

Introduction
In this book, many authors have discussed the prevention of sexual harms, and the reduction of risks. However, the stark reality of the field is that many doctors are living with the long-term consequences of sexual trauma. For some, this is not their first exposure to trauma. Many survivors, particularly those who live with intersectional disprivilege, have survived multiple sexual traumas, including childhood trauma.
It is often assumed that healing comes with justice. However, survivors have different goals. Some do seek justice, but others simply want safety, for themselves and their colleagues, while others seek quiet healing. Many try to keep their trauma walled off from their professional lives, despite the fact that the barrier between personal and professional has been shattered by the abuse. Unfortunately, some doctors never seek care at all. Every time we present this sort of work, survivors disclose trauma, sometimes for the first time after decades of silent suffering.
In this chapter, we focus on overcoming barriers to care and healing. Barriers can be conscious, with stigma, shame and fear of retribution preventing the reporting of sexual harassment. Other barriers are unconscious, where survivors bury their trauma and attempt to ‘soldier on’, hiding their trauma from the world and even themselves in a locked box buried deep in their minds.
In Stone’s study, a number of survivors discussed the barriers to reporting. ‘You’re just so tired all of the time, because of this emotional energy that’s expended managing the trauma, that you just almost don’t have the energy to fix your life or change anything’, said one participant. ‘You’ve got to be a survivor, and being a survivor takes a lot of energy, and it means that other things in your life suffer.’ Other participants alluded to unconscious coping mechanisms that impeded their own awareness of trauma. “I had pushed it away’, said one participant, ‘but then I got those feelings again back and remembered what it was like and I clarified in my head that it was something that he did wrong rather than me overreacting.’
The cognitive dissonance we, as authors, often encounter when presenting this work is present in survivors. It seems difficult to believe that sexual harm can happen in the cold, hard light of day in a busy teaching hospital. Survivors can invalidate their own experience in the wake of this confusion. One participant in Stone’s study described this as ‘going into numb mode’. ‘I remember wondering whether his behaviour was normal and if there was something wrong with me’, she said. ‘I had difficulty believing that his behaviour was actually real. Sometimes I felt like I was going mad and this made me feel even more unconfident and uncertain about myself.’
These quotes and others in this book suggest that there are considerable intrapersonal barriers to reporting, that may be overlooked when considering the substantial conscious barriers, such as career threat. In addition, rehabilitation involves re-entering the workforce that was the site of the original trauma. In one of our studies, a participant who returned to work described how bewildering it was to re-enter the hospital. ‘I found myself hugging the walls’, she said, ‘because the floor no longer felt safe.’ Another described the difficulty she experienced overcoming her own silence, finding herself stuttering and unable to express herself, which was immensely frustrating.
In this chapter, we focus on two specific concerns. The first is experiencing and overcoming the dissociative response to trauma. The second is learning to overcome the silencing that occurs in its wake. Both are necessary if a survivor is to heal and reclaim their personal and professional sense of self.
Doctors usually start their long careers steeped in an idealistic view of medicine. Many survivors have idealised their perpetrators, and this deep respect can be manipulated as a form of grooming. In chapter 18, Dr Lee describes this experience. ‘My whole belief system collapsed’, she says in her victim impact statement.
For weeks, I could not comprehend what had happened. I could not understand why my trust was betrayed. I wondered how I could have so stupidly misunderstood the intentions of someone I considered a mentor. I called all other staff specialists in the department by their first name, but I always called the offender Prof because … I respected him so much.
Survivors have been betrayed by their professional ‘family’ and have to reshape their ideas of themselves as people and as doctors. One of the participants in Stone’s study was very clear about the next steps the profession needed to take. ‘If we are going to manage this’, she said, ‘we need a curriculum of recovery.’ This chapter forms part of that curriculum.
Becoming Aware: Overcoming Dissociation to Manage Trauma and Shame
Sexual harassment can be deeply traumatic. However trauma is defined, the core experiences are usually disempowerment and disconnection from others. (Reference Herman1) However, survivors can also experience disempowerment and disconnection from parts of themselves, and can therefore experience difficulty understanding and communicating their needs. This sort of disconnection is profoundly distressing.
When sexual harassment occurs within a relationship of trust, such as the relationship between a senior and junior colleague, both aspects of this definition are important. Disempowerment captures the central feature of helplessness, with one’s usual defences being overwhelmed. It is worsened because there is already an inherent power differential in this relationship. Indeed, the hierarchal nature of medicine emphasises the earlier power dynamics of parent–child and the situational dynamics of doctor–patient.
This is what might be called an oppression trauma, defined by Hardy as the interlocking of socio-political oppression and trauma that is systemic, pervasive and protracted over time. The complex interlocking of intersectionality with female trainees and male consultants, or white consultants and black, indigenous or people of colour (BIPOC) junior doctors suggests systemic oppression plays a part in the trauma. (Reference Hardy2) Trauma within the profession can also be considered betrayal trauma, a concept developed by Freyd. (Reference Freyd3)
In Freyd’s theory, abused children separate the trauma from their consciousness in order to preserve the relationship with the needed caregiver. This may occur during the trauma (i.e. the child does not recognise that his parent is hurting him), after the trauma (i.e. the child is unable to remember what happened during the abuse), or both. This dissociation from the abuse facilitates the child’s survival by helping him remain connected with the important attachment figure.
The model of child sexual abuse is one way of understanding the impact of this particular attachment trauma in the medical arena. The medical profession is like a family, with its own culture, mutual dependence and hierarchies, as well as expectations of behaviour. Professional survival is often linked to the perpetrator holding considerable power, and senior colleagues may be invested with trust, respect, admiration and need by the victim. While differences are, of course, evident for an adult experiencing abuse, it is also important to recognise that vulnerability to this occurring as an adult is enhanced by a history of child sexual abuse. This adds to the complexity as not only might a perpetrator ‘recognise’ the vulnerability and exploit it, the repetition of an attachment abuse will increase the likelihood of serious consequences for the survivor.
Dissociation is a powerful defence employed when fight/flight is not possible, and the parasympathetic activation of the freeze response begins. Ferenczi, (Reference Ferenczi4) in writing about child sexual abuse, describes how the child uses dissociation so that the mind is wiped clean of desires, emotions and thoughts. In doing so, the child can suppress their own needs, and focus on meeting the needs of the aggressor. This allows an attuned compliance, unconsciously attending to what the perpetrator needs as a survival tactic. Junior doctors are already well versed in self-sacrifice, suppressing their own needs in service to the patient and the team. The more professional exploitation is normalised (through inhumane working conditions for instance), the more familiar this form of dissociation becomes.
Dissociation is the escape when there is no escape, and is strongly linked to the freeze response. ‘Freezing’ occurs as the next step on from fight and flight, when helplessness and terror is overwhelming and physiologically the body shuts down. The mind then detaches from what is occurring with the consequence that the experience is compartmentalised, separated off from the rest of the mind in what Stern (Reference Stern5) describes as ‘unformulated experience’. This is experience without words, held in the body in the form of somatic flashbacks, fragmented images and potentially relationship templates.
Dissociation Is Another Form of Silencing, Where Trauma Is Wordless, and so Becomes Unspeakable.
The identification with the aggressor as described by Ferenczi also captures the way in which the victim takes in the imagined guilt and shame of the perpetrator. This process has often already begun in the grooming process leading up to an assault. Nathanson (Reference Nathanson, Stubley and Young6) writes of sexual abuse as a relational trauma which is a form of oppression and tyranny. He suggests that it is at the time of grooming that victims begin to lose their capacity to resist. He says:
It is as if the abuser subtly breaks in, steals the authority to say no and leaves a corrupt presence behind, an entity which would make sure that the door would never be locked again.
It is this corruption that is central to the oppression, stealing away the freedom to say no and to reach out to others, to disclose and to break the silence, asking for help and companionship as an essential step in any struggle for freedom. The victim feels implicated, isolated and alone.
Thus, Herman’s description of disconnection from others in trauma relates to the grooming process, the isolation in the moment of the event and the consequences and repercussions of the assault. Silencing, shame, stigmatisation, guilt and despair separate the victim from the rest of society. This is further compounded by the avoidance that is a part of the post-traumatic response, a shutting down from self and others to avoid re-triggering, dissociation and hyperarousal states.
In these multiple ways the survivor may struggle to speak out, to disclose what has occurred. Caught in their isolation and feelings of guilt and shame, lacking the words to have a narrative, or lacking the memories due to dissociation, frightened by the potential loss of the attachment figure and the consequences this will bring – silencing may take many forms.
Survivors who do manage to disclose are likely to have different needs, but general principles for healing, whatever is offered, apply.
Laub and Auerhahn (Reference Laub and Auerhahn7) suggests that trauma therapy involves the communication of ‘testimony’ to a witness willing ‘to be totally present to the survivor, and to receive as well as experience what he / she wants to transmit’.
Trying to bear what is being communicated, without action or attempts to be rid of it, is the beginnings of containment. Wilfred Bion (Reference Bion8) described this notion in terms of mothers and babies, when in the normal course of development, a baby is filled with the early, powerful anxieties, and employs projective identification to communicate what is unbearable to the mother. It is her role to try to take this in, to think about it and attempt to understand what might be going on in the baby’s mind so that she might relieve him of his distress. Over time this gives the baby the experience of someone who can bear what they feel is unbearable and thus can lessen the need to rid oneself of distress.
Where Freud and Klein made love and hate central to psychic life, Bion adds knowledge, particularly the inability to know. The inability to know results from the failure to have found someone, generally in early life, willing and able to contain unbearable feelings, feelings that cannot be put into words, but have more the quality of fragments of feelings. It is only by encountering another mind willing and able to hold these unbearable pieces of feeling that one can learn to put them together for oneself.
Traumatic experience may be understood as a rupture of the container so that knowledge is attacked, the ability to link associated experiences is lost, and the capacity for thought which allows an experience to be recognised and owned is lost. As Alford (Reference Alford9) describes in the quote above, love wants to know, and hate would break what we know into pieces to save us the horror of knowing. Not knowing empties the world of the connections that give it meaning and life its vitality.
Bion’s model of containment highlights the need for another mind to know, to be open to recognising, feeling and thinking about unbearable experiences. This includes all of the complex emotional responses to what has occurred and the mourning process that is needed to heal. Mourning involves working through sadness, despair, guilt, shame, and rage.
There is a moment in the television adaptation of Margaret Atwood’s The handmaid’s tale that captures a central question for those who have been abused, violated and oppressed by a cruel patriarchal system. June, the main protagonist, asks a group of traumatised women who have been talking about how to find a way forwards after such violence and degradation. She says: ‘Why does healing have to be the only goal? Why can’t we be as furious as we feel? Do we have that right?’
June’s suggestion that survivors may need to feel the fury – to have the right to do so – alongside the healing, brings in a broader question than the therapeutic treatment of traumatised individuals. To feel the rage is to allow this aspect of the necessary grieving that is a part of the healing process, to allow the feelings that were cut off through dissociation when it was too dangerous to feel. It is also empowering, and this is a vital aspect of its function when disempowerment is so central to oppression trauma.
Psychoanalyst Beverley Stoute (Reference Stoute10) describes Black Rage arising out of repeated acts of injustice without opportunities for redress that is at the heart of racism. This form of oppression leads to moral injury – inhumane behaviour experienced as a betrayal of what is right. Stoute suggests that indignant rage – in this case Black Rage – is an appropriate response to such injury, that it is an adaptive mental construct and a powerful and necessary defensive psychic force which serves to preserve dignity and self-worth and mitigate the impact of racial trauma.
This links with the need for justice, acknowledgement of what has happened and reparations. Herman (11) emphasises the necessity of a political movement alongside the practices of studying and treating psychological trauma. She argues that:
advances in the field occur only when they are supported by a political movement powerful enough to legitimate an alliance between investigators and patients and to counteract the ordinary social processes of silencing and denial.
The thesis put forward in Herman’s book, Trauma and recovery (Reference Stoute10) is that the process of healing from trauma is essentially embedded in a wider socio-political framework that must always be taken into account. Within this particular context, a robust process of responding to disclosures and supporting doctors in the process of ensuring safety (for themselves and their careers), healing and justice is vital.
Learning to Speak: Overcoming Silence to Manage Trauma and Shame
The problem of employee silence is widespread in hospital-based health care, (Reference Peadon, Hurley and Hutchinson12) and new professionals, including junior doctors, are especially prone to silence. (Reference Donovan, O’Sullivan, Doyle and Garvey13–14) In management and organisational research, employee silence occurs when employees individually or collectively ‘withhold ideas, information about problems, or opinions on work-related issues’ including those where they ‘do not speak up about errors, unfair treatment, or behaviours that violate personal, moral, or legal standards’. (Reference Morrison15, p81)
Junior doctors are inducted into the medical profession via formal and hidden curricula imparted during medical education and training. (16) The implicit messages they receive communicate their place in the medical professional hierarchy and let them know they are to be ‘seen and not heard’ and that the views and preferences of senior colleagues are to be privileged. (Reference Lister, Spaeth, Edwards, Martin and Ashkanasy17) They also experience and witness negative behaviours such as incivility, bullying, harassment and discrimination (Reference Llewellyn, Karageorge, Nash, Li and Neuen18) that are typically perpetrated by doctors higher in the hierarchy (Reference Talash, Corfield, Latcham, Lavelle, Williams and Machin19) and reinforce the silent status quo. (Reference Rai and Agarwal20)
The messages junior doctors receive are effective to the extent they frequently fail to speak up for patient safety and care, (Reference Brennan and Davidson21; Reference Dendle, Paul, Scott, Gillespie, Kotsanas and Stuart22) subverting their professional commitment to do no harm (Reference Loewenbrück, Wach, Müller, Youngner and Burant23) and the organisational obligation to report adverse events and errors. (24) Those who do voice concerns can become victims of symbolic violence, (Reference Bourdieu and Wacquant25) a type of reputational harm that ensures they are effectively blacklisted, unable to secure ongoing employment or progress their training, in which they have invested significant time and resources.
In an environment where speaking up about professionally and organisationally mandated issues can lead to bullying and harassment as well as tarnished reputations and stalled careers, junior doctors are even less likely to voice concerns related to their working conditions and wellbeing. Issues related to hours, pay, rosters, leave and fatigue are therefore also left unsaid, (Reference Creese, Byrne, Matthews, McDermott, Conway and Humphries26) and those related to abuse are even harder, if not impossible, to raise.
In the military, female soldiers who were victims of workplace rape lapsed into two forms of employee silence, acquiescent and quiescent silence. (Reference Pinder and Harlos27) The former is characterised by a sense of futility (speaking up is useless and nothing will change if I do). The latter is associated with suffering in silence – with hopelessness and a lack of self-efficacy to voice that makes speaking up at any point unlikely. Acquiescent silence, however, holds the promise of voice: some victims spoke up about their experiences years later, when similar reports surfaced in the public domain.
The problem of employee silence is, however, a compounding one, and left unchecked it leads to organisational silence, defined as the group-level belief that it is not safe to speak up or it is futile to do so. (Reference Morrison and Milliken28) This creates widespread ‘climates of silence’ in which silence at work becomes the self-perpetuating norm (Reference Morrison and Milliken28, p. 708).
Breaking the Vicious Circle of Silence: Restoring Agency and Confidence to Voice
Much of the literature on employee silence focuses on addressing organisational and structural barriers to voice, and in health care research professional factors have also been identified as significant. Solutions include improving mechanisms for voice, for example via protected reporting programmes such as the Freedom to Speak Up Guardians initiative in the NHS in the UK; (Reference Hughes29) programmes that teach health care professionals how to speak up (see Reference Jones, Blake, Adams, Kelly, Mannion and Maben30 for a review); and attempts to improve organisational or professional culture, the Royal Australasian College of Surgeons’ Operating with Respect programme (31) being one example of professional accountability training designed to reduce bullying and harassment.
Little attention has been paid, however, to ways employees might be supported to address the problem of silence themselves – an oversight that perpetuates the kind of individual inertia Pinder and Harlos (Reference Pinder and Harlos27) identified in their study on silent soldiers. Yet their conceptualisation of acquiescent silence hints at two ways junior doctors, who also work in highly stratified and oppressive environments, might progress from silence to voice.
That victims spoke up after someone else had suggests collective voice could be one way for junior doctors to break their silences. Associated with unions and other forms of employee representation, (32) collective voice has recently been exercised by junior doctors in several jurisdictions in Australia on the topic of systemic unrostered and unpaid overtime. The doctors joined forces in the form of class actions against their hospital employers and the first case was recently found in their favour. (Reference Yu, Jeuniewic and Brook33) Finding ways to connect junior doctors who are victims of work-related sexual assault, via class actions or other means, could provide a safer way to speak up.
That some of the soldiers in Pinder and Harlos’ (2001) study (Reference Pinder and Harlos27) eventually broke their silence, despite long-term fear and inertia, suggests interventions that enhance individual agency could also be useful, workplace coaching being one example. Coaching is an agentic activity that empowers individuals in several ways. (Reference Jones, Woods and Guillaume34) First, it provides a space where they are listened to and heard. Second, it uses questions that prompt people to find solutions to work-life problems. Third, it uses goal setting to enable people to develop accountability and track their performance.
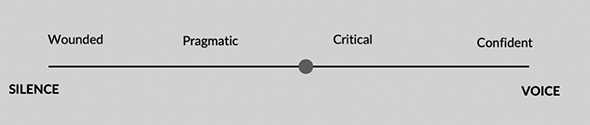
Research on junior doctor silence, conducted by one of the authors of this chapter, suggests the movement from silence to voice occurs on a spectrum as individuals develop agency, and that the journey takes place in stages (Figure 35.1). In the first or wounded stage, junior doctors are at the silent end of the spectrum, overwhelmed by their circumstances and hurt by their experiences to the extent voice (on any topic) is impossible. In the second, pragmatic stage, junior doctors are aware of their plight but continue to believe voice is not welcome. Highly functional, they accept their situation with stoicism. In the third stage, junior doctors become critical – and cynical – about their situation. Anger can propel them to speak up about the things that matter most to their wellbeing, such as the inability to obtain parental leave. In the final, confident stage, junior doctors are more likely to raise concerns. They have learnt how to navigate the complex systems in which they are immersed, established allies who can support their efforts to raise concerns and have greater self-efficacy to voice.
The transition from silence to voice.

This trajectory supports the notion that increasing junior doctors’ sense of personal and professional agency is required if they are to break free of their deeply held beliefs that speaking up – be it about sexual harassment, other working conditions concerns or patient safety and care – is neither permitted nor welcomed. Coaching encourages individuals to become active leaders of their own lives rather than the passive recipients of life. Focused workplace coaching that aims to develop communication skills could offer junior doctors a path to voice. As the ability to speak up has also been linked with increased employee wellbeing, (Reference Brooks, Wilkinson, Brough, Gardiner and Daniels36) workplace coaching could also be a path to recovery.
Designing a Curriculum that Incorporates the Tools for Recovery
We are no longer in an era where doctors are expected to be relentlessly objective. The symbolic separation of doctors from their patients, in the form of white coats, special obscure language and other symbols of power, is breaking down. It has been interesting to watch doctors return to special clothing in the form of scrubs during the pandemic, perhaps as a way to re-establish appropriate infection control and symbolic therapeutic distance.
Doctors are taught to relentlessly suppress their personal and emotional needs. Medicine demands sacrifice. It chooses the elite thinkers, who dedicate their early lives in achieving high academic goals. It then expects over a decade of commitment to higher learning, and this includes lengthy hours, including hours that are never captured in a timesheet. In addition, doctors in training still tolerate and may expect ‘beneficial mistreatment’, the years of harsh expectations and feedback which they believe will make them better doctors.
Medical training and practice may come at considerable expense. Doctors have high rates of mental illness, alcohol and other substance misuse and relationship breakdowns. Suicide rates are high. Doctors live with high and often unachievable personal expectations. At this time in history, they also live with growing occupational violence, in workplaces that are becoming psychologically unsafe.
In order to survive the brutality of medicine, the painful procedures that must be carried out on vulnerable patients like children, the bad news that must be delivered, and the witnessing of appalling trauma that must be endured, doctors need to learn to moderate their empathy. In difficult consultations, and during difficult procedures, doctors will often revert to objective, theory-based thinking, partly to protect themselves from the trauma, and partly to ensure the patient gets what they need without the doctor being distracted by their own distress. It is therefore understandable that doctors may not have the language, experience or frameworks to manage their own trauma. Although there have been moves to destigmatise mental illness in medicine, to encourage the sharing of feelings, and to provide non-specific support mechanisms for doctors, often these are couched in terms that imply the doctor is responsible for managing their own distress. It is even a requirement in some codes of conduct that ‘doctors maintain their own wellbeing’. Some now describe this as ‘wellbeing washing’, the illusion of care that is a light dressing over a deep wound. One cartoonist described this well, when talking about the NHS. In response to a request for more support for doctors, the manager responds, ‘we’ve given them a room to cry in, what more do they want?’
In this environment, doctors who experience their own trauma may lack the words, let alone the theories, to understand what has happened to them, and to communicate it to others. Their defences have been shattered, the personal and the professional selves are no longer walled off, and underneath their thick layer of protective objectivity, they may lack the capacity to make sense of the experience. The injunction ‘it’s good to talk about things’ doesn’t help if there are no words to describe the feelings experienced, or no-one who the survivor feels is safe to hear the message.
As educators, colleagues, therapists, leaders and regulators, we need to consider how we can use the frameworks doctors already have in place to manage this wordless trauma. One way, of course, it is to teach trauma theory and trauma management early in training. Doctors revert to theory if a situation is distressing. We need to supply theory they can use. Psychological trauma should also be debriefed in a formal, objective way, perhaps with structures like root cause analysis that are already well known, so doctors have appropriate scaffolding to discuss difficult challenges. When trauma occurs, it is naïve to assume that all doctors need is kindness, compassion and non-specific support. Although these are helpful in themselves, trauma-based therapy is a difficult skill that requires expert practitioners. Assuming this form of trauma can always be managed with non-specific kindness and empathy underestimates the impact this form of trauma can have on a survivor. Doctors deserve well-trained and capable trauma-based practitioners who can help them name their experience, understand it and find ways to move beyond it to return to practice if they choose to do so.
Conclusion
While it is much more comfortable to talk about the primary prevention of sexual trauma in the medical profession, it is more realistic to accept that there are many survivors in the medical community who are still affected by their own experience. If we are to relieve their suffering, and prevent others from the silent endurance of long-term psychological harm, it is important to find ways to help survivors speak. In order to make that possible, they need the words, the narratives and the expert safe spaces to facilitate healing and rehabilitate their personal and professional sense of self.

 Open access
Open access