

1. Introduction
Pharmaceutical waste (PW) is a significant environmental, economic and public health concern that arises from various stages of the pharmaceutical lifecycle including manufacturing, distribution, consumption and disposal. The World Health Organisation defines pharmaceutical waste as: “Pharmaceuticals and items that are expired or no longer needed, or contaminated by or contain those contaminated molecules” (WHO, 2024). This definition includes tablets and capsules, syrups, injections, IV fluid bags, infusion sets, dressings, adhesive plasters, packaging If it is expired, no longer required, or contaminated, it is PW.
Some waste is inevitable, such as waste arising from patient recovery, patient death, changes to medication, and use by dates there is some. However, there is significant waste that is avoidable, such as through stock piling and habitual dispensing (Reference Hazell and RobsonHazell and Robson, 2015). Pharmaceutical waste has received increasing attention within healthcare sustainability agendas. This research is part of the Design HOPES (Healthy Organisations in a Place-based Ecosystem, Scotland) project, that aims to develop healthcare approaches in context of National Health Service (NHS) Scotland through design. It is a transdisciplinary research cohort-project that exploits the potential of design-led thinking and making to innovate and tackle multifaceted health delivery challenges to meet urgent Net Zero goals for a sustainable health and social care system. In this paper, we take a design-led and behaviourally informed approach that addresses the social, cultural and practical factors that are influencing wasteful medicine use and disposal behaviours. To this end, it reports on the use of co-design to support the development of effective interventions to reduce PW.
2. Background
This section reviews existing literature on the economic, health and environmental impacts of PW to establish the need for behaviourally driven and design-led strategies to mitigate PW.
2.1. Economic impact of pharmaceutical waste
According to NHS Greater Glasgow and Clyde (n.d) 10% of the medicines that are dispensed go to waste. Although people in Scotland are not charged for their prescription medication, each item still costs the NHS £11 on average. This equates to an estimated £100,000 per day in Greater Glasgow and Clyde alone. In Scotland, pharmaceutical expenditure has increased, reaching a total of £1.76 billion in 2019 (Reference Alejandre, Frascaroli, Escudero, Pahl, Price, Pfleger and HelwigAlejandre et al., 2022). This represents 16.1% of the total NHS health budget. Beyond procurement costs, additional financial burdens arise from storage, distribution and high-temperature incineration required for disposal. As medicine costs continue to rise, the economic implications of avoidable waste are likely to increase further. Currently, the cost of waste in NHS GGC equates to a day’s wages for more than 700 nurses a day, or more than 200 hospital consultants a day (NHS Greater Glasgow & Clyde, n.d). This highlights the significant economic opportunity cost and the need for improved strategies to ensure NHS resources are used as efficiently as possible.
2.2. Health impact of pharmaceutical waste
Prescribing pharmaceuticals is the most commonly used healthcare intervention and plays a critical role in maintaining and improving human health. However, the risks associated with overprescribing, polypharmacy and the improper management of medicines are increasingly recognised (ATACH Community, 2026). When pharmaceutical substances enter the environment, they contribute to the growing global threat of antimicrobial resistance (AMR) (Reference Rogowska and ZimmermannRogowska and Zimmermann, 2022). The presence of antimicrobials in soil and water systems has been linked to the development and spread of resistant bacterial strains. Antimicrobial resistance was associated with approximately 4.5 million deaths worldwide in 2019 (Reference Alejandre, Frascaroli, Escudero, Pahl, Price, Pfleger and HelwigAlejandre et al., 2022), underscoring the global health implications of inappropriate prescribing and disposal practices.
At the individual level, health risks also arise from medicine mismanagement within the home. Stockpiling unused medication increases the likelihood of accidental consumption of expired or degraded medicines, particularly among vulnerable populations (Reference Sapkota and PariatambySapkota and Pariatamby, 2023). Medicine-related harm also places a substantial burden on healthcare systems. Estimates suggest that a significant proportion of hospital admissions are associated with adverse drug reactions, medication errors or issues in medicine management, with higher rates observed among older adults and those experiencing polypharmacy (ATACH Community, 2026). In Scotland, medicine-related harm has been reported as a major contributor to avoidable admissions and extended hospital stays. These findings indicate that pharmaceutical waste is closely intertwined with prescribing practices, review processes and everyday medicine management behaviours. Addressing avoidable waste therefore has implications not only for environmental sustainability but also for patient safety and healthcare system resilience.
2.3. Environmental impact of pharmaceutical waste
Improper disposal of unused medicines allows pharmaceutical substances to enter aquatic environments via wastewater systems, posing significant threats to aquatic organisms. As such, pharmaceuticals are not only a major contributor to the healthcare sector’s carbon emissions (Reference Alejandre, Frascaroli, Escudero, Pahl, Price, Pfleger and HelwigAlejandre et al., 2022) but also persist in the environment at concentrations capable of harming ecosystems. These environmentally relevant concentrations have been linked to declines in biodiversity, as they can disrupt the natural balance of aquatic and terrestrial habitats. With new medications continually entering the market, the number of active pharmaceutical ingredients is increasing; over 300 compounds have now been identified as potential contaminants in aquatic environments (Reference Alejandre, Frascaroli, Escudero, Pahl, Price, Pfleger and HelwigAlejandre et al., 2022).
Global antibiotic consumption increased by 65% between 2000 and 2015 (Reference Rogowska and ZimmermannRogowska and Zimmermann, 2022), contributing to their widespread presence in the environment. Such contamination can affect the survival and reproduction of various organisms, altering ecological functions such as biomass production and overall biodiversity (Reference Rogowska and ZimmermannRogowska and Zimmermann, 2022). As such, it is important that when waste is discovered it is disposed of correctly to reduce PW entering the environment. These risks demonstrate the urgency of developing more responsible behaviours around pharmaceutical use and disposal, and highlight the importance of coordinated, system-wide strategies to prevent medicines from entering the natural environment.
3. Methods
Co-design has increasingly been used within healthcare research and practice to increase the possibility for designing and disseminating effective innovations (Reference Vargas, Zorbas, Longworth, Ugalde, Needham, Sunil, Venegas Hargous, Bennett, Forrester-Bowling, Cardoso Richter and AllenderVargas et al., 2025). It is a collaborative approach that involves diverse stakeholders in the design process to address a specific problem (Reference Vargas, Zorbas, Longworth, Ugalde, Needham, Sunil, Venegas Hargous, Bennett, Forrester-Bowling, Cardoso Richter and AllenderVargas et al., 2025). A key benefit of co-design is that it brings stakeholders together to design solutions that reflect local problems, often resulting in solutions that understand and meet local needs and contexts (Reference Jessup, Osborne, Buchbinder and BeauchampJessup et al., 2018). Involving clinicians and people with lived experience ensures that research findings are impactful (Reference Grindell, Coates, Croot and O’CathainGrindell et al., 2022).
This research involved two co-design workshops with healthcare professionals including general practitioners, pharmacists, nurses, carers and members of the public with lived experience of medicine use. The diverse participant group ensured that insights from both high-level and individual perspectives were represented, creating a balance between professional expertise and everyday practice that enabled the generation of insights both systemic in scope and grounded in lived realities. The workshop format was selected as it prioritises the dynamic and provocative exchanges that emerge when participants challenge a status, a question, a debate or a view. Such interactive settings provide a deeper insight into participants’ perspectives, allowing them to uncover underlying assumptions and collectively identify what holds significance for them. Recognised as a valuable tool for data collection and knowledge sharing (Reference Ørngreen and LevinsenØrngreen & Levinsen, 2017), workshops have been employed in various studies to generate and implement ideas within multimethod research approaches (Reference Storvang, Clarke, Mortensen, Freytag, Young and EvaldStorvang et al., 2024). According to Reference Ahmed and AsrafAhmed and Asraf (2018), workshops enhance the credibility and richness of qualitative research by fostering deep participant engagement, collaborative learning, and constructive feedback. In this instance, both workshops were co-organised by the Design HOPES team and NHS Greater Glasgow and Clyde Pharmacy Services. The first workshop aimed to understand the systems and contexts where PW is problematic, while the second workshop focused on co-designing solutions in response.
3.1. Design-led behaviour change interventions
Reducing avoidable PW requires changes in everyday practices of across multiple actors within the healthcare system. These behaviours are shaped by individual knowledge and attitudes, social norms, healthcare system routines, infrastructures and cultural expectations surrounding medicines. As such, interventions aimed at reducing PW must go beyond providing information to address the psychological, social and contextual factors that sustain current behaviours.
To inform this study, we draw on the COM-B model, which is a core component of the behaviour change wheel (BCW). Behaviour change interventions (BCIs) are defined as “coordinated sets of activities designed to change specified behaviour patterns”. Reference Michie, van Stralen and WestMichie et al. (2011) developed COM-B model which identifies three factors that need to be present for any behaviour to occur: capability, opportunity and motivation. ‘Capability’ refers to an individual’s psychological and physical capacity to engage in the behaviour. In this context, this includes understanding the correct disposal routes, being capable of ordering the correct medicine when required, and having the skills to navigate the returns system. ‘Opportunity’ includes external factors that make the behaviour possible. This includes the availability and convenience of medicine return schemes, visibility of disposal points and organisational norms around prescribing and repeat ordering. ‘Motivation’ refers to the internal processes that energise and direct behaviour. This includes beliefs about personal responsibility to reduce PW, perceived value of medicine, attachment to ‘just in case’ stockpiling habits and attitudes towards environmental impact.
3.2. Motivational design for behaviour change
Motivational design approaches, including gamification, have been used across healthcare and public service settings to encourage engagement and support behaviour change. Gamification refers to the application of game design elements in non-game contexts such as feedback loops, progress indicators or structured challenges that make participation more engaging (Reference Deterding, Dixon, Khaled and NackeDeterding et al., 2011). From an interaction design perspective, gamification aligns with the principles articulated by Don Reference NormanNorman (2004) and Bill Reference MoggridgeMoggridge (2007) who emphasise the importance of designing for usability, emotional engagement, and meaningful user experiences. Reference NormanNorman (2004) argues that effective design must appeal to users on visceral, behavioural, and reflective levels. Gamification leverages these dimensions by creating interfaces that are visually stimulating (visceral), functionally rewarding (behavioural), and personally meaningful (reflective). For example, apps like Duolingo and Fitocracy use feedback loops, progress indicators, and social comparison to sustain engagement, reflecting Norman’s notion of “emotional design.”
Reference MoggridgeMoggridge (2007), in his foundational work on interaction design, highlights the role of iterative prototyping and user-centred design in crafting digital experiences. Gamified systems often rely on these principles, adapting mechanics based on user feedback and behavioural data. Gamification also intersects with behavioural economics, particularly through “nudge” theory. One of the most frequently cited examples is that of the ‘urinal fly’ – a feature in use since the 19th century – is a non-coercive intervention that alters behaviour through subtle design. Similarly, products such as spiral wishing well in which the user can watch a coin roll in a spiral motion into a pit – the act providing a sense of fun and satisfaction to giving away money to charity. A similar notion is applied in animal-themed litter bins. These products encourage the depositing of litter by turning the bin into a living being that needs to be ‘fed’. Also, a recent phenomenon ‘blind date with a book’ provides a sense of mystery and fun for consumers in book buying. These examples illustrate how gamified design can transform mundane tasks, such as returning waste medicine or remembering to take medicine, into engaging experiences, leveraging intrinsic and extrinsic motivators to promote desired behaviours.
However, the effectiveness of gamification is contingent upon its alignment with user motivations and contextual goals. Reference KimKim (2015) emphasises the importance of understanding user typologies, drawing on frameworks such as Marczewski’s classification, which includes players, achievers, socialisers, free spirits, and philanthropists. Each type responds differently to game elements, necessitating a design approach that accommodates diverse motivational profiles. Moreover, poorly designed gamification systems may undermine intrinsic motivation, particularly when rewards are perceived as controlling or manipulative (Reference Deci, Koestner and RyanDeci, Koestner, & Ryan, 1999). In Workshop 2, participants were invited to consider how motivational design elements might be incorporated into potential interventions to reduce waste.
3.3. Co-design workshop 1: understanding the system and problems
Twelve participants took part in the first workshop in August, 2025. Participants were recruited through partnership with NHS GGC. Workshop 1 was structured around four sequential activities designed to elicit reflection, dialogue and collaborative idea generation:
-
• Activity 1: “100 Years of Care”
-
• Activity 2: “The Medicine Cabinet”
-
• Activity 3: “What if…”
-
• Activity 4: “Poster Review”
3.3.1. Activity one: “100 years of care”
This activity invited participants to visualise the medical journey across a lifetime as a collective mapping exercise. Working in small, facilitated groups of four, the participants were asked to construct large scale visualisations that captured how medicines intersect with key stages of life including childhood, adulthood and later years. Participants were encouraged to adopt their own visual logic, and were guided by reflective prompts such as: Where do the major obstacles and problems occur? What kinds of waste are produced, and at what points? Who are the people involved, and how do their roles change over time? How is communication handled, and where does it break down?
3.3.2. Activity two: “Medicine cabinet”
Following Activity 1, participants were invited to individually map their personal or observed experiences of medicine use onto a <0-100> year timeline. This exercise encouraged reflection on how encounters with medicines shift across the life course from childhood prescription and family health routines to long-term treatment in adulthood and later years. Participants were provided with pre-cut icons (Figure 2) which represented common medication forms, such as antibiotics, painkillers and treatments for chronic disease, which they could place along the timeline to indicate moments of use, change or discontinuation. In addition to these icons, participants were encouraged to personalise their maps with their own drawings, annotations or written reflection, thereby expressing unique experiences and perceptions of medicine use.
100 years of care activity (left), pre-cut medicine form icons used by participants (right)

Figure 1 Long description
Panel A: A photo of a person drawing on a large sheet of paper with various sketches and a sticky note. The person is holding an orange marker and drawing on a white sheet of paper that is spread out on a table. The paper contains various sketches of medication forms and notes written in different colors. There is a yellow sticky note with handwritten text attached to the paper. Panel B: A diagram illustrating different types of medications. The diagram features various icons representing different forms of medication such as drops, pills, tablets, patches, inhalers, needles, capsules, and creams. Each type of medication is labeled with text pointing to the corresponding icon.
3.3.3. Activity Three: “What if…”
In the third activity, participants were invited to reimagine medicine journeys through the lens of three well-known global brands (Rolex, Amazon and Apple) each selected for the values and systems they represent. Rolex, as an integrated and independent manufacturer represented trust, quality and longevity: Amazon as a global e-commerce and technology enterprise represented efficiency, accessibility and data-driven logistics: and Apple as a global design and technology company reflected integration, simplicity and design-led user experience. These contrasting brand identities served as creative motivators to enable participants to think beyond existing healthcare conventions and to speculate on how such principles could reshape medicine use and reduce waste. To structure their exploration, participants were guided by six key stages of medicines life cycles. At each stage, groups were encouraged to ask: where does waste arise? Where do communication breakdowns occur? How might a different kind of organisation known for quality, convenience or design approach this differently?
3.3.4. Poster review session
A final activity invited participants to review and provide feedback on three public facing posters developed by the Design HOPES team to communicate the issues surrounding PW. Participants were asked to assess each poster using a 1-5 rating scale, guided by questions derived from the Reference Sekhon, Cartwright and FrancisSekhon et al. (2017) indicators of intervention acceptability (affective attitude, burden, ethicality, intervention coherence, opportunity costs, perceived effectiveness, and self-efficacy). Feedback was captured through written comments on sticky notes, and dot stickers on the 1-5 scale.
3.4. Co-design workshop 2: co-designing solutions
Five participants took part in the second workshop in November 2025. This workshop was structured around two activities which aimed to elicit collaboration, conversation and work to design solutions based on the findings of the first workshop.
-
• Activity 1: Discuss the findings from workshop 1
-
• Activity 2: Co-design solutions to challenges identified in workshop 1
3.4.1. Activity 1: discuss findings from workshop 1
The second workshop opened with a session to ensure a shared understanding of the insights generated in workshop1 to agree the problem statement to carry forward into the co-design session. The facilitation team presented a concise synthesis of workshop 1 outputs and invited dialogue from the group to inform activity 2.
3.4.2. Activity 2: co-designing solutions to challenges
Participants were invited to choose a specific waste-related behaviour identified in workshop 1 (such as stockpiling, issues with returning medicine, over-ordering, issues with medication reviews) and analyse it considering the COM-B model. The groups were then asked to determine whether the primary barrier to change lay in capability, opportunity or motivation, ensuring that proposed interventions were grounded in behavioural theory. To support ideation, participants were introduced to principles of motivational design and gamification. Participants were provided with a design canvas and sticky-notes to encourage structured experimentation and design. Each group worked to make explicit links between psychological drivers and design decisions that would be fun and motivate behaviour change.
4. Results
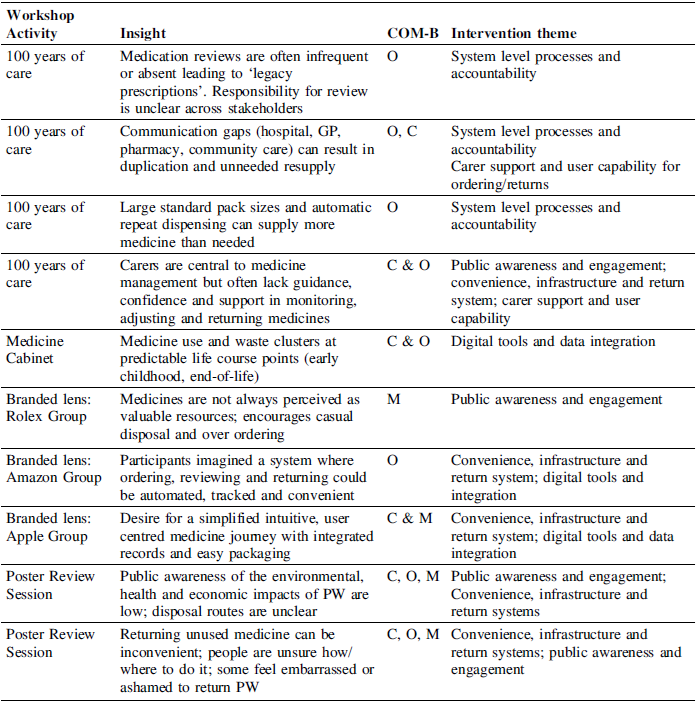
To analyse the workshop outputs, all visual artefacts, written notes and discussion summaries were digitised and collated by researcher 1. An initial round of coding was conducted by researcher 1 to identify recurrent areas, practices and points of tension across the medicine lifecycle. These codes were then reviewed collaboratively with researcher 2, who contributed to refining the coding structure and grouping data into thematic categories aligned with the COM-B framework. Through iterative discussion the two researchers established the thematic clusters presented in Table 1 and developed the accompanying workshop report. Researcher 3 formatted the results for the workshop report.
Participants interacting and discussing during workshop 1

Results from workshop 1

4.1. Results from workshop 1
The findings from workshop 1 highlight that pharmaceutical waste arises through interconnected behavioural, social and systemic challenges. These challenges can be grouped into five overarching thematic categories, which informed the focus of workshop 2:
-
• Theme 1: Public awareness and engagement: there is limited understanding of the environmental economic and health implications of PW, resulting in low motivation to return unused medicines and limited confidence in how to do so properly. Pharmacies identified as last point in the chain before medicine becomes waste therefore opportunity to increase public awareness in the pharmacy setting.
-
• Theme 2: Convenience, infrastructure and return systems: Existing mechanisms for ordering, managing and returning medicines are fragmented, inconsistent and inconvenient, which contributes to stockpiling and discourages responsible disposal.
-
• Theme 3: System level processes and accountability: Structural inefficiencies including unclear responsibility for medication reviews, automatic repeat prescribing and poor communication across settings can create conditions where unnecessary or excess medicines accumulate.
-
• Theme 4: Carer support and user capability: Carers play a significant but often unsupported role in managing medicines and carers may lack the knowledge, confidence or resources needed to monitor, use and adjust supplies or return unused medicines effectively.
-
• Theme 5: Digital tools and data integration: Opportunities to use digital platforms, personalised reminders, automated reviews and transparent tracking are underutilised, limiting the systems ability to optimise supply, monitor adherence and prevent avoidable waste
4.2. Results from workshop 2
Workshop 2 built directly on the thematic areas identified in workshop 1. Participants selected focused areas aligned with their interests and developed concept-level interventions addressing specific behaviours linked to pharmaceutical waste. Across the session, discussions frequently referenced barriers related to opportunities, such as convenience and infrastructure; capabilities such as confidence; and motivation such as value of medicine or engagement with environmental impact. Three developed concepts are described below. While these represent the most fully articulated proposals, additional exploratory ideas also emerged during group work.
-
• ‘Patient Packaging’ (Themes 1 and 2): To address challenges around public engagement, awareness and returns, participants proposed a behaviourally informed intervention using a transparent dispensing bag for receiving medication in the pharmacy. The clear bag would enable patients to visually review all items before leaving. This creates a natural prompt to identify or unnecessary or duplicated medicines and allows items to be declined or returned immediately, preventing them from entering the home as potential waste.
-
• ‘Tactile Communication Tool’ (Theme 3): Participants identified medication reviews as a recurring site where communication breakdowns and unclear responsibility contribute to excess or legacy prescriptions. Discussion highlighted that medicine conversations can feel abstract, hierarchal or rushed, particularly for older adults or carers. In response, one group developed the concept of a tactile, game-like communication tool designed to structure medicine review conversations. The tool was described as a tabletop kit consisting of tokens representing medicines or their effect on the body. This tool could be used during review consultations where clinician and patient would collaboratively move items across the board, discussing each one. Participants likened the format to a simplified board game, noting that structured turn taking could reduce anxiety and hierarchy and make the process more engaging.
-
• ‘Virtual Medicine Cabinet App’ (Themes 4 and 5): A third concept focused on the intersection of carer support and digital infrastructure. Participants developed the idea of a ‘virtual medicine cabinet’ app, designed to visualise, track and support ongoing management of medicines within a caring context. The app could provide a real-time inventory, expiry alters and ordering prompts. To enhance engagement participants suggested integrating gamified features such as progress trackers or avatar-based guidance.
Sketches and note taking from workshop 2

5. Discussion
The co-design approach used in this research demonstrated how design-led and behaviourally informed methods can bring clarity to complex, multi-stakeholder challenges such as pharmaceutical waste. Across the two workshops, participants were supported to first engage in identifying the challenges in reducing waste and second to creatively generate actionable intervention concepts to reduce waste. We approached this issue bottom-up, by beginning with participants experiences and progressing towards collaboratively developed solutions. This ensured that ideas were grounded in everyday realities. A key contribution of this research is the incorporation of motivational design principles within the workshop format. Engaging activities and the introduction of gamification concepts acted as catalysts for idea generation, creating an accessible and participatory atmosphere. Creative tools such as pre-cut icons and idea canvases supported this process, enabling participants to move fluidly between structured analytical exercises in Workshop 1 and speculative, future-oriented ideation in Workshop 2. This sequential design approach fostered ownership and allowed progression from problem exploration to ideation without prematurely narrowing the focus.
From a design research perspective, these workshops exemplify what Nigel Reference CrossCross (1982) termed designerly ways of knowing – an approach grounded in modelling, synthesis, and appropriateness rather than purely scientific empiricism. The integration of motivational design principles demonstrates how tacit, practice-based knowledge can be operationalised to generate actionable insights. While Bruce Reference ArcherArcher (1978) once sought to position design as a branch of science, Reference Galdon and HallGaldon and Hall (2022) highlight the paradox in this view: if design constitutes a distinct culture of thinking, its strength lies not in mimicking science but in embracing its prospective and abductive nature. Our workshops illustrate this by combining a practical-scientific domain (pharmacology) with a designerly approach, leveraging gamification and nudge theory to challenge entrenched assumptions and open new possibilities.
Christopher Reference FraylingFrayling’s (1993) influential framework – Research into, through, and for design – remains relevant here. The activities described align most closely with Research through design, where knowledge emerges from iterative making and reflection. However, as Galdon and Hall argue, this mode must evolve beyond mere documentation to address the “procedural problem” and embrace design’s future-led orientation. In this sense, our approach resonates with Reference SimonSimon’s (1996) notion of exploring how things ought to be, positioning design research as directional and transformational rather than static. By foregrounding abductive reasoning and prospectivity, the workshops contribute to a hybridized research practice that reflects more speculative and ‘open-innovation’ models and advances design’s role in shaping complex, uncertain futures.
6. Conclusion
This study demonstrates the value of a bottom-up, design-led and behaviourally informed co-design approaches in addressing the complex drivers of pharmaceutical waste. By structuring the workshops around visual mapping, speculative prompts and lightly gamified activities, we were able to move beyond high-level system descriptions and uncover detailed, situated behaviours that shape medicine use, management and disposal. These formats encouraged participants to engage more openly, challenge assumptions and explore alternative futures, enabling the extraction of rich insights from a small number of sessions. The concepts generated, including the patient packaging, a tactile communication tool and a virtual medicine cabinet, show how the same motivational and gamified principles used in the engagement process can translate into potential solutions. Each introduces a more interactive, intuitive or confidence-building encounter with medicines, addressing key gaps identified across the COM-B themes. This research shows how playful, design-led methods can support deeper participation, enhance ideation and lead to practical, user-centred interventions that are grounded in lived experience.
Acknowledgement
The authors gratefully acknowledge the support for this work by Future Observatory, the Design Museum’s national research programme for the green transition; and the Arts and Humanities Research Council (grant number AH/Y00373X/1).




 Open access
Open access