


Introduction
In the realm of clinical negligence litigation, it is commonly thought that judicial decision-making is an effective way to improve patient care. This view is widespread among legal academics, doctors, and patients. Legal scholars such as Brazier and McHale have emphasized the role of the courts in raising clinical standards;Reference Brazier 1 McHale in particular notes that the scrutiny of particular clinical decisions in a court of law “may give rise to statements of principles which can be carried forward into practice itself.” Doctors and medical organizations appear to share this view. Guidance emphasizes the need for doctors and medical students to be familiar with the legal decisions which are thought to affect or even guide clinical practice.Reference Sturgess, Duane and Ley 2 Further, the GMC and BMA’s intervention in court cases demonstrates their view that judicial decision-making can have such a significant impact on clinical practice that formal intervention is needed (in the BMA’s words) “if it fears a court case might bring detrimental change to the way doctors practise…”Reference Trueland 3 Conversely, patients often feel that bringing a legal claim can positively influence clinical practice. The reason for bringing a claim cited by many such patients is a desire to prevent repetition of the alleged negligence in the future, implying that they believe that the courts are an effective way to raise standards.Reference Vincent, Phillips and Young 4 Perhaps most famously, Nadine Montgomery said of her claim in Montgomery v Lanarkshire Health Board 5 that her aim in bringing the claim was to “make sure with every fibre of my being that this never happened to another woman again,” 6 a sentiment echoed by her lawyer.Reference Sutherland 7
This view may, however, be misconceived. Concerns have long been raised about the efficacy of the law in driving changes in medical practice.Reference Phillips 8 If this is the case, the role of clinical negligence litigation in shaping clinical practice and promoting patient rights needs to be reconsidered alongside other drivers of change.
This paper considers legal and medical practitioners’ views on the impact of Montgomery in driving the development of patients’ autonomy-based rights in medical practice. Montgomery established a duty for doctors “to take reasonable care to ensure that the patient is aware of any material risks involved in any recommended treatment, and of any reasonable alternative or variant treatments.” 9 This was widely considered to have introduced an autonomy-based duty to disclose the material risks of proposed treatment, with the potential to significantly change clinical practice.
Various conceptualizations of autonomy have been considered in the bioethics and legal literature; perhaps the most-commonly applied is that put forward by Beauchamp and Childress (according to which autonomy is the right to self-governance, to act in accordance with a self-chosen plan with intention, understanding and non-interference).Reference Beauchamp and Childress 10 Informed consent is often considered as practical way of facilitating respect for a patient’s autonomy-based rights:Reference Faden and Beauchamp 11 Patients must be adequately informed about the material risks of medical treatments to make autonomous decisions about receiving them.
Our previous work considered the academic debate over the meaning and significance of the Montgomery judgment but identified that empirical research was required to investigate the impact of the judgment in practice.Reference Le Gallez 12 We therefore carried out interviews with practicing lawyers and doctors to explore their views on the impact and perceptions of Montgomery. During the course of those interviews, it became apparent that their views had significance for the role of case law in driving changes in clinical practice more generally.
In this paper, we present the qualitative analysis of these interviews with lawyers and doctors, focusing on the limitations of case law in incorporating patients’ autonomy-based rights into medical practice. Part I considers three factors that limit the power of case law to drive autonomy-respecting practice. These are the practical and economic considerations which limit the development of new case law, the difficulties of bringing a claim caused by a focus on financial redress and the deficiencies in medical professionals’ understanding of case law. Part II argues that the role of case law in changing medical practice is important and that these findings merit concern. Part III considers ways in which the role of case law along with other levers in confirming autonomy respecting norms in medical practice might be developed further.
Methods
This paper presents an interdisciplinary critical examination of an issue that emerged from transcripts of interviews with practicing lawyers, namely the limitations of litigation in driving autonomy-respecting practice. The interviews were being undertaken primarily to investigate lawyers’ views on the impact and possible implications of Montgomery as part of a research project exploring how diagnosis was formed, communicated and recorded, and the detailed methodologies for the recruitment, data collection and analysis for this study, along with the main outputs are published elsewhere.Reference Mackley, Liddell and Skopek 13 A second part of the project involved doctors working in three acute units, who were observed and interviewed about their experience and views on forming and communicating diagnosis. While it was always intended that the project would involve interviewing doctors, the results of our interviews with lawyers suggested that we ought also to explore doctors’ perceptions as to the efficacy of case law in driving change in clinical practice. Questions were therefore added to the doctors’ semi-structured interview schedule to include questions about their knowledge and understanding of Montgomery and other drivers of change in clinical practice. Detailed methodologies for the recruitment, data collection, and analysis for these studies, along with the main outputs, are published elsewhere.Reference Cox 14 Copies of the full interview guides and details of the settings and data collection can also be found in the appendix.
Interviews were recorded, transcribed, and analyzed using content analysis.Reference Prasad, Rubin and Babbie 15 All transcripts were initially coded by TH and CC; themes were discussed and refined in discussion with the whole research team. The emerging themes presented in this paper were not the initial focus of the interviews; these themes were noted by researchers, and then further discussed and analyzed by the interdisciplinary team, integrating the interview data with critical legal and ethical scholarship. This study (IRAS ID: 265331) was approved by the East of England — Essex Research Ethics Committee. Patient and public involvement: a PPI group was not involved in this study.
A table of quotations from lawyers and doctors relating to the emerging themes identified can be found in Tables 1 and 2 respectively.
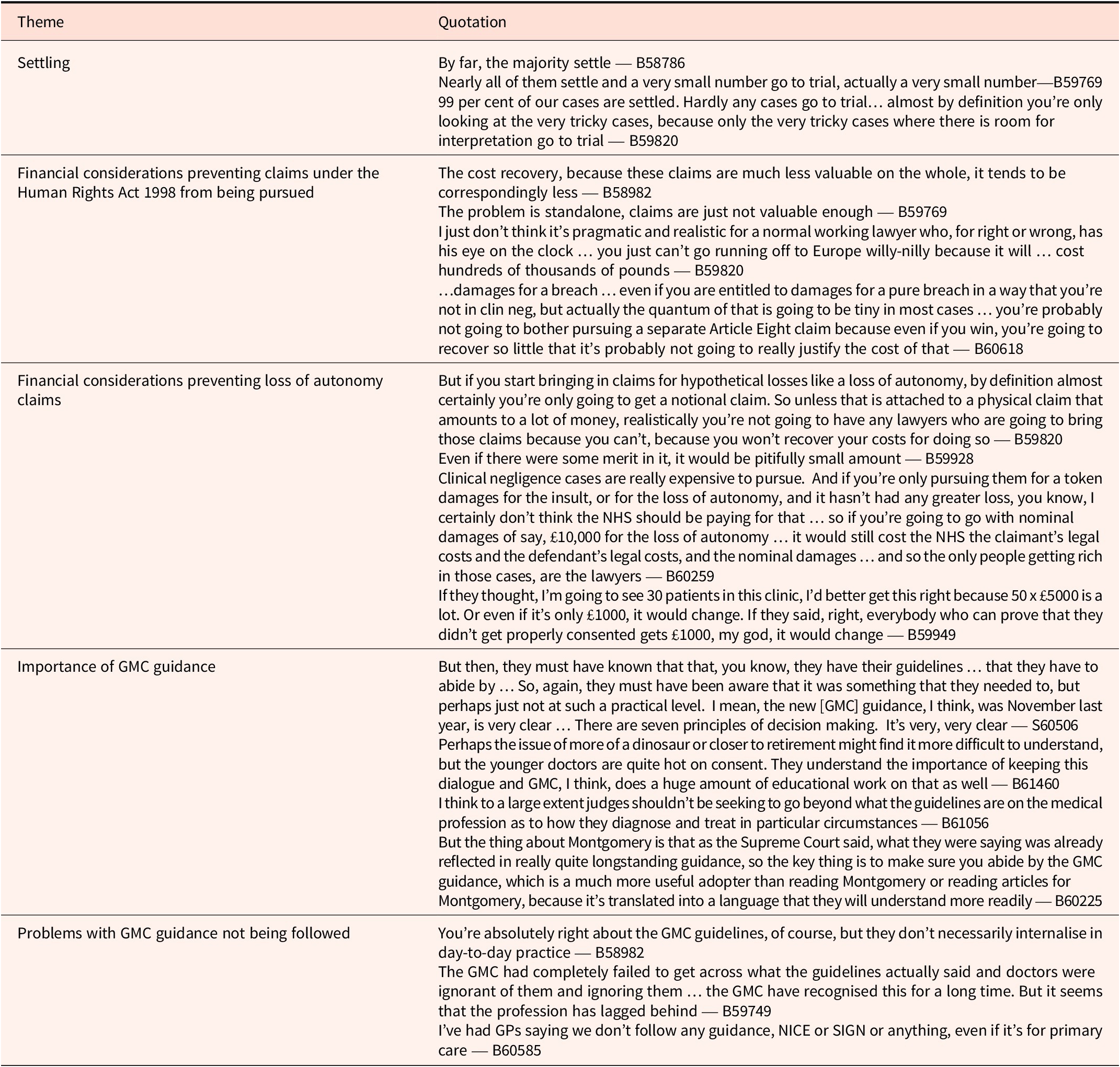
illustrative quotations from lawyer interviews

Table 1. Long description
Beginning at the top, the first row lists the theme Settling, with quotations highlighting that most cases settle, very few go to trial, and only tricky cases proceed to trial. The second row addresses financial considerations preventing claims under the Human Rights Act 1998, with quotations noting low value of claims, impracticality for lawyers, high costs, and minimal damages discouraging pursuit of Article Eight claims. The third row covers financial considerations preventing loss of autonomy claims, emphasizing that hypothetical losses yield only notional claims, insufficient recovery of costs, and nominal damages such as ten thousand pounds for loss of autonomy, with lawyers being the main beneficiaries. The fourth row discusses the importance of G M C guidance, referencing clear guidelines, seven principles of decision making, generational differences in understanding consent, and the Supreme Court's affirmation of longstanding guidance. The fifth row details problems with G M C guidance not being followed, including lack of internalization in daily practice, ignorance and disregard of guidelines, and G P statements about not following any guidance, including N I C E or S I G N.
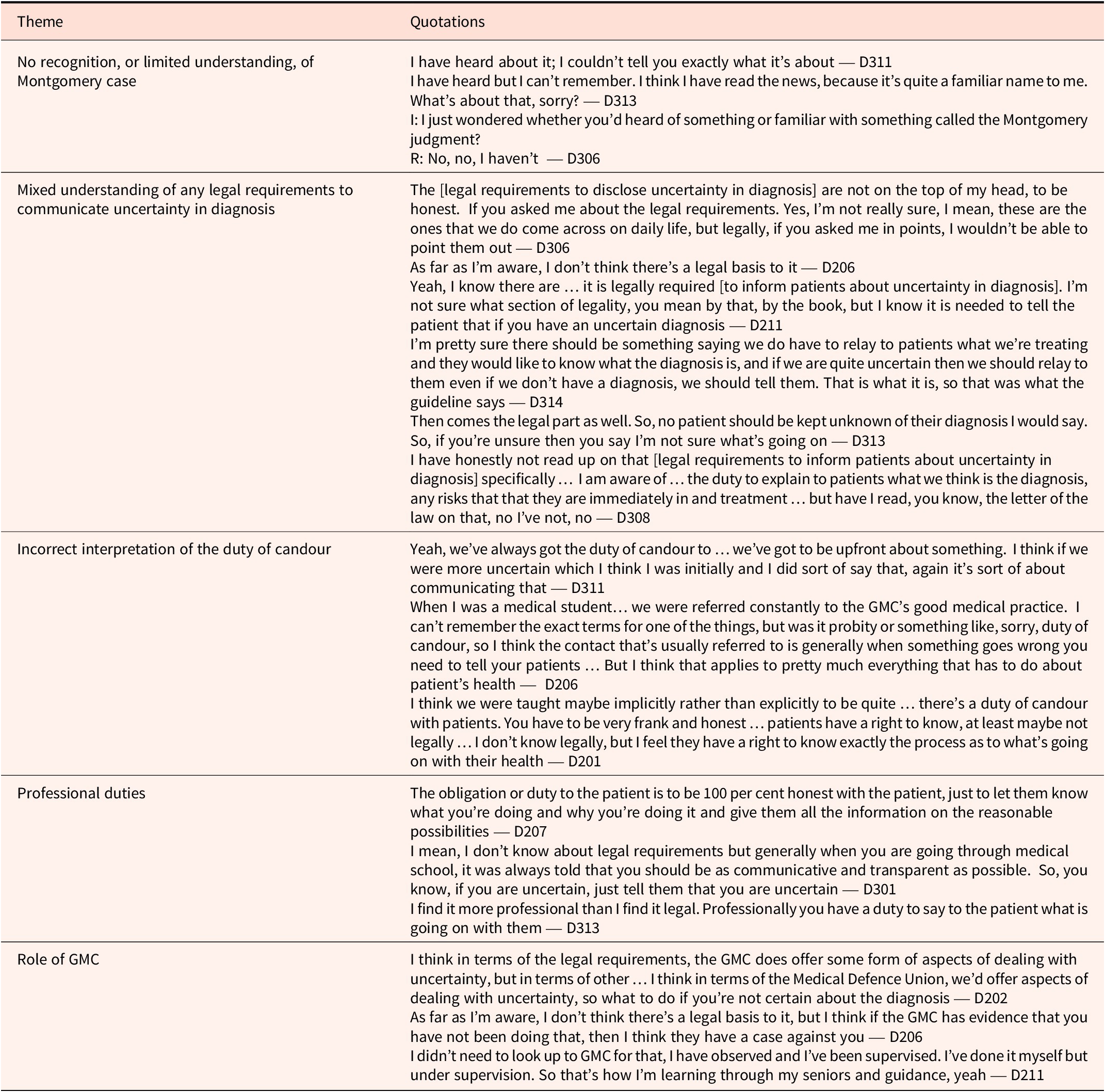
illustrative quotations from doctor interviews

Table 2. Long description
Starting from the top row, the left column lists the theme ‘No recognition, or limited understanding, of Montgomery case’ with quotations from D311, D313, and D306 expressing unfamiliarity or vague recollection. The next row presents ‘Mixed understanding of any legal requirements to communicate uncertainty in diagnosis’ with quotations from D306, D206, D211, D314, D313, and D308, reflecting uncertainty and varied interpretations of legal obligations. The third row is ‘Incorrect interpretation of the duty of candour’ with quotations from D311, D206, and D201, showing confusion about the scope and application of candour. The fourth row, ‘Professional duties,’ includes quotations from D207, D301, and D313, emphasizing honesty and transparency as professional obligations. The final row, ‘Role of GMC,’ contains quotations from D202, D206, and D211, discussing the General Medical Council's guidance and influence on handling uncertainty, with references to supervision and learning from seniors.
Part I: Factors Limiting the Power of Case Law to Drive Autonomy-Respecting Practice
We identified three main factors that limit the power of judicial decision-making to drive autonomy-respecting clinical practice.
First, legal interviewees said that practical and economic considerations significantly influence the number of cases that go to court. Only a small number of clinical negligence claims result in judicial decisions, fundamentally limiting the extent to which judicial decision-making can drive autonomy-respecting clinical practice.
Legal costs were foremost among these practical and economic considerations. Interviewees identified that the costs of bringing a claim can often run into “hundreds of thousands of pounds.” Lawyers taking on any such case must carefully consider whether the claim is likely to succeed and therefore whether they are likely to recover those costs. Various factors could reduce their willingness to accept claims for a breach of a claimant’s autonomy-based rights. Interviewees noted that standalone claims for a nominal sum under the HRA 1998 in particular would be “just not valuable enough,” given that a successful claimant is unlikely to recover a large amount of costs in respect of a low-value claim. Further, as one interviewee noted, the prospect of a fixed recoverable cost regime (as proposed by the Department for Health and Social Care in September 2023) 16 could render certain types of claims commercially unattractive by limiting the amount ultimately recoverable by a claimant’s legal representatives.
Practical considerations also mean that a large number of clinical negligence cases are resolved prior to trial. In 2023/2024, 81% of all clinical negligence claims managed by NHS Resolution were resolved without even entering court proceedings; NHS Resolution only ran 29 clinical negligence claims to trial in that year. 17 Notably, particularly large numbers of claims involving failures of consent per Montgomery settle. Wald, Bestwick, and Kelly have demonstrated that the decision in Montgomery led to a significant increase in settled claims of this type despite there being no such increase in claims for other causes.Reference Wald, Bestwick and Kelly 18
Legal interviewees stated that high rates of settlement reduce opportunities for the law to shape medical practice. This reduces the proportion of cases that reach a judge and therefore limits opportunities for judicial decision-making. Further, once such cases are resolved, there is no public record of the issues involved in the case, which limits discussion and learning. As one interviewee said, “no one goes away and thinks, oh, what can we learn from that case?” although others noted that the expense involved in settling high-value clinical negligence claims should drive NHS Resolution to analyze the outcome of settled cases and use that analysis to inform better patient care. This chimes with the views of academics such as Mulcahy, who has noted that reports of rising clinical negligence claims “reveal nothing about how many of these cases reach the litigation system or how typical they are of the general population of claims … they tell us very little about the trajectory claims make or the characteristics of claims that are abandoned or settled.” Reference Mulcahy19 It therefore appears that the practical and financial considerations that affect what claims end up in court reduce the opportunities for the development of new case law.
Second, legal interviewees also suggested that the practical effects of landmark decisions such as Montgomery may be diluted owing to the legal system’s focus on remedies. As they emphasized, a claimant needs to prove an entire cause of action. This requires that they prove not only that a doctor owed them a duty of care that was breached, but that the breach caused the claimant to suffer some kind of damage for which the law of negligence will compensate. Interviewees emphasized that it was these last requirements that often limit the effect of new case law — a change in what constitutes a breach of duty can have little effect in practice if it remains difficult to show causation and actionable loss. This became apparent when interviewees discussed whether the duty established in Montgomery to disclose the material risks of proposed treatments could extend to the disclosure of diagnostic uncertainty independent of treatment decisions. Interviewees pointed out the difficulty of showing that failure to disclose diagnostic uncertainty causes damage to the individual. They noted that, in general, the requirement to prove actionable loss reduced the potential for Montgomery to shape more patient-focused clinical practice. As one barrister put it, “Montgomery … has to be tied to an injury and … that really dilutes the culture change.”
Some interviewees suggested that recognizing standalone loss of autonomy awards could create positive changes in clinical practice as claimants would no longer need to prove that a failure to obtain informed consent had caused them injury (although we note that this proposal was rejected by the Court of Appeal in Shaw v Kovac). 20 For example, one interviewee stated “if they said, right, everybody who can prove that they didn’t get properly consented gets £1000, my god, it would change.” However, most interviewees thought that even if this type of claim was available, it would rarely be pursued in practice because of the likely small size of the financial awards. Some interviewees even felt that this would be an inappropriate use of NHS resources.
Third, it became apparent from our interviews with medical professionals that doctors had very limited knowledge about the specifics of current case law. Consequently, doctors’ poor understanding of case law may limit the extent to which it meaningfully influences their practice.
When directly asked if they were aware of the Montgomery decision, the majority of doctors interviewed had no recollection of the case. A minority had some awareness of it but were unable to provide any specific details (see Table 2 for quotations). Indeed, no doctor that we interviewed was able to correctly explain or summarize what duties Montgomery established.
Our interviews also revealed a generally mixed understanding about whether there was any legal basis for a duty to disclose information about uncertainty in diagnosis (a matter that has not yet been decided by the courts). Some doctors assumed that there must be such a legal basis, but none were able to explain clearly what specific case law or legislation they thought they were referring to. One doctor said, “I’m not sure what section of legality you mean by that, by the book, but I know it is needed to tell the patient that if you have an uncertain diagnosis.”
Our findings align with other empirical studies that have demonstrated doctors’ poor familiarity with Montgomery. Reference Knight21 It is also notable that even when doctors are aware of Montgomery, they may not change their practice: in one study, although 81% of surgeons were aware of the recent change in consent law, only 35% reported a noticeable change in the local consent process.Reference McKinnon 22 This may be due to practical barriers, such as limited time for consent discussions. However, it may also reflect a lack of understanding among doctors of the potential reach of case law across disciplines. For example, following Montgomery (a pregnancy case) there was a change in how doctors communicated material risk in pregnancy,Reference Bolton, Jha and Ferriman 23 but this did not spread uniformly to other specialties.Reference Wernham 24 In summary, there is a real concern that limitations in doctors’ awareness of relevant case law and in their application of that case law to clinical practice mean that even landmark rulings such as Montgomery are ineffective in driving changes in autonomy-respecting clinical practice.
Part II: The Need to Bolster the Role of Case Law in Improving Clinical Care
The findings from our interviews demonstrate that there are significant limitations to the extent to which case law influences changes in medical practice, particularly as regards the development of autonomy-based rights. Those who consider that the law should have a limited role to play in this sphere may find this unproblematic.Reference Montgomery 25 However, we consider that this gives legitimate cause for concern.
In our view, the law is an important means of driving the development and incorporation of autonomy-based rights in medical practice. As Foster and Miola argue, the law is particularly well-placed to regulate medical practice in circumstances where some individual right is at stake.Reference Foster and Miola 26 In these circumstances, a prospective decision-making body must draw on a variety of societal perspectives in order to make a decision that meets the changing needs and priorities of society.Reference Arvind and McMahon 27 The law is best placed to make these decisions impartially, transparently, and with a level of authority indicating the seriousness with which society takes these decisions. Further, the law performs two important functions by making such decisions.
The first is the law’s hortatory function. This refers to the role of the law as a guide to future conduct. Medical law should not merely respond to past wrongs; as Arvind and McMahon explain, it should also be capable of “encouraging individuals and organisations to conduct themselves in a manner that fulfils the law’s requirements.” 28 Case law can therefore function as a means of guiding the future protection of autonomy-based rights. However, this function is curtailed where legal decisions are poorly disseminated or understood. In those circumstances, legal decisions do not adequately guide doctors’ conduct, giving rise to a risk that the autonomy-based rights developed by such legal decisions will not be properly vindicated for other patients. This also gives rise to a purely practical concern that future negligence claims will arise that could have been avoided, adding to the liability burden on the NHS. In our view, it is therefore important that the hortatory function of clinical negligence law is properly upheld.
The second is the law’s adjudicatory function. As Foster and Miola point out, the law “has the authority to decide and the obligation to do so.” 29 The decision of a court of law can be enforced by a patient in a way that decisions by other regulators cannot. We consider that this provides an important remedy for patients who feel that their autonomy-based rights have been breached. However, the adjudicatory function of the law is diminished where patients struggle to bring their claims before a court, whether because of practical or economic considerations or because of difficulties in formulating a successful claim.
Our interview findings therefore give rise to a legitimate concern that clinical negligence law is not properly fulfilling its functions. In Part III, we consider potential ways to address these issues.
Part III: Levers of Change
The concerns outlined above led us to question what other levers of change might be available to drive autonomy-respecting clinical practice. In addition to civil litigation, a variety of tools are used to regulate medical practice, including self-regulation,Reference Farrell and Brazier 30 criminal proceedings, 31 inquests and public inquiries, 32 government agencies such as the Care Quality Commission, and statutory regulators such as the General Medical Council (which is responsible for, among other things, registration, licensing, revalidation and disciplinary proceedings). The efficacy of all these tools is hotly debated. Here we offer some suggestions as to how better to support and build on case law in changing clinical practice.
We believe that GMC guidance has significant potential to support the role of case law. Professional guidelines are intimately connected with judicial decision-making in the clinical negligence sphere. Perhaps the primary example is Montgomery itself; many scholars have argued that the effect of Montgomery is simply to repeat the patient-oriented professional duty of risk disclosure that had been recommended by the GMC for years. 33 Professional guidelines also benefit from being able to generalize judicial decisions across a range of different clinical scenarios, making it easier for clinicians to understand what their legal obligations are beyond the specific facts of any individual case.
We were therefore concerned to find that a number of our interviewees felt that GMC guidelines had little impact on clinical practice. One lawyer interviewed suggested that, prior to Montgomery, “the GMC had completely failed to get across what the guidelines actually said and doctors were ignorant of them.” This was reflected in the response of one of the doctors interviewed, who said that “I didn’t need to look up to GMC for [guidance on communicating uncertainty in diagnosis],” despite the fact that the GMC guidance then applicable on decision-making and consent emphasizes the need to convey precisely such uncertainties. 34 This is echoed by surveys showing that, in 2019, only 22% of doctors surveyed felt supported by the GMC to deliver high-quality care, and only a fifth of those attributed this feeling to the GMC’s provision of guidelines. 35
As one of our interviewees noted, NHS Resolution has a valuable role to play in learning from clinical negligence litigation (which is indeed one of NHS Resolution’s strategic priorities). It is uniquely placed with access to insight from both settled and litigated claims and the ability to share its findings with a wide variety of stakeholders, including clinicians. One of its current initiatives is the creation of a “Recommendation to Implementation” tool. 36 This aims to address information overload by consolidating recommendations from different sources into a single tool, currently for use by emergency medicine practitioners. This has been described by the Health Services Safety Investigations Body as “easy to use” with “early indications that these discussions could lead to clinical improvement for patient safety.” 37 While the tool is still in its early phases, it is possible that further collaboration between NHS Resolution and professional guideline providers, such as the GMC, will lead to better dissemination and implementation of case law in clinical practice.
Another legal mechanism that can be used to support autonomy-respecting clinical practice is the careful use of legislation. The legislative duty of candor 38 featured prominently in our interviews with doctors. Similarly, we consider that legislation concerning matters such as the use and storage of human tissue 39 and assisted dying (under consideration at the time of writing), 40 has the potential to further autonomy-respecting clinical practice. Such legislation must, of course, be drafted extremely carefully with proper regard for the views of parliamentarians, NHS Resolution, medical organizations, professionals, and the public.
Legislative changes must be properly disseminated to clinicians if they are to be effective. It was notable in our analysis that none of the doctors interviewed were aware of the precise parameters of the legislative duty of candor — when asked to describe it, one doctor said “I don’t know legally, but I feel they have a right to know exactly … what’s going on with their health.” This is echoed by recent analysis by the Department of Health and Social Care, which found that over 50% of the respondents felt that the duty was not fully known and understood by healthcare staff and less than 25% felt it was correctly complied with. 41 Inconsistency in understanding and a lack of proper training were identified as key problems. In our view, this underscores the need for proper dissemination of developments in legislation as well as case law.
Conclusion
These interviews — and our analysis — suggest that clinical negligence litigation is not a reliable means for enforcing or driving changes in clinical practice. The practical and economic barriers to bringing a case to trial are considerable. Even when judicial decisions are made, dissemination to doctors is poor, resulting in inconsistent understanding of the law among doctors. We consider that this is a matter of concern. The law has value in guiding clinical practice and ensuring that patient rights are protected, but these functions are evidently subject to considerable limitations.
We have set out suggestions as to how the role of case law in driving autonomy-respecting clinical practice can be both supported and supplemented by other drivers of change. We believe that GMC guidelines are an important way of communicating changes in case law, particularly when supported by evidence-backed tools to help clinicians avoid being overwhelmed by recommendations We further believe that legislative change has the potential to help drive change in clinical practice.
However, the critical message from our interviews and analysis is that changes in the law must be properly disseminated to clinicians if any of these levers of change are to be effective in the continuing development of autonomy-respecting clinical practice.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/jme.2026.10242.
Acknowledgements
Thank you to the lawyers and doctors who took part in this study. Thank you to Isabelle Le Gallez (ILG), Kathy Liddell (KML), Jeffrey Skopek (JS), Thea Hatfield (TH) and Janet Willars (JW) for their respective roles in undertaking interviews and providing comments and insights into earlier drafts of this manuscript.
Data Availability Statement
The participants of this study did not give written consent for their data to be shared publicly, only that the anonymized data collected may be used to support other researchers in the future. As such, the data that support the findings of this study are only available on request from the corresponding author, ZF.
Funding and Ethics
This research was funded in whole, or in part, by the Wellcome Trust 208213/Z/17/Z. For the purpose of open access, the author has applied a CC BY public copyright license to any Author Accepted Manuscript version arising from this submission.
CC and ZF are based in The Healthcare Improvement Studies Institute (THIS Institute), University of Cambridge. THIS Institute is supported by the Health Foundation, an independent charity committed to bringing about better health and healthcare for people in the UK. CC is a National Institute for Health Research (NIHR) academic clinical fellow.
The views expressed in this article are those of the authors and not necessarily those of the NHS, the NIHR, the Wellcome Trust or Crown Office Chambers. This study (IRAS ID: 265331, REC Reference: 19/SS/0089) was approved by the Health Research Authority and Essex Research Ethics Committee.
Contribution Statement
ZF conceived of the study and wrote the protocol. ILG conducted the lawyer interviews; TH and JW conducted the doctor interviews. ILG and AM coded the lawyer interview transcripts, CC and TH coded the doctor interview transcripts. ZF, AM and CC conducted the analysis and wrote the manuscript, with early discussions and input from KML and JS.
Competing Interests
No competing interests to disclose.



 Open access
Open access