


The prolonged military offensive in Gaza has taken a serious toll on the mental health of Palestinian children, who have been found to have a significantly higher prevalence of psychological disorders compared with global averages. Reference Khan, Khan, Albobali and Alabdulla1 The escalation beginning in October 2023 occurred within a context of prolonged military violence, displacement and structural instability that has shaped the experiences of Palestinian children for generations. Acknowledging this cumulative and intergenerational dimension is essential to understanding the psychological impact observed. The recent ongoing escalation of violence, including airstrikes and ground incursions, has worsened the mental health crisis among Palestinian children, who face heightened risks of post-traumatic stress disorder (PTSD), depression and anxiety disorders. Reference Khoodoruth, Albobali, Selmi, Ouanes, Abdelkarim and Elhassan2,Reference Shukri, Holmes, Shukri, Shukri and Saada3 Research shows alarmingly high PTSD rates, with studies reporting prevalence as high as 41% among children in Palestine Reference Shukri, Holmes, Shukri, Shukri and Saada3 and severe PTSD symptoms in over half of those exposed to military violence. Reference Qouta, Punamäki and El Sarraj4,Reference Qouta and Odeh5 Differences in genders have been found, with girls showing a higher susceptibility to manifesting PTSD symptoms, particularly when their mothers also exhibit PTSD symptoms. Reference Qouta, Punamäki and El Sarraj4
Systematic reviews have found that armed conflict is consistently associated with high rates of mental disorders among refugees, asylum seekers and populations living in war zones, particularly depression, anxiety and PTSD, with children and adolescents being among the most vulnerable groups. Reference Carpiniello6 Palestinian children have witnessed bombardments, seen mutilated bodies and experienced direct military violence, which has led to severe psychological distress. Reference Thabet, Abdulla, Elhelou and Vostanis7,Reference Dimitry8 Data from systematic reviews also show that up to 75% of children have observed people being killed by rockets and nearly all have experienced home shelling. Reference Dimitry8,Reference Agbaria, Petzold, Deckert, Henschke, Veronese and Dambach9 Reported PTSD prevalence among children and adolescents in Gaza and the West Bank has ranged from 6 to 70%, with an overall pooled estimate of 36%, highlighting the widespread impact of political violence. Reference Agbaria, Petzold, Deckert, Henschke, Veronese and Dambach9 The wide variation in reported prevalence reflects substantial methodological heterogeneity, including differences in sampling strategies, timing of assessment relative to exposure, and measurement instruments. A dramatic escalation in the conflict on 7 October 2023 led to a large-scale humanitarian disaster. More than 62 000 children were reported to have been killed and over 110 000 others injured as of early 2025. 10
The dire need for mental health services in Gaza is obvious, yet the provision of such services is fragmented and poorly funded. Reference Dabbagh, Jaber, Raboczki, Tina and Al-Uzri11 Attacks on healthcare facilities and personnel in Gaza have compromised service delivery and restricted humanitarian access, contributing to the psychological burden among affected populations. 12 To effectively address the psychological needs of Palestinian children, a multipronged approach is needed that can coordinate international efforts to deliver comprehensive, trauma-informed care and prevent long-term consequences. There is a critical need for context-specific understanding, tailored assessment methods and specialised mental health interventions. Qatar launched a humanitarian programme to support Palestinians affected by this conflict. The first group of injured Palestinian children and their families arrived in Doha on 9 December 2023 as part of a support programme to sponsor 3000 orphans and provide medical treatment to 1500 injured individuals. This initiative is a testament to Qatar’s pivotal role in addressing the urgent medical and psychological needs of Palestinian children. Notably, Qatar’s mental health services recently led a similar initiative for the displaced Afghan refugees, which proved highly successful and offered a useful model for the current response. Reference Khan, Khan and Alabdulla13
This paper expounds the efforts of Qatar in response to the current crisis, focusing on the comprehensive support provided to displaced Palestinian children and adolescents. It examines Qatar’s integrated approach, which includes trauma-focused mental health interventions, primary care services and psychosocial support within a broader humanitarian framework. The role of multidisciplinary teams in delivering specialised psychiatric and psychological care is highlighted. The paper discusses Qatar’s commitment to address both acute trauma-related conditions and the ongoing management of pre-existing psychiatric disorders through dedicated mental health clinics. Additionally, it explores ongoing research initiatives at Hamad Medical Corporation’s Child and Adolescent Mental Health Service (CAMHS), which assess elevated symptoms of anxiety, depression and PTSD among the displaced children and adolescents. Since these children and young people were residing in Qatar and not experiencing ongoing exposure to active hostilities at the time of assessment, the use of standardised Western diagnostic frameworks, although necessary for clinical care, may not fully capture the collective and cumulative dimensions of their trauma histories.
Integrated healthcare, accommodation and psychosocial support
Primary care forms an essential part of Qatar’s response for displaced Palestinian families, with free access to general health assessments, immunisation and the management of chronic conditions. The close integration of these services and continued collaboration between the medical and psychiatric teams has allowed effective management of the physical and psychological needs of the affected young people. Several national and international humanitarian organisations work alongside Qatar’s health services, providing medical treatment, essential supplies, financial assistance and broader social support.
Families are accommodated at the Al Thumama Complex in southern Doha, which offers fully furnished apartments, green spaces, recreational areas and children’s play zones, ensuring safety, privacy and stability. Within this setting, children take part in sports activities, art and play therapy, and structured recreational programmes designed to support emotional recovery and restore a sense of normality. In addition, families receive free meals, healthcare and educational support, including school placement and transport for school-age children. Together, the provision of integrated healthcare, safe accommodation, education and psychosocial activities plays a central role in reducing stress, supporting recovery and addressing the wider well-being of the displaced children and their families.
Specialist mental health interventions
Qatar has established specialised psychiatry and psychology clinics to address the mental health needs of individuals affected by conflict, including children, adolescents and adults. These clinics offer trauma-focused interventions, cognitive-behavioural therapy (CBT), play therapy and art therapy for children and young people. The interventions are delivered primarily in individual sessions, with family involvement and group-based sessions provided when appropriate. More specialised interventions such as trauma-focused CBT or eye movement desensitisation and reprocessing (EMDR) were available through referral to the local specialist child and adolescent mental health out-patient service, when clinically indicated. These evidence-based approaches are designed to help individuals process traumatic experiences, develop coping mechanisms and build emotional resilience.
A dedicated mental health clinic was created to look after children and adolescents (aged 3–18 years) from Gaza, Palestine, who were affected by the recent war. This clinic operates within a multidisciplinary framework including a child and adolescent psychiatrist, psychologists, specialist mental health nurses and social workers. Over 1 year, 73 children (39 boys, 34 girls) were referred to the clinic following initial screening by primary care clinicians based at the complex. Of these, 31 (42.5%) presented with war-related physical injuries, including head trauma, limb amputations, burns and other trauma-associated conditions.
Among the children referred to the mental health clinic, nearly two-thirds were living with at least one parent, while the remainder were accompanied by adult first- or second-degree relatives. A very small number had guardians appointed by the state. Referral to specialist services was based on observed psychological distress or other clinical indications, often following initial assessment by the on-site primary care clinicians. Not all children, including orphans residing in the Al Thumama Complex, required specialist mental healthcare.
Psychiatric assessments showed a range of diagnoses: 10 children (13.7%) met criteria for PTSD, 21 (28.8%) exhibited post-traumatic stress features not fulfilling full PTSD criteria, 7 (9.6%) were diagnosed with depressive illness and 3 (4.1%) with anxiety disorders. Additionally, 6 (8.2%) displayed behavioural changes secondary to traumatic brain injury, 3 (4.1%) were diagnosed with attention-deficit hyperactivity disorder, 7 (9.6%) with other behavioural challenges and 1 (1.4%) with an intellectual disability. Only 14 (19.2%) showed no psychiatric illness (Fig. 1). All children and young people received therapeutic interventions, including supportive therapy, CBT, trauma-focused therapy and play therapy, and 17 (23.3%) required adjunctive pharmacotherapy.
Distribution of psychiatric diagnoses among patients (n = 73) presenting to a mental health clinic for displaced children and young people from Gaza over a 1-year period. ADHD, attention-deficit hyperactivity disorder; TBI, traumatic brain injury; PTSD, post-traumatic stress disorder.

Although PTSD is one recognised outcome, the mental health services provided addressed a broad spectrum of trauma-related psychological difficulties, including anxiety, depression, behavioural challenges and emotional distress, reflecting the wider impact of conflict on children’s well-being. The services are designed to address both acute trauma-induced conditions and the ongoing management of pre-existing psychiatric disorders. Displaced individuals, including those with anxiety, depression or PTSD, receive comprehensive care, including medication management and therapeutic interventions.
The programme is integrated into Qatar’s national healthcare system, allowing continuity of care beyond the immediate humanitarian phase. Individualised follow-up plans are developed for children requiring longer-term intervention, and those with ongoing needs can be referred to local child and adolescent mental health services (CAMHS), ensuring sustained support and reducing the risk of abrupt discontinuation.
Ongoing and completed research
A major research project conducted under the auspices of Hamad Medical Corporation’s CAMHS has examined the mental health impact of war and displacement on Palestinian children and adolescents in Qatar. Analyses relating to anxiety and depressive symptoms have been completed and published, demonstrating a substantial mental health burden, with over two-thirds of participants showing clinically significant anxiety symptoms and nearly half meeting thresholds for depressive symptoms. Reference Khoodoruth, Albobali, Selmi, Ouanes, Abdelkarim and Elhassan2 Separation anxiety was particularly prominent, and higher symptom severity was associated with female gender, exposure to death or physical injury, and disrupted caregiving environments.
Analyses focusing on post-traumatic stress symptoms form part of the same study and are currently being prepared for publication. These findings are expected to further inform understanding of trauma-related presentations and service needs within this population. In addition, a related project is underway to support the development of an artificial intelligence (AI)-powered prototype assessment tool for the early identification of elevated symptoms and red flags of PTSD in children and young people aged 8–18 years affected by humanitarian crises. This work aims to support earlier identification and timely intervention for at-risk groups.
Family satisfaction with services
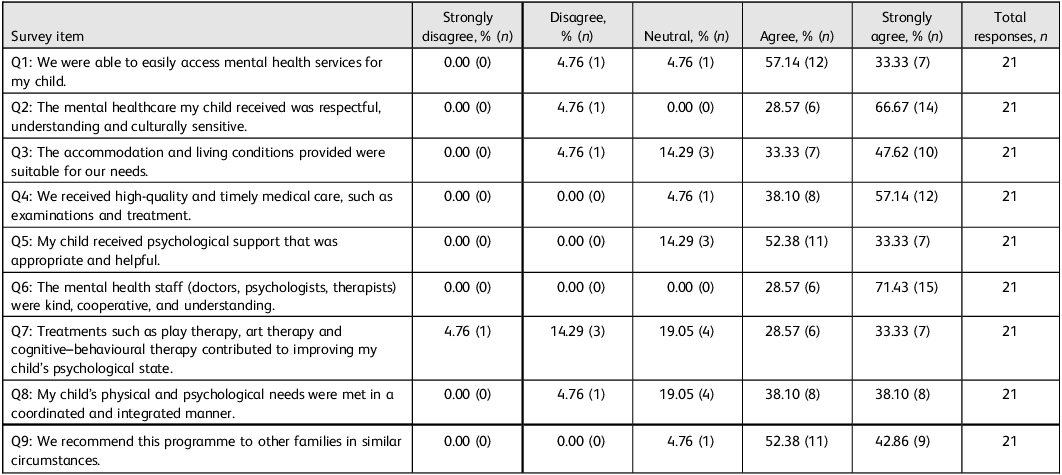
A structured Likert-scale questionnaire, developed locally and translated with forward and backward translation by psychiatrists fluent in English and Arabic, was used to assess family satisfaction with services. Although not formally validated, the survey was piloted to ensure clarity and relevance of items. Twenty-one families whose children received psychological and psychosocial support as part of Qatar’s humanitarian response took part in the survey (Table 1). The findings indicate consistently high satisfaction across all aspects of care. In total, 90.47% of families reported easy access to mental health services, and over 96% felt that the care their child received was respectful, empathetic, culturally appropriate and delivered in a timely and high-quality manner. The accommodation and living conditions, referring to families’ self-reported perceptions of adequacy, privacy and access to basic amenities within modern apartment blocks provided for resettlement, were considered suitable by 80.95% of respondents.
Family satisfaction with Qatar’s humanitarian programme for displaced Palestinian children and young people: survey responses

The feedback on clinical care was particularly strong. All families described the staff – including doctors, psychologists and therapists – as kind, cooperative and deeply understanding. In total, 85.71% reported that the psychological support received was appropriate and helpful, and over 95% stated that they received timely, high-quality medical services and that they would recommend the programme to other families in similar situations. Most families reported that interventions such as play therapy, art therapy and CBT contributed positively to their child’s psychological state, although around 38% of respondents were neutral or disagreed. This may reflect variability in individual responses, differences in symptom severity and the timing of assessment relative to the stage of intervention. Overall, the results of the survey underline the positive impact, accessibility and cultural relevance of the mental health and psychosocial services provided.
Conclusions
-
(a) Qatar’s coordinated humanitarian and mental health programme provides a holistic and coordinated approach by addressing both the physical and mental health needs of the Palestinian children and young people affected by war and displacement.
-
(b) Trauma-focused therapies, play-based interventions and specialist psychiatric care help children and young people to recover from the mental health implications of war.
-
(c) Families need to receive accessible and culturally sensitive care through the integration of physical and mental healthcare, education and social support.
-
(d) Research initiatives, including the development of AI-based tools for early PTSD detection, highlight Qatar’s commitment to improving outcomes for this population.
-
(e) Although the scale of resources available in Qatar may not be universally replicable, the model’s core elements, including integration within the national healthcare system, multidisciplinary collaboration and culturally responsive care, may be adapted to other settings according to local capacity and infrastructure.
Data availability
The data are not publicly available but can be requested from the corresponding author, Y.S.K.
Acknowledgements
Open access was funded by Qatar National Library.
Author contributions
Y.S.K. and Y.A. wrote the initial draft of the paper. A.W.K. suggested significant revisions. O.S. supported with data collection. M.A. provided supervision. All authors reviewed and approved the final draft of the manuscript.
Funding
This work received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.
Ethics approval
This initiative did not involve human subjects research and did not require approval from an institutional review board. Approval was obtained from the chairman of mental health services for the survey reported in Table 1. Departmental approval to publish this description of the clinical and humanitarian initiative along with relevant administrative data was obtained from Mental Health Services, Hamad Medical Corporation.


 Open access
Open access
eLetters
No eLetters have been published for this article.