


Introduction
Anomalous origin of the left coronary artery from the pulmonary artery, also referred to as Bland-White-Garland syndrome, is a rare congenital anomaly in which the left coronary artery arises abnormally from the pulmonary artery instead of the aorta. Reference Pena, Nguyen, Merchant and Dennie1 Without timely intervention, this defect can lead to myocardial ischaemia, left ventricular dysfunction, mitral regurgitation, and ultimately death during infancy or early childhood.
The preferred surgical management involves re-establishing a two-coronary system. Direct coronary reimplantation (translocation) into the aorta is widely regarded as the optimal technique due to its anatomical and physiological restoration of coronary flow, and is associated with favourable outcomes. Reference Past2 However, in certain cases where the origin of the left coronary artery is distant from the aorta or arises from a non-facing sinus, direct transfer may be technically infeasible without risking coronary tension, distortion, or haemorrhage. Reference Hoashi, Kagisaki, Okuda, Shiraishi, Yagihara and Ichikawa3
In such anatomically challenging scenarios, the Takeuchi procedure offers a valuable alternative. This technique involves the creation of an intrapulmonary tunnel (or baffle) that redirects oxygenated blood from the aorta to the anomalous coronary ostium via an aortopulmonary window. Although effective in re-establishing dual-coronary perfusion, the Takeuchi repair is associated with unique long-term complications, including baffle leaks and pulmonary artery stenosis. Reference Yuan, Li and Sun4
This study aims to evaluate the mid- to long-term outcomes of the Takeuchi repair for anomalous origin of the left coronary artery from the pulmonary artery at a single tertiary centre. Specifically, we assess survival, functional recovery, left ventricular function, and the incidence of late complications and reinterventions during follow-up.
Materials and methods
Study design and patient selection
This retrospective, single-centre study included paediatric patients (≤18 years of age) who underwent the Takeuchi procedure for the repair of anomalous origin of the left coronary artery from the pulmonary artery at our institution between 2007 and 2023. Patient selection was based on operative reports, institutional surgical databases, and imaging-confirmed diagnosis of anomalous origin of the left coronary artery from the pulmonary artery. The study period of 2007 to 2023 was selected because it marks the beginning of our institutional experience with Takeuchi repairs. All patients undergoing Takeuchi repair during this period were included; no cases were excluded.
Preoperative, intraoperative, and postoperative data were collected, including age at surgery, body weight, body surface area, sex, New York Heart Association functional class, presence of mitral regurgitation, left ventricular ejection fraction, need for preoperative mechanical ventilation or inotropic support, and surgical details. Patients were followed postoperatively via hospital records, national health database queries, and structured telephone interviews with caregivers or follow-up physicians.
Imaging and surgical approach
All patients underwent transthoracic echocardiography, and those who were clinically stable were evaluated with CT angiography to assess coronary anatomy. The Takeuchi procedure was chosen when the left coronary artery originated from a remote or non-facing sinus position, making direct aortic translocation technically unfeasible.
The surgical approach included median sternotomy and establishment of moderate hypothermic cardiopulmonary bypass via ascending aortic and bicaval venous cannulation. Left atrial decompression was achieved through the right superior pulmonary vein. After aortic cross-clamping, antegrade Buckberg cardioplegia (30 mL/kg) was administered via the aortic root, followed by additional cardioplegia through the anomalous origin of the left coronary artery from the pulmonary artery ostium after pulmonary arteriotomy.
An aortopulmonary window was created, and an intrapulmonary tunnel was fashioned using fresh autologous pericardium to redirect oxygenated blood from the aorta to the left coronary artery. Following patency testing with blood cardioplegia, the pulmonary arteriotomy was closed either primarily or with a pericardial patch based on arterial dimensions and surgeon discretion.
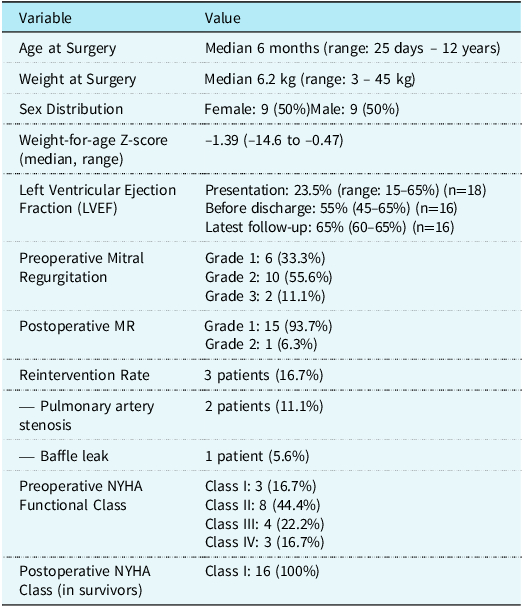
Demographic, Preoperative, and Follow-up Characteristics of Patients Undergoing Takeuchi Repair for ALCAPA

LVEF = Left Ventricular Ejection Fraction; MR = Mitral Regurgitation; NYHA = New York Heart Association.
Postoperative evaluation and follow-up
Echocardiographic assessment was performed during early postoperative recovery and at follow-up visits. Evaluations included left ventricular ejection fraction, mitral regurgitation grade, tunnel patency, pulmonary artery flow gradients, and the presence of aneurysm or baffle leaks. Functional class was documented according to New York Heart Association classification.
Complications and reinterventions, including those for pulmonary artery stenosis or baffle leaks, were recorded. Follow-up duration was calculated from the date of the primary operation to the last clinical contact or death.
Ethical consideration
The study was approved by the institutional ethics committee (Approval number: 23-11.1T/32), and conducted in accordance with the Declaration of Helsinki. Written informed consent for data usage was obtained during follow-up where applicable
Statistical analysis
Statistical analyses were conducted using Jamovi for Mac (version 2.5.2, The Jamovi Project, Sydney, Australia). Continuous variables were expressed as medians with ranges, given the non-normal distribution of most parameters. Categorical variables were presented as absolute numbers and percentages.
To assess paired changes in pre- and postoperative continuous and ordinal variables, the Wilcoxon signed-rank test was used due to the non-normal distribution of the data. Specifically, this test was applied to evaluate changes in left ventricular ejection fraction and mitral regurgitation grade among surviving patients. A two-sided p-value of <0.05 was considered statistically significant.
Survival analysis and freedom from reintervention were evaluated using the Kaplan–Meier method. The time-to-event was calculated in years from the date of the Takeuchi operation until the event of interest (death or reintervention), or the last follow-up date for censored patients. The number of patients at risk was reported at standard intervals. Given the relatively small cohort size and limited event numbers, confidence intervals were not calculated to avoid overestimation of statistical precision.
No formal hypothesis testing or multivariate modelling was performed due to the limited sample size, which restricts the power to detect significant associations. Descriptive statistics and survival estimates were emphasised instead to characterise outcomes and identify trends over the follow-up period.
Results
Patient demographics and preoperative characteristics
A total of 18 paediatric patients underwent the Takeuchi procedure for anomalous origin of the left coronary artery from the pulmonary artery between 2007 and 2023. The median age at surgery was 6 months (range: 1 month to 12 years), and the median body weight was 6.25 kg (range: 3 to 45 kg). The median preoperative left ventricular ejection fraction was 31% (range: 15–65%). Preoperative mitral regurgitation was present in all patients: 55.6% had grade 2 mitral regurgitation (n = 10), 33.3% had grade 1 (n = 6), and 11.1% had grade 3 (n = 2).
Preoperative clinical deterioration was common: five patients (27.8%) were intubated preoperatively, and three patients (16.7%) presented with New York Heart Association functional class IV status and required inotropic support. No patients were supported with extracorporeal membrane oxygenation prior to surgery. Preoperative demogragphic and postoperative results were summarized at Table1.
Operative findings
Fresh autologous pericardial patch was used for pulmonary artery closure in 12 patients (66.7%), while primary closure was performed in six patients (33.3%). No patients underwent concurrent mitral valve repair.
Mortality and survival outcomes
Early postoperative mortality occurred in two patients (11.1%). Both patients were under one year of age, preoperatively intubated, and classified as New York Heart Association class IV. The first patient was 3 months old, weighed 4.2 kg, had a preoperative left ventricular ejection fraction of 17%, and moderate (grade 2) mitral regurgitation. The second patient was 5 months old, weighed 5.1 kg, had a preoperative left ventricular ejection fraction of 15%, and severe (grade 3) mitral regurgitation. Postoperative echocardiography in both patients showed functional intrapulmonary tunnels with preserved coronary flow, but progressive low cardiac output led to multiorgan failure. Despite maximal medical therapy, their condition deteriorated. Extracorporeal membrane oxygenation was considered but not initiated due to rapid clinical decline and poor overall prognosis
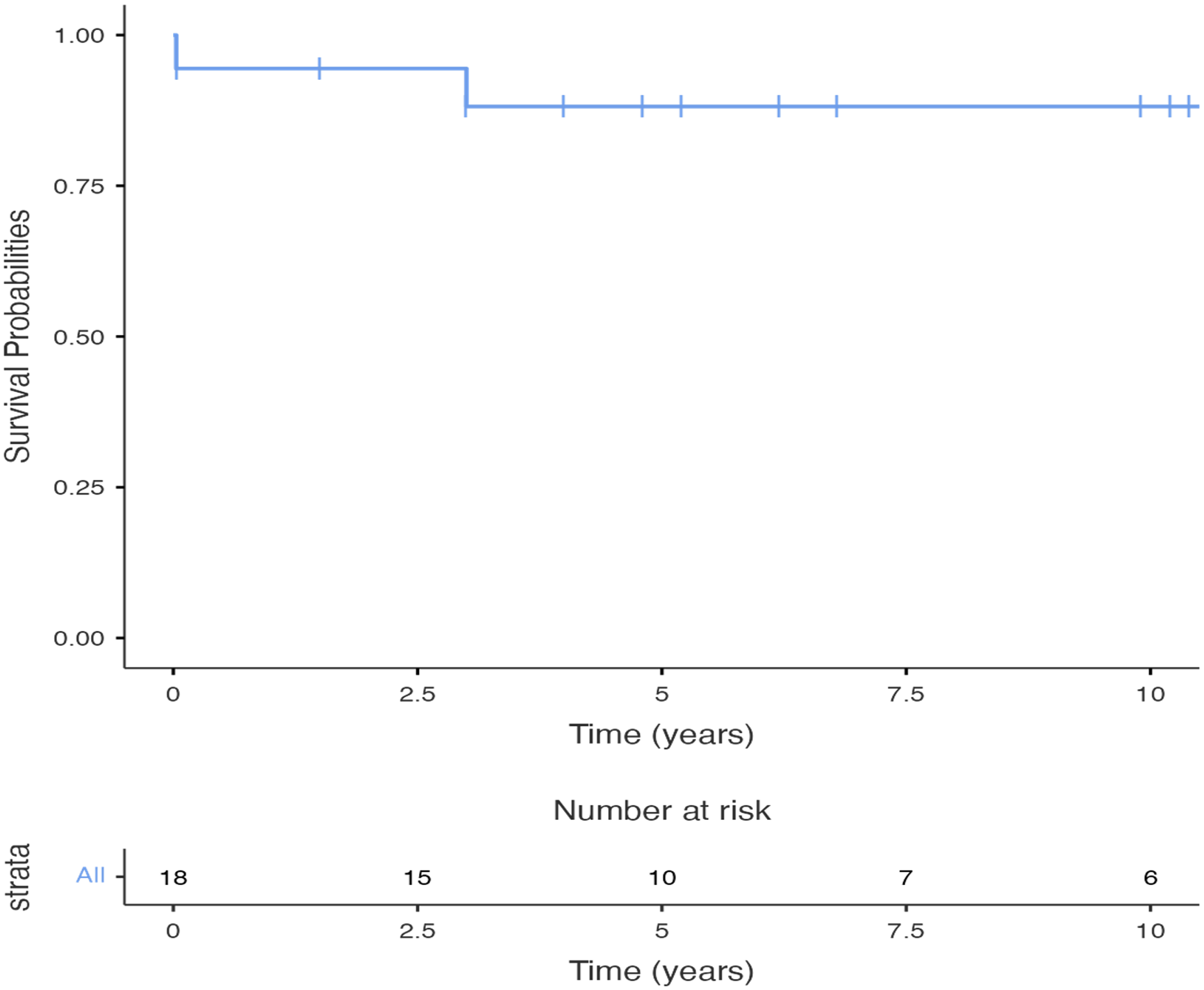
No late mortality was observed during follow-up. The maximum follow-up period in surviving patients was 10.9 years. The Kaplan–Meier estimated survival at 1 and 10 years was 88.9%, with no deaths occurring beyond the early postoperative period (Fig 1)
Kaplan–Meier curve demonstrating the probability of overall survival following the Takeuchi procedure for anomalous origin of the left coronary artery from the pulmonary artery. Two early deaths occurred within the first month postoperatively. No late mortality was observed during follow-up.

Left ventricular function and functional recovery
Among the 16 surviving patients, statistical comparison confirmed a significant improvement in left ventricular function. The median left ventricular ejection fraction increased from 23.5% (IQR 15–65%) preoperatively to 65% (IQR 60–65%) at late follow-up. A Wilcoxon signed-rank test demonstrated this increase to be statistically significant (p < 0.0001)
Mitral regurgitation outcomes
Similarly, mitral regurgitation grade showed a significant postoperative reduction. Preoperatively, 66.7% of patients had moderate to severe mitral regurgitation (grade 2 or 3), whereas postoperatively, 94.4% had only mild mitral regurgitation (grade 1), with no worsening in any case. The reduction in mitral regurgitation grade was statistically significant (p < 0.001).
Reinterventions and late complications
Reintervention was required in three patients (16.7%). Two patients underwent pulmonary artery reconstruction due to progressive stenosis at 3 and 8.4 years after the initial surgery. One patient required surgical revision for a baffle leak identified 2.6 years postoperatively, associated with a decline in left ventricular ejection fraction. The leak was repaired via direct suture closure during a reoperation (Figs 2 and 3). The baffle leak in this patient was not identified during early postoperative follow-up imaging, including echocardiography at discharge and subsequent outpatient visits, suggesting that it likely developed in the later postoperative period. The delayed presentation, coupled with associated decline in ventricular function, indicates the possibility of late structural degradation or suture line dehiscence rather than a primary intraoperative technical issue. No similar complications were observed in other patients, and surgical revision was successful.
Transthoracic echocardiographic image showing intrapulmonary baffle leak. The leak was visualised as colour Doppler flow between the aorta (AO) and pulmonary artery (PA).

Intraoperative view during surgical reintervention for baffle leak. The yellow circle indicates the site of the defect in the intrapulmonary tunnel. (PA: pulmonary artery).

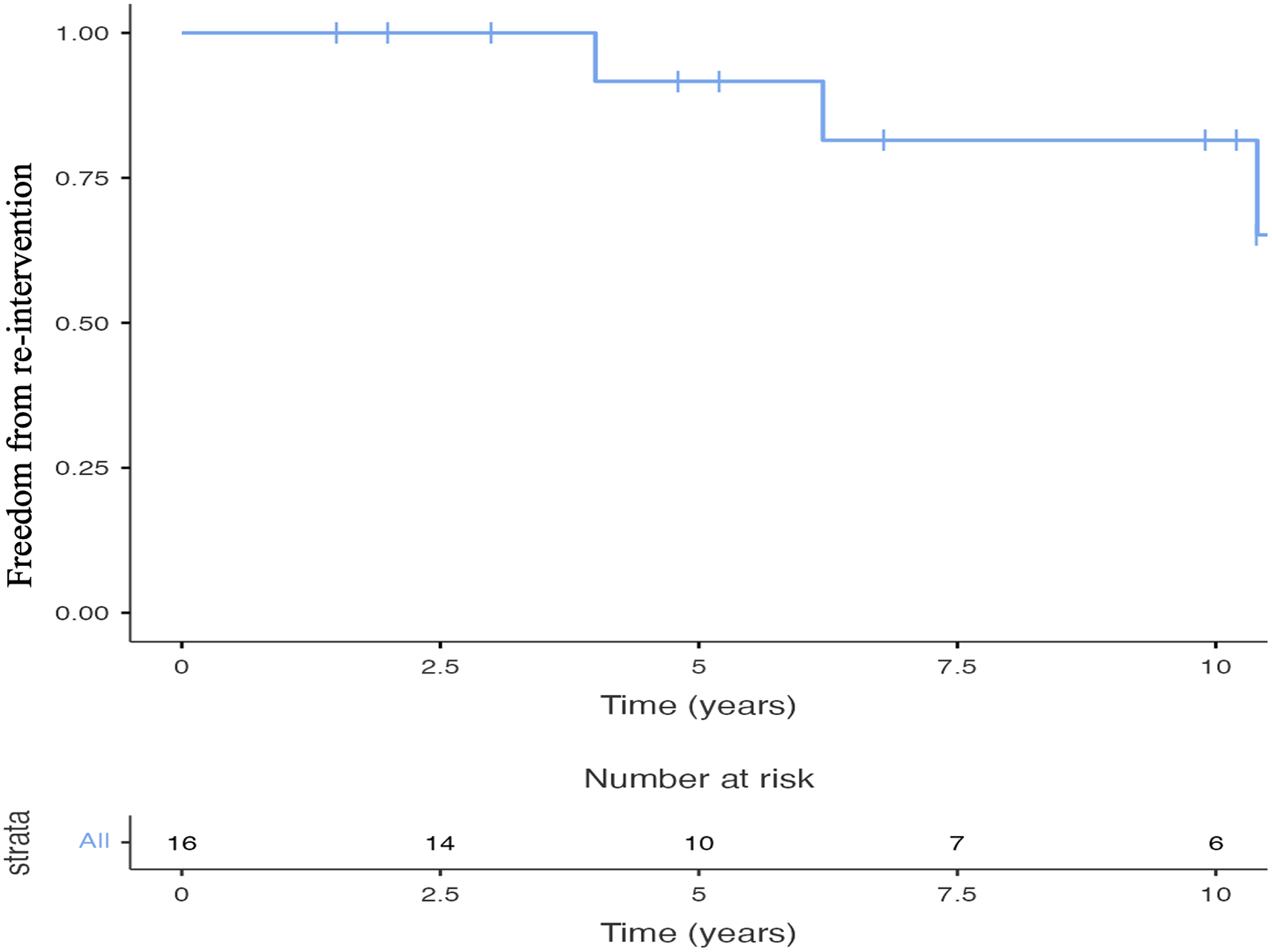
The estimated freedom from reintervention was 100% at 1 year, 83.3% at 5 years, and 66.7% at 10.9 years. These outcomes are presented in the Kaplan–Meier curve in Figure 4.
Kaplan–Meier curve showing the probability of freedom from reintervention following the Takeuchi procedure. Reintervention was required in three patients at 2.6, 3, and 8.4 years postoperatively. Freedom from reintervention was 100% at 1 year, 83.3% at 5 years, and 66.7% at 10.9 years.

Discussion
The Takeuchi procedure remains an essential surgical option for the repair of anomalous origin of the left coronary artery from the pulmonary artery in patients for whom direct coronary translocation is not anatomically feasible. In our cohort, the procedure demonstrated excellent mid- to long-term survival and functional recovery, with a low incidence of serious complications and reinterventions.
Survival and functional recovery
Our observed survival rate of 88.9% over a maximum follow-up duration of 10.9 years is consistent with prior reports that document early mortality in the range of 10–15% for high-risk paediatric patients undergoing anomalous origin of the left coronary artery from the pulmonary artery repair. Reference Hoashi, Kagisaki, Okuda, Shiraishi, Yagihara and Ichikawa3,Reference Ginde, Earing, Bartz, Cava and Tweddell5,Reference Yokohama, Toh and Kotani6 Notably, both deaths in our cohort occurred within the first month after surgery and were associated with severe preoperative heart failure requiring intubation and inotropic support.
Importantly, all surviving patients recovered to New York Heart Association class I functional status and demonstrated substantial improvement in left ventricular ejection fraction, which increased from a preoperative median of 31% to over 50% at follow-up. Our quantitative analysis confirmed this improvement to be statistically significant (p < 0.0001), supporting the notion that restoration of dual coronary circulation leads to meaningful recovery of myocardial function. These findings underscore the capacity of the Takeuchi repair to restore adequate myocardial perfusion and support long-term ventricular recovery, even in patients with initially depressed function. Reference Akkaya, Bilen, Tuncer, Ayik and Atay7– Reference Zhang, Zhang and Yan10
Mitral regurgitation
Mitral regurgitation is commonly associated with ischaemic left ventricular dysfunction in patients with anomalous origin of the left coronary artery from the pulmonary artery. While some studies report that preoperative mitral regurgitation may persist despite successful coronary repair, Reference Bicer, Korun and Yurdakok11 none of the patients in our cohort had persistent moderate or severe mitral regurgitation during follow-up, and 94.4% demonstrated only mild residual regurgitation. This supports the notion that mitral regurgitation in anomalous origin of the left coronary artery from the pulmonary artery is typically functional rather than structural and may resolve with normalisation of ventricular dimensions and function. Reference Akkaya, Bilen, Tuncer, Ayik and Atay7,Reference Yu, Ren and Chen12
Reinterventions and late complications
Three patients required reintervention during follow-up. Two underwent surgical reconstruction for pulmonary artery stenosis, while one underwent repair of an intrapulmonary baffle leak.
Our reintervention rate of 16.7% compares favourably to the findings reported by Radman et al. (2021), a multi-institutional study that documented a higher reintervention incidence among patients undergoing the Takeuchi procedure. One possible explanation is our routine use of preoperative CT angiography for surgical planning, which may improve anatomical selection and baffle construction. Additionally, our institution has developed substantial experience with the Takeuchi technique over the past 16 years, reflected in the higher proportion of Takeuchi repairs compared to direct coronary transfer. This likely reflects both surgeon preference and case selection based on coronary anatomy. These factors may account for our relatively low complication rate and favourable long-term outcomes. Reference Radman, Mastropietro and Costello13
Pulmonary artery stenosis is a well-recognised late complication of the Takeuchi procedure, typically attributed to patch-related scarring, tension, or adverse remodelling at the site of arteriotomy closure. Reference Ginde, Earing, Bartz, Cava and Tweddell5 In our series, both affected patients had either primary closure or patch repair, suggesting that individual anatomy and postoperative healing responses may play a role in stenosis development. The observed pulmonary gradients remained modest (≤15 mmHg) in the rest of the cohort, and no routine interventions were necessary.
Baffle leaks represent another important concern, given their potential to compromise coronary perfusion and precipitate ventricular dysfunction. In our study, one patient was diagnosed with a baffle leak during routine echocardiographic follow-up prompted by a decline in left ventricular ejection fraction. Prompt surgical revision was successful, with complete recovery. Previous reports suggest baffle leak rates of up to 27%, highlighting the need for meticulous surgical technique and vigilant postoperative imaging. Reference Ginde, Earing, Bartz, Cava and Tweddell5,Reference Yokohama, Toh and Kotani6,Reference Kwiatkowska, Herrador Rey and Meyer-Szary14,Reference Naqvi, Joynt, Prasad and Ling15
No arrhythmias were reported in our cohort during follow-up. However, given the known risk of conduction disturbances following anomalous origin of the left coronary artery from the pulmonary artery repair—particularly with intrapulmonary tunnelling—routine rhythm monitoring remains advisable. Reference Neumann, Sarikouch and Bobylev16
Clinical implications
Our findings reinforce the role of the Takeuchi procedure as a safe and effective alternative to coronary translocation in selected patients with complex coronary anatomy. Key factors in optimising outcomes include accurate preoperative imaging (preferably CT angiography), intraoperative judgment to determine suitability for baffle creation, and vigilant long-term follow-up to detect potential complications.
Routine preoperative CT angiography was a standard part of our institutional protocol since 2007. Compared to transthoracic echocardiography, CT angiography provided superior spatial resolution and detailed visualisation of the anomalous coronary origin, its course, and the relationship to adjacent structures. This allowed for more accurate surgical planning and better identification of patients anatomically suitable for Takeuchi repair. We believe that the routine use of CT angiography contributed to our relatively low reintervention rate and consistent postoperative outcomes.
The consistent functional recovery and stable postoperative left ventricular ejection fraction observed in our cohort also suggest that routine mitral valve intervention may not be necessary unless structural abnormalities are evident.
Several factors may explain the favourable outcomes observed in our cohort. First, the surgical procedures were performed by a limited number of experienced congenital heart surgeons using a standardised technique, reducing variability. Second, the routine use of preoperative CT angiography likely enhanced surgical planning and appropriate case selection. Third, our institution’s postoperative care protocols emphasise early haemodynamic optimisation, vigilant monitoring, and structured follow-up, which may have contributed to the absence of late mortality and preserved ventricular function. Finally, patient selection may have played a role, as patients with significant extracardiac comorbidities or complex syndromes were rarely referred for surgical intervention at our centre.
Study limitations
This study is limited by its retrospective, single-centre design and small sample size, which may restrict generalizability. Additionally, the limited number of events precludes meaningful multivariable analysis to identify risk factors for complications. Despite these limitations, the long follow-up duration and consistency of outcomes provide valuable insights into the durability of the Takeuchi procedure.
Conclusion
The Takeuchi procedure remains a valuable and reliable surgical option for the repair of anomalous origin of the left coronary artery from the pulmonary artery in cases where direct coronary translocation is anatomically unfeasible. In our single-centre experience, the procedure demonstrated excellent mid- to long-term survival and functional recovery, even among patients presenting with severe preoperative ventricular dysfunction.
Despite its effectiveness, the procedure carries a moderate risk of late complications, most notably pulmonary artery stenosis and baffle leaks, both of which may necessitate reintervention. However, with careful surgical technique, appropriate patient selection, and regular long-term follow-up, these complications can be identified early and managed successfully.
Given the favourable outcomes observed in our cohort—with stable left ventricular function, improved mitral regurgitation, and no late mortality—the Takeuchi procedure should continue to be considered a safe and effective alternative in the surgical management of ALCAPA in select paediatric patients.



 Open access
Open access