


Introduction
There has been a considerable volume of literature addressing the intersection of cancer and mood disorders, particularly concerning the relationship between cancer and depression. It has been recognized as early as since the 1930s that depressive episodes may predispose an onset of cancer. Mood symptoms that emerge before cancer diagnosis have been known as “premonitory depression” (Lauter Reference Lauter1973; Cosci et al. Reference Cosci, Fava and Sonino2015). A recent study demonstrated that 21% of patients with pancreatic cancer had a history of depression prior to their cancer diagnosis (Seoud et al. Reference Seoud, Syed and Carleton2020; Michoglou et al. Reference Michoglou, Ravinthiranathan and San Ti2023). The argument has been continuing regarding whether depression arises as a psychological response to a cancer diagnosis, or a biological reaction to cancer. Recent research increasingly focuses on the biological mechanisms underlying the association between depression and cancer (Bortolato et al. Reference Bortolato, Hyphantis and Valpione2017). Chronic exposure to elevated inflammatory cytokines due to cancer leads to alterations in neurotransmitter systems and can develop neuropsychiatric disorders such as depression (Felger and Lotrich Reference Felger and Lotrich2013).
Bipolar disorder (BD) is a mental disorder that accompanies both depressive symptoms and manic symptoms. Its estimated prevalence rate is 2% and shows a gradual increase globally (Merikangas et al. Reference Merikangas, Jin and He2011; He et al. Reference He, Hu and Ren2020). In contrast with the research on depression and cancer, research on the relationship between BD or manic episodes and cancer has been relatively limited. Epidemiological data from large-scale cohort studies on breast cancer indicate that the incidence rate of breast cancer is 2.06 times higher in individuals with BD compared to the control group (Hung et al. Reference Hung, Liu and Tsai2013). Kanani et al. reported that breast cancer patients with comorbid mood disorders (depression or BD) experience poorer overall survival compared to those without such mood disorders (Kanani et al. Reference Kanani, Davies and Hanchett2016).
Literature to date suggests that the causes of manic states in patients with cancer have been categorized into three etiological perspectives: organic, drug-induced, and psychogenic. Krauthammer and Klerman (Reference Krauthammer and Klerman1978) introduced the concept of “secondary mania” in their seminal work on cancer and manic states. They reviewed various organic and pharmacological factors, such as drugs, infections, neoplasms, epilepsy, and metabolic disorders, that can induce manic states.
An increasing number of reports support the possibility of a pathophysiological link between cancer and BD (Asevedo et al. Reference Asevedo, Brietzke and Chaves2013). Cytokine-induced abnormalities in inflammation, hormones, and the immune system in individuals with cancer may represent a key pathophysiological pathway in the onset of manic episodes in BP (Goldberg and Schwertfeger Reference Goldberg and Schwertfeger2010; Błogowski et al. Reference Błogowski, Deskur and Budkowska2014; Van den Ameele et al. Reference Van den Ameele, van Diermen and Staels2016). Cytokine levels (such as TNF-α and IL-6), which rise in manic states, are known to increase in cancer patients as well. Hormonal abnormalities, specifically dysfunction of the hypothalamic-pituitary-adrenal axis, can cause impairments in neuroplasticity and brain dysfunction (Bauer et al. Reference Bauer, Pascoe and Wollenhaupt-Aguiar2014; Rosenblat et al. Reference Rosenblat, Cha and Mansur2014). The incidence of BP increases by 70% within five years following an autoimmune disease diagnosis (Eaton et al. Reference Eaton, Pedersen and Nielsen2010; Benros et al. Reference Benros, Eaton and Mortensen2014; León-Caballero et al. Reference León-Caballero, Pacchiarotti and Murru2015).
Manic episodes may develop as a reaction to psychological stress (“psychogenic”) (Morgan et al. Reference Morgan, Beckett and Zolese2001), although the current diagnostic criteria, such as DSM-5 (American Psychiatric Association. 2013) and ICD-11 (World Health Organization 2019), do not formally recognize the term psychogenic mania. Studies have demonstrated the correlation between stressful life events and the onset or recurrence of manic episodes of BD (Kessing et al. Reference Kessing, Agerbo and Mortensen2004; Carmassi et al. Reference Carmassi, Shear and Corsi2020; Rodrigues Cordeiro et al. Reference Rodrigues Cordeiro, Côrte-Real and Saraiva2023).
BD remains a significant therapeutic challenge due to its symptom fluctuations and the resulting deterioration of patients’ functioning, heightened risk of suicide, and need for psychiatric hospitalization (Pompili et al. Reference Pompili, Gonda and Serafini2013; Harrison et al. Reference Harrison, Geddes and Tunbridge2018). Manic symptoms are particularly problematic due to patients’ heightened impulsiveness, aggression, irritability, and excitement (Gonçalves-Pinho et al. Reference Gonçalves-Pinho, Freitas and von Doellinger2022). In cancer patients, manic episodes may hamper the initiation or continuation of cancer therapy due to the patients’ aggression and medication non-compliance. Typically, the treatment of psychiatric symptoms (including admission to psychiatric beds) is prioritized over cancer treatment, resulting in the postponement or cessation of cancer therapies, which can exacerbate the progression of cancer (Tohen and Grundy Reference Tohen and Grundy1999). Additionally, patients with BD may refuse medication during their manic episodes, which also poses significant challenges for cancer treatment. Further, mistrust and aggression towards medical staff and family members prevent appropriate cancer treatment and care (Perlick et al. Reference Perlick, Clarkin and Sirey1999; Osawa et al. Reference Osawa, Ukai and Tsuji2013). Even after the manic episodes are remitted, the family may not be as emotionally supportive as before to the patient, which may lead to missed opportunity for the patient for appropriate cancer care. Also, psychological damage to family members may remain.
To the best of the authors’ knowledge, there are only sporadic studies of the emergence of manic states in the context of cancer, leaving a gap in understanding the etiology and the influence of manic episodes on cancer treatments. Therefore, in the current study, the authors conducted a systematic review to elucidate the characteristics of manic states in cancer patients. Once the review has been done, the authors expect that therapeutic strategies for manic episodes in patients with cancer would be made clearer.
Method
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline (Page et al. Reference Page, McKenzie and Bossuyt2021) and the protocol for this study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) of the National Institute for Health and Care Research, UK (CRD42020182372). The following studies were eligible: (1) cases of comorbid cancer and manic states (manic or hypomanic states), (2) without a history of mental illness prior to cancer diagnosis, (3) epidemiological studies or case reports, and (4) written in English or Japanese. The following reports were excluded: (1) cases of benign proliferative diseases, or (2) cases with a history of mental illness that were not attributable to cancer. We searched the following electronic databases: PubMed, Cochrane, CINAHL, and Igaku Chuo Zasshi, for the studies published between 1950 and 6 August 2021. Boolean searches were performed using the following Mesh terms: (“mania” OR “hypomania” OR “bipolar disorder”) AND (“cancer”). After removing duplicates, two authors (K.O. and D.F.) screened the titles and abstracts, then reviewed the full texts. References from the selected papers were manually searched. Any discrepancies between the two reviewers were discussed until agreement.
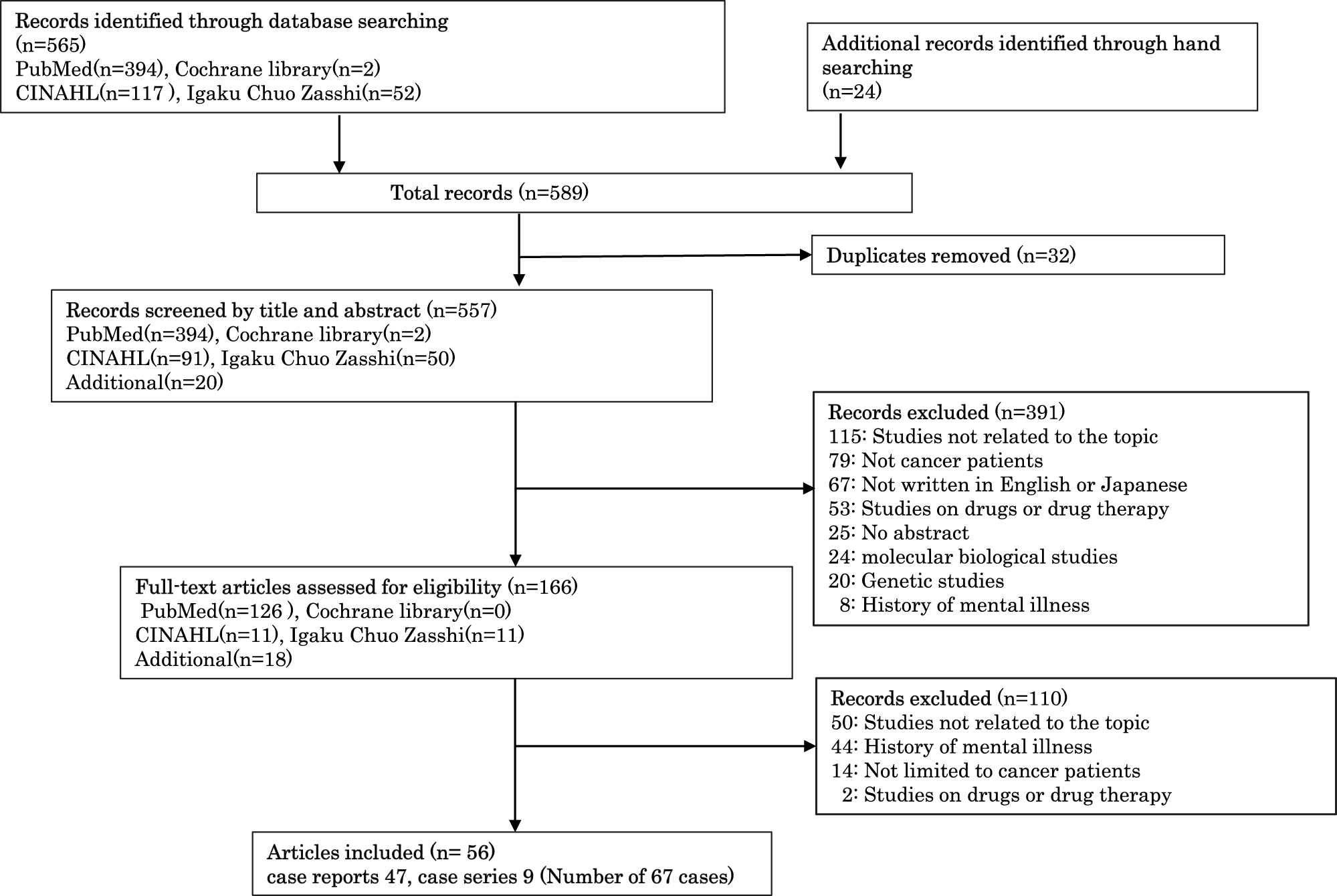
The following information was collected: the causes, timing of onset of manic states, their course and outcomes, including admissions to a psychiatric ward, pharmacotherapy and maintenance therapy for manic symptoms, duration until remission of manic states, recurrence of manic states, and the impact of manic states on cancer treatment. The flow diagram of the systematic literature search is presented in Figure 1.
Flow diagram of the systematic literature search.

Results
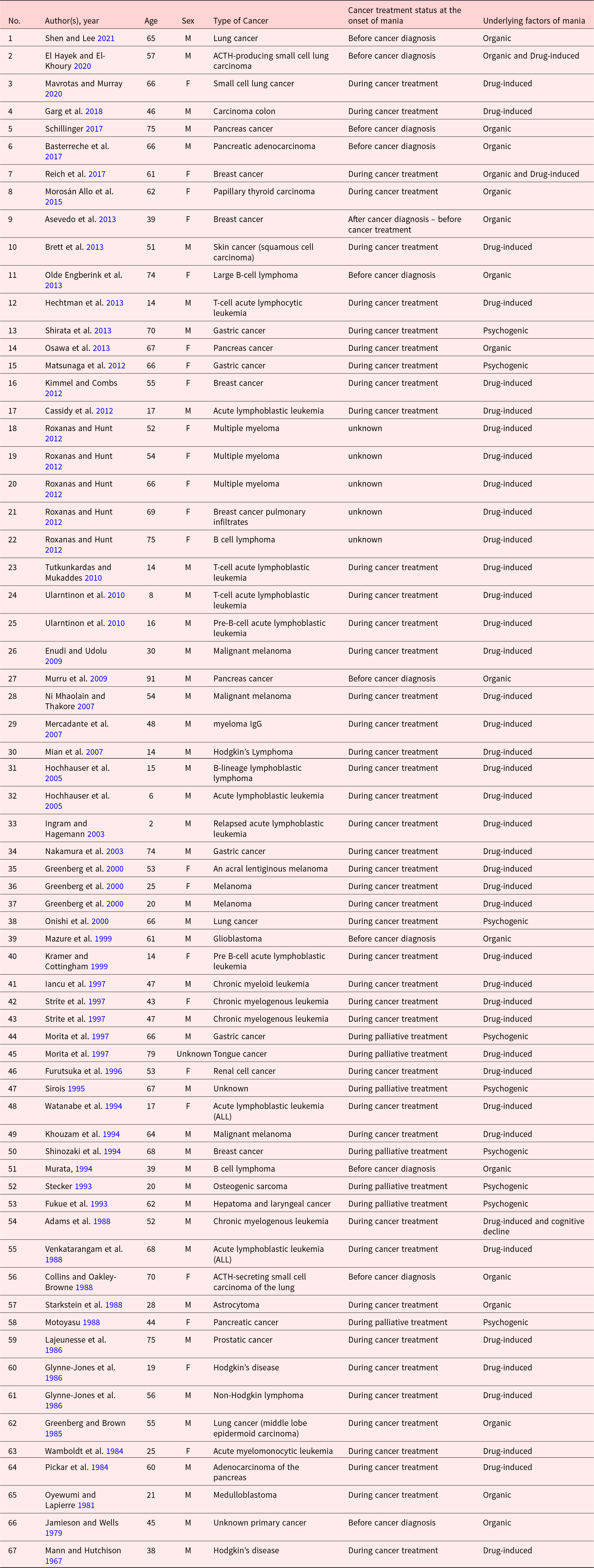
The search finally retrieved 56 papers (9 case series and 47 case reports), which included 67 cases in total (see Table 1).
Summary of reports on cancer patients presenting with manic state

Overview of the cases
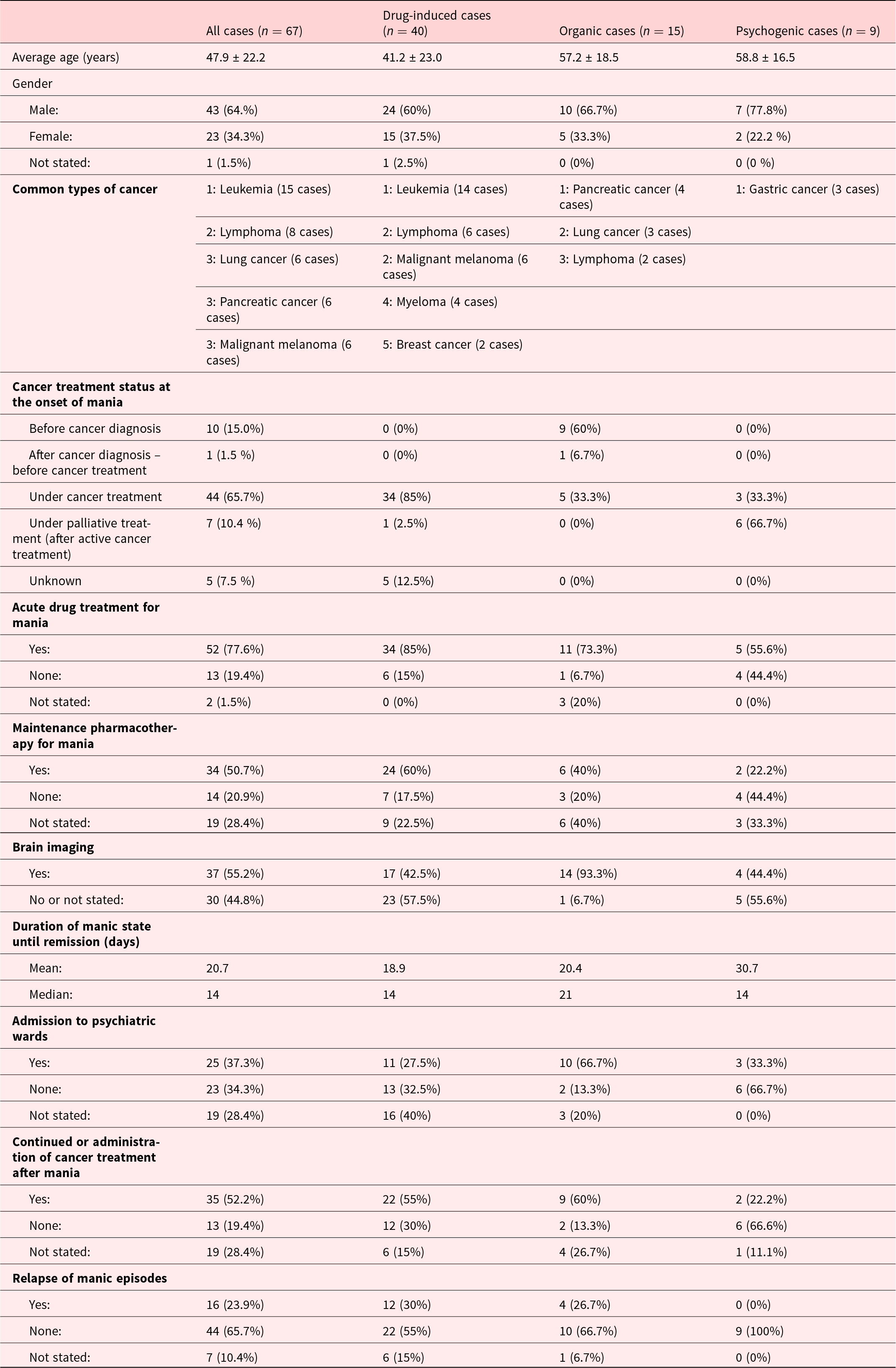
The overview of the 67 cases is shown in Table 2. The mean age of the cases was 47.9 years, with 64% of male patients. The most common cancer was leukemia (15 cases), followed by lymphoma (8 cases), lung cancer, pancreatic cancer, and malignant melanoma (6 cases each).
Manic states in 67 cancer patients

Etiology of manic episodes
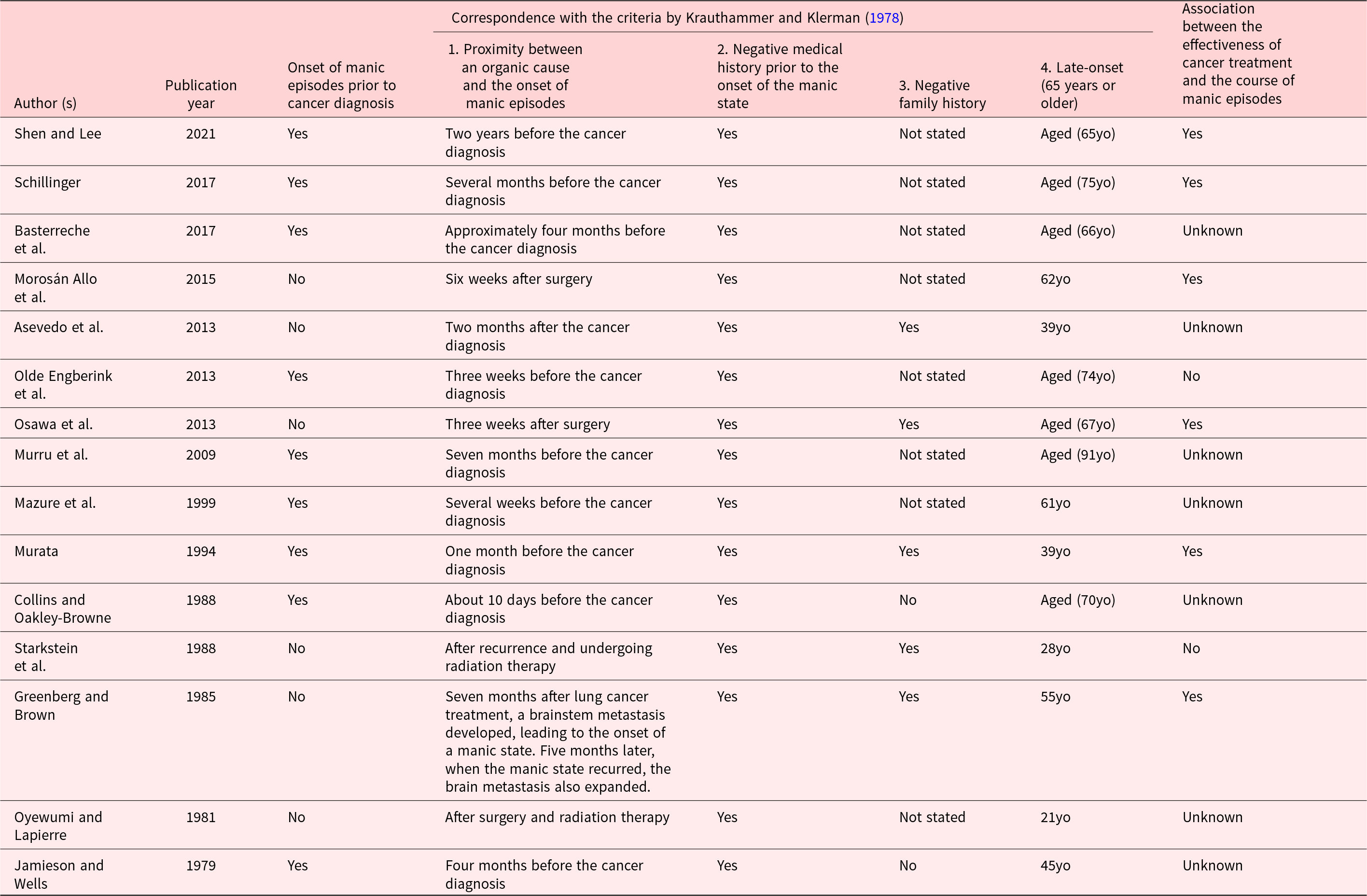
The etiology of manic states was documented in 64 cases, which were classified into organic, drug-induced, and psychogenic. Drug-induced factors were most common (40 cases), followed by organic (15 cases), and psychogenic (9 cases). Three cases were attributed to the overlapping of drug-induced and organic factors. In Table 3, we presented the details of the organic cases.
Details of organic cases

Timing of the onset of manic episodes
Manic states predominantly occurred during cancer treatment (44 cases: 66%), followed by those that occurred before cancer diagnosis (10 cases: 15%). Of the 10 cases that exhibited the onset of manic episodes prior to the diagnosis of cancer, contributing factors for the manic episodes were identified in nine cases.
Clinical management of manic episodes
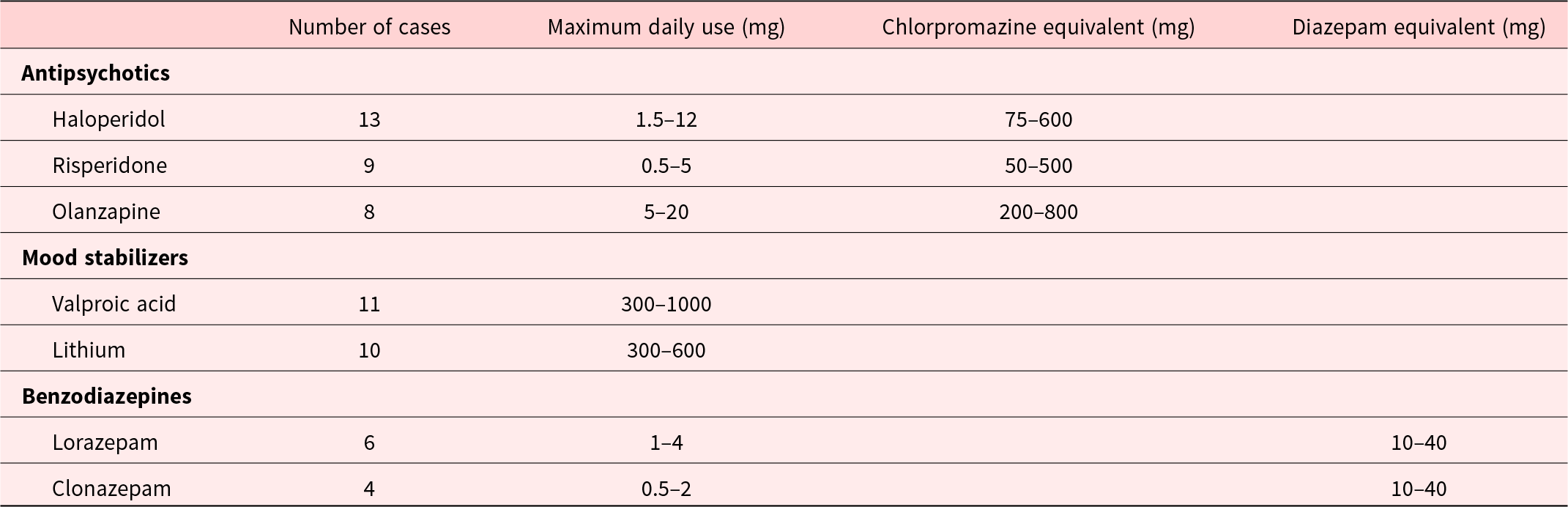
Pharmacotherapy for manic states was administered in 52 cases (78%). Maintenance pharmacotherapy after remission of manic states was administered in 34 cases (51%). The administered pharmacotherapy for manic states is summarized in Table 4. Among the 52 cases where pharmacotherapy was administered, monotherapy with an antipsychotic or a mood stabilizer was most common, comprising 22 cases (40%). Combinations of antipsychotics and mood stabilizers, often accompanied by benzodiazepines, were also common. While benzodiazepines were frequently used for sleep, their daytime administration was also noted. In challenging cases, the first antipsychotic was switched to another or was augmented with other classes of medications.
Medications used to treat manic states

Multiple medications were used in some cases; therefore, the total number of cases in the table outweighs the actual number of cases.
Among the antipsychotics, haloperidol was predominantly used, followed by risperidone and olanzapine. Among mood stabilizers, both valproic acid and lithium were frequently used. In the cases of drug-induced manic states, reducing or discontinuing causative medications such as steroids or interferon while concurrently administering therapeutic agents for the manic state was often observed. The doses of medications were generally comparable to or lower than those used for common mood disorders (Marzani and Neff Reference Marzani and Neff2021).
Brain imaging was conducted in 37 cases (55%).
Clinical course of manic episodes and cancer treatment
The mean and median duration until remission of manic states were 21 and 14 days, respectively. Approximately one third of the cases required hospitalization to psychiatric wards (25 cases: 37%).
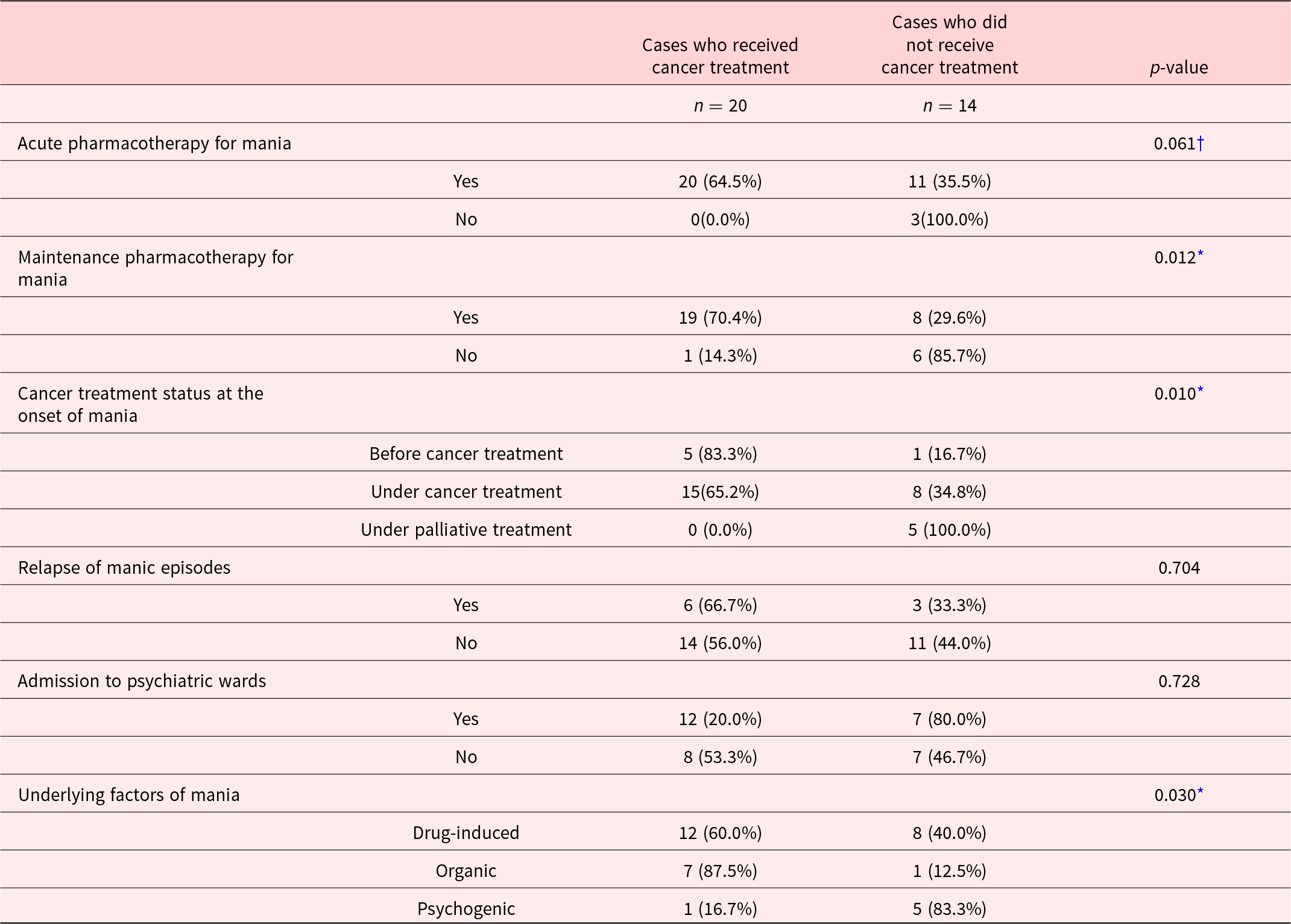
Cancer treatment was continued or initiated after the onset of manic states in 35 cases (52%). In a subset of 34 cases with complete relevant data, administration of maintenance pharmacotherapy, not in the palliative phase, and drug-induced or organic etiologies were significantly associated with continuation of cancer treatment. Administration of pharmacotherapy for acute-phase manic states showed a trend-level association with continued cancer treatment (Table 5). The recurrence of manic states was observed in 16 cases (24%).
Comparison of cases who did and did not receive cancer treatment after a manic state

* P < 0.05, †P < 0.10
Discussion
To the best of the authors’ knowledge, this is the first systematic review that investigated manic states in cancer patients and their influence on cancer treatment.
Clinical characteristics of cancer patients presenting with manic states
The reported cases of cancer patients who developed manic episodes tended to be relatively young, predominantly male, and with hematological malignancies. The manic states most frequently occurred during cancer treatments; however, a substantial proportion of patients (15%) exhibited manic symptoms preceding the cancer diagnosis.
Only half of the cases were able to continue or commence cancer treatment, elucidating the substantial adverse impact of manic episodes on cancer therapy. Nearly 40% required admission to psychiatric wards, indicating the severity of their manic symptoms.
Etiology of manic episodes and their characteristics
Among the three categories of etiology of manic episodes, drug-induced manic states were the most frequent etiology, composing 60% of the cases. Steroid, which has been widely known a causative agent (Ismail et al. Reference Ismail, Lavelle and Cassidy2017), was the most common.
Organic cases were relatively few; however, since brain imaging was not performed in approximately half of the cases, there are chances of overlooked cases.
We compared the clinical characteristics of the three categories. As shown in Table 2, drug-induced cases were relatively young (at 40s), compared with organic and psychogenic cases (late 50s). This can be attributed to the high incidence of leukemia cases in the drug-induced category, which frequently requires high-dose steroids.
A substantial proportion of the patients experienced recurrence of manic episodes in drug-induced and organic cases, while there was no case of recurrence in psychogenic cases. Psychogenic cases were more likely to be seen among patients at the terminal stage, where many patients deceased early in their clinical course.
Timing of the onset of manic episodes and their characteristics
The timing of the onset of manic states varied according to the causative factors: 85% of drug-induced cases occurred during cancer treatment, while many organic cases (60%) presented before the cancer diagnosis, and many psychogenic cases (67%) arose during palliative care.
A substantial proportion (15%) of patients exhibited manic episodes before the diagnosis of cancer. The mean age of onset for mania was 65, which is relatively higher than that of BD in general (Merikangas et al. Reference Merikangas, Jin and He2011; Kroon et al. Reference Kroon, Wohlfarth and Dieleman2013). A few sporadic cases of manic episodes that preceded the diagnosis of pancreatic cancer (Pereira et al. Reference Pereira, Wildenberg and Oliveira2022) have been reported. Sami et al. argued that the first hypomanic episode that occurred after the age of 50 is suggestive of organic factors (Sami et al. Reference Sami, Khan and Nilforooshan2015).
In the current review, we collected the reports in which the authors of the report argued that patients’ manic state was associated with cancer; however, many reports lacked solid evidence to support their arguments. As shown in Table 3, none of the reported cases satisfied the criteria of Krauthammer & Klerman. Further, in their criteria, no specific threshold has been proposed regarding the proximity between an organic cause and the onset of manic episodes.
It has long been known that depressive episodes can precede a diagnosis of cancer, which is known as “premonitory depression” (Lauter Reference Lauter1973). In terms of manic episodes, evidence does not appear sufficient to support a clinical entity of concept of “premonitory mania,” despite there are sporadic reports of manic episodes that precede a cancer diagnosis. Further investigation into the possibility of the concept of “premonitory mania” is warranted.
Clinical management of manic episodes
According to the practice guidelines for BD, pharmacotherapy is the standard approach for manic states (Tajika et al. Reference Tajika, Hori and Iga2022). Significant relief of manic symptoms is usually seen within two weeks (Li et al. Reference Li, Lin and Lu2017). Given the high relapse rate of BD (Keller et al. Reference Keller, Lavori and Coryell1993), maintenance pharmacotherapy is recommended after remission of manic episodes (Kishi et al. Reference Kishi, Ikuta and Matsuda2022). However, in the current review, approximately 20% of the cases with manic episodes did not receive pharmacotherapy, and approximately half of the patients did not receive maintenance pharmacotherapy. The high rate of disrupted cancer therapy may be partly explained by the low rate of administering pharmacotherapy for the acute and maintenance phases of BD. No significant adverse effects have been reported in the use of mood stabilizers and/or antipsychotics in treating manic episodes. There was variability in the dosages of mood stabilizers, and even small doses were effective in many cases. Considering that the median duration to remission of manic states was as short as 14 days even in cancer patients, increasing the awareness of manic states could lead to better management that lead to better cancer treatment.
The current study revealed that brain imaging was conducted in only 55% of the cases. Since central nervous system (CNS) involvement of cancer, such as brain metastases and leptomeningeal metastases, can develop psychiatric symptoms, and the course of manic episodes differs depending on the underlying causes, CNS assessments, such as brain imaging, lumbar puncture, and electroencephalography, are recommended for cancer patients who exhibit psychiatric symptoms.
Clinical course of manic episodes and cancer treatment
After the onset of manic episodes, cancer treatment was provided in 55% of drug-induced cases and 60% of organic cases, but only in 22% of psychogenic cases, suggesting that manic episodes had a significant impact on cancer treatment.
The overall duration until the remission of manic states in drug-induced and organic cases was similar to that of patients in general psychiatric practice (Gonzalez-Pinto et al. Reference Gonzalez-Pinto, Dardennes and de Zélicourt2010). The median duration until the remission of manic states is longer in organic causes than in drug-induced cases, suggesting that organic cases are likely to present with more likely to be treatment-resistant. The duration until remission was relatively long in psychogenic cases, which is attributable to the fact that psychogenic cases occurred in patients in the palliative-care phase, presenting with milder manic symptoms; therefore, no intense psychopharmacological treatment was provided to such patients.
Limitations and implications
The current review has a few limitations. First, this is a narrative review of cancer patients who had manic episodes. The association of manic episodes and cancer relied on the judgment of the reporting authors, and the evidence for the relationship between cancer and manic episodes has not been verified. Second, the classification of contributing factors to the onset of manic episodes (drug-induced, organic, and psychogenic) was based on the argument by the reporting authors. Further, these categories do not match the latest classification of mental illnesses, such as DSM-5 and ICD-11; therefore, the validity of the clinical entity is not established.
Despite these limitations, the current review is worth noting, since, to the best of the authors’ knowledge, it is the first comprehensive review of cancer and manic episodes. Further epidemiological and pathophysiological research is warranted to better understand the linkage between cancer and manic episodes.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951526102466.
Funding
This work was supported by JSPS KAKENHI Grant Number JP23K09528.
Competing interests
The authors declare none.



 Open access
Open access