

Evidence accumulated over the past decade has raised questions about the commonly held notion that bipolar disorder has a benign course. A longitudinal study of 71 adolescents admitted with their first ever mixed or manic episode found that, over 12 months, only 41% of them had achieved full functional recovery, even though 86% were free from affective symptoms.Reference DelBello, Hanseman, Adler, Fleck and Strakowski1 There are growing concerns that bipolar disorder may be associated with cognitive deficits even during euthymic periods. For example, Mora and colleagues examined 28 adults with bipolar disorder and 26 healthy controls (mean age 41 years).Reference Mora, Portella, Forcada, Vieta and Mur2 After a follow-up period of 6 years, participants with euthymic bipolar disorder had experienced a significant decline in tests of executive functioning, processing speed and verbal memory compared with healthy controls.Reference Mora, Portella, Forcada, Vieta and Mur2 Recent meta-analyses of neuropsychological studies of young and elderly euthymic people with bipolar disorder reported results consistent with those findings.Reference Bourne, Aydemir, Balanza-Martinez, Bora, Brissos and Cavanagh3,Reference Samame, Martino and Strejilevich4 In addition, there is evidence that the level of functional impairment in adults with bipolar disorder is correlated with the severity of cognitive deficits,Reference Martinez-Aran, Vieta, Torrent, Sanchez-Moreno, Goikolea and Salamero5 which seem particularly pronounced among those with illness onset in mid or late life.Reference Schouws, Comijs, Stek, Dekker, Oostervink and Naarding6 It remains unclear, at this stage, whether these deficits are progressive in nature and ultimately lead to an increase in the risk of dementia as people with bipolar disorder age. Kessing & Andersen used the Danish Health Register to investigate the risk of dementia among 4248 adults (mean age 57 years) admitted to hospital with a primary diagnosis of bipolar disorder between 1970 and 1986.Reference Kessing and Andersen7 Follow-up for dementia ended on 31 December 1999. They found that the risk of dementia increased, on average, 6% for every additional affective episode that required admission to hospital.Reference Kessing and Andersen7 They also reported, in a separate study, that the probability of dementia over time was more strongly associated with the diagnosis of bipolar disorder than with unipolar depression, schizophrenia or neurosis.Reference Kessing, Olsen, Mortensen and Andersen8 A nested case–control study using data from the Taiwanese National Health Insurance Research Database found that bipolar disorder was associated with a four-fold increase in the odds of dementia, including dementia with onset before the age of 65 years.Reference Wu, Chang, Liang, Wu, Chia-Hsuan Wu and Chen9 It remains unclear, however, whether the relationship between bipolar disorder and dementia is truly causal. Furthermore, existing data suggest that adults with bipolar disorder die prematurely,Reference Kessing, Vradi and Andersen10,Reference Kessing, Vradi, McIntyre and Andersen11 and the same seems to occur in people with bipolar disorder who reach older age.Reference Almeida, Hankey, Yeap, Golledge, Norman and Flicker12 Mortality data on middle-aged and young older adults have been reported elsewhere,Reference Crump, Sundquist, Winkleby and Sundquist13 but information about the causes of death for people with bipolar disorder who reach older age has not been established, so it is unclear whether some of these deaths could be prevented.
The present cohort study aimed to investigate the risk of dementia and death among community-dwelling older adults. We also sought to determine the causes of death in the population and among older people with bipolar disorder.
Method
Study design and setting
The Health in Men Study (HIMS) is a cohort study of a community-representative sample of older Western Australian men that started in 1996. Follow-up data were censored on 30 June 2009, which is the last date for which data on cause-specific mortality are available.
Participants
Men aged 65–85 years were identified using an electronic copy of the Western Australian electoral roll (enrolment to vote is compulsory for all Australian adults). We received a list with the contact details of 49 801 men, the entire population of men in this age group living in the Perth metropolitan region in 1995. Of those, 1839 had died by the time the study started and another 9482 were not selected for participation because they were living outside the immediate Perth metropolitan region. Of the remaining 38 480 men, 407 were excluded because they had a recorded diagnosis of dementia (see below), and another 305 were younger than 65 years. This left a total study sample of 37 768 older men who were alive and free of dementia by 2 April 1996.
This study was approved by the ethics committees of the University of Western Australia and of the Department of Health of Western Australia, as well as by the Legal Data Custodian.
Outcomes: dementia and death
The primary outcome of interest was the diagnosis of dementia recorded in the Western Australian Data Linkage System (WADLS). WADLS links information for all contacts with out-patient and in-patient mental health services in Western Australia, hospital morbidity data, as well as cancer and death registries.Reference Holman, Bass, Rosman, Smith, Semmens and Glasson14 From 1 January 1966 to 31 December 1978 diagnostic codes followed the ICD-8;15 from 1 January 1979 to 30 June 1999, ICD-916 codes were used, and from the 1 July 1999 all codes followed the ICD-1017 system. The following codes identified participants with dementia: 290, 294.1, 294.2, 331.0, 331.1, 331.2, 331.82, F00, F01, F02, F03, G30, G31.0, G31.1, and G31.83. In addition, we systematically scanned the text of death records for the words ‘dementia’, ‘Alzheimer’, ‘Pick’ and ‘Lewy’ to identify men who had a recorded diagnosis of dementia at the time of their death. The diagnoses of dementia were recorded between 2 April 1996 and 30 June 2009.
We also examined the death records of WADLS (secondary outcome of interest). The causes of death were grouped into 12 categories: suicide (ICD codes: E950–E959, X60–X84, Y870 and U03), accident (ICD codes: E80–E929, V00–V999, W00–W199, Y85–Y859), infection (ICD codes: 00–139, 771.3, A00–A99, B00–B99), cancer (ICD codes: 140–208, C00–C97), diseases of the heart (ICD codes: 390–398, 402, 404, 410–429, I00–I09, I11, I13, I20–I51), diseases of the brain (ICD codes: 30–32, 35–37, 290–294, 320–337, 340–349, 430–434, 436–438, I60–I69, G00–G14, G20-G26, F00-F09), vascular diseases that exclude heart conditions and strokes (ICD codes: 401, 403, 440–448, I10, I12, I70–I78), pneumonia or influenza (ICD codes: 480–487, J09–J18), respiratory diseases (ICD codes: 460–466, 470–478, 490–496, 507–519, J00–J47, J60–J99), diseases of the digestive system (including liver) (ICD codes: 520–537, 540–543, 550–553, 555–589, K00–K99), diseases of the kidneys (ICD codes: 580–589, N0–N7, N17–N19, N25–N27), and other causes of death (remaining ICD codes). Mortality data were available for the period between 2 April 1996 and 30 June 2009.
Exposure at study entry: bipolar disorder
We retrieved information about past diagnosis of bipolar disorder from the WADLS, which had to have been recorded prior to 2 April 1996 according to the following ICD codes: 296.1 and 296.3 (ICD-8), and 296.0, 296.1, 296.4, 296.5, 296.6, 296.7, 296.80 and 296.81 (ICD-9). We considered that the date of the first ever episode of bipolar disorder was the same as the date of the first ever contact with the health services with one of these diagnoses (out-patient or in-patient). If a depressive episode had been recorded prior to the episode of mania or mixed state, then the date of the depressive episode was considered the date of onset of the bipolar disorder. The ICD codes used to identify depressive episodes were: 296.0 and 300.4 (ICD-8), and 296.2, 296.3, 311 and 300.4 (ICD-9). The earliest mental health morbidity records available were dated 1 January 1966.
Other study measures
Other variables included date of birth, alcohol use disorder (ICD codes: 291, 303 and 305.0) or substance use disorder (ICD codes: 292, 304 and 305 – excluding 305.0). Past studies have shown that WADLS yields accurate diagnoses for severe mental disorders.Reference Jablensky, Morgan, Zubrick, Bower and Yellachich18 We calculated the age of participants as the difference, in years, between the date at study entry and the date of birth. The duration (in years) of the bipolar episode was calculated as the difference between the date at the beginning of the follow-up period and the date of the first ever recorded affective episode of bipolar disorder.
Statistical methods
We used the statistical package Stata/IC 14.0 to manage and analyse the data (StataCorp LP, 2015). Descriptive statistics summarised categorical data as count and proportions (%), and continuous variables as mean, range and standard deviation of the mean (s.d.). We used the proportion command of Stata to estimate the prevalence of severe mental disorders (95% confidence intervals (95% CIs) were calculated using a logit transformation that allows for the estimation of the standard error of the proportion). We employed logistic regression to estimate the odds ratio (OR) of the association between bipolar disorder and age strata and prevalent alcohol and substance use disorder, and Cox regression to estimate the hazard ratio (HR, and 95% CI) of dementia and death associated with bipolar disorder. The Cox regression models were adjusted for age, with the date of birth of participants set as the origin, the beginning of follow-up as the date of invitation, and the date of first ever diagnosis of dementia or death as the time of the event. Data were censored on 30 June 2009. Survival data were plotted using the Kaplan–Meier survivor function, and the cumulative hazard using the Nelson–Aalen approach. We supplemented these analyses with a competing risk Cox regression model using death as an outcome competing with dementia. The risk estimates, in this case, are expressed as sub-hazard ratios (SHRs) and respective 95% CI. We used the stptime command of Stata to calculate the age-standardised annual rate of dementia and of death for people with and without bipolar disorder. We repeated this analytical approach after stratifying participants with bipolar disorder according to their age at the time of onset of illness (40s or earlier, 50s, 60s, 70s or 80s) and according to the duration of the disorder (<5 years, 5–14 years, >15 years). Finally, we investigated the association between the diagnosis of bipolar disorder (and age at onset/duration of the disorder) and cause-specific mortality using age-adjusted competing risk Cox regression. Alpha was set at 0.05 and all tests reported are two-tailed.
Results
The sample consisted of 37 768 men aged 65–85 years (mean 72.5, s.d. = 4.6), of whom 256 (0.7%, 95% CI 0.6–0.8) had a recorded diagnosis of bipolar disorder at study entry. The age distribution of men with and without bipolar disorder was similar (t = 1.27, d.f. = 37 766, P = 0.203). Table 1 summarises their characteristics.
Characteristics of study participants and of a subsample of men with prevalent bipolar disorder at the time of study entry

| Population (n = 37 768), n (%) | Bipolar disorder (n = 256), n (%) | Odds ratio (95% CI) for bipolar disorder | |||
|---|---|---|---|---|---|
| Age group, years | |||||
| 65–69 | 13349 (35.3) | 94 (38.0) | 1 (1) | ||
| 70–74 | 13021 (34.5) | 97 (37.6) | 1.06 (0.80–1.41) | ||
| 75–79 | 8553 (22.6) | 53 (20.5) | 0.88 (0.63–1.23) | ||
| ⩾80 | 2845 (7.5) | 12 (3.8) | 0.60 (0.33–1.09) | ||
| Alcohol use disorder | 1480 (3.9) | 43 (16.8) | 5.07 (3.64–7.06) | ||
| Other substance use disorder | 5995 (15.9) | 62 (24.2) | 1.70 (1.28–2.27) | ||
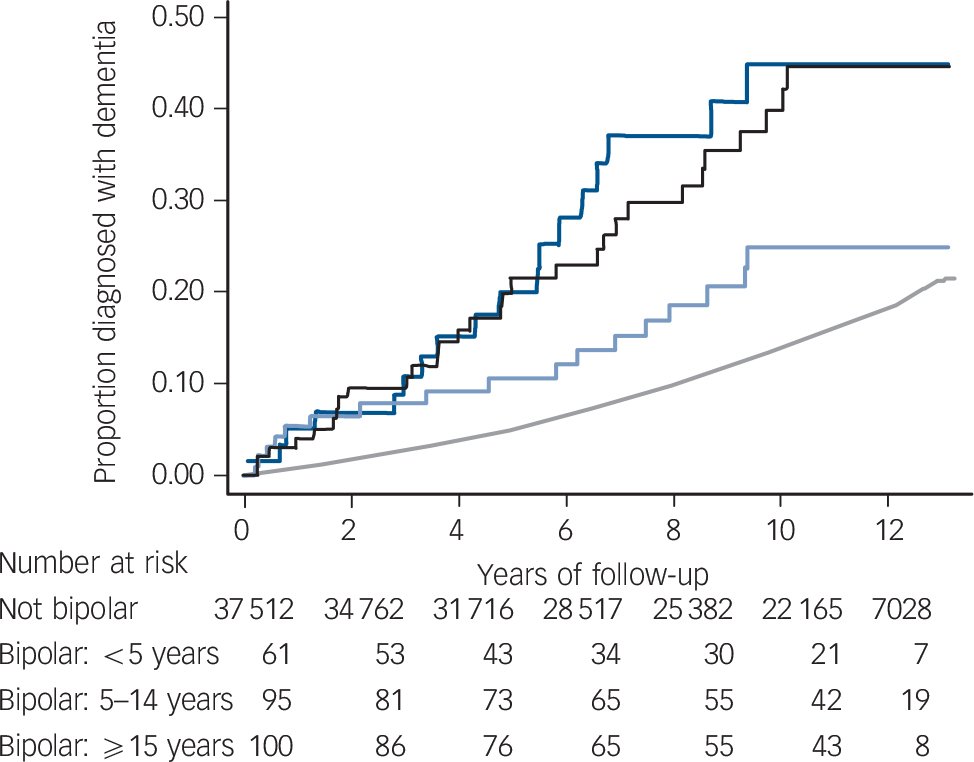
Overall, 13% of participants (n = 4925) developed dementia, which was present in 65 (25.4%, 95% CI 20.4–31.1) of the 256 men with bipolar disorder. Bipolar disorder was associated with higher age-adjusted hazard of dementia (HR = 2.58, 95% CI 2.02–3.30) (Fig. 1), and this association remained largely unchanged after additional adjustment for history of alcohol and substance use disorder (HR = 2.30, 95% CI 1.80–2.94). Competing risk Cox regression yielded an age-adjusted SHR of dementia associated of 2.17 (95% CI 1.67–2.82). The age-adjusted rates of dementia per 1000 person-years for men with and without bipolar disorder were 32.9 (95% CI 25.8–41.9) and 14.3 (95% CI 13.9–14.8) respectively. We stratified these annual rates by age at the time of diagnosis of dementia: 65–70, 70–75, 75–80, 80–85, 85–90 and 90–95 years, which for men without bipolar disorder were 3.0% (95% CI 2.4–3.6), 5.1% (95% CI 4.7–5.6), 11.5% (95% CI 10.9–12.1), 23.8% (95% CI 22.7–24.9), 44.1% (95% CI 41.5–46.8) and 59.9% (95% CI 51.7, 69.5), whereas for men with bipolar disorder rates were 15.3% (95% CI 4.9–47.3), 25.1% (95% CI 15.1–41.7), 33.4% (95% CI 22.2–50.3), 51.1% (95% CI 33.0–79.3) and 41.6% (95% CI 15.6–110.7). There were no participants with bipolar disorder in the age group 90–95 years.
Cumulative hazard of dementia during a follow-up period of 13 years for older men with (light blue line) and without (dark blue line) bipolar disorder.
The age-adjusted hazard ratio of dementia associated with the diagnosis of bipolar disorder was 2.58 (95% CI 2.02–3.30). The age-adjusted sub-hazard ratio of dementia was 2.17 (95% CI 1.67–2.82), with death used as a competing risk. The age-adjusted rates of dementia per 1000 person-years for men with and without bipolar disorder were 32.9 (95% CI 25.8–41.9) and 14.3 (95% CI 13.9–14.8) respectively.

The mean age of the first recorded diagnosis of bipolar disorder in this population was 59.7 years (s.d. = 8.9, range: 37.8–81.7) (see online Fig. DS1 for HR and SHR of dementia by age of bipolar disorder diagnosis). We also investigated the association between time lived with bipolar disorder (in years) and subsequent risk of dementia. These results are summarised in Fig. 2 and show that the HR of dementia was similarly high among men with recent (<5 years) and long-standing history of bipolar disorder (⩾15 years) compared with participants without bipolar disorder.
Age-adjusted cumulative hazard of dementia according to the time lived with the diagnosis of bipolar disorder.
Not bipolar (grey line – reference), <5 years (dark blue line; hazard ratio (HR) 3.23, 95% CI 2.03–5.14), 5–14 years (pale blue line; HR = 1.71, 95% CI 1.06–2.76), ⩾15 years (black; HR = 3.09, 95% CI 2.16–4.43). The respective age-adjusted sub-hazard ratios of dementia were 2.69 (95% CI 1.62–4.48), 1.41 (95% CI 0.86–2.31) and 2.68 (95% CI 1.81–3.95), with death used as a competing risk.

The age-adjusted mortality HR of men with bipolar disorder was 1.51 (95% CI 1.28–1.77), and the mortality rates per 1000 person-years were 69.7 (95% CI 59.5–91.7) and 49.4 (95% CI 48.7–50.2) for men with and without bipolar disorder respectively (online Fig. DS2). Further adjustment of the analyses for past-recorded history of alcohol or substance use disorder had minimal effect on the results (HR = 1.32, 95% CI 1.13–1.55). Table 2 shows the principal causes of death in the population and among participants with bipolar disorder. Competing risk regression showed that bipolar disorder was associated with increased SHR of suicide (SHR = 13.43, 95% CI 5.35–33.73), accidents (SHR = 2.78, 95% CI 1.14–6.75), pneumonia or influenza (SHR = 3.66, 95% CI 1.81–7.40), and diseases of the liver and digestive system (SHR = 2.02, 95% CI 1.00–4.06). The age-adjusted suicide rates per 100 000 person-years among men with and without bipolar disorder were 229.3 (95% CI 95.4–550.8) and 15.3 (95% CI 11.7–20.0) respectively. Similarly, death by accident occurred at a rate of 229.3 (95% CI 95.4–550.8) and 73.4 (95% CI 64.9–83.0) per 100 000 person-years for men with and without bipolar disorder respectively. Mortality data stratified according to the age at onset of bipolar disorder and duration of illness are reported in online Tables DS1 and DS2.
Principal causes of death in community-representative sample of older men and among those with bipolar disorder over a follow-up period of 13 years

| Total sample (n = 37768) n (%) | Bipolar disorder (n = 256) n (%) | Mortality sub-hazard ratio for bipolar disordera | 95% CI | |
|---|---|---|---|---|
| Alive | 20433 (54.1) | 104 (40.6) | 1 | Reference |
| Causes of death | ||||
| Suicide | 58 (0.1) | 5 (1.9) | 13.43 | 5.35–33.73 |
| Accident | 260 (0.7) | 5 (1.9) | 2.78 | 1.14–6.75 |
| Infection | 314 (0.8) | 3 (1.2) | 1.35 | 0.43–4.20 |
| Cancer | 4484 (11.9) | 41 (16.0) | 1.33 | 0.97–1.81 |
| Diseases of the heart | 4273 (11.3) | 26 (10.2) | 0.85 | 0.58–1.26 |
| Diseases of the brain | 3950 (10.5) | 31 (12.1) | 1.12 | 0.79–1.59 |
| Vascular diseases | 532 (1.4) | 6 (2.3) | 1.61 | 0.72–3.62 |
| Pneumonia or influenza | 319 (0.8) | 8 (3.1) | 3.66 | 1.81–7.40 |
| Respiratory diseases | 1636 (4.3) | 10 (3.9) | 0.86 | 0.46–1.60 |
| Liver and digestive diseases | 568 (1.5) | 8 (3.1) | 2.02 | 1.00–4.06 |
| Kidney diseases | 421 (1.1) | 4 (1.6) | 1.35 | 0.50–3.63 |
| Other causes | Men's S520 (1.4) | 5 (1.9) | 1.36 | 0.56–3.29 |
a. Mortality sub-hazard ratio derived from an age-adjusted competing risk regression model.
Results in bold are statistically significant.
Post hoc analyses
We completed a series of additional analyses to clarify whether the excess risk of dementia and death associated with bipolar disorder could be attributed to the inclusion of false negative cases of dementia in the sample. We re-ran our Cox regression models after excluding participants who met criteria for the diagnosis of dementia within the first 2, 3 and 4 years of follow-up. The respective age-adjusted HRs of dementia associated with the diagnosis of bipolar disorder were 2.15 (95% CI 1.61–2.87), 2.22 (95% CI 1.64–2.99) and 2.03 (95% CI 1.45–2.83). In the same way, we examined the mortality HR associated with the diagnosis of bipolar disorder after excluding participants who died within the first 2, 3 and 4 years of follow-up. The respective mortality HRs were 1.52 (95% CI 1.28–1.81), 1.56 (1.30–1.86) and 1.56 (1.29–1.89). Finally, we examined the mortality HR associated with the diagnosis of bipolar disorder after excluding from the analyses participants who received a diagnosis of dementia within the first 2, 3 and 4 years of follow-up – the respective mortality HRs were 1.45 (95% CI 1.21–1.74), 1.49 (95% CI 1.23–1.81) and 1.48 (95% CI 1.21–1.83).
As several unmeasured factors could have confounded the association between bipolar disorder and dementia/mortality, we conducted supplementary analyses with a subsample of men for whom lifestyle and clinical data were collected between 1996 and 1998 by means of a self-report questionnaire. Details about this cohort have been reported elsewhere.Reference Norman, Flicker, Almeida, Hankey, Hyde and Jamrozik19 The sample consisted of 12 147 participants free of dementia, of whom 65 had bipolar disorder (0.5%). Other relevant measured factors included place of birth (Australia v. elsewhere), marital status (married v. not married), education (complete v. incomplete high school), physical activity (<150 v. ⩾150 min/week of vigorous physical activity), smoking (never, past or current), alcohol consumption (never, past, <14 g/week, 14–27 g/week, ⩾28 g/week), body mass index (<18.5 kg/m2, 18.5–25.9 kg/m2, 25–29.9 kg/m2, ⩾30 kg/m2), history or treatment for diabetes or hypertension, and past heart attack or stroke. We included these variables, as well as age, in a Cox regression model to investigate the effect of history of bipolar disorder on the risk of dementia – the relevant adjusted HR was 2.52 (95% CI 1.54–4.15). Similarly, the adjusted mortality hazard associated with the diagnosis of bipolar disorder was 1.40 (95% CI 1.01–1.95).
Discussion
We believe this is the first longitudinal study of older adults with bipolar disorder derived from a community-representative sample. The results showed that dementia and death accrue with greater frequency among older men with than without bipolar disorder. The diagnosis of bipolar disorder was associated with more than double the risk of dementia over 13 years and with a 50% increase in mortality. This excess risk could not be attributed to confounding due to age or use of substances. We also observed that the risk of dementia was highest for men with recent (<5 years) and long-standing history of bipolar disorder (⩾15 years), and that death by suicide, accidents, pneumonia or influenza, and diseases of the digestive system were more frequent among older men with than without bipolar disorder. Finally, we found that the causes of death varied according to the age at onset and duration of bipolar disorder, with diseases of the brain being more frequent among men with <5 years history of bipolar disorder or with illness onset in their 70s or later.
Strengths and limitations
This study has the merit of having used exposure and outcome data for the entire male population of older Australian citizens living in Perth. We acknowledge, however, that older adults living in residential care facilities and those who were not citizens were not approached (about 20% of this population).Reference McLennan20 We are not aware of any evidence indicating that the clinical outcomes of older non-Australian citizens are different from their Australian peers. Another important feature of a longitudinal study such as this is that follow-up data were available through WADLS for all participants, as the internal and external migratory movement of older Western Australians is negligible.21
We concede that the diagnosis of bipolar disorder relied on administrative data, which only became available in 1966. Consequently, participants who were in contact with the health services before 1966, but not later, would not have been identified as cases, although the chronic and recurring nature of bipolar disorder would most likely have ensured identification at a later stage. Nonetheless, if false negative cases were present in the ‘non-bipolar’ sample, this would have decreased the power of the study. The other consequence of the 1966 starting date for WADLS is that it could have biased our estimates of age at onset and duration of illness. We attempted to address this issue by stratifying time-related data into groups (e.g. <5 years, 5–14 years and ⩾15 years of illness), bearing in mind that 30 years of data had already been accumulated by the time we initiated follow-up. We are also reassured by the fact that the lifetime prevalence of bipolar disorder in our sample (0.7%) is consistent with that of other epidemiological surveys that used structured interviews and face-to-face assessments.Reference Kessler, Berglund, Demler, Jin, Merikangas and Walters22
Like bipolar disorder, the diagnosis of dementia relied on data recorded in WADLS. We suspect that many older adults with mild dementia remain undiagnosed or are managed in primary care, which could have led to underestimation of the true rate of dementia in the sample, although our incidence rate figures were within the range of those reported by others.Reference Vardarajan, Faber, Bird, Bennett, Rosenberg and Boeve23 Nevertheless, if we accept that some false negative cases of dementia were present, the calculation of risk associated with bipolar disorder would only be affected if the distribution of these cases in the population were not random. It is conceivable that medical specialists attuned to the assessment of cognitive function and dementia (such as geriatric psychiatrists) review older men with bipolar disorder more often and, thus, establish a diagnosis of dementia for these patients earlier than otherwise would have been the case. Such bias could have potentially inflated the risk ratio of dementia among older men with bipolar disorder compared with the rest of the population. We are unable to dismiss such a possibility outright, but our post hoc analyses showed that the observed risk estimates did not change substantially when we excluded from the analyses participants who had developed dementia during the first 4 years of follow-up (i.e. possible undiagnosed prevalent cases of dementia at study entry). Prior studies that had access to control groups with other mental disordersReference Kessing, Olsen, Mortensen and Andersen8 or medical illnessesReference Kessing and Nilsson24 have also reported a relative excess of cases of dementia among people with past diagnosis of bipolar disorder, thereby suggesting that detection bias may be insufficient to explain the association between bipolar disorder and dementia.
We also concede that several unmeasured factors could have confounded the association between bipolar disorder, dementia and death, such as physical activity, smoking, education, marital status and comorbidities. These data were available for a subsample of 12 147 of our participants – the adjusted post hoc models yielded results that were similar to those observed for the entire sample, which suggests that the link between bipolar disorder and dementia and death cannot be easily attributed to lifestyle and clinical factors, although residual confounding remains a possibility.
The relatively small number of participants with bipolar disorder introduced some imprecision in the calculation of the risk (and rates) associated with different causes of death, as some of the events were uncommon (such as suicides). For this reason, these results would be better viewed as tentative. Finally, we acknowledge that the study was limited to men and it is unclear whether our findings would be equally applicable to women.
Interpretation
Our data showed that older men with past diagnosis of bipolar disorder are at increased risk of dementia and that this risk is greatest for those with long-standing and with recent history of bipolar disorder. The association between a recent diagnosis of bipolar disorder (i.e. <5 years) and dementia is consistent with the possibility that changes in the regulation of mood later in life may represent, in at least some cases, an early clinical expression of neurodegenerative processes that will ultimately lead to the diagnosis of dementia. The doubling in the hazard of death due to diseases of the brain among those in their 70s or 80s as well as among those with bipolar disorder of <5 years duration lends support to this interpretation.
An early case series of 92 older adults admitted to hospital with an episode of mania found that 22 of them (24%) showed evidence of brain disease consistent with dementia, Parkinson's or cerebrovascular diseases.Reference Stone25 Others later reported that 8 of 25 older people (32%) treated for mania developed cognitive impairment over a follow-up period of 5–7 years,Reference Dhingra and Rabins26 whereas recent case reports have highlighted the potential overlap between some cases of bipolar disorder and frontotemporal dementia.Reference Cerami, Marcone, Galimberti, Villa, Scarpini and Cappa27,Reference Floris, Borghero, Cannas, Stefano, Murru and Corongiu28
There is evidence that people with bipolar disorder lose more grey matter volume in the medial temporal cortex over 4 years than controls, and that this loss is correlated with the number of affective episodes.Reference Moorhead, McKirdy, Sussmann, Hall, Lawrie and Johnstone29 In this case, long-standing and recurring bipolar disorder would be expected to be associated with increased risk of cognitive decline, as suggested by othersReference Kessing and Andersen7 and corroborated by our findings. The pathophysiological processes underpinning these changes remain unclear, but some have argued that inflammationReference Bauer, Pascoe, Wollenhaupt-Aguiar, Kapczinski and Soares30 and cardiovascular risk factors may be involved.Reference Schouws, Stek, Comijs and Beekman31 In addition, there have been suggestions that people with bipolar disorder may develop dementia or die earlier because of accelerated ageing, although a meta-analysis of studies of telomere length that included people with bipolar disorder found no difference between patients and controls.Reference Colpo, Leffa, Kohler, Kapczinski, Quevedo and Carvalho32
Existing observational data indicate a lower risk of dementia among people with bipolar disorder who are issued a prescription for treatment with lithium,Reference Kessing, Sondergard, Forman and Andersen33 with a subsequent study reporting that prolonged treatment may be required to consolidate this benefit.Reference Kessing, Forman and Andersen34 These studies found no evidence of benefit associated with the use of other mood stabilisers, and high-quality corroboration from randomised controlled trials remains sparse. A 13-week placebo-controlled trial of 71 patients with Alzheimer's disease found that treatment with lithium was not associated with cognitive gains,Reference Hampel, Ewers, Burger, Annas, Mortberg and Bogstedt35 although the 12-month treatment of 21 adults with amnestic mild cognitive impairment led to a decrease in the concentration of phosphorylated tau in the cerebrospinal fluid and a trend for improved cognitive performance compared with the 20 placebo-treated participants.Reference Forlenza, Diniz, Radanovic, Santos, Talib and Gattaz36 Hence, treatment with lithium could contribute to prevent dementia, but a sufficiently powered randomised placebo-controlled trial would be required to test this hypothesis.
Several past surveys have reported that bipolar disorder is associated with higher mortality due to general medical illnesses,Reference Kessing, Vradi and Andersen10,Reference Kessing, Vradi, McIntyre and Andersen11,Reference Roshanaei-Moghaddam and Katon37 but relevant data for older adults with bipolar disorder have not been reported. Self-harm behaviour, including suicide, is more frequent among older adults with affective disorders than in the general community.Reference Lawrence, Almeida, Hulse, Jablensky and Holman38 Our data confirmed the excess mortality due to suicide and accidents among older men with bipolar disorder, although the number of individuals affected was small. It is possible that certain lifestyle practices associated with bipolar disorder may also contribute to decrease survival (e.g. excessive use of substances), but other factors may play a part. Investigations have suggested that chronic inflammation drives some of the neurocognitive changes associated with bipolar disorder,Reference Berk, Kapczinski, Andreazza, Dean, Giorlando and Maes39 and may also increase the long-term risk of death due to infections, including influenza and pneumonia.Reference Ritchie, Würtz, Nath, Abraham, Havulinna and Fearnley40 Moreover, the use of mood stabilisers, antipsychotics, antidepressants and benzodiazepines could contribute to increase cognitive impairment and mortality among older adults with bipolar disorder.Reference Almeida, Alfonso, Hankey and Flicker41–Reference Vinkers, Gussekloo, van der Mast, Zitman and Westendorp43
In summary, this large community-based cohort study of older men showed that bipolar disorder is associated with increased risk of dementia and with premature death. The pathways linking bipolar disorder to these clinical outcomes are yet to be established, but currently available evidence suggests that some of them may be amenable to change, in which case prevention might not only be desirable but also feasible.





eLetters
No eLetters have been published for this article.