


Introduction
Public attitudes towards individuals with schizophrenia, bipolar disorder, autism and epilepsy can vary widely in both nature and severity (Hargreaves et al. Reference Hargreaves, Loughnane, Grasso and Mothersill2024; Mothersill et al. Reference Mothersill, Loughnane, Grasso and Hargreaves2023). Stigma towards serious mental illnesses such as schizophrenia and bipolar disorder is well documented, while conditions such as autism and especially epilepsy are typically associated with less public fear or blame. This distinction allows epilepsy to serve as a useful baseline comparator for examining how stigma differs across diagnostic categories. Public stigma is associated with worse mental health outcomes and lower life expectancy (Corrigan Reference Corrigan2004; Gissler et al. Reference Gissler, Laursen, Ösby, Nordentoft and Wahlbeck2013; Link et al. Reference Link, Struening, Neese-Todd, Asmussen and Phelan2001; Nearchou et al. Reference Nearchou, Bird, Costello, Duggan, Gilroy, Long, McHugh and Hennessy2018; World Health Organization 2013).
Anti-stigma interventions, such as education and social contact programs, have demonstrated effectiveness in reducing public stigma towards mental health conditions (Thornicroft et al. Reference Thornicroft, Mehta, Clement, Evans-Lacko, Doherty, Rose, Koschorke, Shidhaye, O’Reilly and Henderson2016). A recent systematic meta-review of 19 meta-analyses by McCullock and Scrivano found that contact-based interventions were moderately effective in reducing stigmatizing attitudes, while education-based interventions also showed effectiveness, albeit with smaller reductions (McCullock and Scrivano Reference McCullock and Scrivano2023). However, most anti-stigma initiatives, such as Ireland’s See Change Green Ribbon campaign, focus on mental health stigma broadly (See Change 2021). Educational interventions aim to improve general mental health knowledge, which may in turn promote more positive attitudes and behaviours towards people with mental health conditions (Griffiths et al. Reference Griffiths, Carron-Arthur, Parsons and Reid2014; Corrigan et al. Reference Corrigan, Morris, Michaels, Rafacz and Rüsch2012). However, evidence on whether increased knowledge alone leads to behaviour change remains mixed (McCullock and Scrivano Reference McCullock and Scrivano2023), highlighting the need to test this relationship directly.
There also remains a need for targeted interventions addressing stigma towards specific groups, as different populations may face distinct forms of prejudice and discrimination. The perception that individuals with schizophrenia are dangerous is a well-documented driver of stigma (Mannarini et al. Reference Mannarini, Taccini, Sato and Rossi2022). This belief is inconsistent with evidence showing that people with schizophrenia are rarely violent and are, in fact, more likely to be victims rather than perpetrators of violence (Silverstein et al. Reference Silverstein, Del Pozzo, Roché, Boyle and Miskimen2020). Greater insight into these factors is essential for designing more nuanced and impactful interventions.
In Ireland, the prevalence of these conditions is notably high compared to other countries. For example, a recent nationally representative survey of 1,110 adults found that 42.5% met the criteria for at least one mental health disorder, and 11.1% reported having attempted suicide (Hyland et al. Reference Hyland, Vallières, Shevlin, Bentall, Butter, Hartman, Karatzias, Martinez, McBride, Murphy and Fox2022). Recent research by Mothersill et al. and Hargreaves et al. examined mental health stigma in a pilot study of 307 adults in Ireland, focusing on schizophrenia, bipolar disorder, and autism (Hargreaves et al. Reference Hargreaves, Loughnane, Grasso and Mothersill2024; Mothersill et al. Reference Mothersill, Loughnane, Grasso and Hargreaves2023). Schizophrenia was included due to prior evidence suggesting it is one of the most heavily stigmatized psychiatric conditions, and stigma towards this group has increased in both Europe and the United States in recent decades (Pescosolido et al. Reference Pescosolido, Halpern-Manners, Luo and Perry2021; Schomerus et al. Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022). Bipolar disorder was selected for its overlap with schizophrenia in symptoms, familial patterns, genetic risk, outcomes, and treatment response, supporting the continuum theory that positions bipolar disorder closer to normal functioning and schizophrenia at the severe end (Yamada et al. Reference Yamada, Matsumoto, Iijima and Sumiyoshi2020). Autism was included as a comparator due to its genetic and molecular overlap with schizophrenia and bipolar disorder but as a non-psychotic condition, it provides a contrasting perspective (Carroll and Owen Reference Carroll and Owen2009; Gandal et al. Reference Gandal, Haney, Parikshak, Leppa, Ramaswami, Hartl, Schork, Appadurai, Buil and Werge2018). Autism is increasingly understood within the framework of neurodiversity, which views it as a natural variation in brain function (Silberman Reference Silberman2015).
The findings of these studies revealed notable differences in knowledge, attitudes, and self-reported behaviours towards these groups. Schizophrenia elicited more negative attitudes and behaviours compared to bipolar disorder and autism. Familiarity with any of these conditions was associated with more positive attitudes and behaviours and a lower perception of schizophrenia as dangerous. These results align with prior evidence on the effectiveness of social contact interventions in reducing stigma. Importantly, perceived danger is a critical factor driving stigmatizing attitudes, such as the desire to maintain social distance from individuals with schizophrenia (Mannarini et al. Reference Mannarini, Taccini, Sato and Rossi2022). However, a more comprehensive understanding of stigma towards mental, neurodevelopmental, and neurological conditions in Ireland requires larger, more diverse samples that represent various demographic groups, including differences in gender, location, and education.
The purpose of this study is to build on prior research by conducting a large-scale survey of over 1,200 participants in Ireland. This study examines knowledge, attitudes, and behaviours towards schizophrenia, bipolar disorder, and autism to validate previous findings and explore the effects of both mental health familiarity and knowledge on these measures. Additionally, stigma toward epilepsy is included as a comparator. Although epilepsy shares genetic overlap with the other conditions and affects the brain, it is not classified as a psychiatric disorder in the Diagnostic and Statistical Manual of Mental Disorders (DSM) (Vonberg and Bigdeli Reference Vonberg and Bigdeli2016). Although epilepsy is not typically associated with the same degree of stigma as psychiatric disorders, it has historically been subject to misunderstanding and social distance (Jacoby et al. Reference Jacoby, Snape and Baker2005). Including epilepsy therefore provides a useful neurological baseline for evaluating whether stigma towards mental and neurodevelopmental conditions such as schizophrenia, bipolar disorder, and autism is indeed distinct and more severe.
Based on prior research, the study tested the following hypotheses:
Hypothesis 1: Public perceptions of societal attitudes and self-reported behaviour are more negative towards schizophrenia compared to bipolar disorder, autism, or epilepsy.
Hypothesis 2: Personal familiarity with mental, neurodevelopmental, and neurological conditions predicts more positive self-reported behaviour towards schizophrenia and this relationship is mediated by perception of danger.
Hypothesis 3: Greater knowledge of mental health in general as measured by the Mental Health Knowledge Questionnaire (MHKQ) predicts more positive behaviours towards those with mental health conditions.
It is hoped that testing these hypotheses will provide a more detailed understanding of stigma in the Irish population, informing future anti-stigma interventions to reduce public stigma and improve health outcomes in this country.
Methods
Participants
1,232 participants were recruited across the Republic of Ireland between June and November 2022 by Qualtrics using representative non-probability sampling methods. Given the population of the Republic of Ireland of 5,149,139 in the year the survey was conducted, 2022, and assuming maximum variability in the sample, sample size calculation using Cochran’s sample size formula states that a sample of 1,067 participants is associated with a 95% confidence level and 3% margin of error as a representative sample (Cochran Reference Cochran1963; Central Statistics Office, 2022). Demographic information for participants is presented in Table 1 below.
Demographic breakdown of participants

Measures
Participants completed an online survey delivered over Qualtrics and adapted from research by Durand-Zaleski et al. Mothersill et al. and Hargreaves et al. (Durand-Zaleski et al. Reference Durand-Zaleski, Scott, Rouillon and Leboyer2012; Hargreaves et al. Reference Hargreaves, Loughnane, Grasso and Mothersill2024; Mothersill et al. Reference Mothersill, Loughnane, Grasso and Hargreaves2023). Firstly, participants were asked demographic questions to collect information on age, gender, year of birth, occupation, level of education, income level, living location, country of residency, and country of birth. Next, participants completed validated scales to measure knowledge, attitudes, and behaviour, towards individuals with mental, neurodevelopmental, and neurological conditions. Finally, participants completed individual questions on familiarity, knowledge, perception of danger, and intended behaviour, towards each of the conditions of interest.
The MHKQ consists of 20 items that examine participants’ knowledge about mental health, including questions such as, “Mental health is a component of health” (true) and “Mental disorders are caused by incorrect thinking” (false) (Chen et al. Reference Chen, Wang and Phillips2018; Wang et al. Reference Wang, He, Jiang, Cai, Wang, Zeng, Miao, Qi, Chen and Bian2013; Yin et al. Reference Yin, Wardenaar, Xu, Tian and Schoevers2020). Correct answers are added together to give a total score that ranges from 0 to 20, with higher score associated with higher mental health knowledge. Previous research on a sample of 1,237 participants suggests the MHKQ has high internal consistency, with a Cronbach’s alpha of 0.73 reported, and high test–retest reliability (r = 0.68; p < 0.001) (Wang et al. Reference Wang, He, Jiang, Cai, Wang, Zeng, Miao, Qi, Chen and Bian2013). Internal consistency within the current sample was 0.84.
The Level of Contact Report consists of 12 items that examine situations in which a participant was in contact with mental health difficulties, e.g., “Never observed person with mental illness”, “Watched television documentary about mental illness”, etc. (Holmes et al. Reference Holmes, Corrigan, Williams, Canar and Kubiak1999). The rank score of the statement corresponding to the most intimate level of contact is the participant’s score.
The 5-Question Stigma Indicator-community stigma (5-QSI-CS) consists of five questions that examine perceptions of societal stigma towards a particular group and has previously been used to examine leprosy, (Hanoeman et al. Reference Hanoeman, Van Brakel, Arif and Waltz2017). Participants select “Never” (0), “Sometimes” (1), “Often/usually” (2), and “Don’t know” (0). Scores are added together to provide a total score that ranges from 0 to 10, with higher scores associated with higher levels of perceived societal stigma towards that group. Prior research on leprosy indicates that the 5-QSI-CS has a Cronbach’s alpha of 0.52. In our study, participants completed the 5-QSI-CS for each group of interest, with Cronbach’s alpha of 0.76, 0.79, 0.77, and 0.80, for schizophrenia, bipolar disorder, autism, and epilepsy, respectively.
To examine knowledge of schizophrenia, bipolar disorder, and autism, participants were given a score of 1 for each correct answer to the following questions (“Agree” or “Strongly agree” was deemed the correct answer if the statement was true, “Disagree” or “Strongly disagree” was deemed the correct answer if the statement was false, “Neutral” always received 0).
Schizophrenia/bipolar disorder/autism…:
-
… Is Contagious (false)
-
… Is a condition with which one can live normally, with treatments (true)
-
… Is hereditary (genetic) (true)
-
… First appears in young adults (true - schizophrenia/bipolar disorder, false - autism)
To examine perceived danger associated with schizophrenia, bipolar disorder, autism, and epilepsy, participants answered two questions on each of the four conditions, selecting “Strongly agree”, “Agree”, “Disagree”, or “Strongly disagree”.
-
A person with X represents a danger to themselves (suicide, prison, indebtedness…)
-
A person with X often represents a danger to others (murder, rape, violence …)
Answers were reverse-coded so that a higher score meant greater perceived danger.
To examine intended behaviour towards schizophrenia, bipolar disorder, autism, and epilepsy, the following questions were used:
-
Would you work with someone who had X?
-
Would you allow your children to be in the same class as a child with X?
-
Would you accept to live under the same roof as a loved one if s/he had X?
“Yes happily” was rated as 3, “Yes if I had to” was rated as 2, and “Absolutely not” was rated as 1. These scores were added to give a total score associated with more positive intended behaviour towards the group in question, which ranged from three to nine.
Design
The study used a correlational, cross-sectional research design. To test our hypothesis that public perceptions of societal attitudes and self-reported behaviour are more negative towards schizophrenia compared to bipolar disorder, autism, or epilepsy, we examined condition of interest as the predictor variable (i.e., questions referring to schizophrenia, bipolar disorder, autism, or epilepsy), and measures of public perceptions of societal attitudes and self-reported behaviour as criterion variables, in a series of statistical tests (see below). To test our hypothesis that personal familiarity with mental, neurodevelopmental, and neurological conditions predicts more positive self-reported behaviour towards schizophrenia and this relationship is mediated by perception of danger, we examined familiarity with mental, neurodevelopmental, and neurological conditions as the predictor variable, self-reported behaviour as the criterion variable, and perception of danger as the mediating variable, in a mediation analysis.
Procedure
Participants completed the survey online over Qualtrics, and responses were sent to the authors from Qualtrics as a Microsoft Excel. xlsx file, which we converted to an IBM SPSS Statistics. sav file for descriptive statistics and calculating variables of interest. Cumulative Link Mixed Models and mediation tests were performed in R. Full ethical approval for this research was provided by the National College of Ireland Research Ethics Committee on 24/08/2018 (Research Ethics Committee approval number: 2408201801).
Statistical analysis
Participants with missing values for over half of their questions were eliminated from the study, leaving 1,002 participants, 895 of whom had less than 10 missing values for all questions. Knowledge, Community Stigma, Behaviour and Danger to Others scores were calculated as noted in the relevant questionnaire sections above, and averaged for each score. The Level of Contact Report was used to calculate Familiarity, with levels 1 to 6 coded as No Experience, levels 9 to 11 as Family Member, and level 12 as Oneself. Levels 7 and 8, relating to working with people with mental health conditions, were excluded for low numbers and due to the fact they did not easily integrate thematically into any of the other coded groups. Finally, MHKQ scores were split into quartiles, with lower quartiles indicating less knowledge.
We then analysed effects of independent variables (IVs) Disorder and either Familiarity or MHKQ plus interactions on the four main dependent variable (DVs) measures Knowledge, Community Stigma, Behaviour and Danger to Others, each done separately. This was done using cumulative link mixed models using the ‘Ordinal’ package in R. Random intercepts were specified for Participants. Specifically, the models specified were of the form: DV ∼ IV1*IV2 + (1 | Participant). For example, the formula for the effect of Disorder and Familiarity on Knowledge was: Knowledge ∼ Familiarity*Disorder + (1 | Participant). Effects were tested by performing an ANOVA for the full model against that model minus the relevant effect being tested. If an interaction proved significant, post-hoc tests were performed across different levels of Disorder and considered significant if they passed a Bonferroni-corrected alpha threshold = 0.05*number of tests performed.
Finally, a mediation analysis was performed to focus in on the relationship between perceived Danger to Others and negative Behaviour towards those with Schizophrenia. The mediation model was specified as the effect of Disorder (specifically the contrast of EP (baseline) vs SZ) on Behaviour, as mediated by Danger to Others. This was done with linear mixed effects models using the ‘lmer’ package in R, in combination with the ‘mediation’ package.
Results
Knowledge, community stigma (Attitude), and stigma behaviour across condition
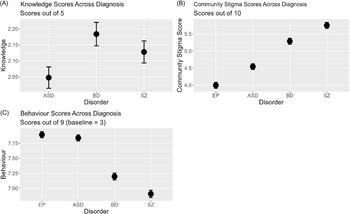
Knowledge scores differed slightly but significantly when referring to ASD, BD and SZ (χ2(df = 6) = 20.52, p = 0.002), specifically being greater for BD compared to both ASD (χ2(df = 3) = 16.22, p = 0.001), see Figure 1. Community Stigma scores differed more strongly, with strongest community stigma for SZ, followed by BD, ASD, then EP in that order (χ2(df = 9) = 473.16, p < 0.001, all pairwise comparisons p < 0.001). Finally, Behaviour scores differed strongly between condition (χ2(df = 9) = 653.67, p < 0.001, all pairwise comparisons p < 0.001), with SZ then BD having worst Behaviour scores compared to EP and ASD.
(A) Knowledge scores about each disorder, ASD, BD and SZ. (B) Community stigma scores across disorder. Higher scores indicate more community stigma towards the cohort with that disorder. (C) Behaviour scores with respect to each disorder. Higher scores indicate better behaviour towards the cohort with that disorder.

Impact of familiarity with mental, neurodevelopmental, and neurological conditions on knowledge, community stigma (Attitude), and stigma behaviour across condition
Knowledge scores differed slightly according to familiarity, with lower familiarity scores indicating less knowledge (χ2(df = 6) = 14.09, p = 0.02), but no interaction between this effect and condition, see Figure 2. Community Stigma was lowest for those with least familiarity with MH issues (χ2(df = 8) = 27.61, p < 0.001), while an interaction between Condition and Familiarity (χ2(df = 6) = 19.12, p = 0.004) indicated this effect was strongest for ASD and BD (p < 0.001 and p = 0.026 respectively). Behaviour was impacted strongly by Familiarity across all conditions (χ2(df = 8) = 82.62, p < 0.001), with an Interaction between Familiarity and Condition showing a stronger effect of Familiarity for SZ, followed by BD, ASD then EP respectively (all p < 0.001).
(A) Knowledge scores about each disorder, ASD, BD and SZ, split into three familiarity groups, no experience of mental health issues, family member with any mental health disorder, and oneself having a mental health disorder. (B) Community stigma scores across disorder and familiarity group. Higher scores indicate more community stigma towards the cohort with that disorder. (C) Behaviour scores with respect to each disorder and familiarity group. Higher scores indicate better behaviour towards the cohort with that disorder.

Impact of mental health knowledge (MHKQ) on knowledge, community stigma (Attitude), and stigma behaviour across condition
As a means of cross validating our Knowledge scores from our original questionnaire (specific to each Condition) versus the MHKQ (relating to knowledge of mental health in general), we looked at the relationship between each measure. Knowledge scores differed strongly according to MHKQ scores (χ2(df = 9) = 140.33, (p < 0.001, no interaction), with lower scores on MHKQ predicting lower Knowledge scores, see Figure 3. There was an interesting relationship between MHKQ and Community Stigma (interaction effect:) χ2(df = 9) = 144.37, p < 0.001), whereby lower MHKQ scores predicted greater Community Stigma with respect to EP (χ2(df = 3) = 34.76, p < 0.001), but lower MHKQ scores predicted lower Community Stigma for SZ (χ2(df = 3) = 43.57, p < 0.001), with no relationship between MHKQ and Community Stigma for ASD or BD. Finally, there was a strong relationship between MHKQ and Behaviour for EP, ASD and BD with lower MHKQ scores predicting worse Behaviour, but interestingly no such effect for SZ (interaction effect: χ2(df = 9) = 161.67, p < 0.001; all comparisons within Condition p < 0.001 except for SZ, p = 0.07).
(A) Knowledge scores about each disorder, ASD, BD and SZ, split into four mental health knowledge questionnaire (MHKQ) groups, where a lower position group indicates lower MHKQ score. (B) Community stigma scores across disorder and MHKQ group. Higher scores indicate more community stigma towards the cohort with that disorder. (C) Behaviour scores with respect to each disorder and MHKQ group. Higher scores indicate better behaviour towards the cohort with that disorder.

Relationship between familiarity and mental health knowledge (MHKQ) on perception of danger to others across condition
Overall, there was a pattern whereby there was a greater perception of Danger to Others (i.e. lower scores on the Danger to Others scale) for SZ, followed by BD, then ASD and EP (χ2(df = 9) = 725.07, p < 0.001, all pairwise comparisons p < 0.001), see Figure 4. Greater Familiarity only seemed to mitigate the sense of Danger to Others with respect to SZ (χ2(df = 2) = 16.48, p < 0.001) and not for any of the other Conditions (interaction effect: (χ2(df = 6) = 26.67, p < 0.001). The opposite effect was found when looking at the relationship between MHKQ and Danger to Others, where greater MHKQ scores predicted less perception of Danger to Others for all Conditions except SZ (interaction effect:) (χ2)(df = 9) = 76.71, p < 0.001, all p < 0.001 except SZ, (p = 0.22).
(A) Danger to others score relating to a given disorder, split by familiarity group. Higher danger to others score indicates greater perceived danger for that given disorder. (B) Danger to others score relating to a given disorder, split by MHKQ group. (C) Mediation analysis of disorder (EP vs SZ) relationship with behaviour, as mediated by sense of perceived danger to others.

Worse behaviour towards SZ is partially mediated by perception of greater danger to others in SZ
Given the above results, we hypothesized that the degree to which our participants may display worse Behaviour towards those with SZ (as compared to a baseline Condition of EP) could be mediated by their Perception of SZ Danger to Others. To test this, we ran a mediation analysis with contrast of SZ vs EP Conditions as the independent variable, Danger to Others score as mediator, and Behaviour as outcome. We found a significant and sizeable mediation, where the proportion of the total effect of Condition on Behaviour which was mediated was estimated at 32.1%, with a 95% confidence interval [27.7, 37%], p < 0.001) (Figure 4).
Discussion
This study aimed to investigate knowledge, attitudes, and behaviours towards schizophrenia, bipolar disorder, autism, and epilepsy in Ireland, utilizing a large sample of adults. The primary objective was to compare community stigma, knowledge, and intended behaviours across these groups. Consistent with our pilot study, findings revealed significant disparities in community stigma and behaviours, with higher stigma and less favourable intended behaviours towards individuals with bipolar disorder and in particular schizophrenia compared to epilepsy and autism.
A secondary objective examined whether familiarity with these conditions predicted lower stigma and more positive behaviours. Increased familiarity was associated with more positive behaviours across all conditions, with the strongest effects observed for bipolar disorder and schizophrenia. Interestingly, familiarity also correlated with perception of greater stigma among the community towards a particular group. So instead of this questionnaire measuring internal stigma projected onto society/community, it instead potentially reflects greater empathy and awareness of stigma among those more familiar with these conditions.
The third objective explored the influence of mental health knowledge on stigma and behaviour. Higher scores on the MHKQ predicted more positive behaviours for all conditions except schizophrenia, which appeared less responsive to increased knowledge.
Finally, the study examined perceptions of danger associated with each condition. Bipolar disorder and schizophrenia were linked to higher perceived danger. For schizophrenia, perceived danger was mitigated by familiarity but not by mental health knowledge, contrasting with other conditions that showed the opposite pattern. A mediation analysis further demonstrated that perceived danger contributed to worse intended behaviours towards individuals with schizophrenia. These findings highlight critical implications for anti-stigma policies and interventions in Ireland and comparable Western societies.
Stigma towards individuals living with schizophrenia in Ireland
The results indicate that adults in Ireland hold more negative attitudes and engage in less favourable behaviours towards individuals living with schizophrenia compared to those with other conditions. These findings corroborate our earlier pilot study (N = 307) and align with international research showing elevated stigma towards schizophrenia in Western countries (Durand-Zaleski et al. Reference Durand-Zaleski, Scott, Rouillon and Leboyer2012; Mothersill et al. Reference Mothersill, Loughnane, Grasso and Hargreaves2023; Pescosolido et al. Reference Pescosolido, Halpern-Manners, Luo and Perry2021; Schomerus et al. Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022; Wood et al. Reference Wood, Birtel, Alsawy, Pyle and Morrison2014). These findings have important implications for mental-health policy and service design in Ireland. The consistency of elevated stigma towards schizophrenia suggests that generic anti-stigma campaigns may not sufficiently address public fears and misconceptions specific to this condition. Targeted efforts may be needed, such as campaigns that humanize lived experience and directly challenge myths relating to unpredictability and dangerousness.
In France, Durand-Zaleski et al., observed similar trends, finding greater stigma towards schizophrenia compared to bipolar disorder and autism among 1,000 participants (Durand-Zaleski et al. Reference Durand-Zaleski, Scott, Rouillon and Leboyer2012). In the United States, Pescosolido et al. reported a decline in acceptance of schizophrenia between 1996 and 2018, in contrast to improved acceptance of depression (Pescosolido et al. Reference Pescosolido, Halpern-Manners, Luo and Perry2021). Schomerus et al. documented similar patterns in Germany, with attitudes towards depression improving over time while stigma towards schizophrenia worsened (Schomerus et al. Reference Schomerus, Schindler, Sander, Baumann and Angermeyer2022). Likewise, in the UK, schizophrenia was rated more negatively than depression or anxiety in a survey of 1,070 participants (Wood et al. Reference Wood, Birtel, Alsawy, Pyle and Morrison2014). Together, these studies reinforce the persistently high stigma surrounding schizophrenia across Western contexts.
Familiarity, knowledge and perception of danger
Familiarity with mental health issues, whether through personal diagnosis or a close relationship with someone diagnosed, predicted more positive attitudes and behaviours towards all conditions. This finding aligns with previous research suggesting that social contact interventions effectively reduce stigma (Corrigan and Nieweglowski Reference Corrigan and Nieweglowski2019; Hargreaves et al. Reference Hargreaves, Loughnane, Grasso and Mothersill2024; McCullock and Scrivano Reference McCullock and Scrivano2023). A slightly different pattern was found however with respect to mental health knowledge and behaviours, where greater knowledge predicted more positive behaviours towards all conditions except for schizophrenia, which appeared not to gain any benefit from greater knowledge. It is important to note here that knowledge as we have measured it refers to cumulative knowledge from life experience. One possible implication of these findings is that social contact interventions designed to increase familiarity might be more effective at reducing prejudice and discrimination towards schizophrenia compared to interventions without social contact (albeit these interventions might be effective for other groups). To examine this in more detail, more research is needed, and particularly research evaluating new social contact and educational interventions themselves.
Focusing on schizophrenia, we found that worse stigmatizing behaviours towards those with schizophrenia was mediated by a higher perception of danger. Schizophrenia is often perceived as more dangerous than conditions like depression or anxiety (Mannarini et al. Reference Mannarini, Taccini, Sato and Rossi2022; Wood et al. Reference Wood, Birtel, Alsawy, Pyle and Morrison2014). Perceived danger has been shown to predict stigmatizing attitudes, such as a desire to maintain social distance (Mannarini et al. Reference Mannarini, Taccini, Sato and Rossi2022). In the U.S., increased perceptions of danger have been accompanied by declining acceptance of schizophrenia over recent decades (Pescosolido et al. Reference Pescosolido, Halpern-Manners, Luo and Perry2021).
This perception may be influenced by biological explanations and media portrayals. For instance, Kvaale et al., found that biogenetic explanations for psychological conditions can increase perceptions of danger (Kvaale et al. Reference Kvaale, Haslam and Gottdiener2013). Western media frequently associates schizophrenia with violence, reinforcing public fears (Gwarjanski and Parrott Reference Gwarjanski and Parrott2018; Maletta and Vass Reference Maletta and Vass2023; Ross et al. Reference Ross, Morgan, Jorm and Reavley2019). While the role of Irish media remains unclear, there is an opportunity to challenge stigmatizing narratives. For example, 54.8% of respondents in our pilot study felt uninformed about mental illness by the media (Mothersill et al. Reference Mothersill, Loughnane, Grasso and Hargreaves2023). Furthermore, an analysis of 656 online news articles showed that while most avoided reinforcing stigma, few actively challenged it, such as by incorporating first-person perspectives (Godfrey et al. Reference Godfrey, Gavin, Haskins, O’Meara, O’Connor and Donohoe2024).
Autism and epilepsy, in contrast, were associated with substantially lower levels of community stigma and more favourable behavioural intentions. Individuals with autism were perceived as less dangerous than those with schizophrenia or bipolar disorder, and mental health knowledge was associated with more positive behaviours towards this group – a pattern not observed for schizophrenia. This may partly reflect the growing influence of the neurodiversity framework, which positions autism as a natural variation in brain function rather than a disorder requiring correction (Silberman Reference Silberman2015). Epilepsy, included as a neurological comparator, attracted the lowest stigma of all four conditions. While epilepsy has historically been subject to misunderstanding and social exclusion (Jacoby et al. Reference Jacoby, Snape and Baker2005), our findings suggest that public attitudes have shifted considerably, consistent with its classification outside the realm of psychiatric disorders.
Strengths and limitations
This study’s key strength lies in its use of a large sample to examine stigma across four groups, providing robust comparisons and statistical power to detect various effect sizes. Additionally, this is the first large-scale investigation of stigma towards schizophrenia and other conditions in Ireland.
However, some limitations should be noted. First, while the overall sample size was large (N = 1,232), the subgroup analysis comparing the four groups was based on a slightly smaller sample (N = 847). Future research should confirm these findings in nationally representative samples. Second, as a correlational study, causal relationships between familiarity, stigma, and perceived danger cannot be established. Although prior studies suggest that social contact interventions reduce stigma, further research is needed to assess interventions targeting beliefs about danger specifically (McCullock and Scrivano Reference McCullock and Scrivano2023). For example, Amsalem et al. showed that brief video-based interventions could reduce stigma towards schizophrenia, but additional studies are required to explore their impact on perceptions of danger (Amsalem et al. Reference Amsalem, Yang, Jankowski, Lieff, Markowitz and Dixon2021).
Finally, the findings are specific to Ireland, and stigma is influenced by social and cultural factors. For instance, preliminary findings from a study in Liberia (N = 1,148) using the same survey indicate relatively higher acceptance of schizophrenia compared to other conditions. Direct comparisons between countries could provide valuable insights into the factors shaping stigma in different cultural contexts (Dossen et al. Reference Dossen, Mulbah, Hargreaves, Kumar, Mothersill, Loughnane, Byrd, Nyakoon, Quoi and Ebuenyi2024).
Conclusion
In conclusion, this study explored knowledge, attitudes, and behaviours towards schizophrenia, bipolar disorder, autism, and epilepsy in Ireland, using a large sample of 1,232 adults. The findings highlight more negative attitudes and behaviours towards schizophrenia, with familiarity associated with more positive outcomes but not greater mental health knowledge. Furthermore, worse behaviours towards schizophrenia were mediated by a higher sense of perceived danger. These results suggest that future national stigma-reduction strategies should consider condition-specific messaging, particularly for schizophrenia, rather than broad, undifferentiated mental-health campaigns. Evidence from other countries supports approaches using structured social-contact elements, recovery stories, and myth-busting educational components tailored to schizophrenia-related stereotypes. These results also emphasize the importance of targeted anti-stigma interventions with a focus on challenging perceptions of danger, increasing familiarity, and enhancing public understanding.
Data availability statement
Data reported in this paper are available upon request through Smardy: Marketplace for Technology Transfer of Research Data, Software, and Results (https://smardy-project.eu/).
Acknowledgements
The authors would like to acknowledge all individuals who participated in this survey.
Funding statement
This research is generously funded by ESTHER Ireland (REF NUMBER_72939).
Competing interests
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008. The study protocol was approved by the ethics committee of each participating institution: HREC approval number 2408201801.





 Open access
Open access