


Depression is the most common mental illness globally, affecting over 300 million people worldwide. Reference Liu, He, Yang, Feng, Zhao and Lyu1,Reference Vos, Abajobir, Abate, Abbafati, Abbas and Abd-Allah2 It is a leading cause of years lived with disability. Reference Vos, Abajobir, Abate, Abbafati, Abbas and Abd-Allah2 The manifestation of depressive symptoms can vary across ethnic groups, often influenced by cultural notions of distress, religious beliefs, social norms and language. Reference Shafi and Shafi3 A systematic review of depression symptoms worldwide found that individuals in South Asia had a higher prevalence of somatic symptoms – bodily sensations and physical dysfunctions Reference Kapfhammer4 – compared with those in other regions. Reference Haroz, Ritchey, Bass, Kohrt, Augustinavicius and Michalopoulos5 In South Asian countries, four of the five most common depression symptoms reported were somatic, including ‘headaches and issues with the heart’, which are not recognised in ICD-11 diagnostic criteria. Reference Haroz, Ritchey, Bass, Kohrt, Augustinavicius and Michalopoulos5–7 Only one of the two cardinal symptoms listed in ICD-11 – low mood – was ranked in the top five. There is a gap in knowledge of symptom experiences in South Asian diaspora populations, which might be influenced by adaptation to a new cultural environment (acculturation). There is also a lack of understanding of differences in depression symptomology among different South Asian populations, including different ethnicities represented in the South Asian diaspora. Reference Poole, Rickford, Martinez, Gill, Frith and Ronaldson8 Awareness of different clinical presentations is necessary for accurate diagnosis, and thus understanding symptom heterogeneity is important for combatting health inequalities.
In the UK, South Asian groupsFootnote a form the largest minority ethnic population. 9 A systematic review found higher rates of total depressive symptoms for South Asian compared with White British groups. Reference Rees, Stokes, Stansfield, Oliver, Kneale and Thomas10 However, despite consulting with their GP more frequently than their White counterparts, Pakistani women in the UK have been found to be less likely to receive treatment for depression. Reference Gater, Tomenson, Percival, Chaudhry, Waheed and Dunn11 Ethnic differences in depressive symptomology, and associated problems with the validity and reliability of diagnostic screening tools, may be factors in explaining such findings.
This review aims to explore reported depression symptoms among the South Asian diaspora, comparing these with ICD-11 diagnostic criteria, considering acculturation and ethnic differences. It forms part of the National Institute of Health Research (NIHR)-funded ‘Prescribing Antidepressants in Primary care: Ethnic inequalities in tReatment’(PAPER) Study, which is investigating symptoms and treatment of depression among people of South Asian populations in the UK. Reference Poole, Ronaldson, Frith, Gill, Sajid and Rickford12 Because evidence suggests that there may be a relationship between language and reported depression symptoms, Reference Kim, DeCoster, Huang and Bryant13 in order to maximise relevance to the UK context, this review focuses on symptomology among South Asian populations in English-speaking countries with large South Asian diasporas.
Method
A systematic scoping review was selected as the appropriate method because it allows a systematic search strategy in order to produce evidence synthesis for broad research questions, with the inclusion of a wide range of different types of literature. Reference Peters, Marnie, Tricco, Pollock, Munn and Alexander14
Search strategy and selection criteria
The review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Scoping Reviews (PRISMA-Scr) guidance. Reference Tricco, Lillie, Zarin, O’Brien, Colquhoun and Levac15 It included original qualitative, quantitative and/or mixed-method studies, written in English, that were based on findings from adult participants of the South Asian diaspora living in the UK, USA, Canada, Australia and/or New Zealand,Footnote b and where reported findings included details of symptoms of study participants experiencing depression (diagnosed or self-identified), or mental distress where authors identified symptoms as being potential indicators of depression. Studies were excluded if South Asian-specific findings could not be extracted from wider demographic categories and, for quantitative studies, where depression symptoms were not reported item by item. Studies in which depression was considered alongside another disease, such as diabetes or cancer, were also excluded, as were studies that focused solely on postpartum depression. There was no limit on publication date. The review protocol was pre-registered with Open Science Framework. Reference Francois-Walcott, Ramasawmy and Poole16 A detailed search strategy is presented in Appendix 1.
Information sources
Database searches of SCOPUS, EMBASE, PubMed, PsychInfo, Web of Science, Google Scholar, ProQuest and The Kings Fund were conducted in March–May 2024 and updated in July–October 2024 (R.F.-W., R.R.). Search terms were identified to target three core concepts: depression, South Asian and people living in the UK, USA, Canada, Australia and New Zealand. Search terms designed to target these concepts were piloted for validity before the final searches were conducted.
Study selection
Search results were de-duplicated in EndNote 21 for Windows (Clarivate, Philidelphia, PA, USA; see =https://support.clarivate.com/Endnote/s/article/Download-EndNote?language=en_US) and then imported into Rayyan for Windows (Rayann, Cambridge, MA, USA; see https://www.rayyan.ai/) for screening. Titles and abstracts were screened against inclusion and exclusion criteria (R.F.-W., O.O., R.R.), with 10% of papers reviewed by two reviewers. Full-text screening was conducted (R.F.-W., O.O,. A.M., R.R.), with at least two authors screening each paper. Throughout the screening process, disagreements were resolved first through discussion between two reviewers, followed by consultation with a third reviewer (L.P. or M.R.) if consensus could not be reached. Once an initial list of full texts had been identified, forward-and-backward citation searching was carried out (R.F.-W., R.R.) to identify further relevant studies.
Data analysis
A data-charting form (see Appendix 2) was drafted by R.R. in consultation with A.M., L.P. and M.R. The form was piloted by R.R. and A.S. using five randomly selected studies to check consistency among authors. A summary of charted data is provided in Appendix 3.
Qualitative content analysis, Reference Schreier17 an established method for use in reviews, Reference Snilstveit, Oliver and Vojtkova18 was used to identify (a) reported symptoms and common ways of describing or expressing distress and depression experiences and (b) symptom comparisons between ethnicities. Studies were categorised into three groups: (a) those in which an overall list of symptoms/symptom prevalence in the sample was presented; (b) those in which symptoms were analysed in comparison with a White majority population in the country where the study was based; and (c) those in which symptoms were mentioned only in passing, or in data extracts while presenting other findings.
To identify reported symptoms and ways of describing and expressing distress and depression, findings and quotations from all papers were coded using NVivo 12 for Windows (Lumivero, Denver, CO, USA; see https://lumivero.com/products/nvivo/). Coding captured symptoms not currently widely recognised as indicative of depression, as well as those that are. For qualitative studies, in which participants described their experience in their own words, all reported symptoms were coded.Footnote c For quantitative studies, where participants selected symptoms from a predetermined list, the most frequently selected symptoms were coded.Footnote d To identify symptoms that are more common among South Asian populations than other ethnic groups, comparative findings from Group B articles were additionally charted in Excel. The final principal findings were developed by comparing codes and charting from the two subanalyses to identify widely reported depression experiences among South Asian diaspora populations, including when compared with other populations, which are not currently recognised in diagnostic criteria for major depressive disorder.
Results
Papers selected for review
A total of 9689 unique papers were identified through searches. Forty were selected through screening (n = 30) and forward-and-backward citation searching (n = 10), of which 26 were qualitative, 13 were quantitative and 1 used mixed methods. See Fig. 1 for a PRISMA flowchart of the screening process.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram.

The included papers reported research conducted in the UK (n = 25), Canada (n = 9), USA (n = 4) and Australia (n = 2), with participants of Pakistani (n = 15), Indian (n = 14), Punjabi (n = 8), Bangladeshi/Bengali (n = 5), Sri Lankan (n = 1), Tamil (n = 1), Nepalese (n = 1) and Afghan (n = 1) heritage.Footnote e The remaining studies focused on non-specified South Asian diaspora populations (n = 8). Of the papers that reported the birth country of participants (n = 27), the majority (85%) of participants were first-generation immigrants from South Asian countries.
Twenty-two (22) of the papers (11 qualitative, 11 quantitative) included an authors’ analysis of depression symptoms in South Asian participants. Reference Mansour, Tsamakis, Rizos, Perera, Das-Munshi and Stewart19–Reference Malik40 This included 14 studies (10 qualitative, 4 quantitative) reporting depression symptoms among a South Asian sample (Group A) (Fig. 2), and 11 studies (8 quantitative, 3 qualitative) comparing the symptomology of South Asian and White samples (Group B) (Table 1). Three studies are included in both groups. Reference Brijnath and Antoniades22,Reference Mallinson and Popay29,Reference Malik40
Symptoms of depression among South Asian diaspora samples (Group A papers).

Comparison of South Asian diaspora and White samples (Group B papers)

K10, Kessler Psychological Distress Scale; DSM-IV, Diagnostic and Statistical Manual of Mental Disorders; ADI, Amritsar Depression Inventory; GHQ-12, General Health Questionnaire; BSI, Bradford Somatic Index; HADS, Hospital Anxiety and Depression Scale; AKAUDS, Aga Khan University Anxiety and Depression Scale; SRQ, Self-Reporting Questionnaire; SCAN, Schedules for Clinical Assessment in Neuropsychiatry; LEDS, Life Events and Difficulties Schedule; NR, not reported; N/A, not applicable.
a. White and South Asian samples were not matched on gender or age.
All reported symptoms

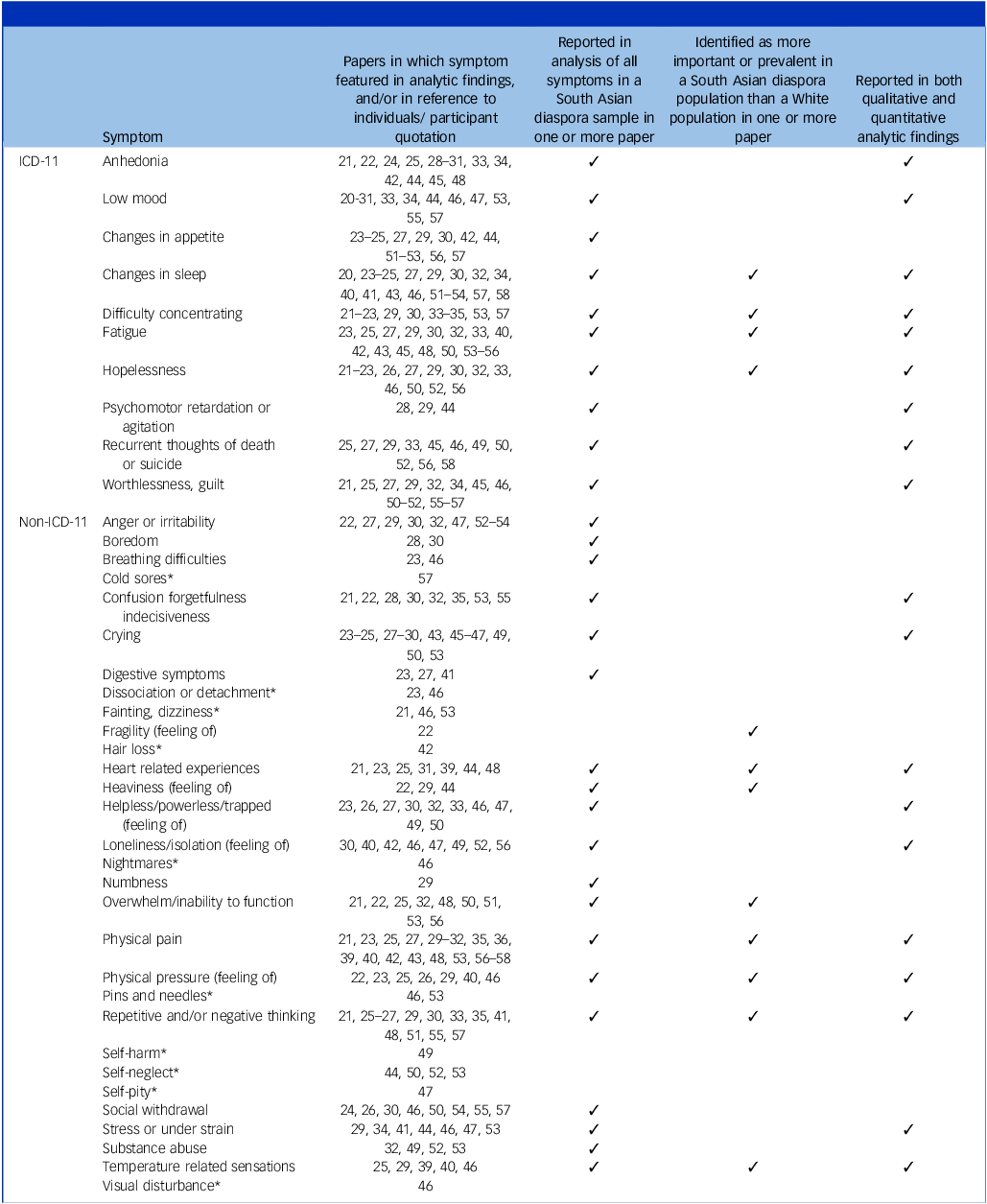
* Symptom mentioned only in description of individuals or in participant quotation. Not included in any paper’s reported analytic findings.
The remaining 18 papers focused their analyses on other topics (e.g. depression coping strategies; barriers to accessing care; cultural conceptions of mental illness) and included ad hoc content on depression symptoms while reporting other findings. Reference Agarwal-Narale41–Reference Husain, Creed and Tomenson58 This content was coded and contributes to the full list of symptoms featured across the reviewed literature (Table 2), and is drawn upon in the written analysis.
Principal findings
Qualitative content analysis generated a list of symptoms reported across the literature (Table 2). Three principal findings are outlined in detail below. These are symptoms, or groups of symptoms, reported widely across the literature in both qualitative and quantitative studies, including studies comparing South Asian diaspora populations with White populations. The first finding is that somatic symptoms of depression are prevalent, particularly sleep disturbance, which is listed in ICD-11, and physical pain, which is not. Second, individuals described their depression using language relating to the heart. Third, there is a prevalence of repetitive negative thinking, which may be related to trauma.
Our analysis also identified multiple reports of ‘tension’. Reference Akram21,Reference Mallinson and Popay29,Reference Yusuf32,Reference Malik40,Reference Agarwal-Narale41,Reference Bottorff, Johnson, Venables, Grewal, Popatia and Hilton44,Reference Upadhya57 Rather than being presented as a symptom of depression, this was described as being similar to enduring stress and is therefore not included as a principal finding, but is summarised in Appendix 4.
Principal finding 1: somatic symptoms of depression
Figure 2 maps the number of papers identifying different ICD-11 and non-ICD-11 features of depression in 14 papers reporting symptoms among South Asian participants (Group A). This includes ten qualitative papers examining experiences reported by participants during interviews, Reference Akram21–Reference Gask, Aseem, Waquas and Waheed26,Reference Mallinson and Popay29,Reference Rafique30,Reference Yusuf32 and four quantitative papers reporting symptoms measured using questionnaires. Reference Ahmed, Ahmed, Carmichael and Sami20,Reference Lai and Surood28,Reference Silveira and Ebrahim31,Reference Malik40 The cardinal symptom of low mood was reported in the greatest number of papers (12 of 14). Reference Ahmed, Ahmed, Carmichael and Sami20–Reference Silveira and Ebrahim31 However, the cardinal symptom of anhedonia was reported in the same number of papers (8 of 14 Reference Akram21,Reference Brijnath and Antoniades22,Reference Chalal24,Reference Fenton and Sadiq-Sangster25,Reference Lai and Surood28,Reference Rafique30,Reference Silveira and Ebrahim31,Reference Bottorff, Johnson, Venables, Grewal, Popatia and Hilton44 ) as the non-cardinal somatic symptoms of sleep disturbance (8 of 14 Reference Ahmed, Ahmed, Carmichael and Sami20,Reference Burr23–Reference Fenton and Sadiq-Sangster25,Reference Grewal27,Reference Mallinson and Popay29,Reference Rafique30,Reference Yusuf32 ) and physical pain (8 of 14 Reference Akram21,Reference Burr23,Reference Fenton and Sadiq-Sangster25,Reference Mallinson and Popay29–Reference Yusuf32,Reference Malik40 ), one of which (pain) is not listed in ICD-11. Reports of sleep disturbance included difficulty falling asleep, early morning awakening and disturbed sleep. Reports of pain included unspecified physical pain, body aches and pains, neck pain and headaches. Other somatic symptoms reported included nausea and vomiting, Reference Burr23,Reference Gask, Aseem, Waquas and Waheed26,Reference Grewal27 sensations related to the heart, Reference Akram21,Reference Burr23,Reference Fenton and Sadiq-Sangster25,Reference Silveira and Ebrahim31 temperature-related sensations, Reference Fenton and Sadiq-Sangster25,Reference Mallinson and Popay29 feelings of heaviness, Reference Brijnath and Antoniades22,Reference Mallinson and Popay29 feelings of numbness Reference Mallinson and Popay29 and sensations of pressure, squeezing or squashing. Reference Brijnath and Antoniades22,Reference Burr23,Reference Fenton and Sadiq-Sangster25,Reference Gask, Aseem, Waquas and Waheed26,Reference Mallinson and Popay29 Somatic symptoms were also reported in quotations provided in the 18 papers in Group C, in which authors did not specifically analyse depressive symptoms (in studies including Pakistani, Indian, Bangladeshi, Punjabi, Sri Lankan, Afghan, Tamil and unspecified ‘South Asian’ participants Reference Agarwal-Narale41–Reference Dein46,Reference Hussain and Cochrane48,Reference Morrow and Krishna52,Reference Robinson54–Reference Upadhya57 ), with participants reporting, for example ‘terrible headache’, Reference Pandalangat53 ‘felt sick’, Reference Agarwal-Narale41 burning sensations Reference Bottorff, Johnson, Venables, Grewal, Popatia and Hilton44 , dizziness and fainting Reference Akram21,Reference Dein46,Reference Pandalangat53 and hair loss. Reference Ahmad, Shik, Vanza, Cheung, George and Stewart42
Table 1 reports the 11 papers (8 quantitative, 3 qualitative) that compared symptoms between South Asian and White participants (Group B). Only the two most recent of these reported their findings in relation to ICD or DSM 7 symptoms, and neither found a significant difference in somatic symptoms between South Asian and White patients. These included a 2017 qualitative study comparing Anglo-Australian and Sri Lankan depression patients living in Australia, Reference Antoniades, Mazza and Brijnath33 and a 2020 quantitative study using clinical records of south London (UK) depression patients aged over 65 years. Reference Mansour, Tsamakis, Rizos, Perera, Das-Munshi and Stewart19 However, earlier studies comparing South Asian and White participants included symptoms not listed in ICD and, overall, these studies indicate a possible pattern of South Asian individuals experiencing higher rates of somatic symptoms compared with White individuals. A 2007 qualitative study used semi-structured interviews and distress screening tools (Self-Reporting Questionnaire, Reference Beusenberg and Orley59 Schedules for Clinical Assessment in Neuropsychiatry Reference Wing, Babor, Brugha, Burke, Cooper and Giel60 and Life Events and Difficulties Schedule Reference Brown and Harris61 ) to explore representations of distress among Pakistani and White people in north-west England. While the authors reported no clear difference in the prevalence of somatic symptoms overall, Pakistani participants reported temperature changes and feelings of pressure and heaviness in the head, which White patients did not. Reference Mallinson and Popay29 A 1996 quantitative study compared rates of depression symptoms (measured through the Hospital Anxiety and Depression Scale (HADS) Reference Zigmond and Snaith62 ) and somatic symptoms (measured through the Bradford Somatisation Index (BSI) Reference Mumford, Bavington, Bhatnagar, Hussain, Mirza and Naraghi63 ) among White and Asian (predominantly Pakistani and Indian) patients at two GP practices in England. Affective and cognitive elements of depression measured using HADS were similar between groups, but Asian patients were more likely to report a ‘weak or sinking heart, ‘aches and pains all over the body’ and ‘a feeling of heat inside your body’ on BSI. Reference Sham, Farooq, Gahir, Okyere, Sheikh and Oyebode39 A 2004 study measured symptoms among White English and Punjabi primary care patients in London using the General Health Questionnaire (GHQ-12) Reference Goldberg64 and the Amritsar Depression Inventory (ADI), Reference Singh, Verma, Verma and Kaur65 the latter having been developed in the Punjab region of India, containing somatic symptoms not included in GHQ-12. Reference Bhui, Bhugra, Goldberg, Sauer and Tylee36 The researchers also conducted a second-stage interview that included questions about somatic symptoms. They found that Punjabi patients with somatic symptoms (defined as ‘any sort of ache or pain, for example headache or indigestion, or any other sort of bodily discomfort’ that the patient considers is ‘due to, or made worse by, feeling low, anxious or stressed’) were more likely to report depression than White English patients with somatic symptoms defined in the same way; Reference Bhui, Bhugra, Goldberg, Sauer and Tylee36 however, another paper from the same team reported that the ADI item ‘I feel sad because of aches and pains’ was a predictor of depression cases in White English patients but not in Punjabi patients. Reference Bhui, Bhugra and Goldberg34 (We suggest that the presence of physical illnesses may affect responses to this latter item, but because physical illnesses were not reported in the paper their impact cannot be assessed.) A 1997 thesis used GHQ-28 to compare symptoms of Pakistani people in Britain with both a White British sample and a sample of Pakistani people living in Pakistan. Reference Malik40 GHQ-28 includes somatic symptoms such as temperature-related sensations, headaches and a feeling of pressure in the head and, when using this tool, the study found that Pakistani people living in Britain had levels of somatic symptoms similar to those living in Pakistan, which were higher than for the White British sample.
Overall, our analysis paints a picture of South Asian diaspora patients experiencing a range of somatic symptoms of depression, with sleep changes and physical pain reported in the most studies. Studies directly comparing recognised symptoms among South Asian and White participants did not find that sleep changes, or any ICD somatic symptoms, were more prevalent among South Asian participants. However, other somatic symptoms not captured in ICD, such as physical pain, sensations of pressure and heaviness, and temperature-related sensations, were found to be more prevalent among South Asian than White samples.
Principal finding 2: references to the heart
A 1996 study used BSI to measure somatic symptoms among patients of different ethnicities in south London. The authors found that South Asian (predominantly Pakistani, some Indian) patients were more likely than White patients to report ‘weak or sinking heart’ on BSI. Reference Sham, Farooq, Gahir, Okyere, Sheikh and Oyebode39 This was identified as potentially being related to idiomatic use of these phrases in both Punjabi and Urdu. In Punjabi, ‘sinking heart’ refers to a condition that has both physiological and psychological aspects, which are understood to interrelate. Reference Krause66 ‘The heart sinks’ is used in Urdu to express sadness and despair, while ‘weakening heart’ can be used to describe someone who is easily fearful or overwhelmed. Similar language was used in qualitative studies. In a 1996 qualitative study of South Asian (mostly Punjabi) women in the UK, participants used expressions including ‘my heart kept falling and falling’, ‘the life would go out of my heart’, ‘my heart is weak’ and ‘my heart felt as if someone was pushing it down’. Reference Fenton and Sadiq-Sangster25 A 2012 qualitative study of Pakistani (85%) and Indian (15%) Muslim immigrants in Toronto, Canada, reported that Punjabi-, Hindi- and Urdu-speaking participants described heart-related experiences including ‘sinking heart’, ‘dead heart’ and ‘emptiness of heart’. Reference Akram21
It is not possible to clearly delineate between references to the heart that refer to somatic symptoms and those which do not. Indeed, there are different perspectives on whether references to the body in accounts of distress and depression should be understood as somatic, metaphorical or as expressions of a way of understanding distress that understands the body and mind as part of a single experience. A 1995 quantitative study of elderly Bengali people in London found that 77% of participants reported heart-related symptoms such as pounding and breathlessness. Reference Silveira and Ebrahim31 In contrast, Akram, author of the aforementioned 2012 study of South Asian Muslims in Toronto, interpreted expressions relating to the heart as referring to affective, rather than somatic, experiences, including sadness and emotional turmoil. Reference Akram21 However, quotes from participants in her thesis suggest that heart-related symptoms were, at times, experienced physically:
‘I was feeling as if someone has held my heart in his hand tightly and squeezing it continuously … sometimes I was not able to breathe properly.’ (p.113) (Pakistani Urdu speaker)
Some have suggested that references to the body, including the heart, in South Asian expressions of distress should be understood within the context of a non-Cartesian understanding of the relationship between mind and body. Krause argues that, for Punjabis, sinking heart ‘has at the same time a somatic and psychological meaning’. Reference Krause66 Participants in several studies made reference to cognitive symptoms in relation to the heart, using phrases including ‘thinking too much in my heart’ (Punjabi participants Reference Fenton and Sadiq-Sangster25 ), ‘my heart was sinking with these thoughts’ (Indian Hindi speaker Reference Akram21 ) and ‘thoughts and words in my heart’ (South Asian Muslim Reference Hussain and Cochrane48 ). Participants in some papers made references to causal relationships between body and mind. For example, in a 1996 study of South Asian women in the UK, participants (who were mostly Punjabi) expressed that thinking in the heart led to illness, including pressure in the head (causing headaches Reference Fenton and Sadiq-Sangster25 ). In a 2015 study on mental health conceptualisations among young Nepalese people in the UK, one participant expressed the belief that ‘the worry or stress or tension keeps adding up and makes somebody have headaches or fever’. Reference Upadhya57 Meanwhile, a 1997 study comparing Pakistani patients with depression in the UK with White British and Pakistani (in Pakistan) patients found that Pakistani patients living in Britain, and those living in Pakistan, understood depression through a conceptualisation of the ‘emotional body’ (a term coined by Ots in relation to Chinese medicine Reference Ots67 ), rejecting the body–mind dichotomy, and this distinguished them from White UK patients. Reference Malik40 These accounts appear to support a non-dualistic conceptualisation of depression symptoms, with cognitive and somatic symptoms being experienced holistically. This is consistent with the Ayurveda and Unani Tibb medical systems, which are widely practised in South Asian countries. Reference Sheehan and Hussain68,Reference Obeyesekere69
Principal finding 3: repetitive negative thinking
A 2006 cross-cultural comparison of conceptualisations of depression in the UK found that older South Asian adults were more likely to see depression as related to trouble with the mind and thinking, compared with older Black Caribbean and White British adults, who were more likely to see it as related to mood. Reference Lawrence, Murray, Banerjee, Turner, Sangha and Byng51 A 2007 comparison of British Pakistani and White British patients found that Pakistani patients were more likely to refer to ‘too much thinking’. Reference Mallinson and Popay29 A 2017 cross-cultural comparison of experiences of depression in Australia found that people of Sri Lankan heritage explained their depression in terms of ‘overthinking’, while Anglo-Australians did not. Reference Antoniades, Mazza and Brijnath33
Repetitive thinking was a reported symptom in five symptom analyses (Group A Reference Fenton and Sadiq-Sangster25,Reference Gask, Aseem, Waquas and Waheed26,Reference Mallinson and Popay29,Reference Rafique30,Reference Yusuf32 ), and was also reported by participants in studies that did not provide an analysis of symptoms (Group C). Ways of describing this included ‘thinking negatively all the time’, Reference Akram21 ‘thoughts go around in your head’, Reference Lawrence, Murray, Banerjee, Turner, Sangha and Byng51 ‘thinking too much’, Reference Fenton and Sadiq-Sangster25 thoughts repeating themselves ‘like a film’ Reference Fenton and Sadiq-Sangster25 and ‘I repeatedly kept thinking about things’. Reference Gask, Aseem, Waquas and Waheed26 These experiences sometimes included references to a sense of thoughts being uncontrollable, and/or that repetitive thinking was having a detrimental impact on health. Reference Rafique30,Reference Upadhya57 Repetitive negative thinking is not listed as a symptom of depression in ICD-11. One form of repetitive negative thinking is rumination, Reference McEvoy, Mahoney and Moulds70 which has been found to be more common in depression where trauma is a factor, than in depression without trauma. Reference Birrer and Michael71,Reference Cano-López, García-Sancho, Fernández-Castilla and Salguero72 Some studies reported depression symptoms as responses to trauma among Punjabi, Afghan, Tamil and Indian participants. Reference Chalal24,Reference Agarwal-Narale41,Reference Johnson50,Reference Morrow and Krishna52,Reference Pandalangat53 Meanwhile, trauma is known to be a common aspect of experience among migrant populations, Reference Tummala-Narra73,Reference Lijtmaer74 and it has been argued that mental health among the South Asian diaspora is impacted by intergenerational trauma. Reference Qureshi, Misra and Poshni75 It is possible that the prevalence of repetitive negative thinking among the South Asian diaspora may be related to trauma among this population.
Gap identified: acculturation and ethnic differences
Only four papers considered acculturation differences in their analyses of depression symptoms, Reference Lai and Surood28,Reference Bhui, Bhugra and Goldberg34,Reference Bhui, Bhugra, Goldberg, Sauer and Tylee36,Reference Malik40 and each of these is at least 17 years old. A 2000 study assessed the validity of GHQ-12 and ADI (developed in the Punjab region of India) among Punjabi and White English primary care patients in south London. Reference Bhui, Bhugra and Goldberg34 The team found that ADI was better at detecting depression among White English patients than Punjabi patients, but that it was not a valid tool for use with either group. Among Punjabi patients who had been in England for more than 30 years, ADI was no better than chance. GHQ-12 was a more valid tool for measuring depression in both Punjabi and White English patients, and its validity among Punjabi patients did not change depending on length of residency in England, which suggests that there were no acculturation differences in the validity of GHQ-12. The article did not include analysis of acculturation differences in specific symptoms. A 2008 study of older South Asian Canadians (majority Indian) used the Geriatric Depression Scale (GDS) and found that length of residency was not significantly associated with depression caseness, but that those who had been in Canada for <10 years were more likely to report ‘feeling not in good spirits most of the time’ and ‘not feeling happy most of the time’ than those who had been in Canada >10 years. Reference Lai and Surood28 It should be noted, however, that GDS includes only one somatic symptom – psychomotor agitation. This means that none of the somatic symptoms most prevalent in South Asian countries Reference Haroz, Ritchey, Bass, Kohrt, Augustinavicius and Michalopoulos5 were assessed. Two further studies found no acculturation differences. Reference Bhui, Bhugra, Goldberg, Sauer and Tylee36,Reference Malik40 Overall, no acculturation pattern can be discerned from these four studies. There was a lack of literature on the specific experience of people of South Asian heritage born in English-speaking countries, and no papers compared this population with first-generation South Asian migrants.
No papers included in this review considered differences between people of different South Asian ethnicities. One study considered religious differences and found that Muslims reported ‘often get bored’ and ‘feel pretty worthless’ more often than Hindus and Sikhs, while there was no significant difference in overall depression prevalence between these groups. Reference Lai and Surood28 Overall, there was insufficient evidence to draw conclusions regarding the effects of acculturation or ethnic differences in depression symptomology. This indicates a gap in research.
Discussion
This systematic scoping review has found that the South Asian diaspora in English-speaking countries experience symptoms of depression that differ from those of the White majority in those countries, and in ways that differ from the diagnostic criteria detailed in ICD-11. Physical pain (specifically headaches) and heart-related sensations are prevalent symptoms of depression in South Asian countries, Reference Haroz, Ritchey, Bass, Kohrt, Augustinavicius and Michalopoulos5 and this review has found that these are also widely reported among diaspora populations. Sleep disturbances are commonly reported among South Asian diaspora populations and were found in the same number of studies as anhedonia, but studies directly comparing South Asian and White patients have not found sleep symptoms to be more prevalent in South Asian than in White samples. Repetitive negative thinking may be more prevalent among South Asian diaspora groups than White majority groups in English-speaking countries, which could be associated with trauma among South Asian migrant populations. Reference Birrer and Michael71,Reference Lijtmaer74–Reference George77
Appropriate treatment requires accurate detection. Differences in symptoms of depression may therefore be implicative of inequalities in treatment, if those differences are not accounted for in diagnostic practice. While ICD-11 has increased emphasis on cultural factors and diversity compared with previous versions, culturally informed diagnosis requires clinical judgement informed by cultural competence and cultural humility, Reference Yeager and Bauer-Wu78 rather than simple adherence to nosological criteria. Reference Gureje, Lewis-Fernandez, Hall and Reed79,Reference van de Water, Suliman and Seedat80 Despite attempts to recognise cultural differences in broad clinical guidelines, 81,Reference First, Reed, Hyman and Saxena82 greater attempts are needed within specific diagnostic classifications to recognise diverse experiences. Diagnosis in UK primary care relies on rapid assessment of symptoms during short consultations, within a context of declining rates of continuity of care. Reference Tammes, Morris, Murphy and Salisbury83 Identification of culturally specific patterns of symptomology is important, both for the long-term goal of reducing nosological bias towards White populations in the Global North and for improving diagnostic capacity among clinicians, including in primary care settings.
Statement from the PAPER study patient and public involvement panel
We are a group of five, resident in England and of Indian and Pakistani heritage, all with experience of living with depression or supporting a loved one living with depression. Depression is under-recognised in our communities. Sometimes it manifests as physical symptoms, such as headaches, muscle tension or chest pain. This highlights the significant interplay between mental health challenges and physical discomfort. In some cases, we use terms such as ‘tension’ or ‘worry’ to describe ongoing psychological stress and distress, and we may not always understand how these experiences can relate to mental health diagnoses such as anxiety or depression. Older generations often find it harder to understand emotional struggles, which creates a generational divide in perceptions of mental health. This becomes more complex in immigrant families, and often emotional burdens are carried in silence, especially after difficult caregiving experiences. Our religious practices also have a direct impact on our perceptions of depression, and consequently on our help-seeking behaviours. There is a need for improved understanding of mental health within South Asian communities, as well as a critical need for healthcare professionals to enhance their understanding of South Asian populations to provide the tailored and culturally appropriate support that we need.
Limitations and gaps
Findings are limited by the availability of literature. The review has found gaps in up-to-date literature on depression symptomology among South Asian diaspora populations, particularly in relation to accultural and ethnic differences, and among some South Asian ethnicities.
While 22 papers provided a synthesised list of symptoms of depression/distress or a comparison of symptoms across ethnicities, only 3 of these set out explicitly to describe symptoms of depression among a South Asian diaspora population. Reference Mansour, Tsamakis, Rizos, Perera, Das-Munshi and Stewart19,Reference Grewal27,Reference Lai and Surood28 Other papers focused on related questions such as experiences of migration, Reference Akram21 cultural representations of depression, Reference Antoniades, Mazza and Brijnath33 depression prevalence, Reference Bhui, Bhugra, Goldberg, Sauer and Tylee36 experiences of help-seeking, Reference Chalal24 prevalence of specific symptoms (such as somatic symptoms Reference Farooq, Gahir, Okyere and Sheikh38 or self-harm Reference Cooper, Husain, Webb, Waheed, Kapur and Guthrie37 ) and the cultural appropriateness of depression screening tools. Reference Bhui, Bhugra and Goldberg34 This could mean that the lists of symptoms offered in such papers may not be comprehensive. This discrepancy in the aims and objectives of included papers, compared with the aim of the present review, may have resulted in bias in the findings available for review, and Figure 2 and Table 2 should be viewed in consideration of this. The review has identified a shortage of research specifically aiming to describe depression symptoms among the South Asian diaspora.
Only ten reviewed studies were conducted within the last decade, so some are likely to be based on data that do not reflect the current sociopolitical environment. It was not possible to address the question of whether people of South Asian heritage who are born in English-speaking countries share symptomology with first-generation migrants or those living in South Asian countries. A qualitative study has found that GPs perceive acculturation differences in how South Asian patients present with chronic and unexplained pain, which indicates that these differences may be important for understanding the role of pain in depression. Reference Patel, Peacock, McKinley, Carter and Watson84 Research is needed to explore differences between depression symptoms among first-generation South Asian migrants and people of South Asian heritage born in English-speaking countries.
Because there are substantial cultural, religious, socioeconomic and political differences across the South Asian region, and migration patterns vary substantially, it is anticipated that the South Asian diaspora are unlikely to present as a homogenous group. Reference Poole, Rickford, Martinez, Gill, Frith and Ronaldson8 Available literature is insufficient to support conclusive comparisons between ethnicities. Mood disorders have been found to be more prevalent among Pakistani Muslim women than Indian Hindu women in the UK, which indicates ethnic or religious differences in depression between these groups (which may relate to prevalence, detection and/or help-seeking Reference Anand and Cochrane85 ). Moreover, the majority of papers focused on Punjabi, Indian, Pakistani or unspecified South Asian populations while some South Asian ethnicities, such as Nepalese, Bhutanese and Afghan, were not represented in any of the papers that provided analyses of symptoms.
Implications for clinical practice and policy
This review suggests that GPs assessing South Asian diaspora patients should consider the possibility of non-ICD-11 somatic symptoms in the diagnosis of depression, particularly physical pain. These may be reported by patients as the presenting symptom, rather than affective or cognitive symptoms. Reference Husain, Creed and Tomenson58 People of various South Asian communities use references to the heart when describing their symptoms of depression, and primary care practitioners should be alert to these references as potentially indicative of mood disorders. Members of South Asian diaspora populations also experience repetitive negative thinking as part of depression, possibly at higher rates than the White majority in English-speaking countries. This may be related to high levels of trauma within these populations.
These findings call into question the appropriateness of depression screening tools widely used in UK National Health Service (NHS) primary care settings and in NHS Talking Therapies, in patients of South Asian heritage. For example, the Patient Health Questionnaire-9 (PHQ-9) is based on ICD-11 diagnostic criteria for depressive disorders, which does not include physical pain, heart-related symptoms nor repetitive negative thinking. The findings of this review support arguments for the need for clinical judgement informed by cultural humility in the application of nosology in context. Reference van de Water, Suliman and Seedat80 Training of primary care professionals in specific presentations of depression among South Asian diaspora populations is therefore recommended.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10539
Data availability
A summary of the charted data is included as an appendix. A full copy of the charted data is available on request from the corresponding author (R.R.).
Acknowledgements
This article includes a statement from the PAPER Study Patient and Public Involvement (PPI) Panel, which has five members. Four members are named as authors. The authors thank one additional member, who wishes to remain anonymous. For the purpose of open access, the author has applied a Creative Commons attribution license to any author-accepted manuscript version arising from this submission.
Author contributions
R.R.: data curation; investigation; formal analysis; validation; visualisation; writing – original draft; M.R.: funding acquisition; conceptualisation; supervision; methodology; validation; writing – review and editing; R.F.-W.: data curation; investigation; validation; writing – review and editing; A.M.: validation; writing – review and editing; M.S: PPI facilitation; writing – original draft; O.O.: data curation; investigation; validation; writing – review and editing; A.S.: validation; F.D.: PPI member; H.F.: funding acquisition; conceptualisation; supervision; writing – review and editing; P.G.: funding acquisition; conceptualisation; supervision; writing – review and editing; H.K.: PPI member; A.R.: funding acquisition; conceptualisation; supervision; writing – review and editing; T.S.: PPI member; L.P.: funding acquisition (principal investigator); conceptualisation; methodology; supervision; project administration; validation; writing – review and editing.
Funding
The authors are supported by funding from NIHR (no. 155654).
Declaration of interest
P.G. is supported by the NIHR Applied Research Collaboration and is a NIHR senior investigator. The views expressed in this publication are those of the authors and not necessarily those of the NIHR or the UK Department of Health and Social Care.
Transparency declaration
This manuscript is an honest, accurate and transparent account of the study being reported. No important aspects of the study have been omitted, and any discrepancies from the study as planned and registered have been explained.
Analytic code availability
Qualitative codes used in the thematic analysis presented are available on request from the corresponding author (R.R.).






 Open access
Open access
eLetters
No eLetters have been published for this article.