


Introduction
Over the past 25 years, a growing body of evidence has emerged regarding the presence of cognitive deficits in bipolar disorder (BD) even after remission of mood symptoms. Several meta-analyses consistently reported that euthymic patients as a group show, despite preserved IQ, deficits in verbal memory, attention and executive functions with medium to large effect sizes (Arts, Jabben, Krabbendam, & van Os, Reference Arts, Jabben, Krabbendam and van Os2008; Bora, Yucel, & Pantelis, Reference Bora, Yucel and Pantelis2009; Mann-Wrobel, Carreno, & Dickinson, Reference Mann-Wrobel, Carreno and Dickinson2011; Torres, Boudreau, & Yatham, Reference Torres, Boudreau and Yatham2007. The same profile has been described for both BD type I and BD type II (Bora, Yücel, Pantelis, & Berk, Reference Bora, Yücel, Pantelis and Berk2011; Dickinson, Becerra, & Coombes, Reference Dickinson, Becerra and Coombes2017). The association between cognitive impairments and difficulties in psychosocial functioning was also systematically replicated in both cross-sectional and longitudinal studies (Depp et al., Reference Depp, Mausbach, Harmell, Savla, Bowie, Harvey and Patterson2012; Lomastro, Valerio, Szmulewicz, & Martino, Reference Lomastro, Valerio, Szmulewicz and Martino2021).
In a further step, research advanced by demonstrating the heterogeneity in cognitive profiles within the patient group. The early studies established different cut-off points to define cognitive deficits; depending on whether they were more lax (e.g. performance below 2 standard deviations in a test) or more stringent (e.g. performance below 2 standard deviations on 2 different cognitive domain tests), between one and two thirds of euthymic patients were reported to have no significant cognitive impairment (Gualtieri & Morgan, Reference Gualtieri and Morgan2008; Iverson, Brooks, Langenecker, & Young, Reference Iverson, Brooks, Langenecker and Young2011; Martino et al., Reference Martino, Strejilevich, Scápola, Igoa, Marengo, Ais and Perinot2008; Reichenberg et al., Reference Reichenberg, Harvey, Bowie, Mojtabai, Rabinowitz, Heaton and Bromet2009). One study used simultaneously ‘soft’ and ‘hard’ cut-off points to define cognitive impairment. This study reported that while 30% of the sample of euthymic BD patients had cognitive and psychosocial functioning indistinguishable from that of healthy controls, another 30% of patients had cognitive impairment more profound and extensive than that usually reported in the literature (Martino et al., Reference Martino, Strejilevich, Marengo, Ibañez, Scápola and Igoa2014). A series of subsequent studies used multivariate statistics (i.e. cluster analysis or latent class analysis) instead of cut-off points to explore cognitive heterogeneity. The results were also consistent, with about one-third of patients showing intact neurocognitive functioning, one-third selective deficits, and one-third global impairment (Burdick et al., Reference Burdick, Russo, Frangou, Mahon, Braga, Shanahan and Malhotra2014; Lewandowski, Sperry, Cohen, & Ongür, Reference Lewandowski, Sperry, Cohen and Ongür2014; Solé et al., Reference Solé, Jiménez, Torrent, Del Mar Bonnin, Torres, Reinares and Martínez-Arán2016; Volkert et al., Reference Volkert, Kopf, Kazmaier, Glaser, Zierhut, Schiele and Reif2015).
Despite consistent advances in this field, there is still controversy regarding how to explain the heterogeneity of cognitive deficits, as well as their origin and trajectory throughout the course of the illness (Samamé, Reference Samamé2024; Vieta, Reference Vieta2024). Two hypotheses have been put forward as alternatives to help explain these issues, neuroprogression and neurodevelopmental abnormalities as detailed below.
Neuroprogression as determinant of cognitive impairment
Neuroprogression was conceptualized as a pathological rewiring of the brain that takes place in parallel with the functioning and clinical deterioration in the course of BD (Berk, Reference Berk2009; Kapczinski et al., Reference Kapczinski, Vieta, Andreazza, Frey, Gomes, Tramontina and Post2008). The proponents of this hypothesis argue that BD has a progressive clinical course, evolving through different stages from at-risk to more severe and disabling presentations (Berk et al., Reference Berk, Conus, Lucas, Hallam, Malhi, Dodd and McGorry2007, Reference Berk, Post, Ratheesh, Gliddon, Singh, Vieta and Dodd2017; Gama, Kunz, Magalhães, & Kapczinski, Reference Gama, Kunz, Magalhães and Kapczinski2013; Kapczinski et al., Reference Kapczinski, Dias, Kauer-Sant'Anna, Frey, Grassi-Oliveira, Colom and Berk2009). Regarding neurocognition, this hypothesis proposes a progression from no cognitive impairments in the premorbid and early stages of illness, in which periods of euthymia are well defined, to severe cognitive impairments in later stages of the disorder as a consequence of successive mood episodes (Cardoso, Bauer, Meyer, Kapczinski, & Soares, Reference Cardoso, Bauer, Meyer, Kapczinski and Soares2015; Kapczinski et al., Reference Kapczinski, Dias, Kauer-Sant'Anna, Frey, Grassi-Oliveira, Colom and Berk2009; Rosa et al., Reference Rosa, Magalhães, Czepielewski, Sulzbach, Goi, Vieta and Kapczinski2014). From this perspective, heterogeneity in cognitive functioning might be explained based on the stage of the illness. However, empirical evidence supporting both premises (i.e. absence of cognitive deficits in early stages and worsening of these throughout the course of the illness) is scarce and limited.
The notion of ‘no cognitive impairments in the premorbid and early stages of illness’ might be supported by some cohort studies showing that, unlike in schizophrenia, the IQ or other measures of general intelligence or academic performance of people who later develop BD are not affected (for a review see Martino, Samamé, Ibañez, & Strejilevich, Reference Martino, Samamé, Ibañez and Strejilevich2015). This is not surprising, given that as mentioned above, even most studies done with BD patients report premorbid or current IQ values comparable to those of healthy controls (Arts et al., Reference Arts, Jabben, Krabbendam and van Os2008; Bora et al., Reference Bora, Yucel and Pantelis2009; Mann-Wrobel et al., Reference Mann-Wrobel, Carreno and Dickinson2011; Torres et al., Reference Torres, Boudreau and Yatham2007). However, it cannot be inferred from these results that patients with BD do not have cognitive deficits in premorbid or early stages, since they may have impairment of different cognitive domains (i.e. verbal memory, attention, executive function) that are not reflected in IQ deviations. In fact, the few studies evaluating cognitive domains in subjects at risk who later develop BD show worse performance than controls (for a review see Martino et al., Reference Martino, Samamé, Ibañez and Strejilevich2015). Furthermore, different studies and meta-analyses found that healthy relatives of subjects with BD show some degree of impairments in executive functions, attention and verbal memory (Arts et al., Reference Arts, Jabben, Krabbendam and van Os2008; Bora et al., Reference Bora, Yucel and Pantelis2009). It is evidently contradictory to assume that patients with BD do not have cognitive impairment in the premorbid or early stages of the illness but that their healthy relatives do. Finally, another line of evidence that conflicts with this premise of neuroprogression comes from studies conducted on first episodes of BD. Different meta-analyses have reported that the profile of cognitive deficits found in patients with a first manic episodes or after their remission is similar to that reported in patients in the middle course of the illness (Bora & Pantelis, Reference Bora and Pantelis2015; Lee et al., Reference Lee, Hermens, Scott, Redoblado-Hodge, Naismith, Lagopoulos and Hickie2014).
The notion of ‘severe cognitive impairments in later stages of the disorder’ comes from cross-sectional studies showing a positive association between the number of previous mood episodes and the severity of cognitive deficits. This was a finding consistently reported by almost all research groups, either through correlation/regression analyses or by comparing patients with many and few previous mood episodes (López-Jaramillo et al., Reference López-Jaramillo, Lopera-Vásquez, Gallo, Ospina-Duque, Bell, Torrent and Vieta2010; Martino, Igoa, Marengo, Scápola, & Strejilevich, Reference Martino, Igoa, Marengo, Scápola and Strejilevich2018a; Robinson & Ferrier, Reference Robinson and Ferrier2006; Torres et al., Reference Torres, DeFreitas, DeFreitas, Kauer-Sant'Anna, Bond, Honer and Yatham2010). The authors proposing the neuroprogression hypothesis interpret these findings as meaning that successive mood episodes lead to progressive cognitive impairment (Berk et al., Reference Berk, Post, Ratheesh, Gliddon, Singh, Vieta and Dodd2017; Cardoso et al., Reference Cardoso, Bauer, Meyer, Kapczinski and Soares2015; Kapczinski et al., Reference Kapczinski, Dias, Kauer-Sant'Anna, Frey, Grassi-Oliveira, Colom and Berk2009). However, it has been noted that the direction of causality of this association cannot be inferred from cross-sectional studies (Martino et al., Reference Martino, Strejilevich, Marengo, Igoa, Fassi, Teitelbaum and Caravotta2013; Martino, Samamé, Marengo, Igoa, & Strejilevich, Reference Martino, Samamé, Marengo, Igoa and Strejilevich2016). Even if cognitive deficits were stable over the course of the disorder – and related with mood episodes – the same pattern of findings might be observed (Fig. 1). Consequently, this type of results should not be taken as evidence supporting the neuroprogression hypothesis.
Schematic diagram of the lifetime clinical course of a hypothetical sample of 6 patients with bipolar disorder under the assumption that recurrence of mood episodes (represented by black columns) and cognitive impairment (represented by gray bar with dotted line) is stable from illness onset. The cognitive impairment after a first mood episode is the average of the 6 patients (absent in patients 1–2, moderate in 3–4, and severe in 5–6), but after a third episode it is that of patients 3–6 and after a fifth episode it is that of patients 5–6. Thus comparing cognitive impairment in patients with many v. few episodes can lead to the misinterpretation that these features increase with successive episodes even though they were stable. The same positive results would be obtained in correlation analysis between cognitive deficits and number of mood episodes and, therefore, they should not be used as evidence of neuroprogression.

On the other hand, further lines of evidence also conflict with the notion of progressive cognitive deficits in BD. For example, results of neurocognitive studies in older adults with BD show similar results to those reported in younger patients, suggesting no progression of impairment (for a review see Samamé, Martino, & Strejilevich, Reference Samamé, Martino and Strejilevich2013). More importantly, early meta-analyses of longitudinal studies show stability of cognitive deficits throughout the course of the illness (Bora & Özerdem, Reference Bora and Özerdem2017; Samamé, Martino, & Strejilevich, Reference Samamé, Martino and Strejilevich2014). Another meta-analysis focused on longitudinal studies of patients with recent onset or older adults and found the same pattern of cognitive stability reported in the middle course of the illness (Szmulewicz, Valerio, & Martino, Reference Szmulewicz, Valerio and Martino2020). Furthermore, a longitudinal study of around 6 years of follow-up specifically designed to measure this association found that although verbal memory deficits and executive dysfunction were associated with the number of (hypo)manic episodes and with the time spent with (hypo)manic symptomatology during follow-up, successive episodes did not modify cognitive performance (Martino et al., Reference Martino, Igoa, Marengo, Scápola and Strejilevich2018a). Finally, more recent longitudinal studies in patients belonging to different age groups and with up to 10 years of follow-up also consistently show stability of cognitive performance throughout the course of the illness (Flaaten et al., Reference Flaaten, Melle, Bjella, Engen, Åsbø, Wold and Ueland2024; Frías et al., Reference Frías, Dickstein, Merranko, Gill, Goldstein, Goldstein and Birmaher2017; Jiménez-López et al., Reference Jiménez-López, Sánchez-Morla, López-Villarreal, Aparicio, Martínez-Vizcaíno, Vieta and Santos2019; Schouws, Comijs, Dols, Beekman, & Stek, Reference Schouws, Comijs, Dols, Beekman and Stek2016; Sparding et al., Reference Sparding, Joas, Clements, Sellgren, Pålsson and Landén2021). The same stability profile resulted from a recent meta-analysis based exclusively on controlled studies of long-term (>5 years) cognitive outcomes, with a weighted mean follow-up period of 8.9 years (Samamé, Cattaneo, Richaud, Strejilevich, & Aprahamian, Reference Samamé, Cattaneo, Richaud, Strejilevich and Aprahamian2022).
Overall, empirical evidence does not support any of the premises of the neuroprogression hypothesis. In this context, another alternative hypothesis proposes neurodevelopmental abnormalities in a subset of BD patients to explain the heterogeneity of cognitive deficits, their origin and trajectory throughout the course of the illness.
Neurodevelopment as determinant of cognitive impairment
As mentioned above, one-third of BD patients have global cognitive impairment, and converging evidence from studies of first episodes, at-risk individuals who later develop BD, and healthy family members suggests that these deficits would precede the first mood episodes. Conversely, another third of patients have intact neurocognitive functioning even after the onset of the disease. Interestingly, some recent studies have shown that a similar pattern of cognitive heterogeneity reported in patients is found in their healthy relatives (Bora et al., Reference Bora, Can, Ildız, Ulas, Ongun, Inal and Ozerdem2019; Russo et al., Reference Russo, Van Rheenen, Shanahan, Mahon, Perez-Rodriguez, Cuesta-Diaz and Burdick2017; Valli et al., Reference Valli, Serna, Borràs, Ilzarbe, Baeza, Picouto and Castro-Fornieles2021). Thus, the neurocognitive impairment reported in healthy relatives would depend fundamentally on those of patients with global cognitive deficits, while the same pattern of indemnity would be reproduced in relatives of patients with intact neurocognitive functioning. These same profiles of cognitive subtypes have shown no change over time in longitudinal analyses and have been reproduced in older adults with BD, suggesting the stability of these throughout the course of the illness (Martino, Marengo, Igoa, & Strejilevich, Reference Martino, Marengo, Igoa and Strejilevich2018b; Martino, Scápola, & Strejilevich, Reference Martino, Scápola and Strejilevich2017), which is also consistent with the results of longitudinal studies on neurocognition (Bora & Özerdem, Reference Bora and Özerdem2017; Samamé et al., Reference Samamé, Martino and Strejilevich2014, Reference Samamé, Cattaneo, Richaud, Strejilevich and Aprahamian2022; Szmulewicz et al., Reference Szmulewicz, Valerio and Martino2020). Taken together, these findings support the hypothesis of neurodevelopmental abnormalities. This hypothesis proposes abnormalities in brain development (either genetic or environmental in origin) might affect a subset of BD patients and play a relevant role in the development of cognitive deficits, premorbid behavioral disorders or neurological symptoms.
Other lines of evidence also support this hypothesis. For example, as mentioned above, studies often report average academic performance or general intelligence similar to controls in subjects who later develop BD. However, two of the largest cohort studies reported a bimodal pattern in which both high and low performance increased the risk of BD suggesting some underlying pathophysiological differences in subsets of subjects who later develop the illness (Gale et al., Reference Gale, Batty, McIntosh, Porteous, Deary and Rasmussen2013; MacCabe et al., Reference MacCabe, Lambe, Cnattingius, Sham, David, Reichenberg and Hultman2010). Some prospective cohort studies in at-risk subjects and youth with BD are also consistent with the neurodevelopmental hypothesis. Thus, it has been reported that while some offspring of patients with BD develop the illness without major premorbid abnormalities, others may show cognitive or socialization problems, schizoid or attention-deficit hyperactivity disorder (ADHD) before the onset (Duffy et al., Reference Duffy, Horrocks, Doucette, Keown-Stoneman, McCloskey and Grof2014). Similarly, another study in youth with BD reported that those with low neurocognitive functioning had a higher prevalence of ADHD, more difficulties in academic and social functioning, and more manic and depressive symptoms over 2.5 years of follow-up (Frías et al., Reference Frías, Dickstein, Merranko, Gill, Goldstein, Goldstein and Birmaher2017). These results are consistent with those observed in adults in the middle course of BD, in which patients with cognitive impairment are those with a high density of mood episodes and poor psychosocial functioning, whereas patients with intact cognitive functioning tend to have a more benign clinical course and better functional outcome (Flaaten et al., Reference Flaaten, Melle, Bjella, Engen, Åsbø, Wold and Ueland2024; Lomastro et al., Reference Lomastro, Valerio, Szmulewicz and Martino2021; Martino et al., Reference Martino, Strejilevich, Marengo, Igoa, Fassi, Teitelbaum and Caravotta2013; Reference Martino, Samamé, Marengo, Igoa and Strejilevich2016; Reinares et al., Reference Reinares, Papachristou, Harvey, Mar Bonnín, Sánchez-Moreno, Torrent and Frangou2013; Valerio, Lomastro, & Martino, Reference Valerio, Lomastro and Martino2020). Thus, even when cognitive deficits were stable throughout the course of the illness, they would be more severe in subjects with a greater density of mood episodes (Fig. 1) (Martino et al., Reference Martino, Strejilevich, Marengo, Igoa, Fassi, Teitelbaum and Caravotta2013, Reference Martino, Samamé, Marengo, Igoa and Strejilevich2016). The cause of this association is currently a matter of speculation and may be the focus of future research. It could be hypothesized that both features have a common cause depending on damage to structures (e.g. corticostriatal pathways) involved in both mood regulation and neurocognitive functioning. Alternatively, it could be speculated that those patients with global cognitive deficits might have a worse clinical course (i.e. greater risk of recurrences) as a consequence of their lower adherence to medication or to their lower ability to recognize prodromal symptoms, to maintaining regular lifestyles, or to obtain benefits from psychosocial approaches such as psychoeducation.
Finally, another line of evidence consistent with the model of neurodevelopmental abnormalities in BD comes from studies of soft neurological signs (NSS), which refer to subtle impairments in sensory integration, motor coordination, and the sequencing of complex motor acts. These neurological dysfunctions linked to developmental abnormalities are more prevalent in BD than in healthy subjects, and have been associated with lower premorbid IQ and severe cognitive impairment (Baş, Poyraz, Baş, Poyraz, & Tosun, Reference Baş, Poyraz, Baş, Poyraz and Tosun2015; Bora, Akgül, Ceylan, & Özerdem, Reference Bora, Akgül, Ceylan and Özerdem2018; Valerio, Lomastro, Igoa, & Martino, Reference Valerio, Lomastro, Igoa and Martino2023).
Discussion and future directions
Much progress has been made in understanding neurocognitive functioning in BD, although it is still difficult to obtain a comprehensive view of the topic. Neuroprogression was proposed as a hypothesis that could contribute to explaining heterogeneity, origins, and trajectory of cognitive deficits in BD, although its premises (i.e. absence of cognitive deficits in early stages and progressive cognitive decline with successive episodes) are not supported by empirical data.
The alternative hypothesis of neurodevelopmental abnormalities seems to harmonize better with empirical data available to date (Fig. 2). According to this proposal, the global cognitive dysfunction observed in one-third of BD patients as impairments in verbal memory, attention, and executive functions would be present prior to the illness onset (as suggested by the results of studies of subjects at risk who later develop BD, those in their first episode, and those of healthy relatives). Presumably, these would be patients with a normal-low premorbid IQ, and with a higher risk of academic and social maladjustments and a higher prevalence of comorbidities (i.e. schizoid or ADHD) in the premorbid stage. After the onset of BD, these patients would have a higher density of mood episodes, particularly manic ones, throughout their illness. Likewise, this subset of patients would have a higher prevalence of NSS or other neurodevelopmental markers. Both as a consequence of global cognitive impairments and of the worse clinical course, these patients would be those with the poor functional outcome.
Schematic profiles of bipolar patients with and without neurodevelopmental abnormalities. (a) Patients without neurodevelopmental abnormalities do not have premorbid disturbances or neurocognitive dysfunction (gray bar with dotted line) before or after the onset of the illness. In the postmorbid stage, they have a more benign clinical course with a lower density of mood episodes (black columns) and better functional outcome similar – in some cases – to healthy subjects. (b) Patients with neurodevelopmental abnormalities have different premorbid disturbances such as socialization and academic problems or comorbidities (e.g. schizoid or ADHD). Even though they have normal-low IQ, they may show impairment in measures of verbal memory, attention or executive functions (gray bar with dotted line) in the premorbid stage that are maintained after the illness onset. In the postmorbid stage, they have a higher density of mood episodes (black columns) and worse functional outcome similar – in some cases – to subjects with schizophrenia.
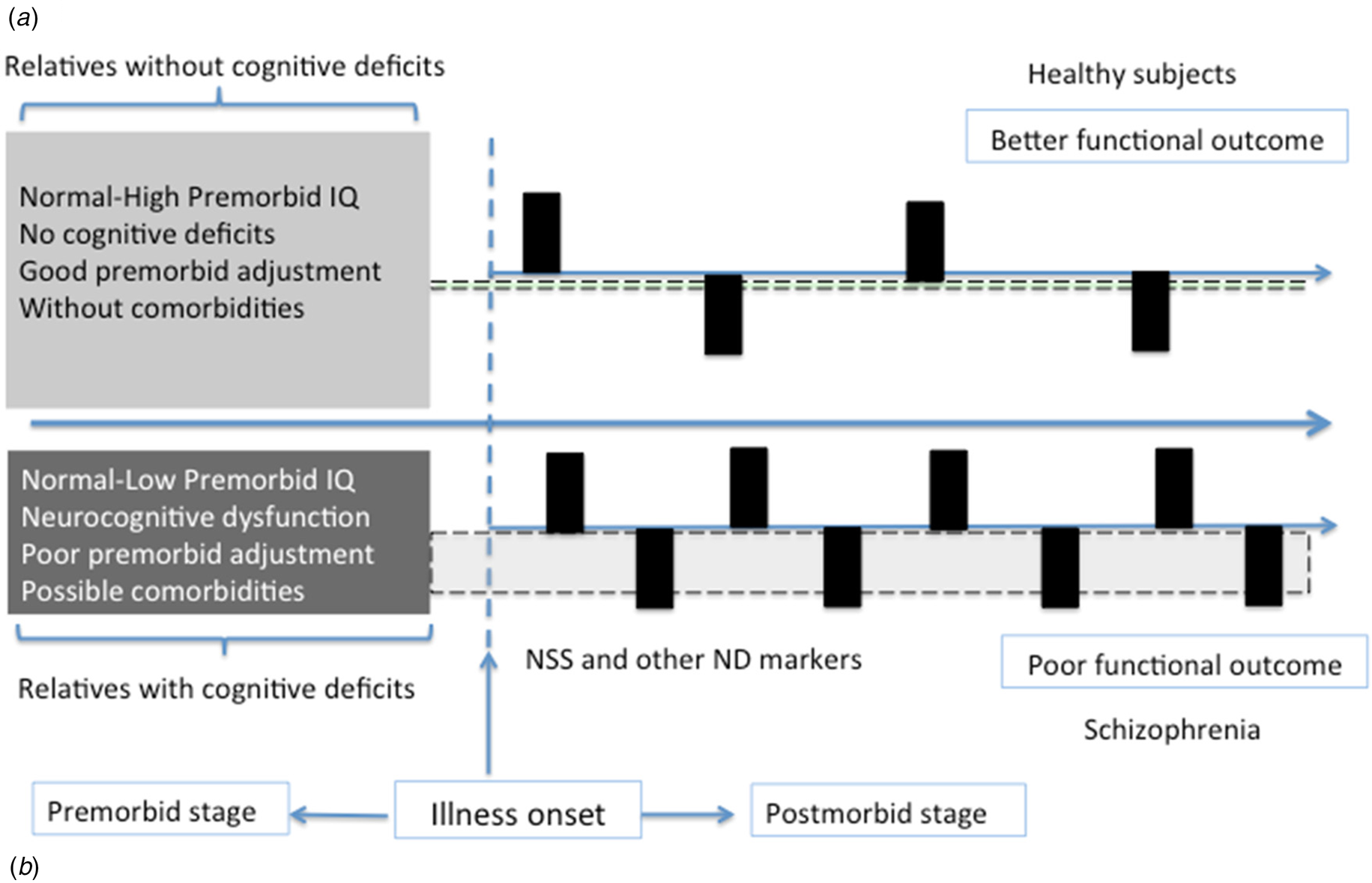
In contrast, the other two-thirds of patients would include those with preserved cognitive functioning or selective deficits (Fig. 2). Most of these patients would have normal-high premorbid cognitive functioning, without major social-academic maladjustment or comorbidities before the onset of BD. Consequently, healthy relatives of these patients would not show significant cognitive impairment. After the illness onset, these patients would have a more benign clinical course with lower mood episode density and better psychosocial functioning. Of course, despite this general pattern, there would be high variability regarding clinical course, neurocognitive performance, and functional outcome within this subset of patients. In fact, about half of these patients might have selective cognitive deficits. Selective cognitive deficits could be a consequence of minor neurodevelopmental abnormalities or, alternatively, of different factors related to cognitive deficits in BD: psychiatric (e.g. anxiety disorders, substance use disorders) or medical (e.g. hypothyroidism) comorbidities, adverse effects of medication (e.g. antipsychotics or benzodiazepines), or unhealthy lifestyle habits (e.g. sleep disturbances, sedentary lifestyle, etc.).
Overall, the neurodevelopmental hypothesis is consistent with the early/premorbid origin of cognitive deficits in a subset of BD patients and their stability throughout the course of the illness. It also allows us to understand neurocognitive heterogeneity in BD, with some patients having impairment similar to that reported in people with schizophrenia at one extreme, and subjects with extraordinary cognitive and creative abilities at the other. This great heterogeneity and its explanation through the neurodevelopmental hypothesis raises the question of whether or not it is appropriate to include all these patients within the same psychiatric disorder (i.e. BD), which could be the focus of future studies. Of course, it should ideally include longitudinal follow-up of subjects at risk for BD, although these are the most difficult studies to implement. Alternatively, analysis of the pattern of cognitive heterogeneity in first-episode patients and their longitudinal follow-up (both in terms of clinical course and neurocognitive functioning) could also provide interesting information. Although the literature supports a pattern of stability of cognitive deficits throughout the illness, this must be further explored separately in these patient subsets (with and without neurodevelopment markers). Finally, neuroimaging and laboratory biomarkers might differ in patients with and without neurodevelopment abnormalities, which could also be the focus of future studies. Similarly, family aggregation and genetic studies in these subsets of patients could also contribute relevant information.
Neurocognition has been one of the most prolific fields of research in BD during the last decades and we must make an attempt to integrate current knowledge and continue to move forward. There is potential to improve our understanding of the heterogeneous clinical features (and longitudinal course) and pathophysiological substrate of BD through this path.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
None.



 Open access
Open access