


Introduction
Health professional burnout is the psychological outcome of chronic work-related stress.Reference Maslach, Schaufeli and Leiter1 It is characterised by emotional exhaustion, depersonalisation, and a low sense of personal accomplishment at work.Reference Maslach, Schaufeli and Leiter1 Even before the COVID-19 pandemic, rates of burnout and psychological stress were high, affecting up to 80% of health professionals.Reference Rotenstein, Torre and Ramos2 The pandemic further intensified burnout,Reference Sexton, Adair and Proulx3 anxiety and depressive symptoms,Reference Dragioti, Tsartsalis, Mentis, Mantzoukas and Gouva4 and insomnia.Reference Herrero San Martin, Parra Serrano and Diaz Cambriles5
The aetiology of burnout among health professionals is complex, with individual, team, organisational, and system-level causes identified.Reference Brigham, Barden and Legreid Dopp6 Greater burnout has been reported among younger, unmarried, and less experienced clinicians.Reference Demerouti, Bakker, Peeters and Breevaart7 Increased workload, inadequate staffing and resources, and low autonomy also contribute to emotional exhaustion.Reference Rotenstein, Torre and Ramos2 Alternatively, compassion satisfaction and coping skills (e.g., boundary setting) have been linked to lower clinician burnout.Reference Algamdi8 Prolonged psychological stress and workplace burnout are linked to adverse health outcomes, such as Type 2 diabetes, anxiety and depression, insomnia, and substance misuse.Reference Salvagioni, Melanda, Mesas, González, Gabani and Andrade9,Reference Xia, Jiang and Rakofsky10 Emotional exhaustion affects concentration, increasing risk for medical errors, while depersonalisation can lead to poor communication with colleagues and patients.Reference Tawfik, Scheid and Profit11 Burnout is also associated with poor workplace engagement, higher absenteeism, and turnover, with fiscal consequences for the health system.Reference Salvagioni, Melanda, Mesas, González, Gabani and Andrade9,Reference Dyrbye, Shanafelt, Johnson, Johnson, Satele and West12
Health professionals working with children with critical or complex chronic illness, such as CHD, provide highly specialised care while navigating difficult conversations with highly distressed families.Reference Akram, Pidcock, Oake, Sholler, Farrar and Kasparian13–Reference Kasparian, Kan, Sood, Wray, Pincus and Newburger15 Health professionals in paediatric cardiac care report burnout, anxiety, and depression;Reference McCormick, Lim and Strohacker16,Reference Dasgupta, Dave, McCracken, Mohl, Sachdeva and Border17 however, few studies provide insight into associated factors. Qualitatively, fears of patient harm and inability to support worried families serve as stressors for many early career clinicians,Reference Brown, Binney, Gauthier and Blume18,Reference Molala and Downing19 while poor staffing and high workload limit mentorship opportunities.Reference McCormick, Lim and Strohacker16,Reference Brown, Binney, Gauthier and Blume18,Reference Molala and Downing19 In contrast, many health professionals report high satisfaction and pride in their work.Reference McCormick, Lim and Strohacker16,Reference Brown, Binney, Gauthier and Blume18,Reference Molala and Downing19
Given the prevalence of burnout in other medical settings and the limited data for health professionals in paediatric cardiac care, the aims of this study were to: (1) assess the prevalence of burnout (i.e., emotional exhaustion, depersonalisation, and personal accomplishment at work; (2) identify demographic, work role, physical, and psychological correlates; and (3) explore support needs and preferences in this population. We hypothesised that younger, single, and less experienced health professionals would endorse greater emotional exhaustion, as would those reporting greater work-life conflict and higher anxiety and depressive symptoms.Reference Dyrbye, Shanafelt, Johnson, Johnson, Satele and West12,Reference Dobson, Malpas and Burrell20 We also hypothesised that health professionals with greater compassion satisfaction would report lower exhaustion.Reference Algamdi8
Materials and Methods
Overview
The study methods, including design and procedures, have been described in detail.Reference Akram, Webb, Pidcock, Farrar and Kasparian14 Briefly, this cross-sectional study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline (Supplementary Table 1). Health professionals from diverse disciplines at a large Australian quaternary hospital service who provide care for children with heart disease were invited to complete one survey. Staff were excluded if they were unable to be contacted. The relevant Human Research Ethics Committee (HREC/15/SCHN/95) provided approval for the study.
Recruitment
Participant recruitment (June 2020–February 2021) included identifying eligible staff members and emailing them a personalised invitation, study information sheet, and customised link to an online survey on the secure Qualtrics platform (Qualtrics, Provo, UT). If a potential participant did not complete the online survey after three reminders, a paper-based survey was provided. Recruitment strategies included introducing the survey via information sessions and the distribution of customised cookies and chocolates, study flyers, and digital posters.
Measures
The WithCare Health Professional Survey included validated and study-specific measures informed by a literature review, the National Academy of Medicine conceptual framework of clinician well-being,Reference Brigham, Barden and Legreid Dopp6 and rigorous piloting.
The primary outcome of emotional exhaustion (9 items, Cronbach’s alpha [α] in the present study = 0.92) as well as depersonalisation (5 items, α = 0.78) and personal accomplishment at work (8 items, α = 0.76) were assessed with the validated, widely used Maslach Burnout Inventory.Reference Maslach, Jackson, Leiter, Zalaquett and Wood21 Participants rated experiences over the past year from 0 (Never) to 6 (Everyday), with greater burnout indicated by higher scores on emotional exhaustion and depersonalisation, and lower scores on personal accomplishment.
Demographics (8 items) were measured with standard items (e.g., age, gender, marital status, gross annual household income), with household income compared with the Australian national average of $120,000 per annum.22 Work role characteristics were assessed with 7 items (e.g., primary role, years of professional experience, days on call in the past month). The work area was categorised as intensive (paediatric and neonatal intensive care units, operating suite), or non-intensive (cardiac ward, outpatient clinic, catheterisation laboratory, office). Participants also indicated the likelihood of choosing the same career again from 1 (Definitely not) to 5 (Definitely yes).
Participants rated their empathy towards patients from 1 (Strongly disagree) to 7 (Strongly agree), using the validated Jefferson Scale of Empathy,Reference Hojat23 with higher scores indicating greater healthcare empathy (20 items, α = 0.81). Compassion satisfaction was rated in the past 30 days from 1 (Never) to 5 (Very often) using the subscale of the Professional Quality of Life Scale,Reference Stamm24 with higher scores indicating greater satisfaction (10 items, α = 0.89).
Nine Brief COPEReference Carver25 subscales (18 items) assessed the frequency of coping responses to work-related difficulties from 1 (I don’t do this at all) to 4 (I do this a lot). Two mean scores were calculated using Eisenberg’s classification for coping styles:Reference Eisenberg, Shen, Schwarz and Mallon26 (1) approach-based coping (α = 0.69), including active coping, positive reframing, and acceptance, and (2) avoidance-based coping (α = 0.71), including self-distraction, denial, substance use, behavioural disengagement, venting, and self-blame. The Social Provisions Scale (SPS-5)Reference Orpana, Lang and Yurkowski27 assessed perceived social support in current personal and professional relationships (5 items, α = 0.87) from 1 (Strongly disagree) to 4 (Strongly agree); higher scores indicated greater perceived social support. Participants rated the helpfulness of psychosocial support options (e.g., critical event debriefing, workshops on managing conflict) from 1 (Not at all helpful) to 5 (Extremely helpful) as well as the current availability of each option (9 items, α = 0.84).
Using the Patient Health Questionnaire (PHQ-4), participants indicated anxiety and depressive symptoms experienced in the past 2 weeks from 0 (Not at all) to 3 (Nearly every day), with higher total scores indicating greater symptoms (4 items, α = 0.87). Scores ≥3 indicated a need for clinical intervention, and participants were contacted by a psychologist to provide support. Using the validated Brief Resilience Scale (6 items, α = 0.84),Reference Smith, Dalen, Wiggins, Tooley, Christopher and Bernard28 participants indicated agreement with statements from 1 (Strongly disagree) to 5 (Strongly agree), with higher scores indicating greater psychological resilience.
Conflict between work and family was assessed (5 items, α = 0.95) with the Work-Family Conflict scale,Reference Netemeyer, Boles and McMurrian29 with participants rating items from 1 (Strongly disagree) to 7 (Strongly agree) to reflect the extent to which work disrupted family life and vice versa. Higher scores indicated greater conflict. Six items were used to assess physical health factors (e.g., chronic health conditions, smoking behaviour, alcohol use). Current cigarette smoking status was rated 1 (Never or <100 cigarettes in my lifetime), 2 (Did smoke but do not smoke now), or 3 (I smoke now). Current smokers indicated the average number of cigarettes smoked per day. Participants indicated how often they had a drink containing alcohol (0 [Never] to 4 [Four or more times per week]) on the 3-item Alcohol Use Disorders Identification Test-Consumption (AUDIT-C).Reference Bush, Kivlahan, McDonell, Fihn and Bradley30 Participants indicating alcohol consumption were asked the number of standard drinks consumed on a typical day (1–2 standard drinks to 10 or more standard drinks), and how often they consumed ≥6 drinks per occasion from 1 (Less than monthly) to 4 (Daily or almost daily). Total scores ≥5 are indicative of unhealthy alcohol use. Finally, the validated Insomnia Severity Index assessed the presence and severity of insomnia in the past two weeks (7 items, α = 0.89).Reference Morin31 Total scores indicate sub-threshold insomnia (8–14) and clinical (severe) insomnia (≥15).
Data analysis
The IBM Statistical Package for the Social Sciences version 27.0 and R version 4.1.3 (R Core team) were used to complete statistical analyses. Participants with <60% of the survey completed were excluded from analysis, and missing data were handled as per the instrument manuals. Chi-squared tests compared characteristics of participants and eligible non-participants (e.g., work role). Descriptive statistics (e.g., means [M], standard deviations [SD]) were used to describe the sample and variables of interest. Potential mean score differences for the two coping subscales were examined with paired samples t-tests.
Hierarchical linear regression models were built to examine correlates of emotional exhaustion. A power analysis was conducted based on a 23-variable model, assuming a moderate effect size (f2 = 0.15), significance level of 5%, and 80% power, resulting in a required minimum sample size of N = 166. Correlate selection was based on published evidence and theory,Reference Xia, Jiang and Rakofsky10 with correlates arranged into five blocks in the following order: (1) demographics, (2) work role, (3) physical health, (4) psychological factors, and (5) social support. Multicollinearity among variables was checked with the Variance Inflation Factor. Assumptions of normally distributed residuals and homogeneity of residual variance for linear regression were checked using residual plots. Despite some collinearity (e.g., years of experience and age, primary work role and hours worked per week, and anxiety and depressive symptoms), no variable had a VIF>5 in the final model. The proportion of variance explained in emotional exhaustion was evaluated with the change in R2 for each block. The statistical significance threshold was set at p < 0.05, with effect sizes (ß) and 95% confidence intervals (CI) calculated.
Results
Response rate and sample demographic and clinical characteristics
Of 552 health professionals identified, 82 were no longer working, 7 were on extended leave, 39 were non-contactable, and 8 completed less than 60% of the survey, leaving 416 eligible health professionals. Of these, 229 (153 nurses, 32 physicians, 5 surgeons, 22 allied and mental health professionals, 17 research and administrative staff) completed the survey (55% response rate). No significant differences were detected between participants and eligible non-participants for work role (p = 0.20) or gender (p = 0.35). Though health professionals working in intensive areas (response rate: 46%) comprised 70% of the eligible cohort, those working in non-intensive areas were more likely to complete the survey (response rate: 71%, χ2 = 21.4, df = 1, p < 0.01).
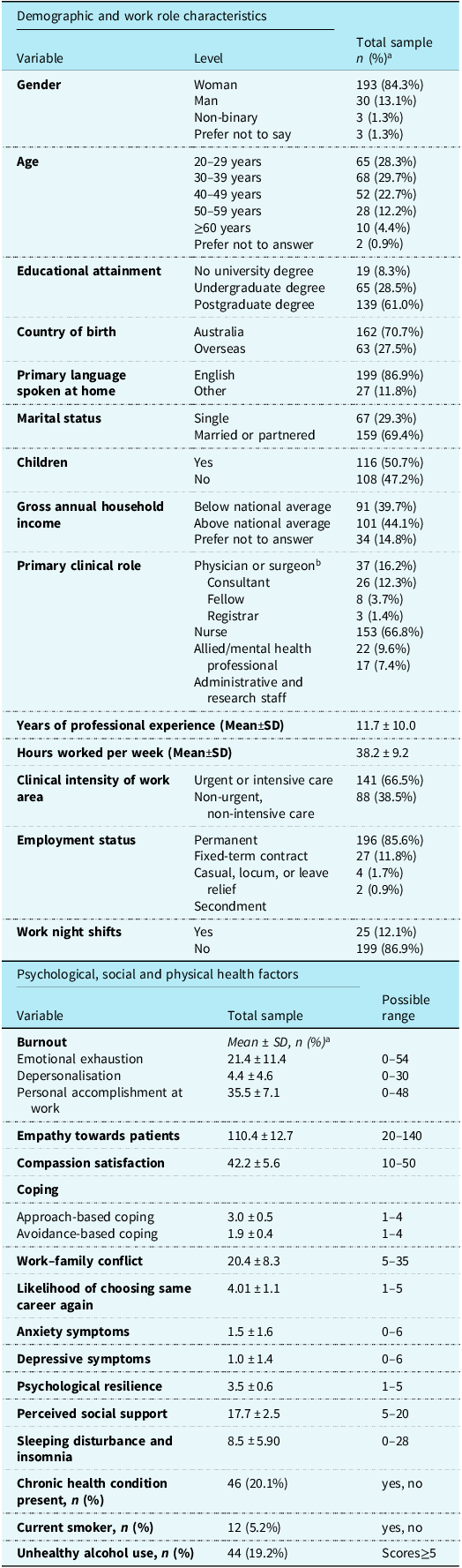
Most participants identified as women (84.3%), were aged between 20 and 49 years (80.7%), married or partnered (69.4%), and Australian-born (70.7%; Table 1). Professional experience ranged from 6 months to 45 years (M = 11.7 ± 10.0 years), and most (85.6%) had permanent employment.
Participant (N=229) characteristics and descriptive statistics for psychological, social, and physical health factors

a Some percentages do not add to a 100 due to missing data.
b Fields of specialisation include fetal or paediatric cardiology (n = 11), neonatology (n = 7), paediatric cardiothoracic surgery (n = 5), paediatric intensive care (n = 6), and anaesthesiology (n = 7).
Physical, psychological, and social health factors
One in five participants (20.1%) reported having a chronic health condition, 5.2% were current smokers, 19.2% exceeded the cut-off for unhealthy alcohol use, and over half met criteria for sub-threshold (38%) or clinical insomnia (14%; Table 1). Overall, 18% reported anxiety and 11% reported depressive symptoms above the clinical cut-off, indicating a need for further assessment. Participants were more likely to use approach-based coping (e.g., positive reframing) than avoidance-based coping (e.g., denial; t = −30.2, df = 227, 95%CI: −1.22, –1.07, p < 0.001). Over half (57.2%) reported work interfered with home and family life, and 73.3% indicated they would “probably” or “definitely” choose the same career again.
Burnout
Mean scores for burnout dimensions are shown in Table 1. Overall, 68% reported feeling “used up at the end of the workday,” 54% felt “frustrated by their job,” and 66% felt “emotionally drained from work’ at least a few times a month; 6% endorsed these feelings every day. For depersonalisation, 23% felt “worried this job is hardening me emotionally,” and 14% believed they had “become more callous (uncaring) towards people since taking this job” at least a few times a month. While 93% of respondents indicated they “deal very effectively with problems of my patients,” 6% never ‘felt exhilarated after working closely with my patients.”
Factors associated with emotional exhaustion
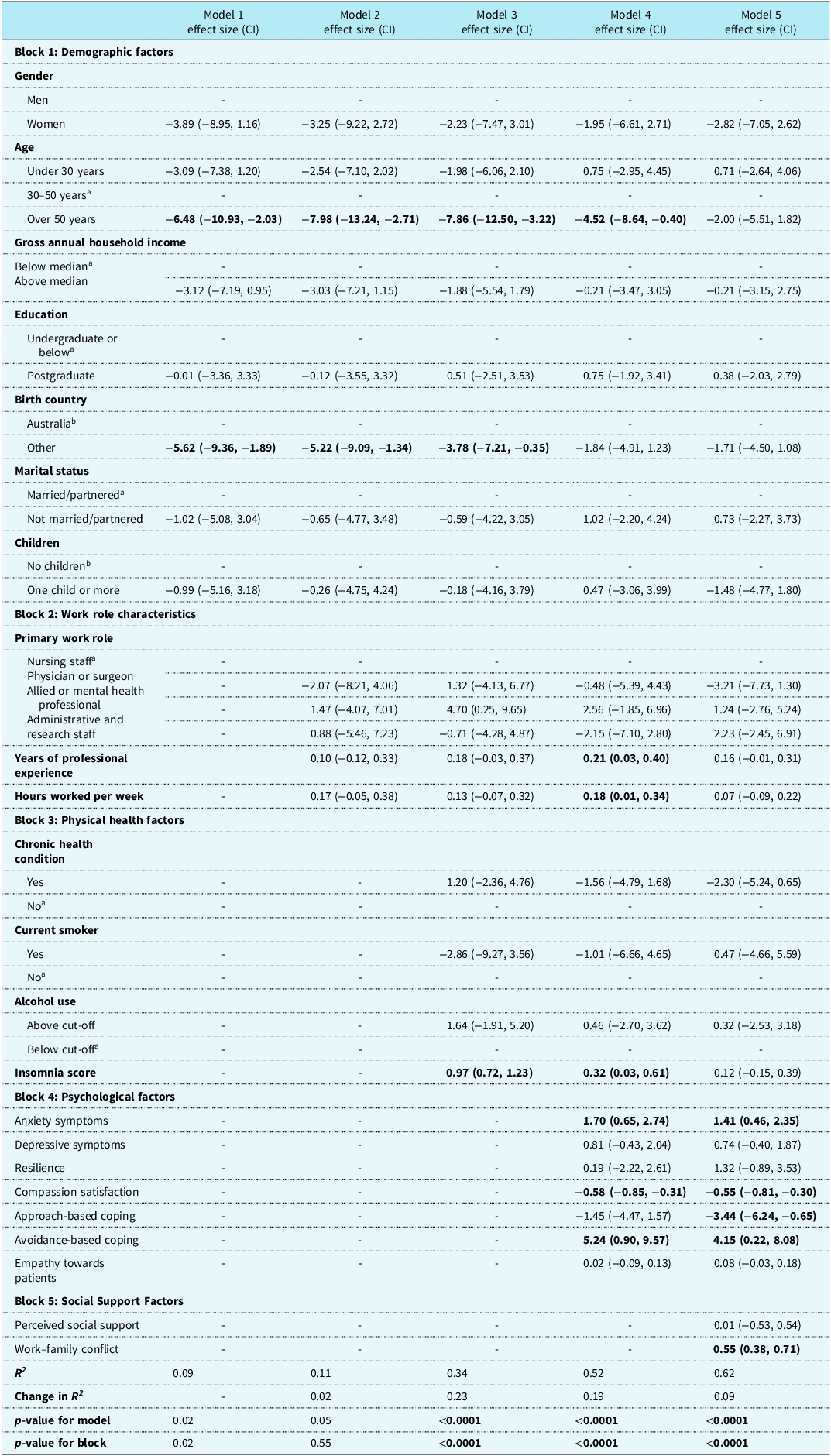
The hierarchical linear regression model (Table 2) explained 62% of the variance in emotional exhaustion, with physical health (23%) and psychological factors (19%) accounting for the greatest proportion. In the final model, greater emotional exhaustion was associated with greater anxiety (ß = 1.41, 95% CI: 0.46, 2.35), greater avoidance-based coping (ß = 4.15, 95% CI: 0.22, 8.08), lower compassion satisfaction (ß = 0.55, 95% CI:−0.81,−0.30), lower approach-based coping (ß = −3.44, 95% CI: −6.24, −0.65), and greater work-family conflict (ß = 0.55, 95% CI: 0.38, 0.71).
Hierarchical linear regression analysis identifying factors associated with emotional exhaustion (N = 229)

CI: Confidence Interval.
a Reference category for categorical variables.
Psychosocial support preferences
Psychosocial support options perceived as most helpful were informal peer support (M = 4.0 ± 0.9), group debrief sessions after critical incidents (M = 3.7 ± 1.1), regular individual debrief sessions (M = 3.6 ± 1.1), and workshops on issues, such as conflict resolution and dealing with burnout, grief, and trauma (M = 3.5 ± 1.1; Figure 1). Informal peer support was available to most participants (74%), while <25% had access to critical incident or regular individual debriefing, and relevant workshops.
Perceived helpfulness and availability of various psychosocial support options.

Discussion
Health professional burnout is increasing at an alarming rate, putting health professionals at risk for adverse personal and professional consequences and affecting patient healthcare.32,Reference Murthy33 In this study of Australian health professionals in paediatric cardiac settings, emotional exhaustion was prevalent and associated with greater anxiety, work-family conflict, and avoidance-based coping, as well as lower compassion satisfaction. One in five reported anxiety symptoms warranting intervention, and one in two met criteria for sleeping problems. While informal peer support was perceived as helpful and available, many reported not having access to critical incident or regular individual debriefing, or workshops on issues, such as conflict resolution and managing workplace trauma, grief, and burnout.
Similarly, in 2020, a single-centre U.S. study of 45 paediatric cardiologists found 65% endorsed at least one symptom of emotional exhaustion.Reference Dasgupta, Dave, McCracken, Mohl, Sachdeva and Border17 Studies among intensive care nurses in Turkey,Reference Efıl, Turen, Yıldız Ayvaz, Bulbul and Yenı34 and early career physicians in the United KingdomReference Zhou, Hann and Panagioti35 reported similar results; however, none identified correlates of emotional exhaustion, impeding opportunities for intervention design. As hypothesised, in the present sample, emotional exhaustion and anxiety were linked, aligning with evidence from other health professional populations,Reference Linzer, Jin and Shah36 and from the COVID-19 pandemic.Reference Akram, Pidcock, Oake, Sholler, Farrar and Kasparian13 Poor physical health was associated with greater emotional exhaustion, most likely caused by energy depletion, disturbance of normal circadian rhythm, and low mood.Reference Alimoradi, Broström and Tsang37 Emotional exhaustion was also associated with greater avoidance-based coping, such as self-blame, denial, and substance use. In the literature, self-blame and substance use have been identified as predictors of burnout,Reference Brigham, Barden and Dopp38 while active coping strategies, such as problem-solving, are protective against burnout.Reference Linzer, Jin and Shah36 Individual-level strategies (e.g., physical activity, mindfulness-based practices, workplace boundaries) may be beneficialReference Akram, Pidcock, Oake, Sholler, Farrar and Kasparian13,Reference Brigham, Barden and Dopp38 ; but form only part of a much larger solution to cultivating workplace health and well-being.
Health professionals in paediatric cardiac settings consistently report high compassion and career satisfaction.Reference Brown, Binney, Gauthier and Blume18,Reference Molala and Downing19 The strong bonds formed with children and families while bearing witness to their resilience and recovery may thwart emotional exhaustion to an extent; however, many participants reported work-family conflict, which, as hypothesised, was associated with emotional exhaustion. High workload and work-life imbalance have been linked with lower team morale and frequent staff turnover.Reference Brown, Binney, Gauthier and Blume18,Reference Molala and Downing19 A cross-sectional survey of 20,627 health professionals (2019–2021) found low workplace autonomy, increased non-patient-facing tasks, and lack of organisational support increased burnout and influenced intentions to leave their profession.Reference Linzer, Jin and Shah36 Greater efficacy of interventions targeting institutions rather than health professionals has been reported in the literature, such as the “Choosing Wisely” campaign which encourages regular review of policies and practices to streamline workflows and reduce administrative work burden.39
The U.S. National Academy of Medicine has highlighted the need for healthcare organisations to ensure robust, regular assessment of health professional well-being; establish work schedules with greater flexibility, autonomy, and meaning for individuals; promote an inclusive and culturally-diverse work environment; and disseminate sustainable workplace initiatives to improve clinician well-being.39 A Cochrane review of 58 intervention studies (N = 7,188 clinicians) found regular breaks, shorter work shifts, and cognitive–behavioural therapy reduced emotional exhaustion compared with no intervention.Reference Ruotsalainen, Verbeek, Mariné and Serra40 Regular, formalised supports in psychologically safe settings, such as the individual and critical incident debriefing in our findings, provide opportunities to acknowledge individual work efforts and challenges, and address difficulties in team communication and workload distribution.39,Reference Ruotsalainen, Verbeek, Mariné and Serra40
Study strengths and limitations
Strengths include the robust response rate, proportionately equal representation from men and women (56%), and use of validated, theory-driven measures to foster comparisons across studies and contexts. Several limitations, however, warrant discussion. The cross-sectional design precludes causal inference, and recruitment across a single health system, with high representation of nursing staff, limits generalisability. The pandemic may have exacerbated distress, and pandemic-related changes in workload and schedules may have prevented clinicians experiencing greater distress from participating, with potential underestimation of the challenges and support needs of this population.
Conclusions
Health professionals in this study reported high emotional exhaustion, which was associated with greater anxiety, avoidance-based coping, and work-family conflict, as well as lower compassion satisfaction. Findings highlight a need for multi-pronged initiatives to bolster psychological well-being and healthy coping, combat high workload and poor work-life balance, and provide regular debriefing and workshops to improve workplace communication, collaboration, and processing of moral distress, demonstrating that health professional well-being is prioritised as an organisational value. The efficacy of these interventions requires multi-centre, longitudinal studies to demonstrate changes in clinician well-being over time.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951125111098.
Acknowledgements
We extend our sincere gratitude to the health professionals who participated in this research and the clinical leaders who generously donated their time to raise awareness and support recruitment. Special thanks to Mrs. Dianne Swinsburg and Ms. Diane Oake for their assistance with this study.
Financial support
This work was supported by an Australian National Health and Medical Research Council (NHMRC) Project Grant (N.K., APP1081001), National Heart Foundation of Australia Future Leader Fellowship (N.K., 101229), the Heart Institute Research Core (N.K.) at Cincinnati Children’s Hospital, Australian National Health and Medical Research Council (NHMRC) Investigator Grant (M.F.) and an Australian Postgraduate Award (F.A.).
Competing interests
The authors declare none.
Ethical standards
The authors assert that all procedures contributing to this work complied with the ethical standards of the relevant national guidelines on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008, and have been approved by The Sydney Children’s Hospitals Network Human Research Ethics Committee (HREC/15/SCHN/95).




 Open access
Open access