


The postpartum period is associated with an increased risk of onset or relapse of psychiatric disorders. Reference Meltzer-Brody, Howard, Bergink, Vigod, Jones and Munk-Olsen1 The most common conditions are depressive and anxiety disorders; however, rare and severe conditions such as bipolar disorder and postpartum psychosis can also occur and recur. Reference Meltzer-Brody, Howard, Bergink, Vigod, Jones and Munk-Olsen1 Both hormonal changes during the transition from pregnancy to postpartum and psychological stressors from giving birth and infant care may play distinct roles in the onset and recurrence during this vulnerable time. Reference Batt, Duffy, Novick, Metcalf and Epperson2,Reference Egsgaard, Bliddal, Lund, Vigod and Munk-Olsen3 Treatment for postpartum psychiatric disorders may include non-pharmacological treatment (e.g. psychological therapies) and, in more severe cases, the use of medication or emergency and psychiatric hospital services. Reference Dennis, Singla, Brown, Savel, Clark and Grigoriadis4
Most research into postpartum psychiatric disorders has focused on postpartum depression (PPD), with an estimated prevalence of 17%. Reference Shorey, Chee, Ng, Chan, Tam and Chong5 Given the complex interplay among biopsychosocial factors, PPD has been suggested to be a heterogeneous disorder with diverse symptom presentation. Reference Putnam, Wilcox, Robertson-Blackmore, Sharkey, Bergink and Munk-Olsen6–Reference Waqas, Nadeem and Rahman8 Some studies have used responses from the Edinburgh Postnatal Depression Scale (EPDS), an internationally validated screening tool, to identify depressive and anxiety symptoms in the perinatal period. These studies found subtypes of PPD that vary in both symptom severity (e.g. moderate or severe) and symptom profile (e.g. anxious, anhedonic or core depressive features Reference Putnam, Wilcox, Robertson-Blackmore, Sharkey, Bergink and Munk-Olsen6,7,Reference Collaton, Dennis, Taylor, Grigoriadis, Oberlander and Frey9,Reference Sun, Cao, Li, Zhang, Wang and Bai10 ). However, EPDS also includes symptoms not specific to depression alone but which could be experienced in a wider range of psychiatric disorders, including anxiety, post-traumatic stress disorder, bipolar disorder or even psychosis. Reference Petrozzi and Gagliardi11 Additionally, it remains unclear whether different subtypes of postpartum depressive and anxiety symptoms captured by EPDS are associated with subsequent psychiatric healthcare use, including specific psychiatric diagnoses, out-patient specialty care, medication use, emergency department visits or hospital admissions. A more nuanced understanding of this area could support a more personalised approach to early identification, tailored treatment and preventive strategies for adverse outcomes.
Objectives
To identify subtypes of postpartum depressive symptoms using EPDS in a population-level cohort of women routinely screened postpartum, and to investigate how subtypes of symptoms relate to subsequent psychiatric healthcare use over the first year postpartum.
Method
We conducted a cohort study linking Danish nationwide health registers with EPDS symptom scores in the HOPE cohort. Reference Zacher Kjeldsen, Mægbæk, Liu, Madsen, Bliddal and Egsgaard12 We utilised latent class analysis (LCA) to identify subtypes of depressive symptoms on EPDS and investigated the association between symptom subtypes and subsequent psychiatric healthcare utilisation 1 year postpartum.
Data sources
The HOPE cohort is a Danish nationwide cohort containing records of EPDS scores in 142 795 postpartum women (defined as all individuals who have given birth regardless of gender identity) following 170 218 childbirths. Reference Zacher Kjeldsen, Mægbæk, Liu, Madsen, Bliddal and Egsgaard12 In Denmark, new parents are offered routine visits by healthcare nurses at approximately 2 months postpartum, where EPDS is used to screen for PPD. The HOPE cohort was established based on records collected from 67 of 98 Danish municipalities between January 2015 and December 2021. The cohort has been evaluated for selection bias and is representative of the Danish population of birthing women. Reference Zacher Kjeldsen, Mægbæk, Liu, Madsen, Bliddal and Egsgaard12
The unique personal identifier assigned to all individuals living in Denmark linked the HOPE cohort to Danish nationwide health registers. Reference Schmidt and Pedersen13 The Danish Medical Birth Register (Birth Register) holds information on all children and their parents, including pregnancy and birth outcomes, since 1973. Reference Bliddal, Broe, Pottegård, Olsen and Langhoff-Roos14 The Danish National Patient Register (Patient Register) holds information on all in- and out-patient hospital contacts and diagnoses, using the ICD-10 classification system, since 1995. Reference Schmidt, Schmidt, Sandegaard, Ehrenstein and Pedersen15 The Danish National Prescription Register (Prescription Register) contains all prescriptions redeemed at Danish pharmacies since 1995. Drugs in the register are classified according to the World Health Organization Anatomical Therapeutic Chemical (ATC) Classification. Reference Pottegård, Schmidt, Wallach-Kildemoes, Sørensen, Hallas and Schmidt16 Statistics Denmark includes sociodemographic information including education, income, cohabitation status and country of origin.
Study population
The study population comprised all women in the HOPE cohort who gave birth between 1 January 2015 and 31 December 2021, and who underwent EPDS screening between 1 and 3 months postpartum. We excluded individuals undergoing psychiatric treatment, defined by either registered psychiatric healthcare use (hospital contact with ICD-10 F00–99) or a redeemed psychotropic prescription (ATC code N05-6) between childbirth and the time of EPDS screening. This was done because women already receiving treatment are not the target group for identification and intervention, and their symptoms could have been mitigated or resolved at the time of measurement.
Postpartum depressive symptoms
EPDS is a self-report scale developed to identify depressive symptoms in the perinatal period. Importantly, EPDS is a screening instrument designed to identify depressive symptoms and should be considered distinct from a clinical diagnosis of depressive disorder. Although originally intended for capturing depression, the tool includes ten items covering a range of psychiatric symptoms, including feelings of sadness, self-blame, feelings of overwhelm, anxiety and thoughts of self-harm. Reference Cox, Holden and Sagovsky17,Reference Smith-Nielsen, Matthey, Lange and Væver18 Each EPDS item is scored between 0 and 3, with a higher score indicating greater severity and a total score ranging from 0 to 30.
Psychiatric healthcare
The primary outcome was any psychiatric healthcare utilisation, defined as either an out-patient, emergency department or in-patient hospital contact in specialised psychiatric care with a registered psychiatric diagnosis (ICD-10 F00–99), or a redeemed prescription for psychotropic medication (ATC code N05-6). Secondary outcomes were prescriptions and type of hospital contact alone, and by the registered diagnosis (regardless of the type of contact): depression (ICD-10 F32–3), anxiety (ICD-10 F40–2), bipolar disorders (ICD-10 F30–1), substance use disorders (ICD-10 F10–19) and psychotic disorders (ICD-10 F20–9).
Additional study variables
We obtained information on the following variables identified at the time of childbirth: maternal age, parity, multiple births, preterm birth (before 37 weeks of pregnancy), Caesarean section (ICD-10 O82, O84.2, O84.3, O84.3D), pre-eclampsia/eclampsia (ICD-10 O14, O11, O15), gestational diabetes (ICD-10 O24.4), hyperemesis gravidarum (ICD-10 O21), postpartum haemorrhage >500 mL (ICD-10 O72.0) and neonatal intensive care admissions, all identified from the Birth Register. From the Patient Register we obtained information on psychiatric history, defined as any psychiatric diagnosis (ICD-10 F00–99) prior to childbirth. We received information on educational level from the highest achieved education (primary, high school or vocational, short- or medium-cycle and long-cycle or PhD), and from household income divided into quintiles in the year prior to childbirth. We defined cohabitation as living with a partner in the year preceding childbirth, and country of origin as either Danish or non-Danish.
Statistical analysis
LCA
We used LCA to identify subtypes of EPDS symptoms. LCA is a modelling approach that assumes unobserved (latent) subgroups within an observed distribution of variables. Reference Sinha, Calfee and Delucchi19 LCA uses probabilistic modelling to estimate the likelihood of each individual belonging to a class, which we used to define distinct subgroups of symptoms on EPDS in the cohort. For LCA we included only women with an EPDS score of 11 or higher, the clinical cut-off score used in Denmark to identify PPD, Reference Smith-Nielsen, Matthey, Lange and Væver18 and also included women with an EPDS score <11 for comparison. We used all ten EPDS items as ordinal class-defining variables, and evaluated models with varying class numbers using the Bayesian information criterion and Akaike’s information criterion. Reference Nylund and Asparouhov20 Based on evaluation criteria and the clinical interpretability of classes, we selected the optimal class solution. Individuals were assigned to classes using modal assignment, and descriptive characteristics were reported for each subgroup. Following selection of the optimal class solution, class separation was assessed using entropy (values >0.8 indicating good separation), average posterior probability (avPP; values >0.7 indicating adequate separation) and odds of correct classification (OCC; values >5 indicating good separation). Reference Nylund-Gibson and Choi21,Reference Masyn and Little22
Subsequent psychiatric healthcare
Using symptom subgroups identified from LCA and the maternal background population with an EPDS score of <11 as exposure groups, we investigated the association with subsequent psychiatric healthcare as defined above. To better reflect differences between latent classes, we considered the mildest EPDS symptom subgroup as the reference and, for all outcomes, we applied a parametric time-to-event analysis based on a Poisson regression model. Reference Carstensen23 Individuals were followed from EPDS measurement until either the outcome of interest, death, emigration or 1 year postpartum, whichever occurred first. Time since childbirth was the underlying timescale, which was divided into 30-day intervals and modelled using restricted cubic splines with 4 knots. We modelled both unadjusted and adjusted analyses, with the latter serving as the primary and the former as supplementary. Adjusted models included age, parity, psychiatric history, country of origin, educational level and income level. Standardised rates were obtained from the marginal distribution (i.e. mean values) of these covariates in the LCA population. Based on these, we estimated cumulative risk ratios at 1 year (360 days) postpartum. For supplementary analyses, we repeated the analysis of the primary outcome stratified by psychiatric history (none or any).
We used the Bolck, Croon and Hagenaars method to account for the uncertainty of latent class membership, Reference Nylund-Gibson, Grimm and Masyn24,Reference Bakk, Tekle and Vermunt25 and clustered all analyses to account for women with more than one childbirth during the study period. Analyses were conducted using R version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria; https://www.r-project.org/) on Windows, including the packages tidySEM for LCA modelling Reference Van Lissa, Garnier-Villarreal and Anadria26 and epi for time-to-event modelling. Reference Carstensen, Plummer, Laara and Hills27
Ethical standards
This study was approved by the Danish Data Protection Agency (Aarhus University, journal no. 2016-051-000001, serial no. 2304). According to Danish law, register-based studies are exempt from requiring ethical approval or informed consent. The Danish Patient Safety Authority approved the use of EPDS data from health records, and data linkage with national registers was permitted by the Danish Data Protection Agency. A study protocol was preregistered at https://osf.io/536e7.
Results
Study population and LCA
After excluding 4566 women in ongoing psychiatric treatment between childbirth and the time of EPDS screening, the study population consisted of 162 079 women with an EPDS screening between 1 and 3 months postpartum (Supplementary Table 1 and Supplementary Fig. 1 available at https://doi.org/10.1192/bjp.2026.10614). Among these, 11 847 (7.3%) had an EPDS score ≥11 and were included in LCA.
Based on the observed EPDS scores alone, women tended to score highest on Self-blame and Anxiety (items 3–4) and lowest on Self-harm (item 1; Fig. 1(a)). We tested solutions ranging from one to seven classes, and found that a five-class solution was the most optimal based on a combination of fit indices and interpretability of classes (Supplementary Table 2 and Supplementary Fig. 2). Although improvements in fit indices from the four- to the five-class solution were modest, the latter was preferred due to greater clinical interpretability. The five-class solution had an avPP ranging from 0.69 to 0.84 across classes, an entropy of 0.61 and OCC ranging from 7.13 to 29.54 (Supplementary Tables 2 and 3).
Observed proportion (a) and probability (b)–(f) of responses to the Edinburgh Postnatal Depression Scale (EPDS) within each latent class.

The latent classes formed five postpartum depressive subtypes: the Mild-depressive subtype (n = 2686; 23%, mean EPDS = 11.9) had the lowest mean score, with no particularly high scores on any specific EPDS items. The Moderate-anxious subtype (n = 2004; 17%, mean EPDS = 12.6) scored particularly high on Anxiety and Panic (items 4–5), the Moderate-depressive subtype (n = 2183; 18%, mean EPDS = 13.0) scored high on Self-blame (item 3) and the Moderate-overwhelmed subtype (n = 3672; 31%, mean EPDS = 14.2) scored higher on being Overwhelmed and also on anhedonia symptoms (items 6 and 1–2)). Finally, a Severe-depressive subtype (n = 1302; 11%, mean EPDS = 19.3) had a high probability of endorsing symptoms across all EPDS items (Fig. 1(b–f)).
Compared with the background population with an EPDS score <11, women included in LCA were less likely to be cohabiting with a partner, to have a higher education, to have a higher income level and to be of Danish origin, and were more likely to have a psychiatric history prior to childbirth and have a pregnancy or obstetrical complication (Table 1). Among the five depressive subtypes, there was a tendency for increased social disadvantage with higher severity of depressive symptoms, except for the Moderate-overwhelmed subtype, where education and income levels resembled the background population. Psychiatric history was highly prevalent among all subgroups, ranging from 41% in the Mild-depressive subtype to 49% in the Severe-depressive (Table 1).
Descriptive characteristics by postpartum psychiatric symptom subtype and background maternal population

IQR, interquartile range; PhD, doctor of philosophy.
a. Background population representing women with an Edinburgh Postnatal Depression Scale (EPDS) score < 11.
Postpartum psychiatric healthcare
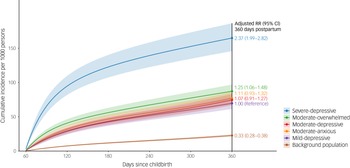
The standardised cumulative incidence rate (CIR) per 1000 persons at 360 days of any psychiatric diagnosis or psychotropic prescription was 69.6 (95% CI, 61.4–79.0) for the Mild-depressive subtype (reference group; Fig. 2 and Supplementary Table 4). Incidence was similar in the subtypes Moderate-anxious (CIR 77.1, 95% CI, 68.5–86.7; adjusted risk ratio (aRR) 1.11, 95% CI, 0.93–1.32) and Moderate-depressive (CIR 74.6, 95% CI, 66.7–83.4; aRR 1.07, 95% CI, 0.91–1.27); however, it was higher in the subtypes Moderate-overwhelmed (CIR 87.3, 95% CI, 78.5–97.0; aRR 1.25, 95% CI, 1.06–1.48) and Severe-depressive (CIR 164.8, 95% CI, 145.7–186.5; aRR 2.37, 95% CI, 1.99–2.82). Incidence of the primary outcome was significantly lower in the background population compared with the reference group (CIR 22.7, 95% CI, 21.0–24.5; aRR 0.33, 95% CI, 0.28–0.38).
Standardised cumulative incidence and adjusted risk ratio (RR) 360 days postpartum of any first psychiatric hospital contact or psychotropic medication, by symptom subtype. Standardised rates were based on the marginal distribution (i.e. mean values) of the latent class study population for included covariates in the adjusted analysis. Values include primiparity: 0.55; age: 30 years; psychiatric history: 0.45; Danish ethnicity: 0.84; third income quintile; and ‘short- or medium cycle’ educational level. Overall, 3734 individuals (2.3%) with missing information were excluded from adjusted analyses.

Secondary outcomes followed a similar pattern to the main analysis (Fig. 3 and Supplementary Table 4). Cumulative incidence rates were substantially higher for any redeemed psychotropic medication than for any psychiatric diagnosis. Regarding the type of hospital contact, CIR was highest for out-patient psychiatric hospital contacts and lowest for psychiatric emergency department visits (Fig. 3 and Supplementary Table 4). Similar to the main analysis, aRRs were consistently highest for the Severe-depressive subtype and slightly elevated or non-different for the other subtypes (Fig. 3 and Supplementary Table 4). Estimation of bipolar disorder, substance use disorder and psychotic disorder was not feasible due to too few cases in each subgroup (Supplementary Table 5).
Standardised cumulative incidence and adjusted risk ratio (RR) 360 days postpartum of various psychiatric outcomes, by symptom subtype. Standardised rates were based on the marginal distribution (i.e. mean values) of the latent class study population for included covariates in the adjusted analysis. Values include primiparity: 0.55; age: 30 years; psychiatric history: 0.45; Danish ethnicity: 0.84; third income quintile; and ‘short- or medium cycle’ educational level. Overall, 3734 individuals (2.3%) with missing information were excluded from adjusted analyses. Note: the y axis ranges up to 150 for panel (a), to 100 for panels (b) and (c) and to 60 for panels (d)–(g).

Analyses stratified by psychiatric history showed overall higher CIRs among women with a psychiatric history than among those with no psychiatric history, but risk ratios between latent classes were more elevated among women with no psychiatric history (Supplementary Figs 3 and 4). Unadjusted CIRs and risk ratios were similar to the adjusted analyses (Supplementary Figs 5 and 6).
Discussion
Main findings
In a population-based sample of 11 847 new mothers with an EPDS score ≥11 postpartum, we identified 5 subtypes of postpartum depressive symptoms reflecting variations in severity and nature of symptom presentation. Psychiatric healthcare utilisation in the first year postpartum was 3 to 8 times higher in these groups than in a background female population with EPDS <11. We observed substantial variability in subsequent healthcare utilisation by subtype, with an increased risk of any utilisation associated with symptom severity. Additionally, within the moderate-severity groups, utilisation was partially related to the nature of the symptoms. Specifically, the subtypes Moderate-overwhelmed and Severe-depressive had a significantly greater incidence of psychiatric healthcare utilisation than the Mild-depressive subtype. Whereas absolute rates varied by type of utilisation (e.g. psychiatric diagnosis was much more common than psychiatric hospitalisation), relative measures were generally consistent with those of the main analysis.
Strengths and limitations
A key strength of this study is the nationally representative HOPE cohort, which minimises selection bias and includes the most extensive collection of EPDS screening records to date. Reference Zacher Kjeldsen, Mægbæk, Liu, Madsen, Bliddal and Egsgaard12 Leveraging Danish nationwide health registers allowed linkage to psychiatric contacts and psychotropic medication use with high information validity, providing a unique potential to combine symptom scores with subsequent psychiatric treatment. Furthermore, we employed advanced methodologies in LCA, including ordinal treatment of EPDS items and the incorporation of class assignment uncertainty when modelling subsequent outcomes. Using parametric models with splines enabled the flexible estimation of rates, allowing us to report both absolute and relative estimates.
The following limitations should be acknowledged. First, LCA assumes that observed data reflect distinct latent subgroups. Although avPPs were acceptable (range 0.69–0.84) and OCCs were good (all >5), entropy was moderate (0.61), suggesting that this may have been only partially fulfilled; this indicates only moderate separation between classes and suggests that delineation of the population into distinct symptom subtypes was only moderately well defined. Similar levels of class separation were observed across alternative class solutions.
Second, we defined psychiatric healthcare based on specialised psychiatric hospital contacts and psychotropic medication, and had no information on behavioural therapies in municipality-based or primary care. Therefore, our findings reflect only healthcare involving more severe intervention. Additionally, it should be noted that EPDS is a screening tool designed to capture depressive symptoms rather than being a diagnostic instrument, and therefore it does not establish a clinical diagnosis of depressive disorder according to standardised diagnostic criteria. A positive result (EPDS ≥11) indicates the need for careful clinical assessment and appropriate treatment and follow-up accordingly based on clinical diagnosis. In particular, the assessment should include consideration of differential diagnoses, including bipolar disorder, because elevated EPDS scores may reflect a depressive episode occurring in the context of bipolar disorder Reference Munk-Olsen, Laursen, Meltzer-Brody, Mortensen and Jones28 or other psychiatric conditions, including trauma-related comorbidity. Third, although we adjusted for several potential confounders, information on factors such as social support was not available and unmeasured confounding cannot be excluded. Finally, generalisability may be limited, because the study was conducted in an ethnically homogenous population within a universal healthcare system with routine postpartum screenings, and findings may not translate to more diverse populations in healthcare settings without systematic screening or comparable access to care.
Comparison with previous studies
We are the first to link subtypes of postpartum depressive symptoms with subsequent healthcare utilisation, although subtypes have been described previously. As with our study, Putnam et al used EPDS scores and LCA modelling to identify five clinical subtypes reflecting variations in symptom severity (moderate and severe) and nature (anhedonia and anxiety). Reference Putnam, Wilcox, Robertson-Blackmore, Sharkey, Bergink and Munk-Olsen6 However, although we included EPDS items as ordinal factors, Putnam et al treated EPDS items as categorical, thereby limiting sensitivity to symptom intensity. Other studies have identified symptom subtypes using screening tools for depression outside the perinatal period, and found subtypes related to physiosomatic symptoms (e.g. sleep and appetite disturbances and fatigue), but also including mood and anhedonia. Reference Sun, Cao, Li, Zhang, Wang and Bai10 However, using a symptom scale not adapted to the postpartum period can obscure subtypes because physiosomatic symptoms may overlap with the natural consequences of parenthood (e.g. poor sleep). Overall, our findings further support the existence of PPD subtypes, including anxious and depressive, but also highlight a distinct ‘overwhelmed’ subtype not previously described.
Interpretation
We found that women with EPDS scores ≥11 had an increased risk for all adverse outcomes examined compared with a background maternal population. This included an elevated risk of severe consequences, such as psychiatric hospitalisation, across all subgroups. Although most women did not experience severe outcomes, our findings underscore the importance of clinical attention, even for those with milder postpartum symptoms.
We observed a clear dose–response relationship between subtypes and their overall symptom severity. In particular, women in the Severe-depressive subgroup were at substantially higher risk, both in relative and absolute terms, underscoring the importance of early identification and intervention for this group. The risk of psychiatric healthcare utilisation was determined primarily by symptom severity, and only to some extent by the specific nature of symptoms. However, we found indications of differing risk profiles among subtypes. Whereas most subtypes had higher levels of social disadvantage, the Moderate-overwhelmed group had sociodemographic characteristics similar to the background population and had a lower proportion of psychiatric history compared with the other moderate subtypes. This suggests that symptoms in this group, particularly those characterised by feelings of being overwhelmed, may have arisen more unexpectedly, warranting further consideration. Additionally, previous studies have reported that postpartum symptom profiles characterised by anxiety may show greater persistence over time, supporting the clinical relevance of distinguishing symptom profiles beyond overall severity. Reference van der Waerden, Galéra, Saurel-Cubizolles, Sutter-Dallay and Melchior29,Reference Sutter-Dallay, Giaconne-Marcesche, Glatigny-Dallay and Verdoux30 Due to insufficient data size, we were unable to estimate the rate and risk ratios for more severe psychiatric diagnoses (e.g. bipolar and psychotic disorders). This could reflect the fact that the most severe psychiatric disorders manifested before the time of screening, as also evident from diagnoses in the excluded population (Supplementary Table 5).
In conclusion, this population-based study identified five distinct subtypes of postpartum depressive symptoms based on EPDS screenings. All subtypes were associated with a substantially higher risk of subsequent psychiatric healthcare utilisation, ranging from both out-patient hospital contacts and prescription use to in-patient hospitalisation, compared with mothers with lower symptom scores, with the risk increasing by symptom severity. These findings highlight the importance of systematic screening and attention to even mild postpartum symptoms to support early intervention and potentially prevent more severe psychiatric morbidity.
Supplementary material
The supplementary material is available online at https://doi.org/10.1192/bjp.2026.10614
Data availability
This study is based on individual-level register data, which are protected under Danish law and cannot be shared according to Danish legislation.
Author contributions
Conceptualisation: S.E., S.N.V., T.M.-O. Formal analysis: S.E. Funding acquisition: S.E., T.M.-O. Methodology: S.E., S.N.V., T.M.-O., L.C.B., H.K.B., X.L. Project administration: S.E. Software: S.E. Supervision: S.N.V., T.M.-O., M.B., X.L. Validation: S.E., X.L. Visualisation: S.E. Writing – original draft: S.E., S.N.V., T.M.-O. Writing – review and editing: S.E., S.N.V., L.C.B., M.B., H.K.B., C.-L.D., M.-M.Z.K., X.L., T.M.-O.
Funding
S.E., T.M.-O. and M.B. are funded by The Novo Nordisk Foundation (grant no. NNF21OC0072397). S.E. is also financed by The Psychiatric Research Fund in the Region of Southern Denmark (grant no. A5752) and The Region of Southern Denmark (grant no. A1784).
Declaration of interest
T.M.-O. has received a speaker honorarium from Lundbeck A/S. Declaration of interest for remaining authors: none.






 Open access
Open access
eLetters
No eLetters have been published for this article.