


Introduction
The establishment of mental health institutions is rooted in seventeenth-century Britain (Smith Reference Smith2010, Reference Smith2014).Footnote 1 Industrial capitalism necessitated distinctions among the indigent, leading to the emergence of workhouses for categorizing and managing them (Scull Reference Scull1977). These workhouses increasingly contained people deemed unfit for labor, including the mentally ill, and alternatively, jails and public hospitals were used to confine them (Scull Reference Scull1977). While there was a growing number of private institutions, neglect, corruption, and the wrongful confinement of the sane were prevalent due to the absence of regulation. Voluntary hospitals were later established as an alternative and formed the foundation of public mental healthcare mandated in 1808 (Melling and Forsythe Reference Melling and Forsythe2006; Porter Reference Porter1987; Smith Reference Smith1999; Walton Reference Walton and Scull1981). Due to administrative mismanagement and the use of severe approaches in treating the mentally ill, most notably through restraint and coercion, early institutions provided inadequate care by the standards at the time (Scull Reference Scull1981; Smith 2010, Reference Smith2014).
While harsh treatment was common, humane approaches were also practiced, with “moral treatment” techniques particularly notable (Porter Reference Porter1987; Scull Reference Scull1981; Smith Reference Smith2014). The effectiveness of moral treatment at the Quaker-run York Retreat led to inquiries about patient treatment in British institutions, and through subsequent reforms, three main aspects of care were implemented: (i) patient classification according to mental disorder, (ii) elimination of mechanical restraint, and (iii) patient employment and occupation. Together, these elements, referred to as moral management, formed the basis for mental healthcare in Britain throughout the nineteenth century (Bartlett Reference Bartlett2017; Fryar Reference Fryar2016; Porter Reference Porter1987; Smith Reference Smith2010, Reference Smith2014; Swartz Reference Swartz2010). However, although widely practiced, general doubts arose about the actual success of moral management (Bartlett Reference Bartlett2017; Fryar Reference Fryar2016; Swartz Reference Swartz2010). This article seeks to explore the effectiveness of moral management by examining mental health institutions within the colonial British West Indies (BWI).Footnote 2
Although the evolution of mental health institutions in the BWI after slave emancipation in 1834 was influenced by British legislation, British practices were not imposed in the colonies, and instead, each colony was left to determine its own approach (Smith Reference Smith2010; Swartz Reference Swartz2010). In fact, as most colonial governments were controlled by local plantation elites, there was little incentive to invest in general public welfare (Holt Reference Holt1993). Moreover, institutions were originally established to control the indigent and create model British citizens (Bartlett Reference Bartlett2017; Hall Reference Hall2002; Scull Reference Scull1977), often serving as sites of confinement for “political dissidents who challenged the legitimacy of colonialism” (Hickling Reference Hickling2021: 33). The result was under-resourced institutions unable to provide adequate patient care (Smith Reference Smith2010; Swartz Reference Swartz2010). Importantly, a scandal at the Kingston Lunatic Asylum in Jamaica in the late 1850s brought patient abuses into public view, leading to a complete overhaul of mental healthcare, not only in Jamaica but throughout the British West Indian colonies (Fryar Reference Fryar2016; Hickling Reference Hickling2021; Smith Reference Smith2010, Reference Smith2014; Swartz Reference Swartz2010). Colonies were subsequently pressured to incorporate the three main principles of British moral management practice into the operations of their mental health institutions (Colonial Office 1864b).
The implementation of moral management depended on the quality of existing facilities, which varied widely across colonies (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010; Swartz Reference Swartz2010). Some institutions were repurposed buildings with inadequate infrastructure to support the implementation of moral management principles (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010, Reference Smith2014). Overcrowding and inadequately trained staff were persistent issues across the colonies (Allen Reference Allen1865; Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010, Reference Smith2014).Footnote 3 Moreover, any challenges were exacerbated by the often limited and volatile local public finances available to address them (Frankema Reference Frankema2010; Swartz Reference Swartz2010; Wright Reference Wright2022). Thus, while some of the institutions were transitioning to treating the mentally ill within the new guidelines, others continued to rely, at least in part, on traditional approaches (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010, Reference Smith2014). The potentially drastic but likely incomplete and varied implementation of moral management across the BWI provides a context for evaluating its success in treating the mentally ill. More specifically, as a consequence of the Kingston scandal, all operating mental health institutions in the British West Indian colonies were in principle required to implement the elements of moral management, a process closely monitored by Britain, but because of different environments, they may have varied in their success in doing so. In essence, this setting provides not only a case study of moral management of the mentally ill in the BWI but also adds more generally to the literature on the impact of institutional change-driven incentives on mental healthcare quality (Geloso and March Reference Geloso and March2021; March and Geloso Reference March and Geloso2020; Sutton Reference Sutton1991.
Importantly for our study, the medical superintendents of the British West Indian institutions, who were trained in Britain, were required to annually complete a detailed report capturing all information deemed relevant to institutional management by colonial authorities from 1870 onward until the start of World War II (WWII) (Swartz Reference Swartz2010). We digitized this information to create a cross-colony, time-varying data set of mental healthcare practices and patient outcomes. This allows us to investigate the application of moral management and its success in the colonial BWI, conditional on the definition of mental illness and its cure at the time. More specifically, we use regression analysis on the data to disentangle the various effects of mental health institution management as well as facility and patient characteristics on the death and discharge of patients.
Historical background
History of mental health institutions in Britain
Mental health institutions evolved as a social control apparatus resulting from capitalism (Scull Reference Scull1977). With the entire population considered as labor resources, workhouses were implemented to distinguish among the indigent. Workhouses were repositories for “the decaying, the decrepit, and the unemployable,” and the presence of a mentally ill person threatened “the order and discipline of the whole workhouse” (Scull Reference Scull1977: 343). Consequently, jails and public hospitals became alternatives for confining the mentally ill (Scull Reference Scull1977). In Britain, the first hospital declaring public care for the mentally ill, Bethlem at Moorfields, was opened in 1676 (Porter Reference Porter1987; Smith Reference Smith2014). Notably, while the hospital symbolized humane care, patients were treated harshly (Porter Reference Porter1987; Smith Reference Smith2014). The increase in public facilities simultaneously occurred with the “trade in lunacy” referring to the growth of private institutions (Melling and Forsythe Reference Melling and Forsythe2006; Porter Reference Porter1987; Scull Reference Scull1977). A key distinction of private institutions was the presence of medical expertise: some lacked it entirely, while others were owned and run by prominent physicians (Porter Reference Porter1987). With no legislation governing the trade in lunacy, there were cases of wrongful confinement of the sane (Porter Reference Porter1987). Legislation was only passed in 1774, but abuses at private institutions continued due to its limited scope. In the late eighteenth century, voluntary mental health hospitals, financed by public subscription, were established (Melling and Forsythe Reference Melling and Forsythe2006). These were viewed as an alternative to private institutions, whereby “effective treatment required early removal of the patient from the environment in which the disorder had originated” (Smith Reference Smith2014: 7) and formed the foundation for mandated mental healthcare in Britain (Porter Reference Porter1987; Smith Reference Smith1999).
Parliamentary investigations of existing institutions in 1807 led to legislation in 1808 promoting the county-wide establishment of public institutions (Walton Reference Walton and Scull1981), with a lunacy reform movement actively promoting the expansion of public institutions (Melling and Forsythe Reference Melling and Forsythe2006). By 1840, there was a well-established network of mental health institutions in Britain (Melling and Forsythe Reference Melling and Forsythe2006; Smith Reference Smith2014), which expanded in 1845 with the passing of the County Asylum Act (Fryar Reference Fryar2016; Mellett Reference Mellett1981; Melling and Forsythe Reference Melling and Forsythe2006; Swartz Reference Swartz2010; Walton Reference Walton and Scull1981). Administrative changes included the reliance on expertise from several fields, the rise of the doctor as an “expert” in mental illness, and an immense collection of written reports on patients (Porter Reference Porter1987; Scull Reference Scull1977; Swartz Reference Swartz2010). A Lunacy Commission was also established to monitor the welfare of the mentally ill (Fryar Reference Fryar2016; Mellett Reference Mellett1981; Melling and Forsythe Reference Melling and Forsythe2006; Swartz Reference Swartz2010; Walton Reference Walton and Scull1981). Various humane approaches to treating the mentally ill were practiced; however, moral management gained prominence and became the official ideology in Britain (Mellett Reference Mellett1981; Melling and Forsythe Reference Melling and Forsythe2006; Porter Reference Porter1987; Smith Reference Smith2014; Walton Reference Walton and Scull1981).
Moral management
Historically, treating patients in mental health institutions involved restraint and coercion (Scull Reference Scull1981; Smith Reference Smith2014; Walton Reference Walton and Scull1981). Although harsh treatment towards the mentally ill was common, humane care also existed with moral treatment being particularly notable (Porter Reference Porter1987). The use of moral treatment techniques was first advocated by Philippe Pinel in Paris in 1792 and first demonstrated at the Quaker-run York Retreat in Britain in 1796. Subsequently, in 1813, a publication about the York Retreat brought the treatment of the mentally ill at other institutions into question (Walton Reference Walton and Scull1981). Parliamentary inquiries in 1815–16 and then in 1827 revealed deficiencies in practices in several public mental health institutions when compared to moral treatment practices. Subsequently, in 1838, the same year slavery was abolished, psychiatric practice in England changed, where “non-restraint became the benchmark for enlightened practice in the management and treatment of mental illness” (Smith Reference Smith2014; Walton Reference Walton and Scull1981).
Reform of mental health institutions led to a national investigation from 1842 to 1844, resulting in legislation that emerged in 1845 (Mellett Reference Mellett1981). Subsequently, “the philosophical basis of British asylum treatment emanated from the humane principles associated with moral treatment […] comprised three main elements: classification or the separation of people according to the nature of their mental disorder and their associated behaviours; the elimination as far as possible of the use of mechanical restraint; and the employment and occupation of patients” (Smith Reference Smith2014: 2). As Smith (Reference Smith2014: 2) noted, “these elements were translated into ‘moral management’, whereby all aspects of the organisational system were geared towards the maintenance of order, control and tranquillity.” With work and occupation of patients being the key element, employment schemes were consistently implemented throughout public institutions in Britain (Smith Reference Smith2014). The approach also included “the provision of books, journals, games, sports, entertainment and other amusements” and “organised religious services” (Melling and Forsythe Reference Melling and Forsythe2006; Smith Reference Smith2014: 3).
Moral management became the embedded practice in most mental health institutions in England and Wales by the late 1850s (Fryar Reference Fryar2016; Smith Reference Smith2010). However, other parts of Britain were lagging in the implementation of moral management (Fryar Reference Fryar2016). Moreover, due to various deficiencies in the subsequent decades, “humane and therapeutic aspirations had become increasingly compromised” (Smith Reference Smith2010: 3). First, while numerous patients recovered and were discharged, there were many patients with chronic conditions. Second, with the “ever-increasing” patient population, overcrowding was a constant issue (Wright and Bartlett Reference Wright and Bartlett1999; Melling and Forsythe Reference Melling and Forsythe2006; Smith Reference Smith2014; Wright Reference Wright1997). Resultantly, mental health institutions were unable to offer personalized patient treatment and were simply a source of food and shelter for patients who were subjected to monotonous routines aimed at maintaining order and control (Hickling Reference Hickling2021; Scull Reference Scull1977, Reference Scull1981). Although implementation of moral management in Britain was incomplete and unsustainable, moral management still provided the model for mental healthcare in the British colonies (Bartlett Reference Bartlett2017; Fryar Reference Fryar2016; Hickling Reference Hickling2021; Smith Reference Smith2010; Swartz Reference Swartz2010).
Mental health institutions in BWI colonies pre-scandal
The first mental health institution in the BWI was adjoined to the public hospital in Jamaica (Hickling Reference Hickling2021; Smith Reference Smith2010). At the same time, in other BWI colonies – Antigua, Barbados, British Guiana, Grenada, Trinidad, and St. Vincent – the mentally ill were “contained within their families or plantation communities,” or in cases of extremely disruptive behavior, they were confined in estate hospitals or local jails (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Hickling Reference Hickling2021; Smith Reference Smith2014, p. 35). Confinement in jails in the BWI remained the practice into the 1840s, where conditions increasingly worsened (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010). Notably, mental health institutions throughout the British colonies were under-resourced, deplorable, and poorly managed, and treatment was harsh, resulting in various abuses, unwanted pregnancies, and high death rates (Hickling Reference Hickling2021; Jones Reference Jones2008; Smith Reference Smith2014; Swartz Reference Swartz2010).
The development of mental health institutions in BWI occurred in the 1840s and 1850s, arguably influenced by the 1845 British legislation (Smith Reference Smith2010). However, British practices were not imposed on the colonies despite the establishment of the Colonial Office in 1854, which had the capacity to regulate the colonies (Swartz Reference Swartz2010). Debates about self-governance of colonies were ongoing, and “interference in matters thought to be the responsibility of colonial governors was reluctantly undertaken,” including management of mental health (Swartz Reference Swartz2010: 163). Additionally, the magnitude of the empire restricted institutional control of colonies, and ideas were circulating regarding whether the mentally ill in colonies were due the same treatment as the British (Fryar Reference Fryar2016; Swartz Reference Swartz2010). These perspectives contrasted with concerns about the inadequacy of mental health institutions in colonies to treat British subjects, possibly leading to greater expenses in order to repatriate them to Britain. The inability of colonies to uphold the humanitarian values of Britain and hence avoid public scandal was also a concern (Swartz Reference Swartz2010). Against these conflicting narratives, the expectation was for colonies to maintain institutions of an acceptable standard. However, the Colonial Office was careful to maintain a good relationship with colonies in their correspondence about cases of inadequate practices (Swartz Reference Swartz2010). Each colony was thus left to determine its own approach, which resulted in “piece-meal” development and responses that were based on parsimony and maintenance of order (Smith Reference Smith2010; Swartz Reference Swartz2010). With low finances post-emancipation and concentrated efforts to address the interests of former slave owners, health and welfare services were low priorities for colonial governments (Jones Reference Jones2008; Smith Reference Smith2010; Swartz Reference Swartz2010). However, there was a willingness to allocate resources to ensure safety from people with disruptive or disorderly behavior. Mental health institutions, therefore, only served as custodial facilities lacking adequate resources to provide therapeutic care (Hickling Reference Hickling1988; Smith Reference Smith2010; Swartz Reference Swartz2010).
The Kingston mental health institution scandal
Pre-emancipation, Jamaica was the only BWI colony with a mental health institution, where it became an addendum to the pre-existing public hospital in 1815 (Jemmott Reference Jemmott2013; Smith Reference Smith2014). Statistics revealed seventy-eight admissions and thirty-three discharges during 1827–28 and a mainly white patient composition with some free-colored admissions (Smith Reference Smith2014). While essentially only the white mentally ill would have been treated pre-emancipation, the racial composition changed post-emancipation with patients mainly comprising the formerly enslaved and their descendants (Hickling Reference Hickling2021; Smith Reference Smith2023). In the late 1830s, many of the patients were kept under restraint, which was discouraged after 1843. In 1840, two years post-emancipation, the “insanitary conditions, overcrowding, neglect, poor staffing standards and ill-treatment in the asylum” were brought to the attention of the Jamaica Assembly and public; however, despite some reform, the underlying challenges subsequently intensified due to growing patient numbers (Smith Reference Smith2010: 10). Due to accountability and economic challenges, adequate medical services were not prioritized by the Jamaican assembly (Hickling Reference Hickling2021; Jones Reference Jones2008). Work on a new institution started in 1844, but delays and corruption hindered its completion (Hickling Reference Hickling2021; Smith Reference Smith2010, Reference Smith2014).
In 1854, concerns were raised about the Kingston Lunatic Asylum and the adjoining hospital (Fryar Reference Fryar2016, Reference Fryar2018). Despite resulting amendments to hospital management, underlying issues of accountability remained. The inadequacies of both institutes were again highlighted in 1858 with moral management as the proposed solution (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Brunton Reference Brunton2015; Fryar Reference Fryar2016, Reference Fryar2018; Smith Reference Smith2010). For more than two years, there were efforts to seek intervention from the Colonial Office, which were unsuccessful. In 1860, undeniable evidence of patients’ ill-treatment emerged. Firstly, a high mortality rate of 27 percent, which was substantially higher than the 11–12 percent rate at a well-managed institution in England, was reported to the Jamaica Assembly (Fryar Reference Fryar2016). Secondly, a former patient of the Kingston Lunatic Asylum published her lived experiences as an inmate, revealing the inhumane treatment she experienced and witnessed (Fryar Reference Fryar2016, Reference Fryar2018; Jones Reference Jones2008). Patients were subjected to physical beatings and verbal and sexual abuses (Jemmott Reference Jemmott2013; Jones Reference Jones2008). Due to the indisputable evidence, the Colonial Office intervened, leading to policy formulation for British colonies (Brunton Reference Brunton2015).
Mental health institutions in BWI colonies post-scandal
Following the Kingston scandal, there was an audit of the Jamaican public hospital and asylum. The investigation confirmed many of the allegations (Jemmott Reference Jemmott2013), and new guidelines for the management of these institutes were outlined in the 1862 Public Hospital Act. The Act established a board of visitors tasked with regular inspections and rules for staff. The Kingston scandal further triggered reform beyond Jamaica (Swartz Reference Swartz2010). In 1863, there was an audit of hospitals and mental health institutions in all British colonies, which found similar conditions in many of the BWI colonies as in Jamaica (Smith Reference Smith2010; Swartz Reference Swartz2010). Classification of patients was lacking, and segregation by sex in some cases was hindered by the small dormitory spaces. A key insight was the absence of a medical officer since many were neither resident nor restricted to only practice at respective institutions (Brunton Reference Brunton2015; Colonial Office 1864b; Swartz Reference Swartz2010).
The audit replies were used to put forth a report in 1864 to ensure the regulation of mental healthcare across the colonies (Colonial Office 1864b). The underlying ideology was “the normal condition and rights of the mentally ill should be infringed upon in as small a degree as may be consistent with efficient management” (Colonial Office 1864b: 13). Sanitation was a primary concern, and an ordinance to manage the design and construction of mental health institutions was suggested. A medical officer who was “resident and restricted” was expected to manage mental health institutions, and regular inspections were recommended. Assessment criteria were outlined regarding the performance of the medical officer and the institution they managed (Colonial Office 1864b). Moreover, the three elements of British practice, namely, classification, non-restraint, and patient occupation, were communicated via publications, Colonial Office correspondence, and doctors originating from Britain who served as the medical superintendents at the colonial institutions (Smith Reference Smith2014, Reference Smith2010; Swartz Reference Swartz2010). The medical superintendent was responsible for the classification of patients and the implementation of moral management, while the warden and matron implemented the classification system and made arrangements for the occupation and amusements of patients (Smith Reference Smith2010). Institutions were subject to frequent announced and surprise inspections from colonial government officials to assess the adequacy of the facilities and services provided. These officials provided a report to the colonial government, thus allowing oversight on the management of the institutions.
Although non-restraint was abandoned in Jamaica in 1843, the facilities made the classification and employment of patients, the other two elements of the British model, impossible (Lake Reference Lake1863; Scott et al. Reference Scott, Keech and Osborn1860; Smith Reference Smith2014). Provisions for outdoor employment were hinged on the new institution; therefore, its opening was hastened to finally occur in 1860. Male patients were admitted to a partially completed building in 1860 and females in 1862, when construction was completed (Jones Reference Jones2008; Smith Reference Smith2010). An experienced medical superintendent from Britain, Dr. Thomas Allen, was appointed in 1863 (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010). He noted many deficiencies and was quick to make necessary changes (Allen Reference Allen1865; Smith Reference Smith2010). The only element upheld in the first few years was non-restraint. Other than female patients assisting with domestic chores and repairing of clothes, it was impossible to systematically classify, treat, or employ patients (Lake Reference Lake1863; Scott et al. Reference Scott, Keech and Osborn1860). Once funds were received, Allen had “the opportunity to turn the Jamaica asylum into a tropical approximation of an English county asylum, based on an extensive and increasingly sophisticated system of patient employment and occupation, which included commercial pork production and a successful sea fishery” (Smith Reference Smith2010: 23).
In British Guiana, a new institution was opened in 1867, and a medical superintendent from Britain, Dr. Robert Grieve, was appointed in 1875 (Smith Reference Smith2010, Reference Smith2014). When he took over, restraint was still used, and patient employment was negligible (Smith Reference Smith2010, Reference Smith2014). Grieve transformed the mental health institution within months, establishing a “sophisticated system of productive work” involving husbandry (Smith Reference Smith2010: 24). Patients were engaged in carpentry, sewing and decorating, and a bakery; a large laundry and a printing office were established (Smith Reference Smith2010, p. 24). When Dr. George Seccombe was appointed as medical superintendent in Trinidad in 1882, the facilities were deemed too inadequate to promote care and cure of patients (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010, Reference Smith2014). In the subsequent years, Seccombe implemented a patient classification system and developed agricultural work and industrial employment focused on renovation of dilapidated buildings (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010, Reference Smith2014). In Barbados, the classification of patients was adopted in 1860, but restraint and seclusion continued (Smith Reference Smith2010, Reference Smith2014). By 1869, restraint was discontinued, though seclusion remained as a practice, and there was some patient employment (Smith Reference Smith2010, Reference Smith2014). A new institution was built in 1893, but the implementation of moral management remained limited, and the use of mechanical restraint was resumed (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2010).
In the smaller colonies of the BWI, the situation was worse than in larger ones due to limited resources, inadequate facilities and staffing, and low patient numbers (Smith Reference Smith2010, Reference Smith2014). As noted by the governor of the Leeward Islands
All that these local Asylums can pretend to do, is to confine the lunatics with more or less comfort, and to feed them and attend to their bodily health. These Institutions could not be rendered really effective for curative purposes except at a cost which the islands individually could not bear, cited by Smith (Reference Smith2010: 14).
In some cases, the health of patients was compromised due to the absence of bathing and toilet facilities, violence among patients, and poor drainage and sewerage (Smith Reference Smith2010, Reference Smith2014). Just as with the larger West Indian colonies, structural improvements were made. The original institution in Antigua during the 1870s became the central institution for the Leeward Islands, housing patients from Dominica, Montserrat, Nevis, St Kitts, and the Virgin Islands (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Smith Reference Smith2014). Centralization also occurred for the Windward Islands in 1879, with Grenada housing patients from Tobago, St Lucia, and St Vincent (Smith Reference Smith2014). St. Lucia retained some of its patients, and with the growing patient population, a rented house replaced the original facility in 1874, which was then replaced by a converted military building in 1912 (Smith Reference Smith2010, Reference Smith2014). The original converted house in British Honduras was replaced by a new institution in 1880 (Smith Reference Smith2010, Reference Smith2014). Despite the centralization in Antigua and Grenada, no patient classification was implemented, mechanical constraint and seclusion were utilized, and plans for occupation and amusement of patients were lacking (Smith Reference Smith2010, Reference Smith2014). In Antigua, classification was implemented when a second institution was constructed to house patients who were quiet, harmless, and convalescent (Smith Reference Smith2010, Reference Smith2014). The other elements of moral management, however, remained unimplemented until a new central institution for the Leeward Islands opened in Antigua in 1907 (Smith Reference Smith2010, Reference Smith2014). In Grenada, some employment was arranged for patients from the 1880s onwards, but the building conditions and poor staffing made classification and non-restraint impossible (Smith Reference Smith2010, Reference Smith2014).
Similar to the written reports and statistics required by Britain, institutions in the West Indian colonies were required to provide regular annual records (Swartz Reference Swartz2010). These records “began to give a much clearer picture of numbers in asylums, and also of diagnosis, supposed causes of insanity, recovery, and death rates, and class, race and sex classifications of inmates” (Swartz Reference Swartz2010: 169). Notably, while these reports indicated improved conditions at many institutions, “more detailed correspondence suggested that adequate housing, sanitation, differentiation between groups of patients, staffing, and attention to physical health continued to be problematic in some instances, and to require ongoing vigilance from Colonial Office administrators” (Scott et al. Reference Scott, Keech and Osborn1860; Swartz Reference Swartz2010: 170). Moreover, there were continuous doubts about the effectiveness of moral management, with its downfall attributed to its quick growth without adequate financial resources, consistent overcrowding, and low quantity and quality of staff (Swartz Reference Swartz2010; Wright Reference Wright2022). In the face of these challenges, ensuring the cure of all patients became nearly impossible, and public interest also declined (Bartlett Reference Bartlett2017; Heuring Reference Heuring2011; Swartz Reference Swartz2010).
Mental health institutions were characterized more by regulatory and economic challenges rather than the ideological intentions of moral management (Bartlett Reference Bartlett2017; Digby Reference Digby1983). They were originally established to confine society’s misfits who were incapable of labor participation and therefore remained facilities of custodial care rather than therapeutic treatment (Wright Reference Wright2022). Hickling (Reference Hickling2021) also noted that institutions in the BWI were sites of confinement for political dissidents challenging the legitimacy of colonial rule. In fact, while the establishment of mental health institutions in the BWI is seen as an extension of British practices, acts of resistance pre-emancipation, which often resulted in flogging or death when viewed through a Eurocentric psychiatry lens, could be considered mental illness (Hickling and Gibson Reference Hickling, Gibson, Hickling and Sorel2005). Post-emancipation, resistance to colonial exploitation and oppression were seen as acts of madness with the previous responses replaced with confinement in jails and mental health institutions (Hickling and Gibson Reference Hickling, Gibson, Hickling and Sorel2005). While Smith (Reference Smith2014) acknowledges the role of mental health institutions as instruments of control, he also highlights their benevolent intentions. Institutions in the BWI were often used to house the physically feeble, elderly, and criminals with mental illness (Allen Reference Allen1878).
The subject of race is also pertinent in the context of the BWI. Hickling (Reference Hickling2021) highlighted an “apartheid-like mini-society” at the Kingston Lunatic Asylum, where white and brown-skinned patients received different treatment. Additionally, there was a prevalent dehumanizing view of non-white patients. For example, while Allen (Reference Allen1872) noted for Jamaica that “the same intellectual, moral, hereditary, and physical causes of insanity as affect the insane in England,” he also highlighted that “a large portion of peasantry of this country, have never had their minds developed at all, and are in a state of actual barbarism.” Accordingly, it was questioned whether moral management practices, initially developed to treat white patients in England and Europe, would have any impact on black patients, who comprised the majority of patients in the BWI post-emancipation.
Legislative and cultural contexts also played a role. Legislation in the West Indies was different from that in Britain, where the former legislation promoted leaving people in the community until they became dangerous or unmanageable (Smith Reference Smith2010), leading to the admittance of patients in detrimental conditions. Allen (Reference Allen1870) states, “There can be no doubt that the small number of patients admitted, and the unfavorable nature of the mental and bodily condition which characterizes them, is due to a great measure in the permissive lunacy law.” Due to changing economic and social relationships owing to industrial capitalism, relatives in South West England played a significant role in patient admissions and discharges (Bartlett and Wright Reference Wright and Bartlett1999; Melling and Forsythe Reference Melling and Forsythe2006; Wright Reference Wright1997, Reference Wright2022). Additionally, Obeah, a prevalent spiritual practice in the BWI, was not only noted as a cause of mental illness but was also relied on as a cure, although there were attempts to suppress its practice by colonial authorities (Beaubrun et al. Reference Beaubrun, Bannister, Lewis, Mahy, Royes, Smith and Wisinger1976; Paton Reference Paton2001, Reference Paton2015; Smith Reference Smith2010, Reference Smith2014, Reference Smith2018, Reference Smith2023). Altogether, the various factors influencing mental healthcare in the BWI present a unique setting for examining the implementation of moral management.
Finally, although mental health institutions were similarly financed as in England, i.e., by both the central government and the parishes,Footnote 4 they were likely much more financially constrained in the BWI (Johnston Reference Johnston2021; Ellis Reference Ellis2008). Prior to WWII, direct spending by the British government in its colonies was limited, while debt as a form of government financing was restricted and had to be approved by the Colonial Office (Constantine 2005; Will Reference Will1970). This left local fiscal spending mostly dependent on highly volatile revenues from tariffs in economies almost exclusively dependent on a few export crops and importing most of their goods (Frankema Reference Frankema2010). Nevertheless, there were some differences depending on the colonial government type, i.e., whether they were Crown Colonies or of the Old Representative System (Wrong Reference Wrong1923). Although all annual expenditure estimates had to first, in principle, be approved by the Colonial Office, in the Old Representative System the local assembly had considerable negotiation power over fiscal expenditures since the taxation legislation depended on their approval (Constantine Reference Constantine2005). However, by the late 1890s, all except four (Barbados, Bahamas, Bermuda, and British Guiana) of the British West Indian colonies were of the Crown Colony type.
Data and methodology
Data
Following the Jamaican scandal, all mental health institutions in the BWI were required to submit annual reports as part of the Colonial Blue Books from 1869 onward (Brunton Reference Brunton2015).Footnote 5 Importantly, these reports contained detailed and temporally consistent information on all aspects deemed relevant to mental health institution management, such as the implementation of moral management and patient outcomes. See Table A1 in Supplementary materials for our empirical sample.
General statistical table
The general statistical table of the report provides statistics on patients by sex during the year, that is, the number of admissions, the average number of patients, the number of deaths, and the number of discharges, where the latter is decomposed into cured, relieved, and not improved. The table also reports the number of male and female attendants employed at the institution.
Patient classification
Patients were classified by mental illness category, specifically into (i) maniacal and dangerous (“maniacal” hereafter), (ii) quiet chronic (“quiet”), (iii) melancholic and suicidal (“melancholic”), and (iv) idiotic, paralytic, or epileptic (“idiotic”). Although the definitions of these categories were not explicitly provided in the Blue Books, given that the reporting template was created by the Colonial Office and that the superintendents and medical doctors were all trained in Britain during our sample period, it seems reasonable to assume that the definitions were the same as those used in Britain. Accordingly, mania was described as an acute mental illness with a quick and unpredictable onset, characterized by symptoms such as irrational behavior, delusions, and restlessness, which in prolonged states resulted in extreme excitement and destructive behaviors (Burtinshaw and Burt Reference Burtinshaw and Burt2017). Melancholia was considered to be a state of profound misery without adequate cause and a manifestation of clinical depression (Burtinshaw and Burt Reference Burtinshaw and Burt2017). The “epileptic” was defined primarily by the occurrence of seizures. However, while mental health institution records often labeled these patients as “dangerous,” such behavior usually occurred only during or immediately prior to a seizure. Those deemed “idiotic” had profound congenital intellectual impairment, typically defined by an IQ below twenty-five or a mental age of less than three years, with severely limited communication abilities (Burtinshaw and Burt Reference Burtinshaw and Burt2017). The “paralytic” referred to individuals suffering from a progressive organic brain disorder that produced a variety of mental and physical symptoms, including dementia, psychosis, seizures, and generalized muscle weakness (Burtinshaw and Burt Reference Burtinshaw and Burt2017). Finally, the classification “quiet chronic” was assigned to patients that were quiet and harmless but whose insanity was difficult to determine (Scull Reference Scull1993). We calculated the percentage of male and female patients assigned to each of these categories for the regression analysis, considering the group “quiet” as the base category. One should note that unfortunately we are unable to take account of any changes in how patients were classified over time.
Management
Mental health institutions were required to note whether restraint by means of attendants or mechanical devices or seclusion was used. We created variables for each of these techniques.
Occupation
Mental health institutions used a number of approaches to keep patients occupied, which were viewed as both a source of income for the institutions and being therapeutic (Freebody Reference Freebody2023; Cochrane Reference Cochrane2018). The mental health institution reports provided the average daily number of males and females employed in agriculture, domestic services (household work, fetching water, etc.), and trade-related activities. These were used to create counts of patients employed in each of these categories by sex. Reports also provided the frequency of religious services and the various types of entertainment services provided – dancing, singing, music, bagatelle board, ninepin bowling, cricket, croquet cards, newspapers (e.g., London news), evening walks, books, concerts, taking pictures, draughts, ping pong, sea-bathing, listening to radio distribution programs, plays, and watching moving pictures. To capture these multiple aspects, we generated counts for religious services per week and a variable summing the distinct types of entertainment.
Space and accommodation table
Detailed information on the total indoor space available as well as bath and toilet facilities in the institution is also provided. The consistency of these data allowed us to create four variables: total amount of dormitory space, number of lavatories, number of baths, and number of latrines.
Nutrition
Mental health institutions were required to provide an account of their weekly meal plan,Footnote 6 that is, for seven days. Following Sluik et al.’s (Reference Sluik, Streppel, van Lee, Geelen and Feskens2015) methodology, we calculated for all islands an annual Nutrient-Rich Food (NRF) index, according to nutrient density. Specifically, the index is calculated by summing the percentage of recommended values of beneficial nutrients (e.g., protein, fiber, vitamins, and minerals) while subtracting the percentage of maximum daily values for the nutrients to limit (e.g., saturated fat, sugar, and sodium).Footnote 7 Data used to calculate the NRF was extracted from the United States Department of Agriculture (USDA) Food Data Central.Footnote 8
Regression analysis
As all dependent variables are counts, i.e., number of deaths, total discharges, cured discharges, relieved discharges, or not improved discharges, we employ a Poisson Conditional Fixed Effects Maximum Likelihood Estimator (PCFE) for all regression specifications (Wooldridge Reference Wooldridge1999). Specifically, the PCFE assumes that the dependent variable(s) Y of count(s) follows a Poisson distribution with mean:
 ${{\bf{Y}}_{it}} = {\rm exp}\{ {\beta _{\bf{X}}}{{\bf{X}}_{it}} + {\beta _{\bf{Z}}}{{\bf{Z}}_{it}} + {\lambda _t} + {\mu _i}\}$
${{\bf{Y}}_{it}} = {\rm exp}\{ {\beta _{\bf{X}}}{{\bf{X}}_{it}} + {\beta _{\bf{Z}}}{{\bf{Z}}_{it}} + {\lambda _t} + {\mu _i}\}$
where subscripts i and t denote colony and time (year), respectively. Y is a vector of the different dependent variables. X are the explanatory variables of interest that capture the relevant features of the mental health institutions. Z is a vector of time- and colony-varying control variables; they include the average number admitted and the average number of patients. The remaining controls are µ, a set of time-invariant colony-specific effects that are meant to capture any uncontrolled differences across colonies that do not vary over time, and λ are year-specific fixed effects that control for shocks common to all colonies. We follow Wooldridge (Reference Wooldridge1999) and cluster standard errors of the coefficients at the level of the colony (i). Since the PCFE is a non-linear model, the estimated coefficients are not interpretable as marginal effects. As is common in practice, we convert and report these and their 95% confidence bands as incidence rate ratios (IRRs).
Results
Summary statistics
On average, annually, there were around 160 male and 142 female patients in British West Indian mental health institutions over our sample period (1869–1942), albeit with considerable variation across years and institutions. The admittance rate compared to the average number of patients was 35 percent and 36 percent for males and females, respectively. However, normalized by the average attendance, about 15 percent of females and 13 percent of males died, while the equivalent figures in discharges were around 20 percent and 22 percent, respectively.
Figure 1, Panel (a), depicts, by sex, the temporal average number of admissions normalized by the average number of patients. In general, the series move in tandem, although the size of fluctuations differs substantially at times by sex. Panel (b) shows the analogous series for deaths. Similar to admissions, the co-movement by sex is striking, with, again, some differences in the size of the spikes. The number of discharges compared to the average number of patients, shown in Panel (c), while still correlated for men and women, appears to be much more volatile than admissions or deaths.
# Admitted, # deaths, & # discharges.

For both males and females, nearly half of all patients are classified as quietly chronic, followed by close to a third as maniacal and dangerous (see Table A4 in Supplementary materials). Slightly more female patients were classified as melancholic and suicidal than idiotic, paralytic, or epileptic, while the reverse is true for males.
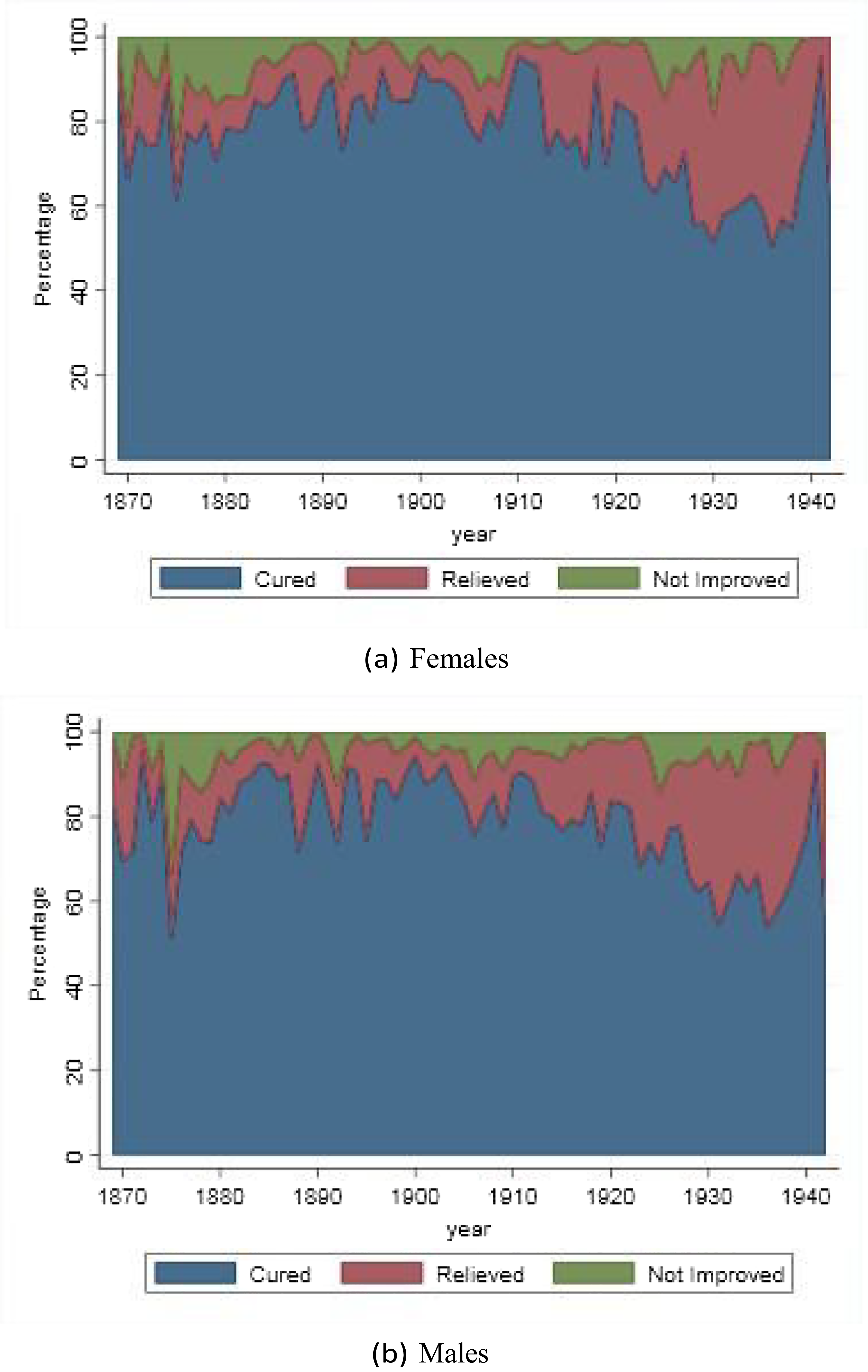
For both men and women, over 70 percent of persons discharged were considered cured, close to 20 percent were classified as relieved, while about 7 percent were discharged with no improvement (see Table A5 in Supplementary materials). Figure 2 depicts the temporal evolution of the decomposition of discharges. While there was some volatility, until the early twentieth century, there was little change in the decomposition of the distinct types for either sex. However, after this, both male and female discharges were, on average, more likely to be classified as relieved, and the number deemed cured decreased.
Decomposition of discharges.
On average, the calculated NRF index is approximately 197, suggesting that the nutrient density of the available food aligns significantly with recommended dietary guidelines (Table A6 in Supplementary materials). There is, on average, about 13 (=1/0.077) patients per bath, 19 per lavatory (=1/0.053), and 9 per latrine (=1/0.118) (see Table A6). The large standard deviations for these variables indicate major differences across institutions. The ratio of the total number of females employed relative to the average number of female patients over a year (0.475) is slightly smaller than the equivalent for males (0.515) (Table A7 in Supplementary materials). For about 8 percent and 9 percent of our sample, no employment opportunities were available for women and men, respectively. Women were predominantly doing chores, whereas men mostly worked in agriculture. When females worked, they were also more likely employed in trade occupations compared to males. Mental health institutions provided four different types of entertainment and about one religious service per week. As with employment, in 9 percent and 14 percent, respectively, no entertainment or religious services were provided. Institutions differed greatly in terms of inspections – announced or surprise visits – per year (Table A8 in Supplementary materials). Relative to surprise inspections, institutions experienced an average of just under 5 per year. Seclusion was widely practiced, with nearly 84 percent reporting doing so on average every year (Table A8 in Supplementary materials). Yearly, patients were also about 25 percent forcefully restrained by attendants. Finally, mechanical restraint remained a common practice in these institutions, being used nearly 50 percent of the time.
Regression results
Deaths and discharges
We graphically depict the estimated IRRs with their 95% confidence intervals by control variable category for each dependent variable – the number of female deaths, male deaths, female discharges, and male discharges. The nutritional value of meals is found to have no effect on deaths or discharges of women and men (Figure 3). Sanitation indicators also have no impact on deaths or discharges. Greater dormitory space reduces the number of deaths among male patients, where an additional 100 square feet of sleeping quarters decrease male patient deaths by 5.2 percent.
Nutrition, sanitation, & accommodation: Deaths & discharges.
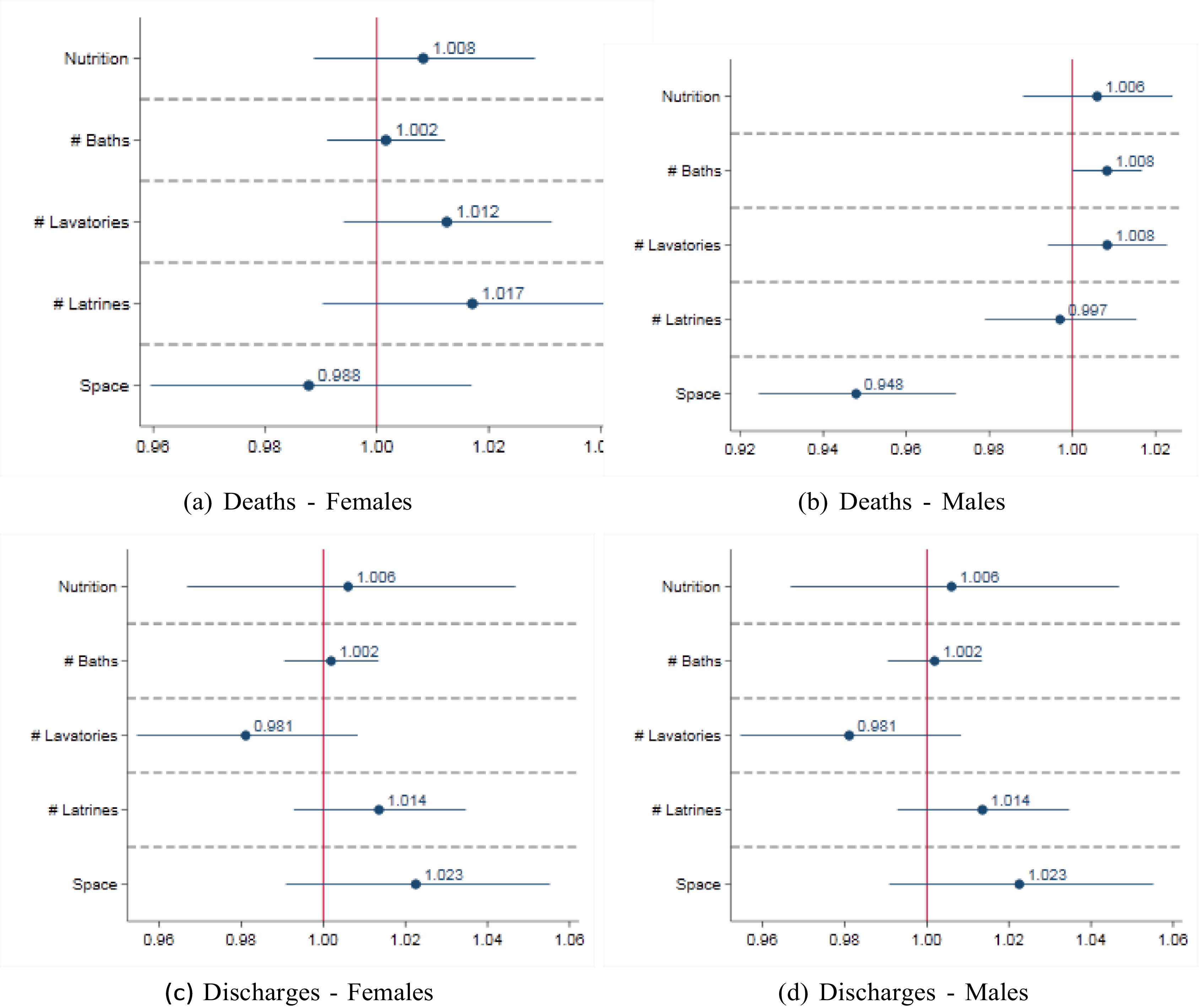
Figure 3 Long description
Panel A: A scatter plot titled Deaths - Females shows the impact of various factors on female deaths. The x-axis ranges from 0.96 to 1.04, and the y-axis lists factors: Nutrition, Number of Baths, Number of Lavatories, Number of Latrines, and Space. Each factor has a data point with an error bar indicating variability. Nutrition has a value of 1.008, Number of Baths 1.002, Number of Lavatories 1.012, Number of Latrines 1.017, and Space 0.988. Panel B: A scatter plot titled Deaths - Males shows the impact of various factors on male deaths. The x-axis ranges from 0.92 to 1.02, and the y-axis lists the same factors. Nutrition has a value of 1.006, Number of Baths 1.008, Number of Lavatories 1.008, Number of Latrines 0.997, and Space 0.948. Panel C: A scatter plot titled Discharges - Females shows the impact of various factors on female discharges. The x-axis ranges from 0.96 to 1.06, and the y-axis lists the same factors. Nutrition has a value of 1.006, Number of Baths 1.002, Number of Lavatories 0.981, Number of Latrines 1.014, and Space 1.023. Panel D: A scatter plot titled Discharges - Males shows the impact of various factors on male discharges. The x-axis ranges from 0.96 to 1.06, and the y-axis lists the same factors. Nutrition has a value of 1.006, Number of Baths 1.002, Number of Lavatories 0.981, Number of Latrines 1.014, and Space 1.023.
Figure 4 depicts the results for the occupation of patients. The number of females employed in agriculture reduces the number of female deaths, where the estimate suggests that one additional woman employed in agriculture reduces deaths by 17.9 percent. For males, deaths were reduced when they were employed in trade, with an effect of around 34%. Being employed in trade activities also reduces the number of female deaths, with an estimated effect of 15 percent. Male discharges were reduced when more men were employed in agriculture (15 percent).
Employment, religion, & entertainment: Deaths & discharges.

Figure 4 confirms that more religious services reduced the mortality of both male and female patients, with impacts for women and men of 15 percent and 15.8 percent, respectively. However, neither religious services nor entertainment affected the number of discharges, regardless of sex.
Figure 5 displays estimates for restraint and seclusion. Mechanically restraining patients reduced the number of reported deaths for both men and women (17.8 percent and 19.9 percent, respectively). Yet, there was no similar impact on discharges. In contrast, the seclusion of patients reduced the number of discharges – a reduction of 28.7 percent for female and 21.8 percent for male patients – but had no effect on deaths. Restraint by attendants only impacted male discharges, increasing these by 48.6 percent.
Management of violence: Deaths & discharges.

Inspections of the mental health institutions, whether announced or unplanned, did not play a role in patient outcomes, except in reducing the number of male deaths when unannounced (Figure 6). In this regard, an additional surprise inspection caused a reduction of 1.8 percent in male deaths. The presence of one more female attendant reduced male and female deaths by 1.3 percent and 0.8 percent, respectively. More female attendants also increased the number of discharged female patients (1.1 percent for each additional female attendant). Only male discharges were affected by more male attendants, implying a reduction of 0.7 percent for each additional male attendant.
Inspection & supervision: Deaths & discharges.

Figure 6 Long description
Panel A: Deaths - Females. A forest plot shows the impact of different factors on deaths among females. The x-axis ranges from 0.98 to 1.00, and the y-axis lists factors: Surpr. Inspection, NSurpr. Inspection, Female Attend., and Male Attend. The plot includes data points with confidence intervals for each factor. Panel B: Deaths - Males. A forest plot shows the impact of different factors on deaths among males. The x-axis ranges from 0.97 to 1.00, and the y-axis lists the same factors. The plot includes data points with confidence intervals for each factor. Panel C: Discharges - Females. A forest plot shows the impact of different factors on discharges among females. The x-axis ranges from 0.99 to 1.02, and the y-axis lists the same factors. The plot includes data points with confidence intervals for each factor. Panel D: Discharges - Males. A forest plot shows the impact of different factors on discharges among males. The x-axis ranges from 0.98 to 1.01, and the y-axis lists the same factors. The plot includes data points with confidence intervals for each factor.
Patient classification was not a good predictor of patient outcomes (Figure 7). The only exception was the percentage of males classified as maniacal and dangerous, associated with more deaths of male patients, where a 10 percent increase in the share of maniacal and dangerous patients resulted in a 4.6 percent rise in male deaths.
Controls: Deaths & discharges.

Figure 7 Long description
Panel A: A scatter plot depicts the percentages of deaths among females categorized as maniac, melancholic, and idiotic. The x-axis ranges from 0.00 to 5.00, and the y-axis lists the categories: % Female Maniac, % Female Melancholic, and % Female Idiotic. The data points are 0.912 for % Female Maniac, 0.902 for % Female Melancholic, and 1.856 for % Female Idiotic. Panel B: A scatter plot depicts the percentages of deaths among males categorized as maniac, melancholic, and idiotic. The x-axis ranges from 0.50 to 2.50, and the y-axis lists the categories: % Male Maniac, % Male Melancholic, and % Male Idiotic. The data points are 1.466 for % Male Maniac, 0.707 for % Male Melancholic, and 1.306 for % Male Idiotic. Panel C: A scatter plot depicts the percentages of discharges among females categorized as maniac, melancholic, and idiotic. The x-axis ranges from 0.50 to 3.00, and the y-axis lists the categories: % Female Maniac, % Female Melancholic, and % Female Idiotic. The data points are 0.735 for % Female Maniac, 1.260 for % Female Melancholic, and 1.218 for % Female Idiotic. Panel D: A scatter plot depicts the percentages of discharges among males categorized as maniac, melancholic, and idiotic. The x-axis ranges from 0.50 to 2.00, and the y-axis lists the categories: % Male Maniac, % Male Melancholic, and % Male Idiotic. The data points are 0.586 for % Male Maniac, 1.091 for % Male Melancholic, and 1.154 for % Male Idiotic.
Decomposition of discharges
Results for each of the three types of discharges by sex are shown in Figures 8 through 12. The nutritional value of the mental health institution patient diet increased the number of relieved male and female discharges, where a one standard deviation increase in nutritional value (2.52) resulted in 53.1 percent and 57.4 percent more relieved discharges, respectively. For female patients, one additional bath increased the number of relieved discharges by 5.4 percent; the corresponding effect for latrines was 23.5 percent. In contrast, an additional lavatory decreased relieved female discharges by 11.2 percent. For male discharges, impacts were qualitatively similar, although slightly lower quantitatively for baths (4.4 percent rise) and lavatories (8.4 percent fall); the number of latrines had no impact. Greater dormitory space only decreased the number of relieved male discharges, not female discharges, with 100 extra square feet reducing male relieved discharges by 5.6 percent.
Nutrition, sanitation, & accommodation: Decomposition of discharges.

Employment only affected cured female discharges, with an additional female employed in trade resulting in a reduction of 13.3 percent, while an additional female employed in agriculture led to a 25.9 percent increase (Figure 9). The number of cured male discharges was only affected by employment in chores, with a quantitative increase of 33.1%. Trade increased the number of relieved male discharges by over 400 percent. Religious services resulted in more cured male and female discharges, where the effects were 16.2 percent and 16.7 percent, respectively, for each additional weekly service. In contrast, entertainment services only reduced, not improved, discharges for females (over 96 percent).
Employment, religion, & entertainment: Decomposition of discharges.

Regarding restraint by mechanical devices and attendants (Figure 10), only mechanical restraint decreased the number of not improved male and female discharges, where its use resulted in decreases of 31.1 percent and 43.9 percent, respectively. Seclusion reduced relieved male discharges by 57 percent. Inspections of mental health institutions had no discernable impact on discharge types (Figure 11). The number of female attendants increased both cured and not improved female discharges, where the effects were 0.6 percent and 33.2 percent, respectively. In contrast, the number of male attendants increased relieved male and female discharges by just over 1 percent but solely decreased cured male discharges by 1.2 percent.
Management of violence: Decomposition of discharges.

Figure 10 Long description
Panel A: Cured - Females. A scatter plot shows the effectiveness of different management strategies for cured female patients. The x-axis ranges from 0.50 to 2.50, and the y-axis lists Seclusion, Restr. Att., and Restr. Mech. The data points are at 0.856 for Seclusion, 1.224 for Restr. Att., and 1.052 for Restr. Mech. Panel B: Relieved - Females. Another scatter plot for relieved female patients. The x-axis ranges from 0.00 to 4.00, and the y-axis lists the same categories. The data points are at 0.517 for Seclusion, 1.338 for Restr. Att., and 0.683 for Restr. Mech. Panel C: Not Improved - Females. A scatter plot for females who did not improve. The x-axis ranges from 0.00 to 8.00, and the y-axis lists the same categories. The data points are at 0.639 for Seclusion, 2.172 for Restr. Att., and 0.561 for Restr. Mech. Panel D: Cured - Males. A scatter plot for cured male patients. The x-axis ranges from 0.50 to 2.00, and the y-axis lists the same categories. The data points are at 0.942 for Seclusion, 1.329 for Restr. Att., and 0.973 for Restr. Mech. Panel E: Relieved - Males. A scatter plot for relieved male patients. The x-axis ranges from 0.00 to 3.00, and the y-axis lists the same categories. The data points are at 0.430 for Seclusion, 1.722 for Restr. Att., and 0.822 for Restr. Mech. Panel F: Not Improved - Males. A scatter plot for males who did not improve. The x-axis ranges from 0.00 to 5.00, and the y-axis lists the same categories. The data points are at 0.746 for Seclusion, 2.113 for Restr. Att., and 0.689 for Restr. Mech.
Inspection & supervision: Decomposition of discharges.

Patient classification seems to have played little role, except in that more female patients classified as idiotic, paralytic, or epileptic is positively related to cured discharges (Figure 12). For each additional 10 percent increase in females classified as idiotic, paralytic, or epileptic, there was a 6.2 percent increase.
Controls: Decomposition of discharges.

Figure 12 Long description
Panel A: A scatter plot shows the percentage of female patients classified as maniac, melancholic, and idiotic who were cured. The x-axis ranges from 0.50 to 2.50, and the y-axis lists the classifications. The data points are scattered with values around 0.750 for maniac, 1.492 for melancholic, and 1.616 for idiotic. Panel B: Another scatter plot shows the percentage of female patients classified as maniac, melancholic, and idiotic who were relieved. The x-axis ranges from 0.00 to 6.00, and the y-axis lists the classifications. The data points are scattered with values around 0.403 for maniac, 1.288 for melancholic, and 0.561 for idiotic. Panel C: A scatter plot shows the percentage of female patients classified as maniac, melancholic, and idiotic who were not improved. The x-axis ranges from 0.00 to 20.00, and the y-axis lists the classifications. The data points are scattered with values around 1.944 for maniac, 0.658 for melancholic, and 2.124 for idiotic. Panel D: A scatter plot shows the percentage of male patients classified as maniac, melancholic, and idiotic who were cured. The x-axis ranges from 0.50 to 2.50, and the y-axis lists the classifications. The data points are scattered with values around 0.633 for maniac, 1.185 for melancholic, and 0.960 for idiotic. Panel E: Another scatter plot shows the percentage of male patients classified as maniac, melancholic, and idiotic who were relieved. The x-axis ranges from 0.00 to 5.00, and the y-axis lists the classifications. The data points are scattered with values around 0.768 for maniac, 1.479 for melancholic, and 1.268 for idiotic. Panel F: A scatter plot shows the percentage of male patients classified as maniac, melancholic, and idiotic who were not improved. The x-axis ranges from 0.00 to 6.00, and the y-axis lists the classifications. The data points are scattered with values around 0.136 for maniac, 1.208 for melancholic, and 1.312 for idiotic.
Discussion
Superintendents viewed occupation as the most important element of moral management as it could potentially distract patients from disorderly thoughts (Smith Reference Smith2014). Our results match these ideas, as occupation was an effective indicator of reduced deaths and increased cures among patients. In particular, employment in agriculture and trade reduced deaths, respectively, for females and males, and agriculture and chores increased cured discharges among women and men. Additionally, results indicate that trade among male patients raised the number of relieved discharges by more than 400 percent. Notably, as a result of patient employment, a report provided by Allen for the Kingston Lunatic Asylum in 1872 noted “a very marked absence of listlessness and idleness which pervades many asylums for the insane” (Allen Reference Allen1872). Additionally, for Jamaica, it was reported that, occupation diminished violent tendencies, improved physical health, and induced calmness and cheer (Colonial Office 1864a). Similar reports were also made for Trinidad (Colonial Office 1883a). According to Ernst (Reference Ernst2016), historians had competing views regarding the role of employment in moral management. It was seen as oppressive due to the subservience required, while other paradigms viewed work as essential to physical and mental health, the improvement of which could support patients’ reintegration into society and contribution to the colonial economy. Our findings support the latter view.
As noted in the Colonial Office (1864b), there was skepticism about outdoor employment in the BWI due to the tropical climate. However, outdoor employment was possible in the BWI, and our results indicate that a diversity of outdoor occupation activities across the colonies yielded positive patient outcomes. Concurrently, employment in trade reduced cured discharges among females, and agriculture decreased overall discharges for males. Interestingly, more females were employed in trade while more males were engaged in agriculture.Footnote 9 Arguably, these results may align with reports of labor exploitation whereby patients were kept in mental health institutions even after they had recovered because their work was useful (Smith Reference Smith2014). For example, in Jamaica, all clothing and bedding were made and repaired by patients, while in British Guiana and Barbados patients were involved in building repairs and maintenance (British Guiana 1896; Colonial Office 1864a, 1907). These tasks were not only useful to the running of the mental health institution but often also brought in financial gain that was reinvested or used for other expenses. For instance, in Jamaica any proceeds obtained from products of employment not consumed or used internally, such as fish, pigs, clothing, and bedding, were put into a patients’ fund (Allen Reference Allen1870, Reference Allen1876, Reference Allen1882). Claims of retaining patients after recovery at the Kingston Lunatic Asylum for financial gain were published in the Jamaica Gleaner (1886). Nevertheless, it should be noted that many patients were considered physically or mentally unable to participate in the available tasks and were not forced to do so, as was the case for Jamaica (Allen Reference Allen1870, Reference Allen1880; Williams Reference Williams1917).
Religious services were important to keep patients occupied, where the silence and order required during services was expected to influence tranquility at the mental health institution. Moreover, they might also indicate the extent of general church involvement in the institution. The results of this study indicated that a greater number of religious services led to reduced deaths and increased cured discharges for both males and females. Entertainment, on the other hand, did not have the same positive influence as religious services. Rather, results only indicated a decrease in not improved discharges for females, although this effect was small. There might be a number of reasons why our data did not capture an effect on patient outcomes, if there was one. More specifically, the information consistently available restricted us to defining entertainment as the total number of types offered, rather than categorizing it into different types or identifying the frequency with which they were provided. For instance, the Bahamas mental health institution only provided a musical box and later musical instruments for patients to use (Bahamas 1883, 1939), while Guiana provided a variety of distractions, such as concerts, magic lanterns, musical instruments, games, and dancing and singing, amongst others, throughout (British Guiana 1870, 1936).
Non-restraint was another essential element of moral management; however, many mental health institutions still practiced restraint using mechanical devices and attendants. According to the results, the use of mechanical restraint had a positive impact, namely, a reduction in deaths among males and females and not improved discharges for females. Mechanical restraint was necessary in cases of violence and self-harm. For example, in British Guiana and Jamaica, it was used on the hands of female patients who had surgical treatments to hinder them from hampering the healing process (Allen Reference Allen1883; Colonial Office 1883b). Violent or suicidal patients in Antigua were restrained from chin to feet (Colonial Office 1864c), and in Grenada and St Lucia, where occupation and entertainment options were limited, restraint was used in response to violent and disruptive behaviors (Smith Reference Smith2014). Restraint by attendants increased overall discharges for males. In these cases, perhaps there was a calming effect on patients when attendants intervened, resulting in a discharge, or maybe there was a discharge of patients considered as troublemakers. Moreover, although restraint by attendants was not supported (Colonial Office 1864b), in cases where mechanical restraints were not applied, perhaps restraint by attendants was viewed as the only means of controlling violent and disruptive behavior, as was the case in Jamaica. Seclusion, on the other hand, reduced overall discharges for females and relieved discharges for males. Seclusion, used to remove violent and unruly patients to a separate space within the institution, was arguably necessary due to overcrowding, inadequacies of the buildings, and low staff numbers (Burtinshaw and Burt Reference Burtinshaw and Burt2017; Smith Reference Smith2014). For example, Allen (Reference Allen1869) states, “It is only resorted to when the patient cannot be at large with safety to himself or to others, and when he is not in a state to be influenced by persuasion, or conciliated by kindness, and it is only continued until the temporary passion has subsided, and the danger is passed.” However, the effect on patients was adverse, arguably due to isolation and decreased social interaction, which probably worsened mental anxiety. Even in modern psychiatric care, seclusion has negative impacts on patients’ mental health, and its avoidance is recommended (Baggio et al. Reference Baggio, Kaiser and Wullschleger2024).
Patient classification was a central element in moral management, as separating patients by the “degree to which they were quiet or noisy, violent or tractable, was thought to remove ‘causes of irritation’ which exacerbated the insanity” (Swartz Reference Swartz1995). Results indicated that an increase in the number of patients classified as maniacal and dangerous resulted in more deaths. This is unsurprising since consistent overcrowding at the mental health institutions arguably hindered the provision of separate accommodations for violent patients, which could result in fatalities (Smith Reference Smith2014). As noted in a Kingston Lunatic Asylum report, patients “belonging to a semi-savage or dangerous class; they require a much larger proportion of single rooms for their isolation” (1868–1870). Moreover, the role of overcrowding in the spread of diseases, including diarrhea, dysentery, and tubercular affections at mental health institutions, is well-documented. In Jamaica, for example, it is noted that “diseases are the outcome of defective hygienic conditions, overcrowdings and fouled surroundings” (Plaxton Reference Plaxton1893: 73). Additionally, results showed that an increase in the classification as idiotic, paralytic, and epileptic resulted in a rise in cured discharges for females.
Nutrition had a positive influence on the number of relieved discharges for male and female patients. This aligns with an observation Donald (Reference Donald1876) made at the mental health institution in British Guiana, specifically, that nutrition improved the mental conditions of patients as they sometimes were undernourished upon admission. Additionally, as noted in a Kingston Lunatic Asylum report for 1898, the weight of many patients at the time of discharge was higher than their weight on admission, which arguably supports the case of malnourishment upon admission (Plaxton Reference Plaxton1898). Diet had no impact on other patient outcomes, arguably because there were many factors influencing it. For example, at the Jamaican mental health institution, the medical superintendent attempted to adjust the dietary allowance for patients because they were eating too much and since a distinction of meals for males and females and working patients or non-working patients was lacking (Smith Reference Smith2014). This attempt was futile as it was met with violence from the patients.
Increased space at institutions reduced deaths of male patients. One should note that overcrowding was a consistent issue throughout the BWI, so the result is not surprising. One possibility is that when limited extra dormitory space was provided, it was preferably allocated to males. For example, in 1902 in Jamaica, when a new small ward was completed, “some relief to the over-crowded male wards was thus given by transferring 60 patients,” but no relief for females (Plaxton Reference Plaxton1902: 170). In contrast, an increase in space decreased relieved discharges for males. Similarly, additional lavatories reduced relieved discharges for females. Lavatories additionally contained a wash basin and were an upgrade from latrines common in the early years across the BWI. Most latrines were based on the dry earth system, or some simply provided a latrine extending over the sea, as was the case for Belize until 1902 (Bahamas 1870, 1902). As many scholars argued, mental health institutions functioned as facilities of custodial care, which could perhaps explain these results. Baths, however, had no effect, although according to Scott et al. (Reference Scott, Keech and Osborn1860), “experience has shewn that in a physical and mental point of view, bathing is an important agent in effecting an amelioration of their condition.” Notably, many of the mentally ill were “paupers.” For instance, in Jamaica in 1869, all admissions but one had been “paupers” (Allen Reference Allen1869). These findings also align with claims that relatives played a role in the discharge of patients from mental health institutions (Bartlett and Wright Reference Wright and Bartlett1999; Melling and Forsythe Reference Melling and Forsythe2006; Wright Reference Wright1997, Reference Wright2022).
Increased presence of male attendants reduced cured discharges for males and increased relieved discharges for males and females. These findings contrast with the impact of female attendants. The reduction of cured discharges could perhaps be linked to labor exploitation. Additionally, superintendents generally had challenges with hiring qualified attendants (Smith Reference Smith2014), and a distinction in female and male attendants was made in Trinidad, whereby the latter were reported as “careless and indifferent” after they settled into the job (Smith Reference Smith2014). This could arguably explain the varying impacts of female and male attendants on patient outcomes. One should note, however, that we do not have information on the extent to which male attendants may have been treating mostly male patients and female attendants female patients. The fact that we find impacts of attendants of the opposite gender indicates that treatment was not exclusive to each gender.
Following the Jamaican scandal, regular inspections at the mental health institutions were recommended (Colonial Office 1864b). The results indicated that unannounced inspections reduced deaths among males, which is unsurprising. It is possible that, where visits were unannounced, management issues were quickly identified and dealt with. In Jamaica, regular surprise visits by the Governor or Colonial Secretary and members of the Board of Visitors were entered in the Visitor’s Book and communicated to the Colonial Secretary. In contrast to surprise visits, as Jemmott (Reference Jemmott2013) noted, when staff were aware of visits, they intentionally hid evidence of atrocities from plain sight.
One potentially important aspect that we did not address in our statistical analysis is the role that race may have played. In this regard, it is possible there was differential treatment among white, brown, and black-skinned patients (Hickling Reference Hickling2021) since black patients were described as having undeveloped minds and residing in barbaric conditions (Allen Reference Allen1872). Unfortunately, the statistical tables in the Blue Books do not report any information regarding race. However, Allen (Reference Allen1883) did report the racial decomposition of admission to the Jamaican mental health institution in 1883. Using these, one can see that the percentage of white, colored, black, and East Indian admissions, respectively, was 4.1, 13.4, 70.3, and 12.2 for males, and 1.5, 14.9, 78.9, and 4.7 for females. Thus, men constituted a higher prevalence of whites and East Indians but lower blacks and colored patients compared to females. Interestingly, Allen (Reference Allen1879) reports that women are more likely to display “savage” conditions associated with blacks. Since the remark is not a reflection of empirical realities but nineteenth-century racial ideologies, it is unsurprising that the prevalence of blacks is higher among women. Arguably, analysis of race and the intersection of race and sex could provide more insights regarding the incidence and treatment of mental illness in the BWI. In particular, it feasibly might provide additional factors explaining differences across colonies both in terms of the composition of the patient population as well as their management. As with race, there is little information available regarding the marital status of patients, unlike, for instance, in South West England (Melling and Forsythe Reference Melling and Forsythe2006). The role of marital status on patient outcomes in the BWI is, however, questionable since, as Allen (Reference Allen1879) argued, marriage had little value as reflected in the high number of illegitimate children.
There may be some concern regarding the reliability of the statistical and other information reported on mental health institutions in the Colonial Blue Books. Feasibly, the superintendents may have strategically misrepresented information in order to exaggerate favorable outcomes and/or their implementation of moral management techniques. While there are no specific studies of the mental health institution sections of the Blue Books, a few researchers have examined the accuracy of other data reported in these. In particular, Westland (Reference Westland2022) compares market prices from the African Blue Books to data constructed from four colonial newspapers to show their likely inaccuracy. In contrast, Gwaindepi and Fourie (Reference Gwaindepi and Fourie2020) show that data on government debt and expenditure reported in the Blue Book for the Cape Colony are fairly reliable. Our inability to do something similar for the mental health institution data remains a weakness of our analysis and conclusions.Footnote 10
Finally, it is important to emphasize the limitations of the generalizability of our findings to moral management as a tool for mental illness treatment. Firstly, the definition of mental illness, the level necessitating institutionalization, and when patients would have been discharged would have depended on the state of medical knowledge and its practice at the time. Secondly, while the lack of surviving historical sources for the colonial BWI does not allow us to further investigate this, practice in British institutions at the time may be suggestive. For example, in nineteenth-century Britain, individuals with Down’s syndrome would have fallen under the classification of “idiotic” and could be institutionalized (Burtinshaw and Burt Reference Burtinshaw and Burt2017). Thirdly, the classification and treatment of mental illness may have also differed in their implementation in the colonial BWI. For instance, Smith (Reference Smith2014) makes a strong argument that racist views may have played an important role in this regard. Secondly, the intake and discharge of patients feasibly may have also depended on non-medical factors, such as administrative pressure, overcrowding, labor needs, family intervention, or colonial governance priorities rather than clinical improvement. One should note in this regard, however, that the only consistent and extensive reports by the mental health institutions available, i.e., those for Jamaica, do not indicate that this was the case. Rather, each year’s budget proposal was submitted based on the expected number of patients, and at times the financing allocated was adjusted when additional funds were necessary or not needed (Jamaica Government Gazette 1877).
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ssh.2026.10141.
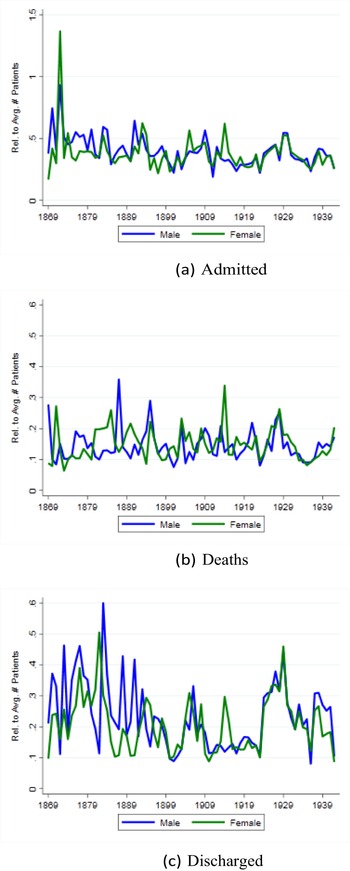
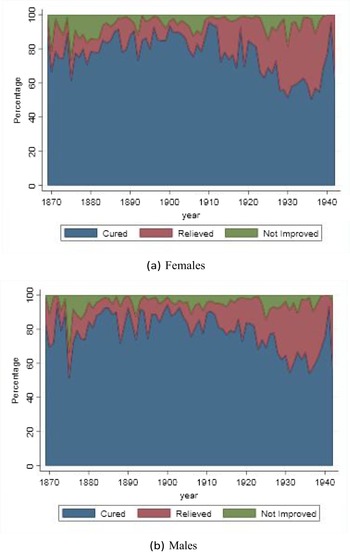

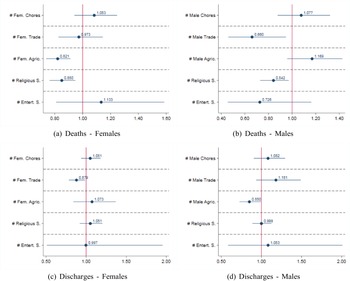
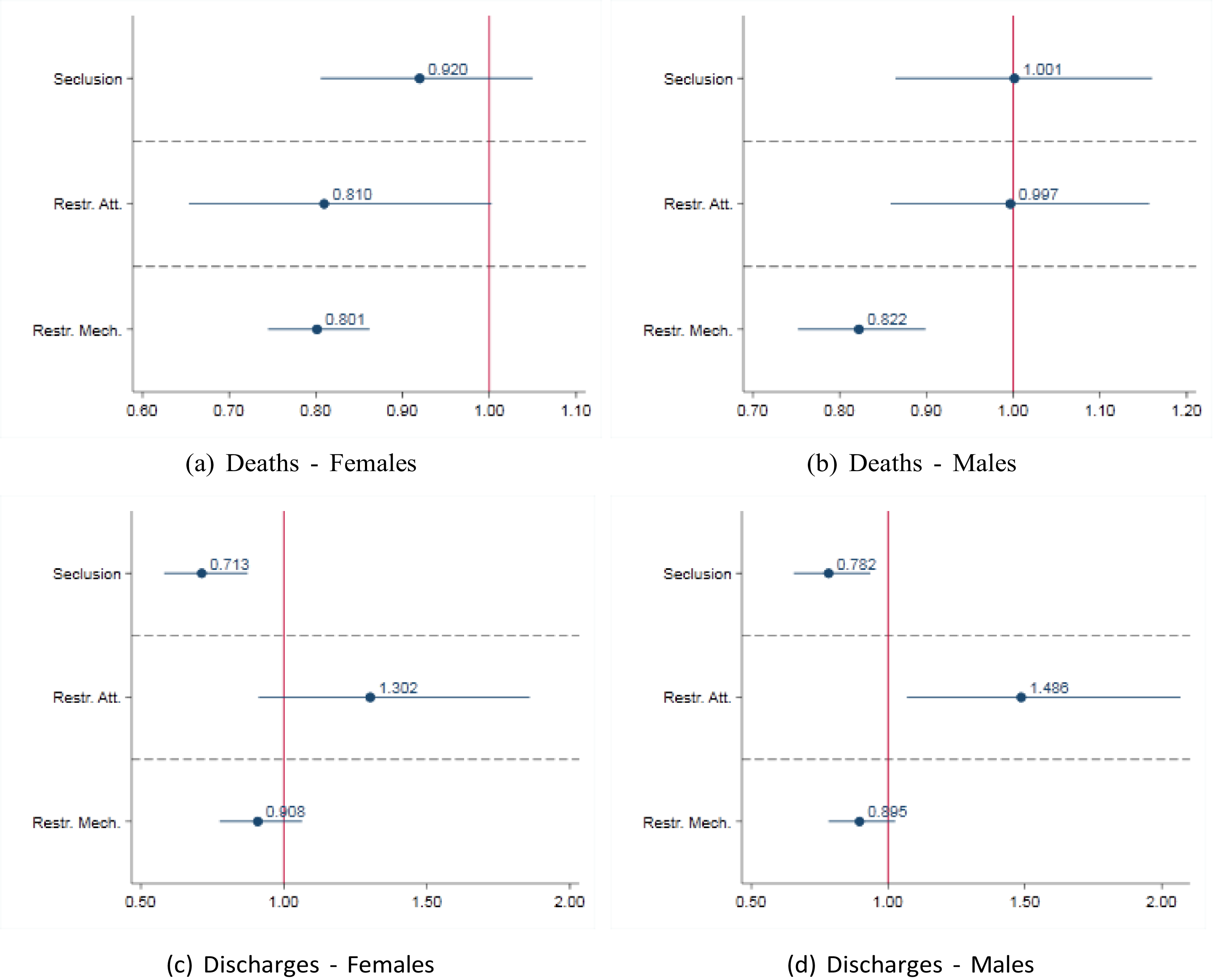
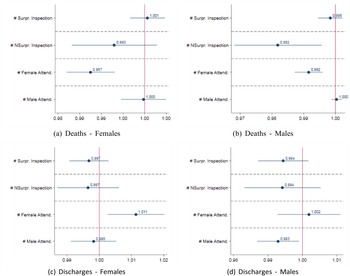
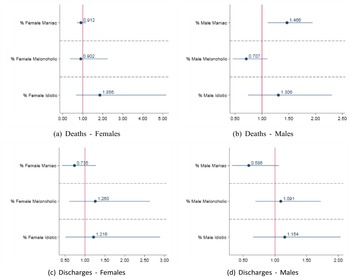
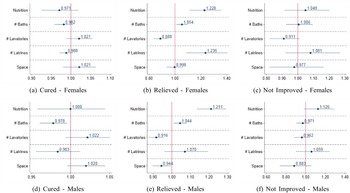
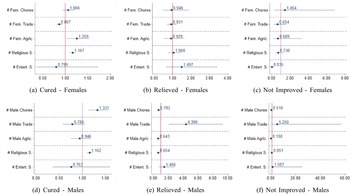






 Open access
Open access