


Introduction
Social anxiety disorder (SAD), also known as social phobia, is an early-onset mental disorder characterised by strong fear of social situations in which the individual may be negatively evaluated by others (American Psychiatric Association, 2013). SAD is one of the most common anxiety disorders, with a lifetime prevalence of around 12% (Ruscio et al., Reference Ruscio, Brown, Chiu, Sareen, Stein and Kessler2008), and is associated with significant impairment and societal costs (Patel et al., Reference Patel, Knapp, Henderson and Baldwin2002; Stein et al., Reference Stein, Lim, Roest, de Jonge, Aguilar-Gaxiola, Al-Hamzawi, Alonso, Benjet, Bromet, Bruffaerts, de Girolamo, Florescu, Gureje, Haro, Harris, He, Hinkov, Horiguchi, Hu, Karam, Karam, Lee, Lepine, Navarro-Mateu, Pennell, Piazza, Posada-Villa, Ten Have, Torres, Viana, Wojtyniak, Xavier, Kessler and Scott2017; Vilaplana-Pérez et al., Reference Vilaplana-Pérez, Pérez-Vigil, Sidorchuk, Brander, Isomura, Hesselmark, Kuja-Halkola, Larsson, Mataix-Cols and Fernández de la Cruz2021).
Epidemiological studies suggest an increased risk of mortality due to both natural and unnatural causes of death in individuals with anxiety disorders (Meier et al., Reference Meier, Mattheisen, Mors, Mortensen, Laursen and Penninx2016; Plana-Ripoll et al., Reference Plana-Ripoll, Pedersen, Agerbo, Holtz, Erlangsen, Canudas-Romo, Andersen, Charlson, Christensen, Erskine, Ferrari, Iburg, Momen, Mortensen, Nordentoft, Santomauro, Scott, Whiteford, Weye, McGrath and Laursen2019; Weye et al., Reference Weye, Momen, Christensen, Iburg, Dalsgaard, Laursen, Mortensen, Santomauro, Scott, Whiteford, McGrath and Plana-Ripoll2020; Russell et al., Reference Russell, Minhas, Chandan, Subramanian, McCarthy and Nirantharakumar2023). Fewer studies have focused specifically on mortality in SAD, and results have been mixed. A US-based study using data from the Epidemiologic Catchment Area Program showed no significantly increased risk of death in SAD (adjusted proportional hazard ratio [HR], 1.08; 95% confidence interval [CI] 0.89–1.32) when comparing 324 individuals with the disorder (105 deceased during the study period) with people without the disorder (Eaton et al., Reference Eaton, Roth, Bruce, Cottler, Wu, Nestadt, Ford, Bienvenu, Crum, Rebok, Anthony and Munoz2013). Similarly, in a German study including 77 individuals with SAD (10 deceased), their time to death was not significantly shorter, compared to the general population (adjusted HR, 1.29; 95% CI 0.68–2.42) (John et al., Reference John, Rumpf, Hanke and Meyer2020). In contrast, a Danish register-based study reported an adjusted mortality rate ratio of 1.50 (95% CI 1.20–1.84) for all causes of death, 1.51 (95% CI 1.21–1.85) for natural causes, and 2.19 (95% CI 1.70–2.77) for unnatural causes in individuals with SAD, compared with the general population (Meier et al., Reference Meier, Mattheisen, Mors, Mortensen, Laursen and Penninx2016). However, deaths due to specific causes within these broader categories were not reported. Because SAD is associated with certain risk behaviours (e.g., alcohol misuse, cannabis dependence) (Buckner et al., Reference Buckner, Schmidt, Lang, Small, Schlauch and Lewinsohn2008; Rosenström and Torvik, Reference Rosenström and Torvik2023), which are in turn associated with various somatic conditions, a more detailed understanding of the causes that contribute to the excess mortality due to natural causes in this group is warranted. Additionally, previous research has established an association between SAD and suicidal ideation and suicide attempts (Thibodeau et al., Reference Thibodeau, Welch, Sareen and Asmundson2013; Buckner et al., Reference Buckner, Lemke, Jeffries and Shah2017; Leigh et al., Reference Leigh, Chiu and Ballard2023), but studies focusing on suicide deaths are rare. One Taiwanese study reported a 3-fold increased risk of suicide in a cohort of over 15,000 individuals with SAD, compared with population controls (Wei et al., Reference Wei, Tsai, Cheng, Chang, Bai, Su, Chen and Chen2025), but studies in other populations and contexts are lacking.
In this population-based matched cohort and sibling cohort study, we estimated the risk of all-cause and cause-specific mortality in over 57,000 individuals with SAD, compared with a cohort of demographically matched unexposed individuals. Models adjusted for sociodemographic covariates and other psychiatric disorders. We hypothesised that adjusting for other psychiatric disorders would attenuate, but not eliminate, the magnitude of the associations. To further adjust for unmeasured familial confounding, we employed a sibling control design comparing SAD-exposed individuals with their unexposed full siblings.
Methods
The Swedish Ethical Review Authority approved the study. Informed consent for register-based studies is waved because participants are not identifiable. The reporting follows the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Data sources
Several Swedish population-based registers were linked through the unique identification number assigned to each Swedish citizen (Ludvigsson et al., Reference Ludvigsson, Otterblad-Olausson, Pettersson and Ekbom2009), including: (1) the National Patient Register (NPR), containing diagnostic information based on the International Classification of Diseases (ICD), with coverage for inpatient psychiatric diagnoses from 1973 and for outpatient consultations in specialised care from 2001 (Ludvigsson et al., Reference Ludvigsson, Andersson, Ekbom, Feychting, Kim, Reuterwall, Heurgren and Olausson2011); (2) the Cause of Death Register, including dates of death and codes for underlying and contributory causes of death based on ICD codes for all deaths of Swedish citizens, since 1952 (Brooke et al., Reference Brooke, Talback, Hornblad, Johansson, Ludvigsson, Druid, Feychting and Ljung2017); (3) the Census register, containing data from individuals living in the country since 1960; (4) the Total Population Register, containing data on all Swedish inhabitants since 1968 (Ludvigsson et al., Reference Ludvigsson, Almqvist, Bonamy, Ljung, Michaelsson, Neovius, Stephansson and Ye2016); (5) the Migration Register, containing data on immigrations and emigrations (Ludvigsson et al., Reference Ludvigsson, Almqvist, Bonamy, Ljung, Michaelsson, Neovius, Stephansson and Ye2016); (6) the Longitudinal Integration Database for Health Insurance and Labor Studies, containing sociodemographic information from all individuals living in Sweden since 1990 (Ludvigsson et al., Reference Ludvigsson, Svedberg, Olen, Bruze and Neovius2019); and (7) the Multi-Generation Register, which connects every person born in Sweden since 1932 and ever registered as living in the country after 1960 to their parents (Ekbom, Reference Ekbom2011).
Study population
We included all individuals born from 1932 that were at least 6 years of age and living in Sweden at any time between 1 January 1997 and 31 December 2020. Individuals that had emigrated or died before 1997 or age 6 years were excluded.
We used a matched cohort to estimate the risk of all-cause and cause-specific death in individuals with SAD (exposed), compared to individuals without SAD (unexposed). Each exposed individual was matched on sex, birth year and county of residence at the time of the first recorded SAD diagnosis with 10 individuals who had never received a SAD diagnosis by the date of diagnosis of the corresponding exposed individual. For exposed individuals, the cohort entry date was the date of the first registered SAD diagnosis. Unexposed individuals were assigned the same cohort entry date as their matched exposed counterparts.
Additionally, from the study population, we identified all clusters of full siblings (i.e., those sharing the same biological mother and father), regardless of their SAD exposure, and assigned them a family identification number. In this cohort, the cohort entry date was the date of their sixth birthday, 1 January 1997, or date of immigration, whichever came last.
Exposure
Individuals were considered exposed if they had a diagnosis of SAD in the NPR (Swedish ICD-10 code F40.1) recorded from 1 January 1997 to 31 December 2020 (i.e., end of the study period), if diagnosed at the age of 6 years or older, to avoid potential misclassifications (Vilaplana-Pérez et al., Reference Vilaplana-Pérez, Pérez-Vigil, Sidorchuk, Brander, Isomura, Hesselmark, Kuja-Halkola, Larsson, Mataix-Cols and Fernández de la Cruz2021). This code has shown good validity (positive predictive value = 0.81) and substantial inter-rater reliability (κ = 0.72) (Vilaplana-Pérez et al., Reference Vilaplana-Pérez, Isung, Krig, Vigerland, Jolstedt, Bjureberg, Högström, Isomura, Rautio, Serlachius, Rück, Mataix-Cols and Fernández de la Cruz2020).
Outcomes
All-cause mortality and specific underlying causes of death for individuals that died during the study period were extracted from the Cause of Death Register. Specific causes of death followed the ICD-10 chapters (Supplementary Table 1), and were grouped into natural (all causes except those classified under the ‘external causes of morbidity and mortality’ group) and unnatural (those classified as ‘external causes of morbidity and mortality’). Any causes of death with <10 individual deaths in either the exposed or unexposed cohorts and those classified as ‘codes for special purposes’ in the ICD were grouped under ‘other causes of death’.
Covariates
Sociodemographic information included country of birth (Sweden or outside of Sweden), level of education (elementary [≤9 years], secondary [10–12 years] or higher education [>12 years]), civil status (single, divorced or widowed, or married or cohabiting), and family income level (lowest 20%, middle or top 20%). The first registered record after the diagnosis of SAD was used for analysis. Lifetime psychiatric disorders were retrieved from the NPR and grouped into: (1) neurodevelopmental disorders; (2) psychotic disorders; (3) bipolar disorders; (4) depressive disorders; (5) phobic, anxiety, obsessive–compulsive and stress disorders (except for SAD), hereafter other anxiety disorders; (6) eating disorders; and (6) substance use disorders (Supplementary Table 2).
Statistical analyses
Mortality rates per 1000 person-years were calculated for both the exposed and unexposed cohorts. Survival curves were calculated using Kaplan–Meier survival estimates.
In the matched cohort, we used stratified Cox proportional hazards regression analyses, stratified on matching clusters, to estimate HRs with 95% CIs for time to death in individuals with SAD, compared with matched unexposed individuals. Individuals were followed from the cohort entry date until the date of death (outcome), date of emigration from Sweden or the end of the study period, whichever occurred first. Unexposed individuals were additionally censored at the date they changed their exposure status, if they were diagnosed with SAD after the cohort entry date. Time since the cohort entry date was used as the underlying time scale. The analysis was first conducted for all causes of mortality and then separately for each specific cause; for the cause-specific analyses, we used cause-specific hazards and thus censored individuals at time of death due to a different cause than the one analysed. Model 1 adjusted for the matching variables (i.e., birth year, sex and county of residence) at the time of the first SAD diagnosis (and at the corresponding date for matched unexposed individuals). Model 2 further controlled for country of birth and sociodemographic variables (i.e., education, civil status and income). Missing data on these covariates were marked as unknown and then included in the Cox models as nominal variables. We also estimated the associations from Models 1 and 2 separately by sex. We further adjusted Model 2 for different groups of psychiatric comorbidities, one at a time (Model 3).
In the sibling cohort, we compared individuals with SAD with their unexposed full siblings on the same mortality outcomes. Using time-varying exposures, which allowed for siblings to change exposure status, each sibling was followed from the date of their sixth birthday, 1 January 1997, or date of immigration, whichever occurred last, until the date of death, emigration from Sweden or the end of the study period, whichever occurred first. Stratified Cox proportional hazards regression models, stratified on each sibling cluster and using attained age as the underlying time scale, were adjusted for sex and birth year for each sibling (Model 1) and then, additionally, for sociodemographic variables (Model 2).
Data management and analyses were performed using SAS 9.4 (SAS Institute Inc.) and Stata 18.0 (StataCorp LLC). All tests employed two-tailed significance set at p < 0.05.
Results
Matched cohort
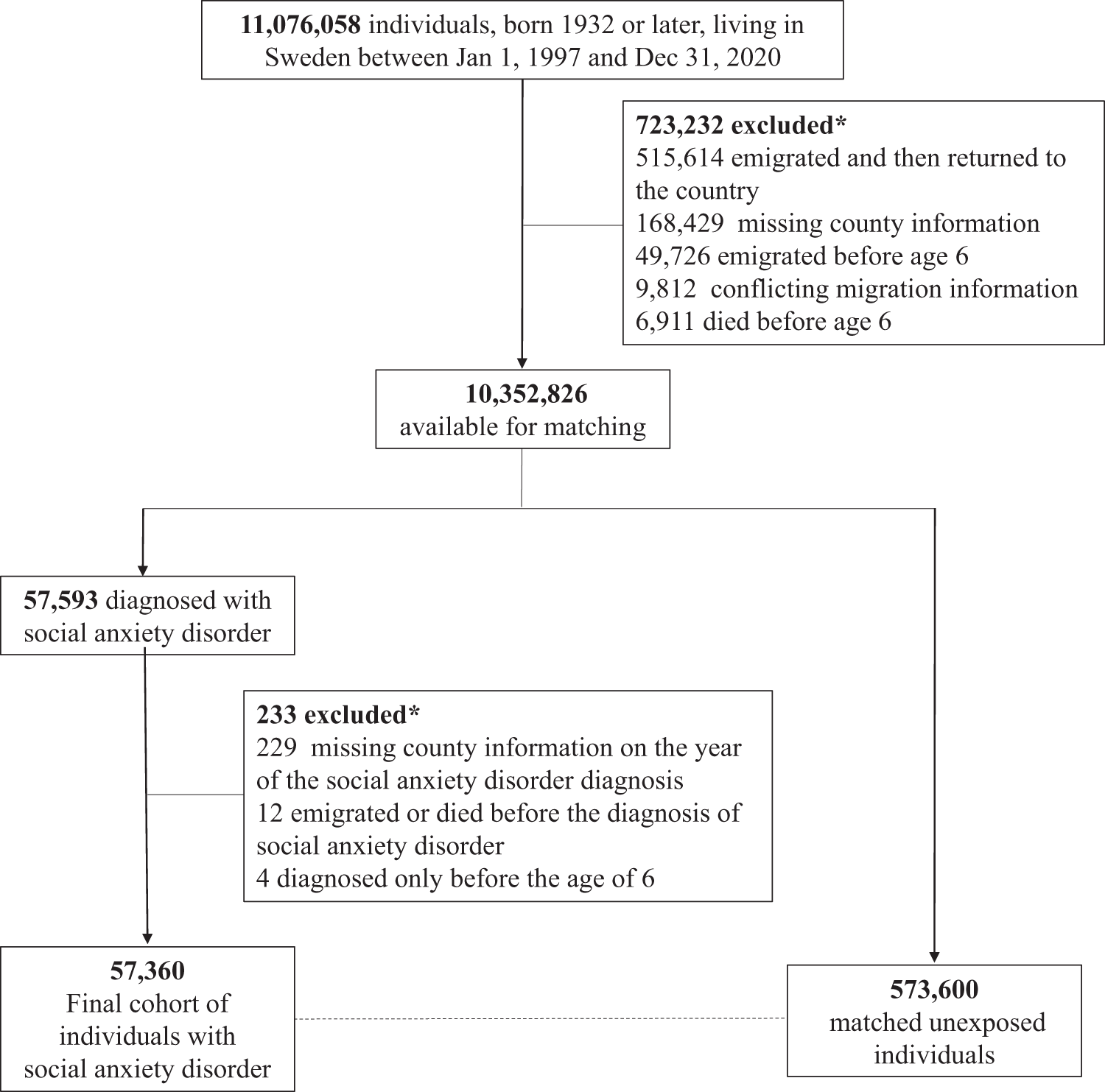
We first identified 11,076,058 individuals who were born in 1932 or later and lived in Sweden at some point between 1 January 1997 and 31 December 2020. After applying several inclusion criteria (see flow of participants in Fig. 1), we identified 57,360 individuals who constituted the final exposed cohort and were matched with 10 individuals without SAD on sex, birth year and county. The full cohort was followed up for a mean of 7.87 years (standard deviation 5.23).
Flow of study participants.

For those exposed, the median age at first diagnosis of SAD was 27.56 years (interquartile range, 20.62–39.12). Individuals with SAD were significantly more likely than matched individuals to be born in Sweden, have a lower level of education, be single, divorced or widowed, have a lower family income, and have higher rates of other psychiatric disorders (Table 1).
Baseline characteristics and follow-up data of study participants

a All differences between individuals with social anxiety disorder and matched unexposed individuals are significant at P < 0.0001, except for sex (matching variable) and follow-up time (P = 0.005). All differences between individuals with social anxiety disorder and their unaffected siblings are significant at P < 0.001, except for mean age at death (P = 0.027).
b The table only reports the characteristics of the siblings in the cohort discordant for social anxiety disorder at the end of the follow-up. Note that more siblings may contribute to the analysis.
c In the matched cohort, individuals with social anxiety disorder and the matched unexposed cohort were followed from the cohort entry date (i.e., date of the first diagnosis of social anxiety disorder, and the corresponding date for comparators), while in the sibling cohort, each sibling was followed from their sixth birthday, 1 January 1997 or the date of immigration, whichever occurred last, which explains the difference follow-up time between cohorts.
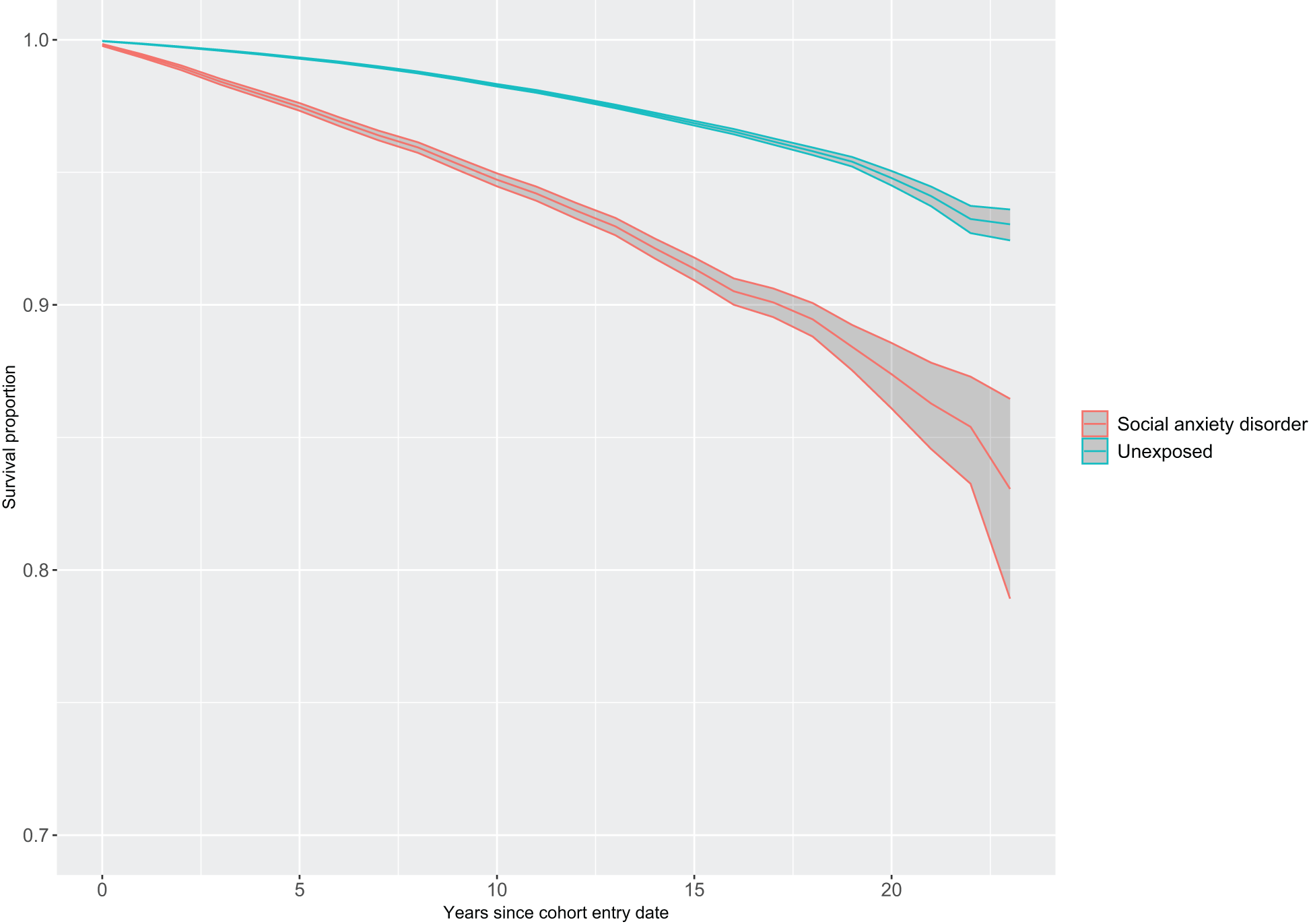
During the follow-up, 2355 deaths were registered within the exposed cohort vs. 7800 deaths in the matched cohort. This translated into crude mortality rates of 5.25 and 1.73 per 1000 person-years, respectively. Kaplan–Meier survival curves for both exposed and matched unexposed cohorts are shown in Figure 2. Estimates adjusting for matching variables (Model 1) showed an increased risk of all-cause mortality in individuals with SAD (HR, 3.23; 95% CI 3.08–3.38), compared with unexposed individuals. Risks were also elevated for the exposed cohort for natural (HR, 2.15; 95% CI 2.02–2.28) and unnatural causes of death (HR, 7.44; 95% CI 6.86–8.06), as well as for all the specific causes within these broader groups, except for the category ‘other natural causes of death’ (Table 2). The magnitude of these risks was considerably reduced when the model further adjusted for sociodemographic variables (Model 2; all-cause mortality: HR, 2.24; 95% CI, 2.13–2.35, natural causes of death: HR, 1.62; 95% CI 1.52–1.72, unnatural causes of death: HR, 4.18; 95% CI 3.82–4.58). The risks of death due to certain infectious and parasitic diseases and diseases of the nervous system were no longer statistically significant. However, individuals with SAD still had a significantly increased risk of death due to mental and behavioural disorders (a group that mostly included deaths attributable to the use of alcohol), diseases of the digestive system (e.g., alcoholic liver disease, fibrosis and cirrhosis of the liver), diseases of the genitourinary system (e.g., kidney failure), diseases of the respiratory system (e.g., chronic obstructive pulmonary diseases, pneumonia), symptoms, signs and abnormal clinical laboratory findings (e.g., unknown causes of mortality), diseases of the circulatory system (e.g., chronic ischemic heart diseases, acute myocardial infarction), endocrine, nutritional and metabolic diseases (e.g., diabetes mellitus, obesity), and neoplasms (e.g., neoplasm of bronchus and lung, neoplasm of pancreas), as well as suicides, accidents and other unnatural causes of death (Table 2).
Survival proportion (Kaplan–Meier estimates with 95% confidence intervals) under the assumption of no competing risks for all-cause mortality in individuals with social anxiety disorder and matched unexposed individuals.

Hazard ratios (HRs) with 95% confidence intervals (CIs) for all-cause and cause-specific mortality among individuals with social anxiety disorder, compared to matched unexposed individuals
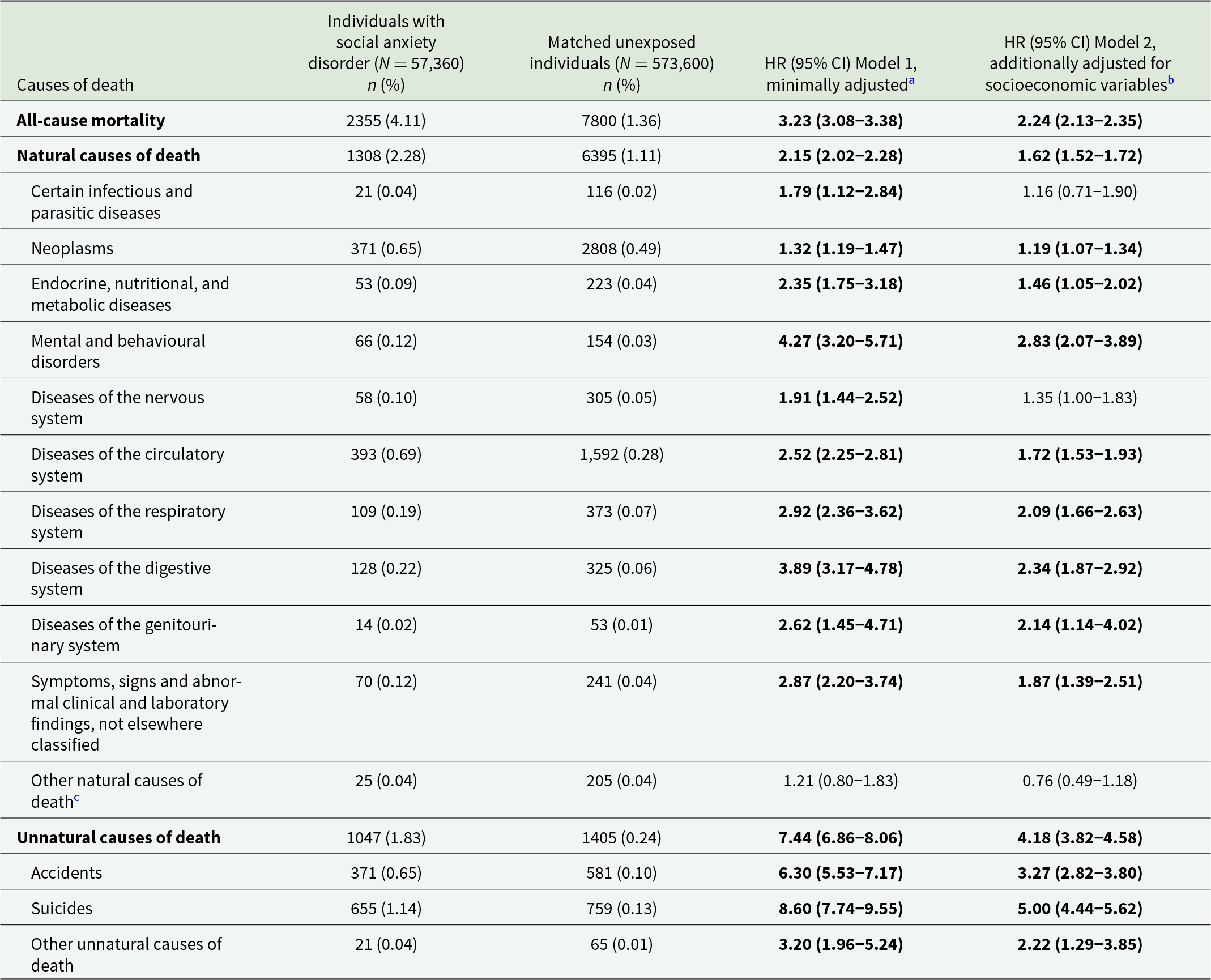
Note: Significant estimates are highlighted in bold.
a Adjusted for all matching variables (i.e., sex, birth year, county of residence at the time of the social anxiety disorder diagnosis).
b Adjusted for all matching variables, country of birth (Sweden vs. abroad) and latest recorded highest level of education, family income level and civil status.
c Includes all groups with a small number of deaths (≤10) and the causes of death classified in the ICD as ‘codes for special purposes’.
Both females and males with SAD, compared with matched unexposed counterparts, had similar risks of death (Supplementary Tables 3 and 4). However, the risk estimates for some of the natural causes of death in individuals with SAD differed according to sex, as indicated by non-overlapping CIs when comparing the estimates for females and males. The risk of death due to mental and behavioural disorders was associated with SAD in males but not in females, while the risk of death due to neoplasms and endocrine, nutritional and metabolic diseases was associated with SAD in females, but not males.
Analyses additionally adjusting for other psychiatric disorders (Model 3; Table 3) showed attenuations of the magnitude of the risks to a different degree, with the estimates for all-cause mortality ranging from an HR of 1.46 (95% CI, 1.39–1.55) when adjusting for substance use disorders to an HR of 2.21 (95% CI, 1.60–2.06) when adjusting for eating disorders. Substance use disorders had the largest impact on the risk estimates. When adjusting for this group, the risks of all-cause mortality, natural causes of death, unnatural causes of death and the specific groups of diseases of the circulatory system, suicides and accidents were significantly reduced (non-overlapping CIs with the corresponding HRs from Model 2 in the main analysis), albeit they were still significant. Additionally, the risk of death due to diseases of the digestive system attenuated to the null when further adjusting for substance use disorders. Adjustment for depressive and other anxiety disorders also significantly reduced the magnitude of the estimates for all-cause mortality, unnatural causes of death and suicide. Adjustment for depressive disorders significantly reduced the risk of natural causes of death, while adjustment for other anxiety disorders significantly reduced the risk of accidents, although they were still significantly elevated.
Hazard ratios (HRs) with 95% confidence intervals (CIs) for all-cause and cause-specific mortality among individuals with social anxiety disorder, compared to matched unexposed individuals, further adjusted for different groups of psychiatric comorbidities (one group at a time)

Note: Significant estimates are highlighted in bold.
a Adjusted for all matching variables (i.e., sex, birth year, county of residence at the time of the social anxiety disorder diagnosis), country of birth (Sweden vs. abroad), latest recorded highest level of education, family income level and civil status, and the specified group of psychiatric comorbidities.
b Includes all groups with a small number of deaths (≤10) and the causes of death classified in the ICD as ‘codes for special purposes’.
Sibling cohort
By the end of the follow-up, among a cohort of 6,363,292 siblings (2,570,996 clusters) from the whole study population, we identified 39,993 who had received a SAD diagnosis and their 64,640 unaffected siblings (Table 1). Individuals with SAD, compared to their unaffected full siblings, were more likely to be born in more recent birth cohorts, male, born in Sweden, less educated, single, divorced or widowed, have a lower family income, and have a significantly higher rate of comorbid psychiatric disorders (Table 1). Individuals with SAD had a higher risk of mortality than their siblings without the diagnosis, although the magnitude of this association was substantially lower than in the matched cohort comparison (HR for all-cause mortality, 1.40; 95% CI 1.36–1.45; HR for natural causes of death, 1.22; 95% CI, 1.17–1.27; HR for unnatural causes of death, 1.71; 95% CI 1.62–1.80). Among the deaths due to specific groups of diseases, results also remained overall robust, albeit the estimates were also reduced. Only the risk of death due to neoplasms became non-significant (HR, 1.01; 95% CI 0.94–1.08), as did the risks of death due to ‘other natural’ and ‘other unnatural’ causes (HR, 0.85; 95% CI 0.68–1.06 and HR, 1.20; 95% CI 0.89–1.62, respectively) (Table 4).
Hazard ratios (HRs) with 95% confidence intervals (CIs) for all-cause and cause-specific mortality among individuals with social anxiety disorder, compared to their unaffected full siblings

Note: Significant estimates are highlighted in bold.
a The reported counts and frequencies refer to the siblings in the cohort discordant for social anxiety disorder at the end of the follow-up. Note that more siblings may contribute to the analysis.
b Adjusted for sex and birth year for each sibling and sibling order.
c Adjusted for all variables in Model 1 plus country of birth and latest recorded highest level of education, family income level and civil status.
d The adjusted model could not be fitted for this cause of death due to complete separation, which resulted from the low number of observations in certain covariates.eIncludes all groups with a small number of deaths (≤10) and the causes of death classified in the ICD as ‘codes for special purposes’.
Discussion
We investigated all-cause and cause-specific mortality in over 50,000 individuals with SAD diagnosed in specialist services, compared with demographically matched unexposed individuals. The risk of mortality in those with SAD was over twofold compared with the unexposed group, attributable primarily to unnatural causes of death, such as suicide, but also to natural causes, even after adjusting for socioeconomic variables.
Our all-cause mortality estimates were higher than those reported in a smaller study in Denmark (Meier et al., Reference Meier, Mattheisen, Mors, Mortensen, Laursen and Penninx2016), which showed a 50% increased risk of death in individuals with SAD, compared with the general population. Both our and the Danish results (Meier et al., Reference Meier, Mattheisen, Mors, Mortensen, Laursen and Penninx2016) differed from previous reports that did not find an excess mortality risk in this group (Eaton et al., Reference Eaton, Roth, Bruce, Cottler, Wu, Nestadt, Ford, Bienvenu, Crum, Rebok, Anthony and Munoz2013; John et al., Reference John, Rumpf, Hanke and Meyer2020). Methodological differences, with the former studies including data from hospital records and the latter based on data from random samples from the population, may be responsible for the different outcomes. In fact, a systematic review and meta-analysis showed no evidence of increased mortality risk among anxious participants from community samples (Miloyan et al., Reference Miloyan, Bulley, Bandeen-Roche, Eaton and Goncalves-Bradley2016). This indicates that the risk may only be present in individuals whose symptoms are severe or complex enough to seek treatment and require specialist treatment.
For the first time, we were able to identify specific natural causes of death in individuals with SAD. Deaths due to mental and behavioural disorders, mostly due to use of alcohol, showed the highest risk estimates, followed by deaths related to the digestive, genitourinary, respiratory, circulatory and endocrine systems and neoplasms. Notably, many of these causes are associated with behavioural factors, such as the use of alcohol and other unhealthy lifestyles. This finding is compatible with the so-called self-medication hypothesis by which individuals with SAD consume anxiolytic substances, such as alcohol, in order to temporarily alleviate social anxiety symptoms (Carrigan and Randall, Reference Carrigan and Randall2003; Rosenström and Torvik, Reference Rosenström and Torvik2023).
There were significant sex differences in the risks of some natural causes of death. Namely, there was no association between SAD and deaths due to mental disorders in females, while there was a significant association between SAD and this cause of death in males, which may have been driven by a higher prevalence of use of substances in males. On the other hand, females with SAD had a higher risk of death due to neoplasms and endocrine, nutritional and metabolic diseases, while risks of death due to these causes were not significant in males with SAD. The reasons for these differences are unknown and puzzling given that females are known to have higher rates of healthcare-seeking behaviours across all health concerns (Rata Mohan et al., Reference Rata Mohan, Jawahir, Manual, Abdul Mutalib, Mohd Noh, Ab Rahim, Ab Hamid and Amer Nordin2025). Further research should explore potential putative mechanisms behind these differences, including sex differences in stress-response, inflammatory, cardiovascular and other biological variables, comorbid somatic illness and substance use, and help-seeking and treatment adherence behaviours.
Our results on deaths by suicide are in line with those from a register-based Taiwanese study (Wei et al., Reference Wei, Tsai, Cheng, Chang, Bai, Su, Chen and Chen2025). To our knowledge, the finding that SAD is associated with an increased risk of death due to accidents is novel and warrants further exploration. Again, it could be hypothesised that the excess number of accidents in this group is associated with the use of alcohol and other substances, as well as with the relatively high levels of neurodevelopmental disorder comorbidity in our cohort. Specifically, previous research has shown that attention-deficit/hyperactivity disorder is associated with transport accidents (Chang et al., Reference Chang, Lichtenstein, D’Onofrio, Sjolander and Larsson2014, Reference Chang, Quinn, Hur, Gibbons, Sjolander, Larsson and D’Onofrio2017; Mataix‐Cols et al., Reference Mataix‐Cols, Brander, Chang, Larsson, D’Onofrio, Lichtenstein, Sidorchuk and Fernández de la Cruz2021).
Nonetheless, additional adjustment of our risk estimates for psychiatric comorbidities, especially substance use disorders, but also depressive and other anxiety disorders, considerably attenuated the mortality estimates, indicating that these comorbidities are likely to explain some of the risk, but did not fully account for it. The sibling comparison also showed an attenuation of the risk of death. This suggests that shared environmental and genetic factors may also contribute, at least to some extent, to the observed association between SAD and mortality.
Importantly, like in other disorders in the broad anxiety spectrum, such as obsessive-compulsive disorder (Fernández de la Cruz et al., Reference Fernández de la Cruz, Isomura, Lichtenstein, Larsson, Kuja-Halkola, Chang, D’Onofrio, Brikell, Rück, Sidorchuk and Mataix-Cols2024), the majority of excess deaths in the SAD cohort in our study are potentially amenable to prevention or early interventions. Those caring for individuals with SAD should put specific emphasis on the management of comorbid psychiatric conditions (specifically substance use disorders, depression and other anxiety disorders) and the long-term monitoring of suicide risk and somatic health, particularly in individuals with substance use.
Strengths and limitations
To our knowledge, this was the first study systematically investigating specific causes of death in a large cohort of individuals with SAD. The ICD-10 SAD codes are well validated in the NPR (Vilaplana-Pérez et al., Reference Vilaplana-Pérez, Isung, Krig, Vigerland, Jolstedt, Bjureberg, Högström, Isomura, Rautio, Serlachius, Rück, Mataix-Cols and Fernández de la Cruz2020). Additionally, the Swedish Cause of Death Register has an outstanding nationwide coverage (Brooke et al., Reference Brooke, Talback, Hornblad, Johansson, Ludvigsson, Druid, Feychting and Ljung2017). We also adjusted for relevant socioeconomic factors and lifetime psychiatric comorbidities. An additional sibling comparison allowed us to consider unmeasured familial confounding.
The study also has limitations. First, the NPR only includes diagnoses in specialist services, with information from outpatient care only available from 2001, which may have resulted in the inclusion of individuals with SAD in the more severe end of the spectrum, given that many anxiety patients are generally managed in primary care. Nonetheless, our previous validation of the SAD codes in the NPR showed a fairly normal distribution of cases according to their severity (Vilaplana-Pérez et al., Reference Vilaplana-Pérez, Isung, Krig, Vigerland, Jolstedt, Bjureberg, Högström, Isomura, Rautio, Serlachius, Rück, Mataix-Cols and Fernández de la Cruz2020). Second, because SAD as an independent diagnosis within the broad neurotic disorders category only appears in the ICD-10, implemented in Sweden in 1997, our exposed cohort only includes individuals with a diagnosis following that date. This may have led to a potential misclassification of cases (e.g., if individuals were diagnosed for the first time as socially anxious before 1997 and never diagnosed again). Also, our cohort was relatively young (note that the mean age at death for the non-exposed matched cohort is around 60, significantly younger than the life expectancy in Sweden), and it may have been too early for many individuals to die from causes that tend to appear later in life. Third, some of the covariates in our adjusted models could be mediators rather than confounders, potentially underestimating the magnitude of the true associations. However, we also presented a model that did not adjust for these variables. Although this model showed higher estimates, the additionally adjusted analyses still showed significant risks for the outcomes of interest. Fourth, our study did not analyse additional variables that may be relevant for mortality, such as the severity of SAD, childhood experiences, lifestyle factors, use of medication or healthcare utilisation. Finally, our study was conducted in a country with universal healthcare and it is unknown whether results generalise to countries with different models.
Conclusion
Individuals with SAD face an increased risk of mortality, particularly due to unnatural causes of death, such as suicide. Psychiatric comorbidities, specifically substance use disorders, significantly contribute to this excess death. Clarifying the underlying mechanisms may inform targeted prevention strategies and ultimately reduce mortality in this population.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S2045796026100535.
Availability of data and materials
Sharing of the individual-level data is restricted by Swedish data protection laws and data underlying the reported findings cannot be deposited in publicly accessible archives. In this study, data were obtained from the National Patient Register held by the Swedish National Board of Health and Welfare (Socialstyrelsen; http://www.socialstyrelsen.se/english) and the Total Population Register maintained by Statistics Sweden (SCB; http://www.scb.se/en/), among others. For enquiries about access to data, any interested parties can contact the data owners via registerservice@socialstyrelsen.se and information@scb.se.
Financial support
This study was supported by grants from Region Stockholm (ALF Medicin project grants; reference 20160143 and 20180078), the Swedish Society of Medicine (Svenska Läkaresällskapets; reference SLS-879801) and Karolinska Institutet (reference FS-2018:0007), all awarded to L.F.C.
Competing interests
L.F.C. receives royalties for contributing articles to UpToDate, Wolters Kluwer Health and for editorial work from Elsevier, outside the submitted work. Z.C. received lecture honoraria from Takeda Pharmaceuticals, outside the submitted work. H.L. receives grants from Shire and Takeda and personal fees from Shire and Takeda, Evolan and Medici outside the submitted work. D.M.-C. receives royalties for contributing articles to UpToDate, Wolters Kluwer Health and is part owner of Scandinavian E-Health AB, outside the submitted work. All other authors report no potential conflicts of interest.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Declaration of Helsinki 1975, as revised in 2000. Ethical approval was granted by the Swedish Ethical Review (reference number 2020-06540). The requirement for informed consent was waived because the study is register-based and the included individuals are not identifiable.







 Open access
Open access