


Introduction
The Fontan procedure is frequently the definitive surgical intervention in a staged palliation approach for individuals with single-ventricle congenital heart disease. This pivotal intervention establishes a connection between the venous and pulmonary circulations, effectively separating the systemic and pulmonary blood flow. This allows passive delivery of deoxygenated blood to the lungs while the single functional ventricle maintains systemic circulation. The advent of Fontan palliation has dramatically improved the survival rates for patients across the spectrum of single-ventricle anatomies, including those with hypoplastic or absent right or left ventricles.
Despite significant improvements in survival, achieving a normal quality and duration of life for Fontan patients remains a significant challenge. A key characteristic of Fontan circulation—chronically elevated central venous pressure coupled with a limited cardiac output, particularly during periods of increased physiological demand—often triggers a cascade of progressive dysfunction across multiple organ systems. Reduced exercise capacity is a frequently observed clinical feature in this population, impacting cardiopulmonary endurance, the ability to perform daily activities, and overall prognosis. This decline in exercise tolerance is closely associated with increased cardiovascular morbidity and mortality, underscoring the importance of its assessment in evaluating functional status and the intricate interplay between cardiac and extracardiac factors. Reference Gewillig and Brown1,Reference Rychik, Atz and Celermajer2
Beyond cardiovascular factors, the systemic effects of Fontan circulation extend to various extracardiac domains. Individuals with Fontan circulation often exhibit altered body composition, including reduced muscle mass, increased adiposity, and shorter stature compared to their healthy peers. Reference Cordina, O’Meagher and Gould3,Reference Powell, Wittekind and Alsaied4 Although the mechanism of muscle loss in Fontan patients remains unclear, Reference Powell, Wittekind and Alsaied4 the association between muscle mass and exercise-induced cardiac output suggests that extracardiac features may reflect underlying cardiovascular function. Reference Tran, D’Ambrosio and Verrall5
Previous studies have suggested that extracardiac factors, including exercise capacity and skeletal muscle function, as reflected by measures such as handgrip strength, Reference Neidenbach, Oberhoffer and Pieper6 body composition, Reference Cordina, O’Meagher and Gould3,Reference van den Berg, Pos, Scheffers, van den Berg and Helbing7 and relevant blood biomarkers, may contribute to functional capacity and overall clinical outcomes in patients with Fontan circulation. Reference Gewillig and Brown1,Reference Rychik, Atz and Celermajer2 This study presents our centre’s experience regarding the cardiac and extracardiac characteristics of patients who have undergone the Fontan procedure. Our primary aim was to comprehensively evaluate these parameters within our patient cohort and to explore the potential relationships between them, thereby contributing valuable experiences to the clinical management of individuals with Fontan circulation.
Methods
Study design and participants
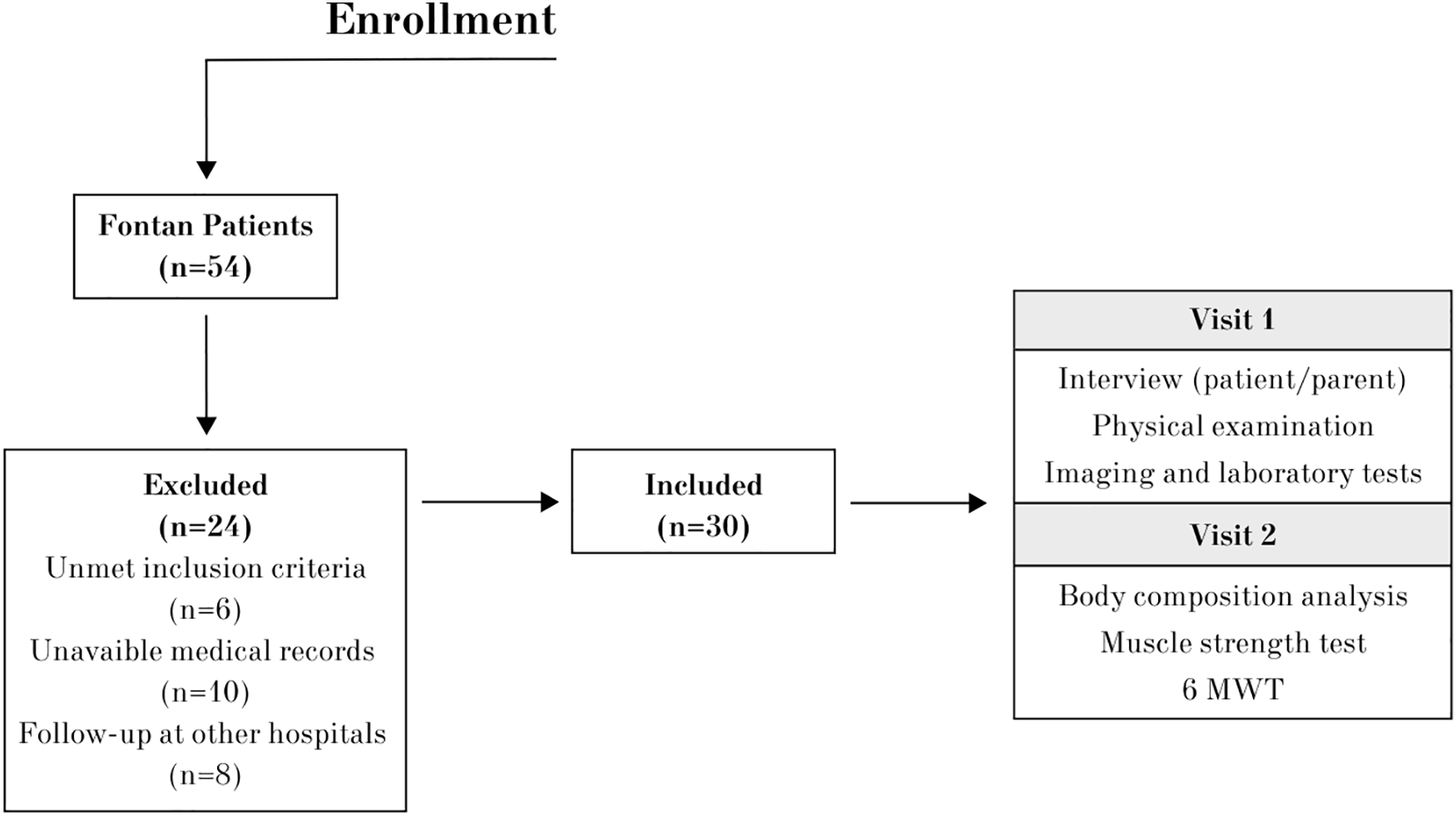
This prospective, single-centre study was conducted at the Division of Pediatric Cardiology, Hacettepe University İhsan Doğramacı Children’s Hospital. The study protocol was reviewed and approved by the Hacettepe University Ethics Committee (Approval No: 16969557-2187, Approval Date: December 2019). Prior to participation, written informed consent was obtained from parents, assent from patients aged 8–17 years, and direct consent from individuals aged 18 years and older. The study adhered to the ethical principles outlined in the 1975 Declaration of Helsinki. We screened the database of Fontan patients who had undergone surgery and were under follow-up at our paediatric cardiology clinic between January 2009 and August 2019. From this database of 54 patients, individuals were contacted and invited to participate in the study. Following contact, 30 patients attended the clinic for eligibility assessment. Patients were included in the study if they met the following criteria at the time of their study visit: clinical stability, no history of exercise-induced syncope, absence of a pacemaker, and no recent medication changes that could affect clinical stability. Following eligibility confirmation, 30 patients were enrolled in the study. A flowchart detailing the patient recruitment and enrolment process is provided in Figure 1.
Study design flowchart.

Procedure and data collection
A multidisciplinary team, including a paediatric cardiologist, paediatrician, and cardiorespiratory physiotherapist, conducted comprehensive assessments. These assessments, conducted over one or two visits (Figure 1):
Visit 1: Patient/parent interview, physical examination, review of imaging and laboratory tests to confirm eligibility, and baseline clinical assessment. Echocardiographic assessments were performed by a paediatric cardiologist, ideally on the same day as Visit 1 or close to Visit 2 to reflect the patient’s current cardiac status.
Visit 2: Body composition analysis, 6-minute walk test, and muscle strength measurements.
Measurements
Demographic data, including age at admission and surgery, associated cardiac anomalies, echocardiographic findings, and cardiac catheterisation results, were collected. Physical examination findings at the time of the study visit were documented. The latest available laboratory test results, including complete blood count, liver and kidney function tests (ALT, AST, creatinine, albumin, uric acid), haemoglobin, red cell distribution width, and B-type natriuretic peptide levels, were analysed.
Body composition
Body weight (kg), body fat percentage (%), and lean body mass (kg) were assessed using a bioelectrical impedance analysis device (Xiaomi Mi Body Composition Scale 2, Xiaomi Corporation, Beijing, China). Reference Alidadi, Metanati and Ataie-Jafari8 Height (cm) was measured with a digital stadiometer, and body mass index (kg/m2) was subsequently calculated and recorded. Reference Alidadi, Metanati and Ataie-Jafari8 The expected handgrip strength in kilograms was calculated separately for participants aged below 18 Reference McQuiddy, Scheerer, Lavalley, McGrath and Lin9 and above 18. Reference Bohannon, Peolsson, Massy-Westropp, Desrosiers and Bear-Lehman10
Exercise capacity
Exercise capacity was assessed using the 6-minute walk test (6MWT), conducted in accordance with the guidelines of the European Respiratory Society and the American Thoracic Society. Participants were given standardised instructions to walk as far as possible within a 30-metre enclosed corridor. Heart rate and oxygen saturation (SpO2) were recorded before and after the test using a pulse oximeter (PalmSAT 2500; Nonin Medical Inc., Plymouth, MN, USA). The oxygen saturation difference (ΔSpO2) was determined by measuring oxygen saturation before and after the 6MWT.
Blood pressure was measured with a sphygmomanometer (Erka, Bad Tölz, Germany), and dyspnoea, leg fatigue, and overall fatigue levels were assessed pre- and post-test using the Modified Borg Scale. The total distance covered was recorded in metres. Reference Holland, Spruit and Troosters11 No adverse events occurred during the 6MWT in any participant.
Handgrip strength
Handgrip strength was measured using a hand dynamometer (Jamar, Sammons Preston, Rolyon, Bolingbrook, IL, USA) in accordance with the standard procedures. Three measurements were taken for each hand, and the highest recorded value from either hand was used for analysis. Reference Haidar, Kumar, Bassi and Deshmukh12 Predicted percentages of normal values for children and adults were calculated by age and sex, based on previously published reference equations. Reference McQuiddy, Scheerer, Lavalley, McGrath and Lin9
Statistical analysis
Statistical analysis was performed using SPSS v23 (Statistical Package for the Social Sciences, SPSS Inc., Chicago, IL). Descriptive values were presented as percentages (%) and frequencies for categorical variables. Continuous variables following a normal distribution were expressed as mean ± standard deviation, while those not following a normal distribution were reported as median (minimum–maximum) and interquartile range (25th–75th percentile). The normality of data distribution was assessed using the Shapiro–Wilk test. Comparisons of independent continuous variables were conducted using the Mann–Whitney U test. The association among categorical variables was observed with Pearson’s chi-square test or Fisher’s exact test. The relationship between continuous variables was observed with Spearman’s rank correlation coefficient. P-value < 0.05 was considered statistically significant for all tests.
Results
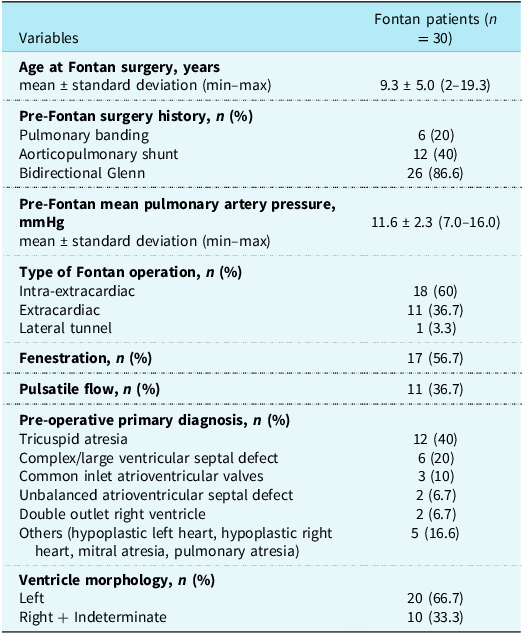
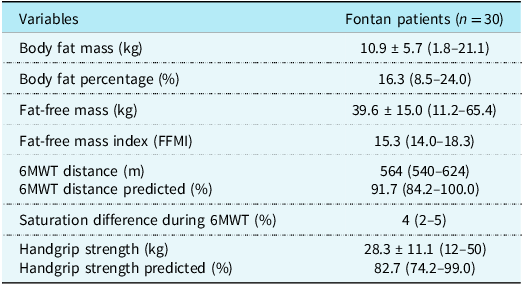
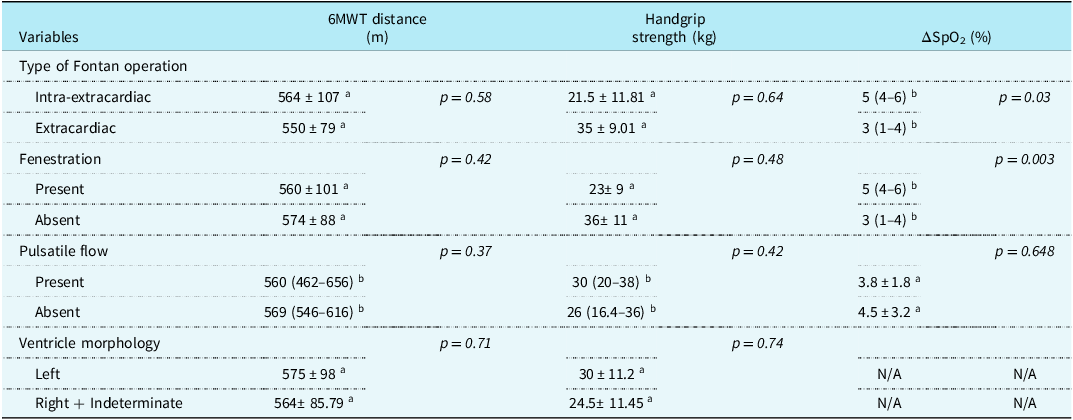
A total of 54 Fontan patients (35 male, 19 female) were assessed for eligibility. Twenty-four patients were excluded due to unmet inclusion criteria (n = 6), unavailable medical records (n = 10), or follow-up at other hospitals (n = 8). Ultimately, 30 eligible Fontan patients (age range: 7.0–33.0 years; 19 male and 11 female) were included in the study. Clinical characteristics and laboratory findings of Fontan patients are summarised in Table 1. The mean age at Fontan surgery for the 30 patients was 9.3 ± 5.0 years. Most patients (60%) had an intra-extracardiac Fontan conduit. Fenestration was present in over half (56.7%) of the cases, and pulsatile flow was observed in 36.7% of patients. Additional details on preoperative diagnoses, ventricular morphology, and Fontan-related surgical and clinical characteristics are provided in Table 2. Data on body composition and functional exercise capacity, as assessed by the 6MWT and handgrip strength measurements, are presented in Table 3. Based on age- and sex-predicted maximal handgrip strength, the median handgrip strength was approximately 82.7% (74.2–99.0). Reference McQuiddy, Scheerer, Lavalley, McGrath and Lin9,Reference Bohannon, Peolsson, Massy-Westropp, Desrosiers and Bear-Lehman10 Similarly, based on age- and sex-predicted maximal 6MWT distance, the median performance was approximately 91.7% (84.2–100.0). Reference Geiger, Strasak and Treml13 In analyses of 6MWT distance, handgrip strength, and ΔSpO2 in relation to Fontan operation type, fenestration status, pulsatile flow, and ventricular morphology, patients with an extracardiac Fontan tended to have a slightly lower 6MWT distance (550 ± 79.6 m) compared to those with an intra-extracardiac Fontan (564 ± 107.7 m), although this difference did not reach statistical significance (p = 0.58). Similarly, handgrip strength did not differ significantly between the groups (p = 0.64). However, post-exercise desaturation (ΔSpO2) was significantly higher in patients with an intra-extracardiac Fontan (p = 0.03) and in those with fenestration (p = 0.003). Pulsatile flow and ventricular morphology did not show a significant effect on the 6MWT distance or handgrip strength (Table 4). Correlation analysis revealed a significant relationship between post-exercise desaturation (ΔSpO2) and functional assessment results. Greater post-exercise desaturation was associated with a shorter 6MWT distance (r = −0.531, p = 0.008) and lower handgrip strength (r = −0.472, p = 0.017). The 6MWT distance showed a positive correlation with handgrip strength (r = 0.537, p = 0.002) and fat-free mass (r = 0.598, p < 0.001). Red cell distribution width was negatively correlated with 6MWT distance (r = −0.631, p < 0.001) and handgrip strength (r = −0.413, p = 0.029). These correlation coefficients and p-values are visually summarised in Figure 2.
Association between physiological assessments and clinical parameters in Fontan patients correlations were assessed using Spearman’s correlation coefficient. Numbers within circles indicate correlation coefficients (r). Colour intensity reflects the strength of the correlation. An asterisk (*) indicates statistically significant correlations (p < 0.05).

Clinical characteristics and laboratory findings of Fontan patient

Descriptive statistics are presented as mean ± standard deviation (min–max) or median (25th–75th percentile) for numerical variables and as number (percentage) for categorical variables.
BMI = body mass index; BNP = brain natriuretic peptide; BUN = blood urea nitrogen; RDW = red cell distribution width; ALT = alanine aminotransferase; AST = aspartate aminotransferase.
Patient characteristics related to history of Fontan surgery

Body composition and functional test results of Fontan patients

Descriptive statistics are presented as mean ± standard deviation (min–max) or median (25th–75th percentile) for numerical variables.
6MWT = 6-minute walk test.
The impact of Fontan-related factors on 6MWT distance, handgrip strength, and oxygen desaturation (ΔSpO2)

Table 4 Long description
The table presents data on the impact of Fontan-related factors on 6MWT distance, handgrip strength, and oxygen desaturation in Fontan patients. It has four rows and three columns. The columns are labeled as 6MWT distance (m), Handgrip strength (kg), and ΔSpO2 (%). The rows are labeled as Type of Fontan operation, Fenestration, Pulsatile flow, and Ventricle morphology. Each row further breaks down into subcategories with corresponding values and p-values. For example, under Type of Fontan operation, the subcategories are Intra-extracardiac and Extracardiac, with values for 6MWT distance, handgrip strength, and ΔSpO2. The table also includes p-values for each comparison. Notable trends include significant differences in post-exercise desaturation (SpO2) based on the type of Fontan operation and the presence of fenestration.
6MWT = 6-minute walk test; ΔSpO2 = oxygen saturation difference; N/A = Not available.
a Data are presented as mean ± standard deviation.
b Data are presented as median (25th–75th percentile).
Discussion
The Fontan procedure, while a vital palliative strategy for single-ventricle physiology, is associated with long-term challenges stemming from circulatory inefficiency and multiorgan dysfunction. Exercise intolerance is a recognised characteristic of Fontan physiology and correlates with increased morbidity and mortality. Reference Cordina, O’Meagher and Gould3,Reference Tran, D’Ambrosio and Verrall5 In this study, we evaluated the overall clinical and functional profiles of 30 Fontan patients at our centre and investigated the relationships between body composition, muscle strength, and exercise performance, demonstrating significant correlations between handgrip strength, fat-free mass, and 6MWT distance. These findings highlight the combined role of skeletal muscle mass and limb perfusion in determining exercise capacity in this complex patient population.
Several studies have investigated the haemodynamic outcomes and functional capacity associated with different types of Fontan procedures, including intra-extracardiac total cavopulmonary connection and extracardiac total cavopulmonary connection. Reference Hirose, Ikai and Murata14 De Leval et al. suggest that surgical techniques that better preserve laminar flow contribute to reduced energy dissipation, thereby improving exercise tolerance and overall functional capacity in Fontan patients. Reference de Leval15 The maintenance of laminar flow is essential for optimising haemodynamic efficiency, as it reduces energy loss within the Fontan circulation. This has been associated with enhanced exercise capacity and improved quality of life. Among various Fontan techniques, the intra-extracardiac approach is hypothesised to offer advantages in minimising energy loss and maintaining physiological flow dynamics. Reference Gewillig and Brown1,Reference de Leval15,Reference Ohye, Schranz and D’Udekem16 Although our study did not reveal a significant difference between surgical techniques in terms of functional capacity (Table 4), the importance of preserving laminar flow in Fontan circulation remains a key factor. Theoretically, the intra-extracardiac Fontan method may offer advantages in preventing energy loss within the Fontan circulation, ensuring a more efficient haemodynamic state. This technique facilitates smoother venous return, reduces turbulence-related energy dissipation, and optimises flow distribution across the pulmonary vascular bed. While our findings did not confirm this distinction, previous studies suggest that optimising flow dynamics through minimising energy dissipation could contribute to better long-term outcomes. Reference Gewillig and Brown1,Reference de Leval15,Reference Ohye, Schranz and D’Udekem16
Red cell distribution width is a quantitative measure of the variation in erythrocyte volume and serves as an indicator of anisocytosis. It is routinely used in the differential diagnosis of microcytic and normocytic anaemias. Although iron deficiency remains one of the most common and clinically relevant causes of elevated red cell distribution width, this parameter may also reflect other underlying pathophysiological processes. Reference Cordina, O’Meagher and Gould3,Reference van den Berg, Pos, Scheffers, van den Berg and Helbing7 An increased red cell distribution width has been associated with a range of cardiovascular diseases, including acute coronary syndromes and heart failure. Reference Felker, Allen and Pocock17
In our study, red cell distribution width was negatively correlated with both the 6MWT distance (r = −0.631, p < 0.001) and handgrip strength (r = −0.413, p = 0.029), suggesting that higher red cell distribution width values were associated with reduced functional performance. This association might be partially explained by unrecognised iron deficiency or anaemia, both of which are known to impair exercise tolerance and peripheral muscle strength. A recent review by Wittczak et al. emphasised that red cell distribution width can serve as a surrogate marker of iron deficiency and has been associated with reduced exercise capacity in patients with Fontan circulation. Reference Wittczak, Mazurek-Kula, Banach, Piotrowski and Bielecka-Dabrowa18 Iron studies were not available in this cohort, which limits the interpretability of the red cell distribution width findings. Therefore, the observed relationship between elevated red cell distribution width and impaired functional status in our Fontan group may be multifactorial—potentially reflecting the combined effects of unmeasured disturbances in iron metabolism and Fontan-specific haemodynamic and systemic factors. We recommend that future studies incorporate comprehensive iron status assessments (e.g., ferritin, transferrin saturation, haemoglobin) to better understand the respective contributions of iron deficiency and Fontan-related mechanisms to red cell distribution width elevation and functional impairment.
Exercise capacity is a well-established determinant of morbidity and mortality in patients with Fontan physiology. Reference Ohuchi, Negishi and Noritake19 Our findings align with previous studies highlighting myopenia and skeletal muscle dysfunction as key contributors to exercise limitation in Fontan patients. Reference Cordina, O’Meagher and Gould3–Reference Tran, D’Ambrosio and Verrall5 Cordina et al. demonstrated that Fontan adults exhibit significant skeletal muscle atrophy, with lean mass deficits correlating with reduced peak oxygen consumption. Reference Cordina, O’Meagher and Gould3 Similarly, Tran et al. identified a “myopenic profile” in Fontan patients, characterised by lower appendicular lean mass and impaired muscle metabolism, which strongly predicted exercise intolerance. Reference Tran, D’Ambrosio and Verrall5 Powell et al. further supported these findings, reporting that skeletal muscle mass was positively associated with peak oxygen uptake and oxygen pulse, underscoring the importance of preserving muscle integrity to optimise cardiovascular performance. Reference Powell, Wittekind and Alsaied4 Similarly, in our previous case–control study evaluating Fontan patients, quadriceps isometric muscle strength was significantly lower in Fontan patients than in controls (25.53 ± 8.12 kg vs. 33.04 ± 12.04 kg, p = 0.043), despite comparable body composition. Furthermore, both submaximal (6MWT: 583.95 ± 99.18 m vs. 692.79 ± 94.87 m, p = 0.001) and maximal (ISWT: 622.00 ± 192.15 m vs. 838.57 ± 200.13 m, p = 0.001) exercise capacities were markedly reduced in the Fontan group. Reference Tekerlek, Saglam and Kucukdagli20 These findings highlight the importance of peripheral muscle function in exercise performance and support the role of targeted interventions aiming to preserve or improve skeletal muscle strength in Fontan patients. Consistent with these reports, our finding of a positive correlation between handgrip strength and 6MWT distance suggests that greater muscle strength is associated with better physical performance in our study. Given the reliance of Fontan physiology on peripheral muscle function to augment venous return, skeletal muscle health emerges as a critical determinant of overall functional capacity.
Alterations in body composition, including reduced lean mass, have been documented in Fontan patients and may further compromise exercise performance. Reference Tran, D’Ambrosio and Verrall5,Reference van den Berg, Pos, Scheffers, van den Berg and Helbing7 A systematic review by van den Berg et al. found that Fontan patients often exhibit higher fat mass and lower skeletal muscle mass compared to healthy controls, despite a normal body mass index. Reference van den Berg, Pos, Scheffers, van den Berg and Helbing7 This paradox suggests that body mass index alone is insufficient for assessing functional status in this population. Our findings are consistent with previously published studies, demonstrating that fat-free mass positively correlates with exercise capacity and handgrip strength, whereas reduced fat-free mass may exacerbate exercise limitation. These findings support the notion that preserving muscle integrity can enhance exercise tolerance in Fontan patients. In clinical practice, exercise prescription for Fontan patients is often based on laboratory tests such as cardiopulmonary exercise testing. However, the positive association between handgrip strength and 6MWT distance in our study suggests that simple field tests may also have clinical value for monitoring and guiding rehabilitation. The 6MWT, which we have previously shown to be a practical tool in this population, Reference Tekerlek, Saglam and Kucukdagli20 may serve as a useful complement to handgrip strength in identifying patients with reduced peripheral muscle function who could benefit from targeted resistance or combined training programmes.
In a previous longitudinal study, we observed that exercise capacity and muscle strength remained stable over a 20-month follow-up period, whereas body mass index and fat weight increased during somatic growth. Reference Tekerlek, Sağlam and Selçuk21 These findings indicate that even without measurable declines in muscle strength, changes in body composition may still influence functional performance. The current correlation between 6MWT distance and fat-free mass further supports the potential role of 6MWT as a clinically relevant indicator for designing and adjusting individualised exercise programmes in Fontan patients. Overall, these observations underscore the need to preserve skeletal muscle integrity through structured, resistance-based, and personalised rehabilitation to enhance venous return, maintain functional capacity, and support long-term cardiovascular health. Reference Cordina, O’Meagher and Gould3
Oxygen desaturation following exertion is a key indicator of circulatory efficiency in Fontan patients, reflecting their limited ability to meet increased metabolic demands during exercise. In our study, greater post-exercise desaturation was associated with a shorter 6MWT distance (r = −0.531, p = 0.008) and lower handgrip strength (r = −0.472, p = 0.017). A significant negative correlation was observed between ΔSpO2 and both 6MWT distance and handgrip strength, suggesting that greater post-exercise desaturation is associated with reduced endurance and muscle strength. These findings are consistent with prior research indicating that oxygen delivery limitations in Fontan physiology contribute to exercise intolerance and increased cardiovascular morbidity. Reference Russell, Moldenhauer and Rychik22 In our study, while Fontan type and fenestration status were not significantly associated with 6MWT distance, patients with intra-extracardiac Fontan and fenestration exhibited higher oxygen desaturation. This may be explained by the fact that our clinic recently preferred the intra-extracardiac Fontan modification and routinely performed fenestration in this modification, in contrast to previous techniques. Therefore, the finding of higher oxygen desaturation in patients with surgical fenestration can be interpreted as an expected situation. Exercise-induced desaturation can be explained by two distinct mechanisms other than ventricular dysfunction. One factor is the presence of fenestration, which, as expected, was associated with significantly greater desaturation compared to patients without fenestration. In addition to fenestration, the development of veno-venous collaterals may indicate a compensatory response to increased central venous pressure and serve as an indicator of adverse Fontan haemodynamics. Reference Sugiyama, Yoo, Williams and Benson23 Their presence may reflect inefficient circulation and systemic venous congestion, which could contribute to reduced exercise capacity and progressive cardiovascular dysfunction. Over time, this may further impair circulatory efficiency and potentially represent an early marker of clinical deterioration.
Limitations
This study has several limitations. The relatively small sample size may have limited the statistical power to detect certain associations, underscoring the need for larger, multicentre studies to validate our findings. The heterogeneity in patient age and the evolution of Fontan subtypes over time precluded direct comparisons between groups. Paediatric and adult Fontan patients may differ in cumulative haemodynamic burden and age-related changes in muscle and organ function; these differences should be considered when interpreting functional outcomes. Furthermore, due to changes in the hospital’s electronic medical record system over the years, access to some historical clinical data was restricted, which may have influenced the assessment of disease progression and functional outcomes. The absence of iron status evaluation limits the interpretability of elevated red cell distribution width and its potential association with functional impairment. Future studies should incorporate iron parameters to better clarify the interplay between red cell distribution width, iron metabolism, and exercise capacity, while also prioritising longitudinal assessments of targeted interventions aimed at improving muscle preservation, cardiovascular health, and quality of life in the Fontan population.
Conclusion
Our findings suggest that functional capacity in the Fontan population is associated with extracardiac factors, particularly skeletal muscle strength, fat-free mass, and exercise-induced oxygen desaturation. Incorporating simple functional and muscle strength assessments into routine follow-up may facilitate detection of functional decline and help guide individualised long-term management.
Data availability statement
All authors accept responsibility for the reliability and objectivity of the data presented and its interpretation.
Financial support
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Competing interests
The authors have no relevant financial or non-financial interests to disclose.
Ethical standard
Hacettepe University Ethical Board approved this study (16969557-2187, December 2019).



 Open access
Open access