones and McMillan2,Reference Cabrera, Kibler and Easley4–Reference Tseng, Anixt and Meinzen-Derr5 Following bidirectional Glenn palliation, there is a rise in the superior vena cava pressure (Glenn pressure) and thus cerebral venous pressure, when compared to pre-surgical shunted physiology. Reference Cabrera, Kibler and Easley4,Reference Neunhoeffer, Michel and Nehls6–Reference Cabrera, Kibler and Easley9 There is a decrease in cerebral blood flow velocity through cerebral arteries; however, there are no signs of blood pooling in the capillaries related to this elevated superior vena cava pressure noted during the first 36 hours post-operatively. Reference Neunhoeffer, Michel and Nehls6 Cerebral autoregulation helps maintain steady cerebral blood flow to promote flow through the Glenn and is dependent on oxygen and carbon dioxide levels. Reference Neunhoeffer, Michel and Nehls6,Reference Bertolizio, DiNardo and Laussen8,Reference Hoskote, Li and Hickey10 Bidirectional Glenn patients can be managed with permissive hypercapnia to increase cerebral vasodilatation and cerebral blood flow, which then increases pulmonary blood flow to optimise cardiac output. Reference Hoskote, Li and Hickey10–Reference Li, Hoskote and Hickey11 Increased superior vena cava pressure, with subsequent increased intracranial pressure, is thought to contribute to a presumed “Glenn headache.” Reference Tseng, Anixt and Meinzen-Derr5,Reference Tripathi, Hafzalah and Harthan12–14
There is currently no known literature that compares the sedation and analgesia needs of children who undergo bidirectional Glenn palliation to similar-aged children who undergo other cardiac repairs, such as ventricular septal defect closure (normal central venous pressure) and repair of tetralogy of Fallot (elevated central venous pressure). Reference Cabrera, Kibler and Easley4,Reference Neunhoeffer, Michel and Nehls6 The objective of this study was to determine whether sedation and analgesia requirements were higher in post-operative bidirectional Glenn patients than those of similar age who underwent tetralogy of Fallot or ventricular septal defect repairs.
Patients and methods
This study complied with the Strengthening the Reporting of Observational Studies in Epidemiology Statement: guidelines for reporting observational studies. Reference von Elm, Altman and Egger15 This was a single-centre retrospective cohort study at a major academic medical centre. A retrospective chart review from January 2018 to February 2021 was performed. Inclusion criteria included all patients who underwent one of the following procedures within the first year of life: bidirectional cavopulmonary anastomosis (bidirectional Glenn), bilateral bidirectional cavopulmonary anastomosis (bilateral bidirectional Glenn), tetralogy of Fallot repair, or ventricular septal defects. Post-operative bidirectional Glenn patients were compared to both tetralogy of Fallot and ventricular septal defect repairs to compare bidirectional Glenn patients to those with low central venous pressure (CVP) (ventricular septal defect repairs) and elevated CVP (tetralogy of Fallot repairs). These were selected due to similar age at repair. Central venous pressure (CVP) and Glenn pressures are typically measured via an internal jugular central venous catheter. Patients were identified through the Society of Thoracic Surgeons database. Exclusion criteria included pre- or post-operative extracorporeal membrane oxygenation, cardiac arrest within 48 hours of cardiac repair, single ventricle patients who remained inpatient during the interstage period or were discharged home during the interstage period on methadone, lorazepam or clonidine and patients who required mechanical ventilation pre-operatively. Institutional Review Board approval was obtained prior to study commencement, with a waiver of consent granted and was conducted in accordance with the Declaration of Helsinki.
All post-operative cardiac patients at our institution utilise a standard post-operative pain and sedation protocol. Reference Donnellan, Sawyer and Peach16 This protocol consists of a standard, weight-based, starting dose of morphine infusion for intubated and extubated patients that is initiated upon arrival back from the operating room (OR). Unless there is bradycardia in the OR, patients will return from the OR with a low-dose dexmedetomidine infusion. A 50 or 100 mcg/kg morphine bolus is prescribed as needed (PRN) every 15 minutes for the first hour and then the frequency decreases to hourly PRN after initial pain control is achieved. Additionally, the morphine infusion can be increased if three PRN morphine doses are needed within the first 2 hours. All patients receive three doses of IV acetaminophen followed by scheduled enteral acetaminophen for a total of 3 days. Non-steroidal anti-inflammatory drugs, ketorolac or ibuprofen, are considered for patients greater than 4 months of age without signs of bleeding or concerns for kidney injury. Additional intermittent sedatives and analgesics can be utilised at provider discretion. These options included chloral hydrate, lorazepam, midazolam, oxycodone, and quetiapine. Chloral hydrate was removed from our institution’s formulary at the conclusion of 2020. All patients included in our study followed this protocol. Additionally, caudal blocks are occasionally utilised. The decision for this modality is based solely on surgeon and anaesthesiologist preference.
Patient and medication data were collected from the electronic medical record. Non-medication data were collected by three cardiac ICU Advanced Practice Providers and 1 cardiac ICU hospitalist, with selected records checked for accuracy by the project leader (AF). Demographic and baseline surgical data, including repair, weight, sex, race, and age at time of surgery, were collected. Additionally, cardiopulmonary bypass time, mechanical ventilation at time of admission to the cardiac ICU (yes/no), total hours of mechanical ventilation, max pain score, utilising the Face, Legs, Activity, Cry, Consolability scale, ICU length of stay, and hospital length of stay were collected. Central venous pressure (CVP), Glenn pressure, and mean arterial pressure at admission, 12, 24, 36, and 48 hours post-operatively were also recorded.
Medication exposure was obtained from the electronic medical record medication orders and nurse charting by a cardiac ICU pharmacist, with selected records checked for accuracy by project leader (AF). These were tracked through the entirety of cardiac ICU admission, or the first six days if admitted longer. Cumulative, weight-based doses of morphine, midazolam, and dexmedetomidine infusions were calculated using infusion rates for the duration. As-needed doses of opioids were tabulated and expressed in total weight-based exposure. Frequently used intermittent analgesic and sedative exposure (including non-steroidal anti-inflammatory drugs, chloral hydrate, clonidine, gabapentin, and quetiapine) were also reviewed and recorded.
Categorical variables were reported as absolute number (n) and relative frequency (%). Continuous variables were reported as median and interquartile range. Comparisons between bidirectional Glenn, tetralogy of Fallot, and ventricular septal defect groups were performed using the chi-squared test and Fisher’s exact test, according to expected counts, as well as the Kruskal–Wallis test, followed by the Dunn test for multiple comparisons, when necessary, to identify significantly different pairs of groups. For all statistical analyses, p < 0.05 was considered statistically significant.
Results
A total of 96 patients met all inclusion criteria. Just over 34% (n = 33) of patients underwent bidirectional Glenn, and 6.3% (n = 6) underwent bilateral bidirectional Glenn. A total of 37.5% (n = 36) of eligible patients underwent tetralogy of Fallot repair, and 21.9% (n = 21) underwent ventricular septal defect closure. In total, 63.5% (n = 61) of patients were male and 36.5% (n = 35) were female. Median (interquartile range) age at surgery was 128 days for BDG, 133 days for bilateral BDG, 181 days for tetralogy of Fallot repair, and 172 days for ventricular septal defect repair, with overall median age of 133 days (119.0–186.0 days). Median (interquartile range) weight was 6 kilograms (5.4–6.5 kilograms). Patients were 84.4% (n = 81) Caucasian, 7.3% (n = 7) Black, 5.2% (n = 5) Asian, and 3.1% (n = 3) Hispanic/Latino (Supplemental Table 3).
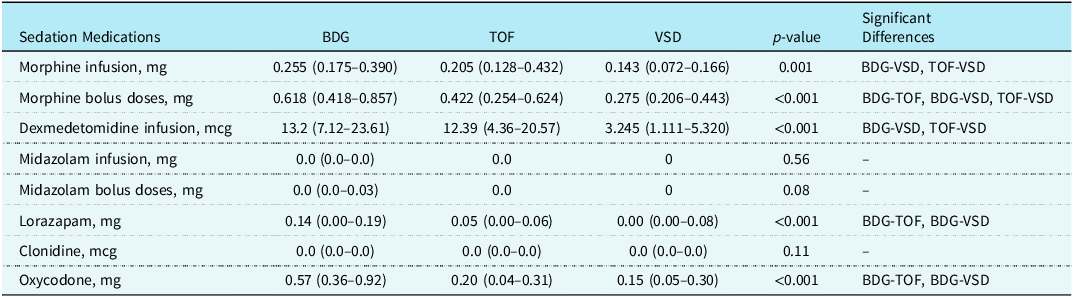
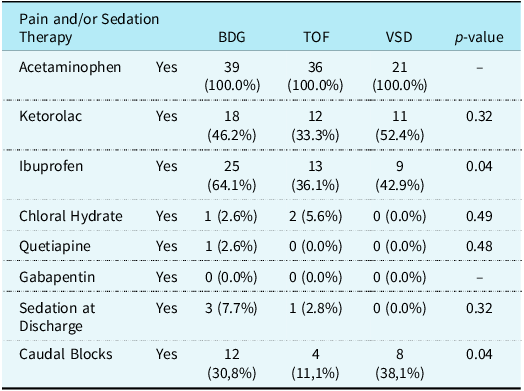
When comparing as-needed morphine bolus (p < 0.001), intermittent lorazepam (p < 0.001), and total dose of oxycodone (p < 0.001), both scheduled and as-needed, between the three groups, patients who underwent unilateral or bilateral bidirectional Glenn showed significantly higher utilisation in comparison with the other two groups. The total dose of morphine (p = 0.001) and dexmedetomidine infusions (p < 0.001) were also higher in the bidirectional Glenn group than in patients after ventricular septal defect repair, but equivalent to tetralogy of Fallot repair patients. Patients who underwent TOF repair utilised a higher total dose of morphine infusions, morphine PRN boluses, and dexmedetomidine infusions when compared to the ventricular septal defect repair group (Table 1). The use of adjunctive pain and sedative agents is displayed in Supplemental Table 2. There was no difference in the use of ketorolac, chloral hydrate, quetiapine, or gabapentin between the three groups, but ibuprofen use was more common in bidirectional Glenn patients (Table 2). Caudal blocks were also utilised for pain control more frequently in bidirectional Glenn (30.8%) and ventricular septal defect (38.1%) patients, than in tetralogy of Fallot patients (11%, p = 0.042). Patients who underwent bidirectional Glenn palliation had a significantly higher Glenn pressure than the CVP of the other two groups at admission, 12, 24, and 36 hours post-operatively. Tetralogy of Fallot and ventricular septal defect patients had equivalent CVP at every time point except for 12 hours post-operatively, when it was higher for patients subjected to tetralogy of Fallot repair. Differences in CVP were not significant at 48 hours post-operatively (Supplement Table 2).
Post-operative cumulative continuous and bolus sedation medications

* Data presented as median (IQR).
Additional post-operative pain and sedation therapies

* Data presented as n (%).
There was no significant difference in intubation status on arrival to the cardiac ICU (p = 0.30) or total hours of mechanical ventilation (p = 0.91) when comparing bidirectional Glenn patients to those who underwent both tetralogy of Fallot and ventricular septal defect repairs. The maximum Face, Legs, Activity, Cry, Consolability score was significantly higher in bidirectional Glenn (9 (interquartile range 9–10)) versus tetralogy of Fallot (8.5 (interquartile range 7–9) patients (p = 0.03). ICU length of stay, measured in days, was statistically different between surgeries, with bidirectional Glenn and tetralogy of Fallot repairs longer than ventricular septal defect repairs (interquartile range 2–4 versus 2–3 versus 1–2, respectively; p < 0.001). Differences in hospital length of stay were also statistically significant (p < 0.001), with unilateral and bilateral bidirectional Glenn length of stay longer than both tetralogy of Fallot and ventricular septal defect repairs (interquartile range 6–17 versus 2.7–7.2 versus 3–4, respectively; p < 0.001), and tetralogy of Fallot repair longer than ventricular septal defect repairs (Supplemental Table 1).
Comment
This study demonstrated that children who have undergone bidirectional Glenn received more sedation and analgesia during the post-operative period as compared to similar-aged children who have undergone tetralogy of Fallot and ventricular septal defect repairs. There are a variety of factors that can contribute to the need for sedation and analgesia during the post-operative periods in the cardiac ICU. All procedures looked at were STAT 1 or 2 category patients who presented from home and had repairs completed via a sternotomy. Bypass times were statistically longer for tetralogy of Fallot and bidirectional Glenn patients when compared to ventricular septal defect patients (p < 0.001), and, though not statistically significant, tetralogy of Fallot had longer bypass time than bidirectional Glenn patients. All patients returned to the cardiac ICU with similar monitoring equipment, including central and arterial lines, blood pressure cuffs, and electrocardiogram (EKG) leads, and there was no significant difference in intubation status upon arrival to the ICU or total hours of mechanical ventilation. A standardised post-operative sedation guideline was used for all patients, ensuring the same approach for pain control was utilised for all included patients. Reference Donnellan, Sawyer and Peach16 ICU length of stay was not statistically significant between bidirectional Glenn and tetralogy of Fallot (p = 0.968), and although significant between Glenn and ventricular septal defect (p < 0.001), ICU length of stay was 1 day and 2 days for ventricular septal defect and post-operative Glenn patients, respectively. Given that morphine and dexmedetomidine infusions can only be administered in the ICU setting, the longer length of stay may have contributed to the higher overall dexmedetomidine and morphine infusion dosages.
When comparing traditional factors thought to contribute to pain and discomfort during the post-operative period, none can demonstrate why bidirectional Glenn patients would need more analgesic and sedative medications during the post-operative period. The data did demonstrate that the Glenn pressure was higher compared to the CVP of patients who underwent ventricular septal defect or tetralogy of Fallot repair at the time of admission (p < 0.001), as well as 12 hours (p < 0.001) and 24 hours (p = 0.001) post-operatively. This pressure remained higher at 36 hours for patients who underwent bidirectional Glenn compared to ventricular septal defect repair.
Previous studies have demonstrated a significant rise in the Glenn pressure and CVP when compared to pre-surgical shunted physiology and those of other procedures. Reference Cabrera, Kibler and Easley4,Reference Neunhoeffer, Michel and Nehls6–Reference Bertolizio, DiNardo and Laussen8,Reference Cabrera, Kibler and Easley9,14 Glenn physiology results in cerebral-pulmonary continuity, causing elevated cerebral pressures, compared to patients without this continuity, including patients who have underwent tetralogy of Fallot and ventricular septal defect repair. This higher cerebral venous pressure is thought to contribute to the development of a “Glenn headache,” similarly seen with superior vena cava syndrome and contribute to the additional post-operative discomfort. Reference Simsic, Bradley and Mulvihill7,Reference Tripathi, Hafzalah and Harthan12–14,Reference Ackerman, Kralik and Daniels17–Reference Azizi, Shafi and Shah19 Our findings align with a previous study, which compared pre- and post-operative CVP in tetralogy of Fallot and bidirectional Glenn patients. Reference Ackerman, Kralik and Daniels17 The study demonstrated a statistically significant increase in CVP for bidirectional Glenn patients, with no significant change in the CVP of tetralogy of Fallot patients. Additionally, the cerebral ventricular size of bidirectional Glenn patients increased significantly from pre- to post-operative imaging, but remained stable for patients who underwent tetralogy of Fallot repair. Reference Ackerman, Kralik and Daniels17 While the post-operative CVP is elevated in both tetralogy of Fallot and bidirectional Glenn, this is a physiologic change for bidirectional Glenn patients and remains unchanged from the pre-operative state for tetralogy of Fallot patients. While bidirectional Glenn patients’ CVP measurements only account for the pressure in the upper compartment vasculature, the elevated CVP associated with tetralogy of Fallot patients allows pressure to be distributed between both the upper and lower vasculature.
Though this is not a new phenomenon to be discussed, this is the first paper known to us to statistically compare the amount of sedation and analgesic post-operative bidirectional Glenn patients receive as compared to other children of similar age undergoing cardiac repair. A previous study investigated the use of phenobarbital to reduce the need for opioids, benzodiazepines, and dexmedetomidine in this patient population. Reference Donnellan, Sawyer and Peach16 The study demonstrated a non-statistically significant reduction in all three medication groups when phenobarbital was administered. Reference Tripathi, Hafzalah and Harthan12 The results of our study can help to solidify clinical experiences with post-operative pain and discomfort in bidirectional Glenn patients, and help providers be more proactive and reactive in treating these patients’ pain and sedation needs. Additionally, future studies assessing whether these patients need alternative strategies and medications than other similar age post-operative patients are warranted.
Limitations
There are several limitations to this study. First, this was a single-centre, retrospective study, thus susceptible to confounders and bias inherent to such study designs. Most children who undergo a bidirectional Glenn have undergone a prior surgical and/or cardiac catheterisation laboratory-based intervention, as compared to few children who undergo ventricular septal defect and tetralogy of Fallot. It is unclear how these prior interventions, and associated narcotic and analgesic exposure, affect subsequent narcotic and analgesic requirements following the bidirectional Glenn. There are no data in our study that suggest this affected our patients post-operatively. To reduce the risk of these effects, all patients included in this study were discharged home during the interstage period. Additionally, all patients on habituation medications after discharge during the interstage period were excluded. While we assessed maximum pain score documented for each patient, we did not correlate individual pain scores during admission with medication administration. Given the psychological consequences of agitation leading to desaturation and potential inability to wait out normal calming measures in post-operative Glenn patients, we could not retrospectively account for the timing of administration of intermittent sedation/analgesia by bedside nurses when comparing them to the other repairs. It is also possible that analgesics may have been used to treat hypertension post-operatively, as post-operative ventricular septal defect and bidirectional Glenn patients are often hypertensive after their repair. Nicardipine and/or Nitroprusside are frequently utilised for hypertension post-operatively, and sedation and analgesia are typically administered based on pain assessment scales such as Face, Legs, Activity, Cry, Consolability and the State Behavior Scale. The use of age-appropriate pain scales, such as Face, Legs, Activity, Cry, Consolability, is utilised within this institution. It is difficult to know exactly what is causing discomfort for this patient population, given the developmental state of infants; however, all subjects were infants, so this challenge was universal amongst all participants. Finally, a limited sample size prohibited multivariate analysis.
Conclusion
This study demonstrates that patients who undergo bidirectional Glenn palliation receive more analgesic and sedation post-operatively than similar-aged patients who undergo tetralogy of Fallot or ventricular septal defect closure. Bidirectional Glenn patients were found to have higher Glenn pressure compared to the CVPs in the other repairs, which may contribute to the development of a “Glenn headache” and the higher sedation and analgesia during the immediate post-operative period.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951125109487
Acknowledgements
None.
Competing interests
All authors have no conflict of interest and no funding.
Ethical standard
Internal Review Board approval was obtained prior to study commencement on 3/2/2021, with a waiver of consent granted.



 Open access
Open access