


Introduction
Suboptimal utilization of antibiotics in healthcare settings is a key, modifiable driver of the 2.8 million antimicrobial-resistant (AMR) infections and 35,000 associated deaths that occur in the United States annually. 1 In 2016, the Joint Commission developed standards requiring hospitals to implement antimicrobial stewardship programs (ASPs). 2 The COVID-19 pandemic was an unprecedented stress test for ASPs in all healthcare settings and significantly accelerated the overuse of antibiotics for viral acute respiratory infections. Reference Pulia, Wolf, Schulz, Pop-Vicas, Schwei and Lindenauer3–Reference Pulia, Griffin and Schwei8 Unfortunately, ASP efforts were often deprioritized during the pandemic. Reference Mendelson, Sharland and Mpundu9,Reference Campbell, Borek and McLeod10
With the re-emergence of Mpox, Marburg, and avian influenza Reference Sidik11–13 local pandemics continue to present a significant future risk to routine ASP operations. By studying how ASPs responded during the COVID-19 pandemic, we can be better prepared to maintain essential components in times of operational stress. Therefore, guided by the Systems Engineering Initiative for Patient Safety (SEIPS), a systems engineering framework designed to evaluate healthcare work systems, Reference Carayon, Hundt and Karsh14 we characterized multi-level systems challenges to and strategies for resilient, hospital-based antimicrobial stewardship (AMS) during the COVID-19 pandemic.
Methods
Sampling
We conducted semi-structured interviews with physicians, pharmacists and quality leaders involved with ASPs from hospital systems across the United States. We identified hospitals for recruitment using the Premier Healthcare Database, a deidentified database of approximately 25% of annual inpatient admissions in the United States. 15 To be eligible, hospitals must have experienced a significant COVID-19 burden, and participants must have worked at the hospital during the COVID-19 pandemic (March 2020 to May 2023). To define COVID-19 burden, we determined the proportion of non-elective admissions with a COVID-19 diagnosis code (U07.1) and ranked hospitals. Eligible hospitals needed to be in the top 50% of COVID-19 burden.
Once eligible hospitals were identified, a Member Engagement and Recruitment Specialist at Premier connected us with ASP pharmacists and Infectious Diseases (ID) physicians and we confirmed eligibility via email. To ensure perspectives from sites outside of the Premier network, additional national leaders in ASP were recruited by the senior author (MSP) via direct email. We selected participants by purposeful criterion sampling to ensure we had representation based on roles (pharmacist vs physician); geographic region, and years of experience. Reference Palinkas, Horwitz, Green, Wisdom, Duan and Hoagwood16 Interviews and analysis occurred from January 2023-September 2024. The institutional review board approved all study activities. We followed the consolidated criteria for reporting qualitative studies (checklist in supplementary material). Reference Tong, Sainsbury and Craig17 All participants received a financial incentive following the interview.
Design and procedure
We conducted semi-structured interviews to explore broad themes around challenges to and strategies for resilient AMS. We defined resilient AMS as the ability of an ASP to anticipate, absorb, adapt to, and recover from disruptions while continuing to function effectively. Interview questions were primarily open ended so participants could respond freely. Follow up questions were based on elements of the SEIPS framework (interview guide in supplementary material). SEIPS is a systems engineering framework that conceptualizes healthcare delivery as a sociotechnical system, incorporating interactions among people, tasks, tools and technologies, organizational factors, and the physical environment to evaluate care processes and outcomes. Reference Carayon, Hundt and Karsh14
A non-clinical, female study team member with 10 years of qualitative research experience (RJS) conducted the virtual video interviews in a private room. The principal investigator, a male emergency medicine (EM) physician with advanced training in systems engineering and qualitative methods (MSP), attended the first five interviews to observe, ask clarifying questions and refine the interview guide. Other female members of the research team with varying levels of experience (HI, MG, SS, AK) sat in on the interviews as notetakers and to ask clarifying questions. We refined the interview guide after three pilot interviews and continued to make minor adjustments as interviews progressed.
All interviews were audio recorded, professionally transcribed verbatim and reviewed for accuracy. We collected demographic (sex, role, board certifications, years of experience, tenure at current site) and geographic region (Northeast, South, Midwest, West) variables. Sampling, data collection, and data analysis occurred concurrently and data collection was stopped when responses became redundant and probes failed to uncover new themes (i.e. conceptual saturation). Reference Bowen18
Analysis
We used deductive directed content analysis guided by the SEIPS model. Reference Hsieh and Shannon19 The study team developed a preliminary codebook based on post interview memos, interview question domains and elements in the SEIPS model. Reference Saldana20 RJS coded all interviews and one additional study team member (HI, MG, AK, SS) independently coded each interview such that two study team members coded each interview. Coders met to review codes, add new codes and refine code definitions (codebook in supplementary material). As coding progressed, we grouped similar concepts into overarching themes. Discrepancies were resolved by discussion and consensus. Reference Barry, Britten, Barber, Bradley and Stevenson21 We used Dedoose software to organize coding. 22
Results
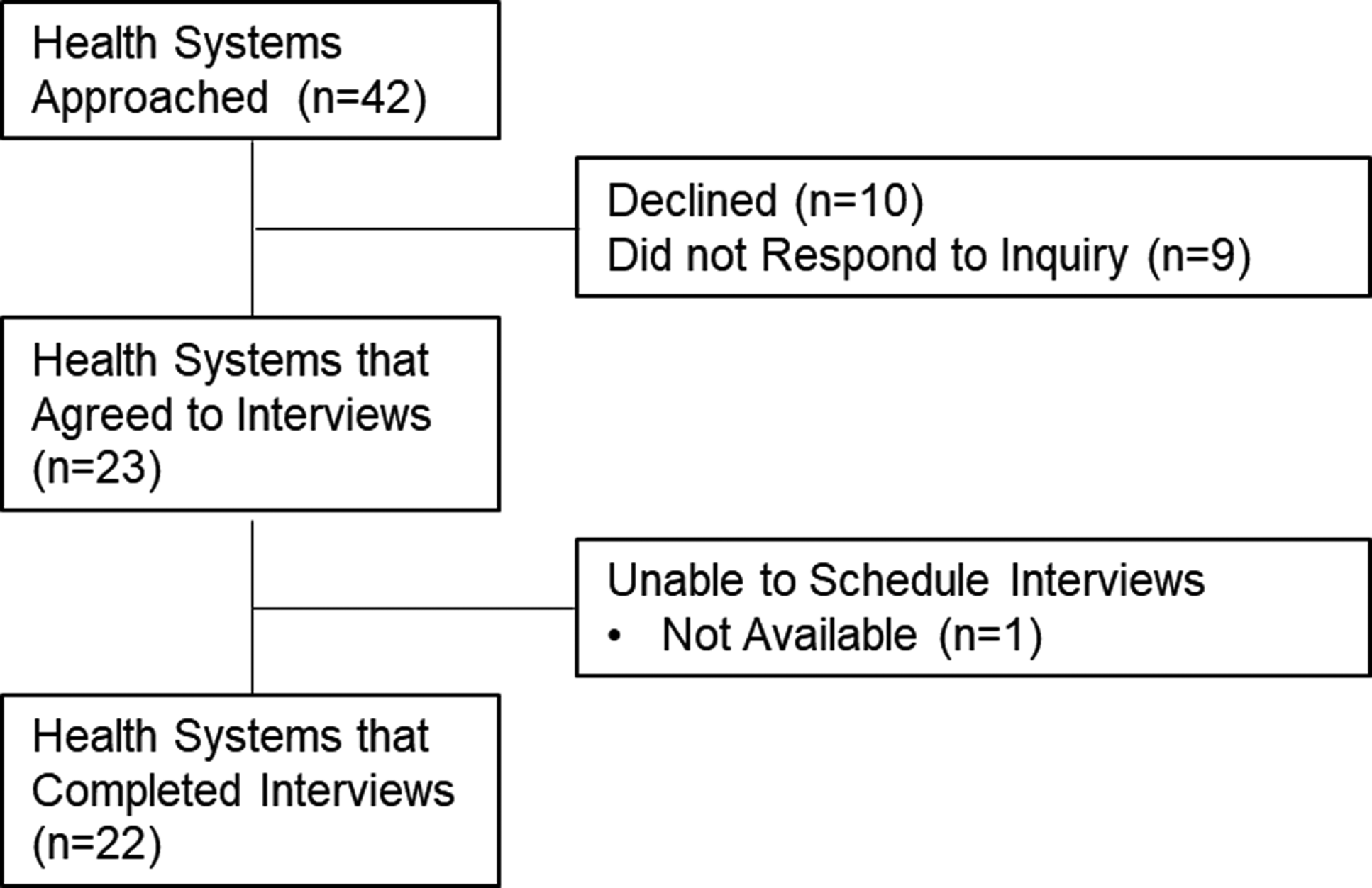
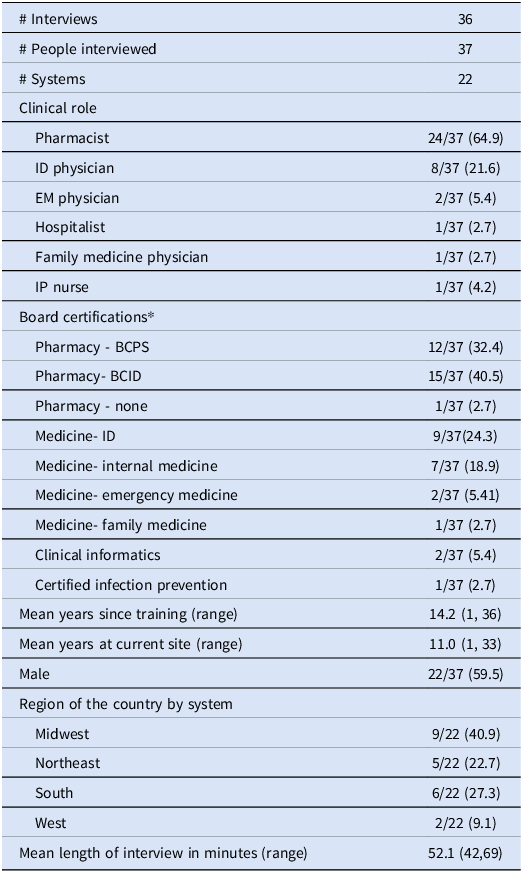
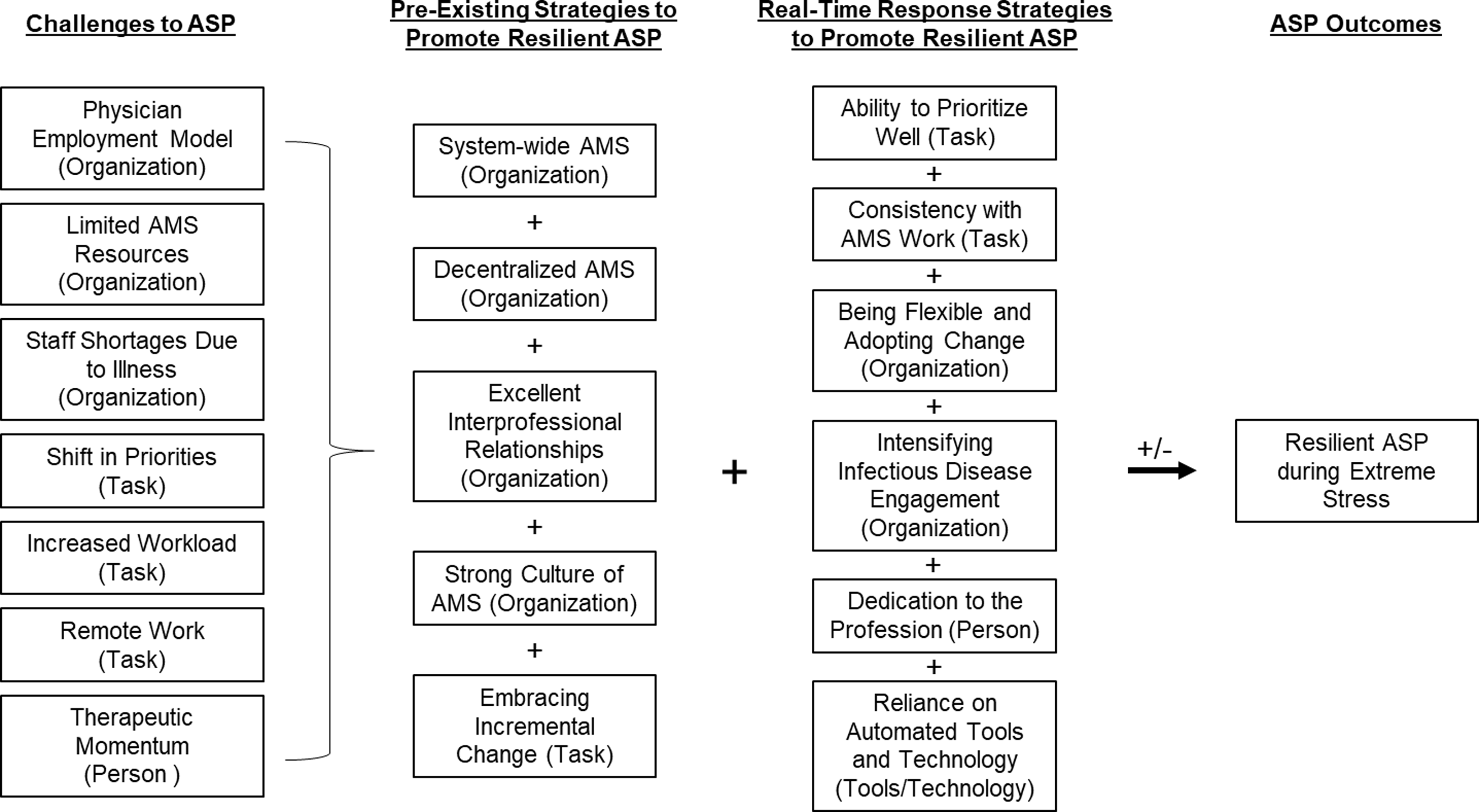
We completed 36 interviews with 37 participants from 22 different healthcare systems (Figure 1). Table 1 describes participant sex, clinical role and the region of the country. Figure 2 is a diagram of the challenges and strategies to ASP resilience presented in the following results sections.
Flow diagram of recruitment.

Demographic and interview characteristics of interviews, n(%)

*Some participants are represented in more than one category. BCID, board certification in infectious diseases pharmacy; BCPS, board certified pharmacy specialist; ID, infectious diseases; EM, emergency medicine; IP, infection prevention.
Description of challenges to antimicrobial stewardship programs that arose during COVID-19 pandemic and how pre-existing and real-time strategies were used to promote resiliency in ASP during the COVID-19 pandemic. SEIPS work system elements are in parenthesis behind each challenge or strategy. Abbreviations: AMS, antimicrobial stewardship; ASP, antimicrobial stewardship program.

Challenges to ASP during the COVID-19 pandemic
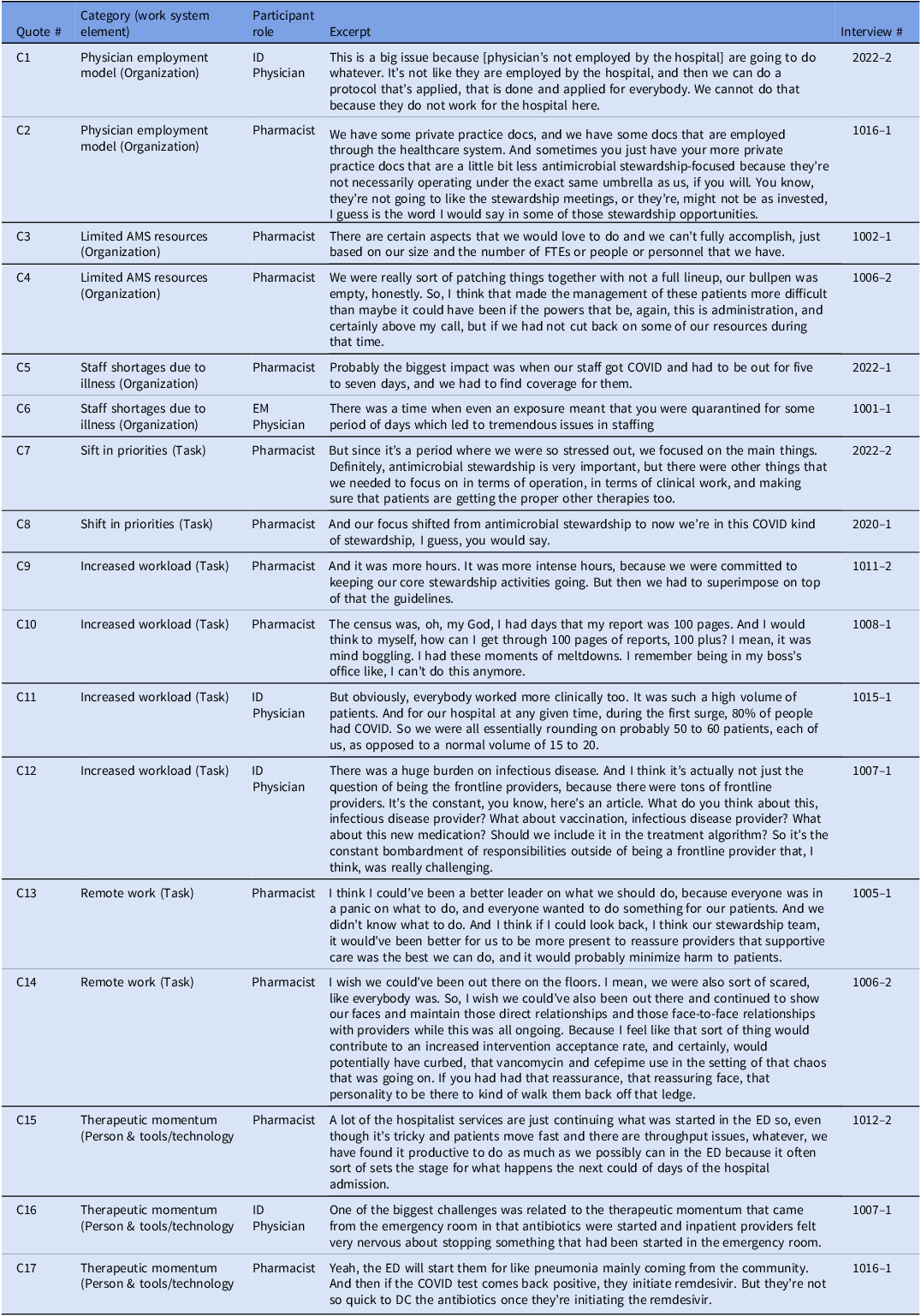
Representative quotes for challenges to ASP during the pandemic are numbered C1 through C17 (Table 2).
Challenges to resilient antimicrobial stewardship programs during the COVID-19 pandemic and representative quotes

Physician employment model (organization)
Physician employment model was defined as instances when physician employment (i.e. hospital employees vs private practice) impacted AMS work. C1 described how private practice physicians employed by their system made it challenging to implement an AMS protocol for all employees. In C2, a pharmacist described how private practice physicians are not as invested in AMS because they are not under the umbrella of the hospital.
Limited AMS resources (organization)
This included baseline limitations and limitations of resources during COVID-19. In C3, a pharmacist described how prior to the pandemic they could not do everything that they would like due to the size of their ASP. Furthermore, one pharmacist described how their ASP resources were cut during the pandemic (C4).
Staff shortages due to illness (organization)
Staff shortages due to illness or exposure were organizational challenges that arose during the COVID-19 pandemic. A reduced number of staff made it difficult to maintain AMS activities during the pandemic (C5, C6).
Shift in priorities (task)
Participants described shifting their priorities due to the COVID-19 pandemic. For example, in C7, one pharmacist acknowledged that AMS is important, but during a pandemic there were more important things to focus on such as ensuring patients received proper COVID-19 therapies. Likewise, in C8, one pharmacist described how her role changed from AMS to COVID-19 stewardship.
Increased workload (task)
This was a major challenge to maintaining AMS work. C9 described how in addition to their normal work, ID pharmacists were tasked with developing COVID-19 guidelines. Participants described how a high hospital census made it difficult to keep up with routine AMS work for pharmacists (C10) and physicians (C11). Finally, in C12, one ID physician described how in addition to being a frontline provider, ID physicians were expected to be available for frequent, informal consultations about patients, vaccines and treatments.
Remote work (task)
Pharmacists felt that antibiotics were overutilized during the pandemic was in part because AMS staff were required to work remotely. In C13, the pharmacist wished that he had been a stronger advocate which would have been easier had he been physically present. Likewise, in C14 another pharmacist described how being physically present may have led to increased intervention acceptance rates.
Therapeutic momentum (person)
Therapeutic momentum was defined as scenarios where it was hard to stop antibiotics once they were initiated. C15 and C16 described how it is hard for AMS pharmacists to stop antibiotics that are started in the emergency department (ED). The pharmacist in C17 said that even when a positive COVID-19 test resulted, providers would be quick to start COVID-19 therapy but would not stop antibiotics.
Strategies for promoting resilient ASP during the COVID-19 pandemic
Participants described strategies for resilient ASP in two categories, preexisting and real-time response strategies.
Preexisting strategies
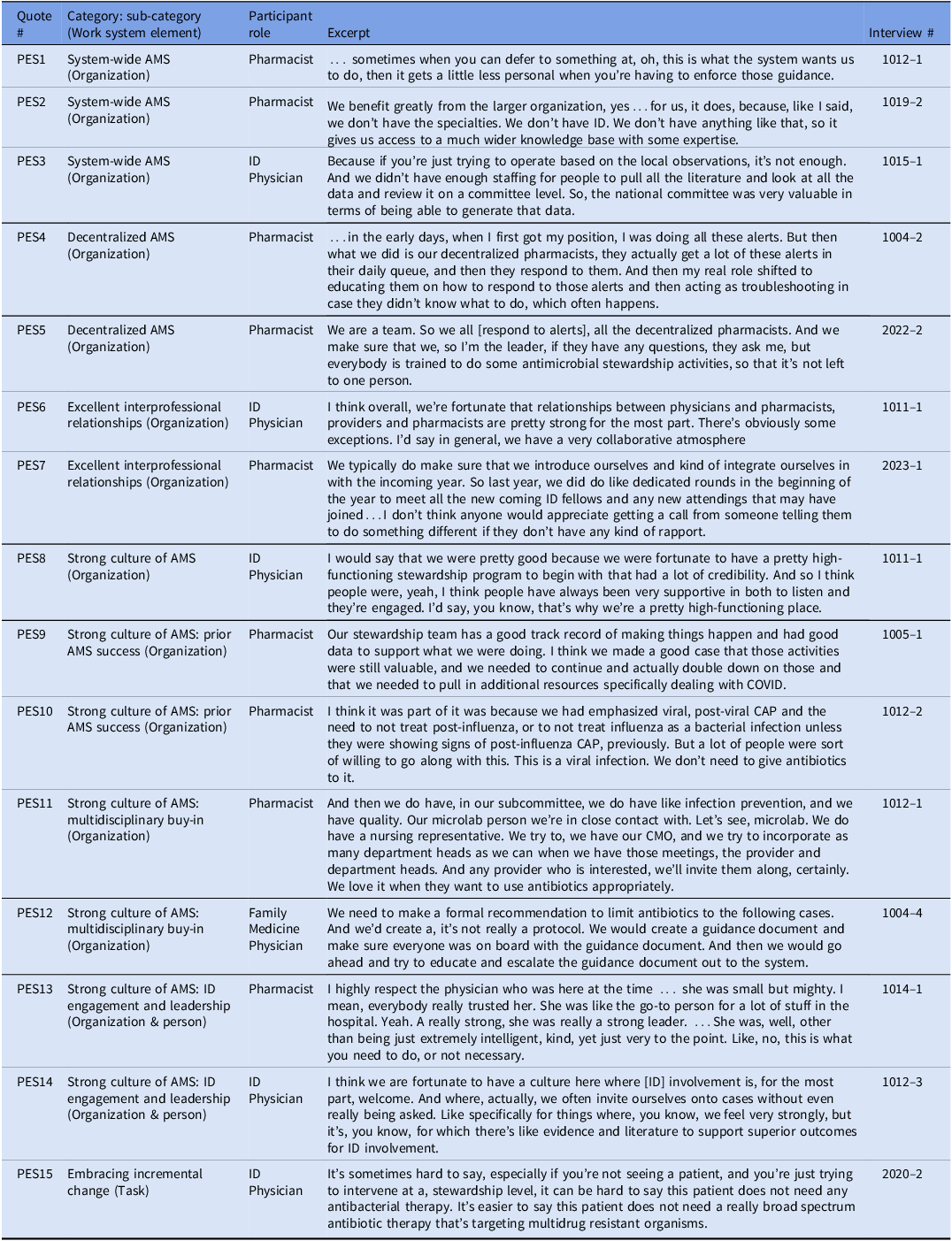
Preexisting strategies were in place prior to the pandemic. Representative quotes are numbered PES1 through PES15 (Table 3).
Pre-existing strategies for resilient antimicrobial stewardship programs during the COVID-19 pandemic and representative quotes

System-wide AMS (organization). We defined system-wide AMS as higher level coordination of AMS that promoted resiliency within hospital-level ASP. In PES1 one pharmacist described how having a system-wide stance on something helps prevent AMS conversations from feeling personal because you can defer to the system decision. Likewise, in PES2, system-wide AMS was helpful because he was from a critical access hospital and they did not have access to ID. Therefore, they relied on the system-wide AMS group to provide ID expertise. In PES3 an ID physician who was part of a national health system described how system wide AMS helped them generate meaningful data during a time of uncertainty.
Decentralized AMS (organization). Decentralized AMS included descriptions of AMS responsibilities being distributed across multiple pharmacists. In PES4, one pharmacist described how her role evolved from more of a centralized AMS model where the ID pharmacist responded to alerts to a decentralized model where the floor pharmacists were responsible for AMS alerts. In PES5 a pharmacist described how the decentralized AMS model works well in their hospital because it ensures AMS activities continue even if the ID pharmacist is out sick.
Excellent interprofessional relationships (organization). Excellent interprofessional relationships included descriptions of how positive working relationships with colleagues promotes AMS. In PES6 one ID physician described how they have a collaborative environment. Likewise, the pharmacist in PES7 described how they introduce themselves to new staff before they reach out about AMS recommendations.
Strong culture of AMS (organization). We defined a strong culture of AMS as descriptions of the hospital or system AMS mindset facilitating AMS work. For example, PES8 described their AMS group as highly functioning with a lot of credibility. Within this category, participants described three subcategories including prior AMS successes, multidisciplinary buy-in and ID engagement and leadership.
Subcategory: Prior AMS success (organization): Participants described how prior AMS success contributed to additional AMS resources and acceptance of COVID-19 treatment recommendations. In PES9, one pharmacist said that because of historically good AMS outcomes, they successfully advocated for additional resources during the pandemic to maintain AMS activities. Likewise, in PES10, the pharmacist described how the AMS program had previously been working on not treating viral infections with antibiotics, and therefore, during the pandemic providers were receptive to not treating COVID-19 infections with antibiotics.
Subcategory: Building multidisciplinary buy-in (organization): Participants talked about the importance of involving a wide variety of disciplines in AMS processes and recommendations. In PES11, one pharmacist described how they invite anyone who is interested to their AMS sub-committee meeting. In PES12, a family medicine physician described how they incorporated multidisciplinary input to their COVID-19 treatment guidance.
Subcategory: ID engagement & leadership (organization and person): ID engagement and leadership contributed to strong AMS culture. In PES13 one pharmacist described how the ID physician at her hospital was a strong leader, and how this set the tone for AMS. PES14 described how the ID group was empowered to consult on cases involving antibiotic stewardship concerns which helps support the pharmacist’s AMS recommendations.
Embracing incremental change (task). We defined embracing incremental change as descriptions of how small gradual changes can make a difference. For example, in PES15, one ID physician described how it can be easier to convince physicians to narrow the spectrum of antibiotics versus discontinue antibiotics entirely.
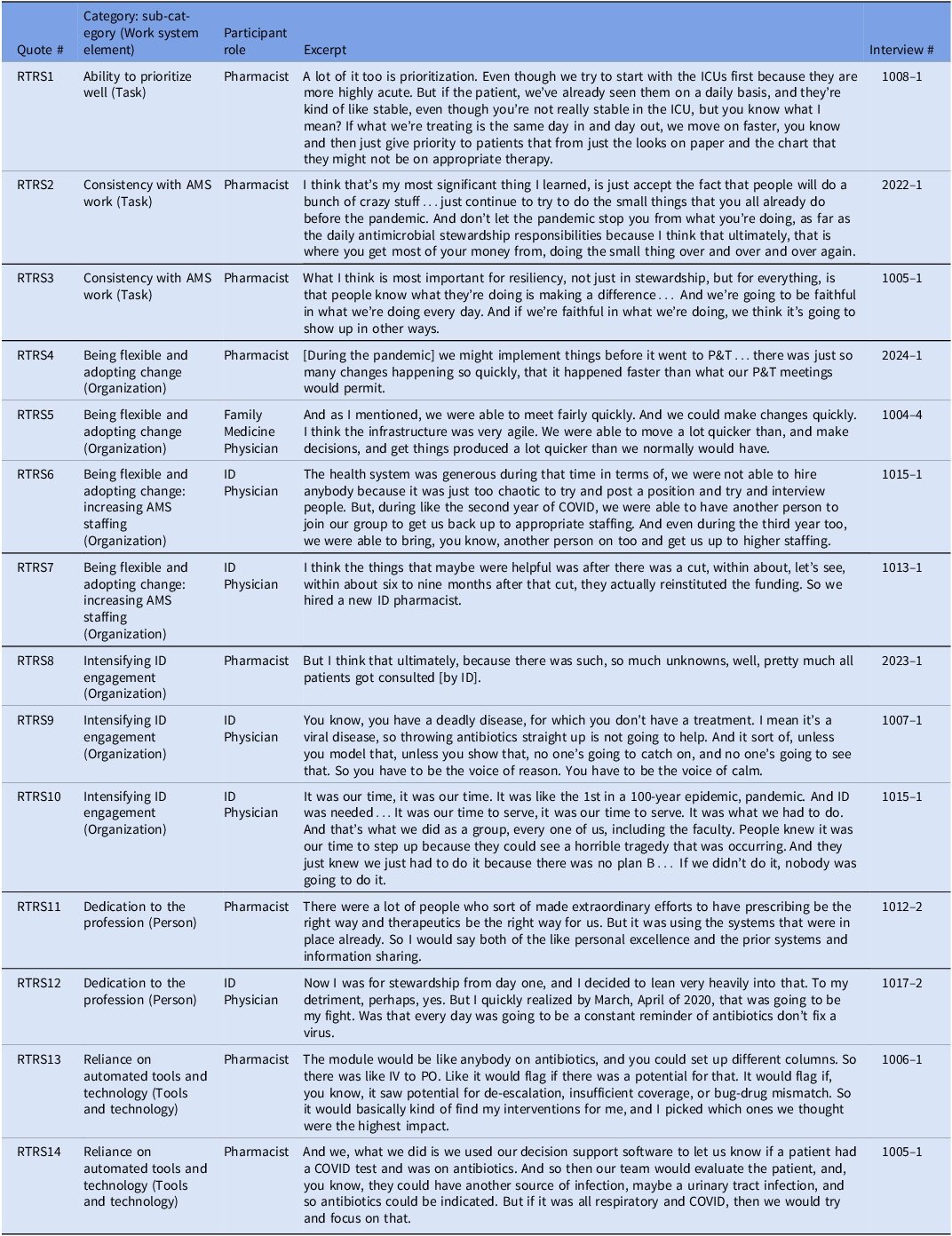
Real-time response strategies. Real-time response strategies (RTRS) were implemented during the COVID-19 pandemic and promoted ASP resiliency. Representative quotes are numbered RTRS1 through RTRS14 (Table 4).
Real-time response strategies for resilient antimicrobial stewardship programs during the COVID-19 pandemic and representative quotes

Ability to prioritize well (task). Ability to prioritize well captured how participants changed day-to-day work due to staff shortages and increased workload during the COVID-19 pandemic. For example, in RTRS1 a pharmacist described prioritizing higher impact aspects of antibiotic appropriateness review during the pandemic.
Consistency with AMS work (task). We defined consistency with AMS work as descriptions of how doing daily AMS tasks leads to improvements and resiliency. In RTRS2 and RTRS3 pharmacists described how even during a pandemic when things were chaotic, it was still important to maintain daily AMS activities.
Being flexible and adopting change (organization). Being flexible and adopting change included when institutions implemented new workflows or described the value of adopting organizational changes during the pandemic. In RTRS4, one pharmacist described how during the COVID-19 pandemic they were allowed to bypass the pharmacy and therapeutics committee approval to rapidly respond. Likewise, in RTRS5 a family medicine physician described how they made decisions and implemented workflows more quickly during the pandemic. Within this category, participants also described a subcategory: increasing AMS staffing to respond to the COVID-19 pandemic
Subcategory: Increasing AMS Staffing (Organization): This strategy allowed ASP to absorb additional responsibilities. In RTRS6 one ID physician described how their health system allocated more people to the ID team because they were the group with the increased workload. Likewise, in RTRS7, an ID physician described how although at the beginning of the pandemic an ID pharmacist position was cut, after about 6 months they were given more staffing resources.
Intensifying ID engagement (organization). Another strategy participants described that promoted ASP resiliency was intensifying ID engagement. In RTRS8 one pharmacist described how due to the uncertainty around COVID-19, most patients received an ID consultation. Likewise, in RTRS9, one ID physician described how they viewed it as their role to be the ‘voice of reason’ and to help other providers understand that it was not appropriate to use antibiotics in a viral infection. Finally, in RTRS10 another ID physician described how because this was a pandemic, ID needed to step up and use their expertise for the greater good.
Dedication to the profession (person).We labeled something as dedication to the profession when participants described going above and beyond their normal duties because of an internal dedication to ID work. In RTRS11, one pharmacist described how throughout the hospital many ID professionals made extraordinary efforts in response to the COVID-19 pandemic. Likewise, in RTRS12, one ID physician described how he made a conscious decision to focus on AMS during the COVID-19 pandemic.
Reliance on automated tools and technology (tools and technology). Throughout the interviews, participants described relying heavily on automated tools during the COVID-19 pandemic. In RTRS13, one pharmacist described how they used an automated program during the pandemic to identify high priority AMS interventions. Likewise, in RTRS14, another pharmacist described how they had a decision support tool built for COVID-19 specifically to help their ASP.
Discussion
Using a systems engineering framework informed qualitative approach, we characterized work system challenges to and strategies for resiliency among ASPs during the COVID-19 pandemic. The SEIPS model allowed us to consider both the hospital and ASP work systems so that we could identify challenges and strategies that extend beyond the patient and the provider.
Participants identified a variety of challenges to AMS resiliency during the COVID-19 pandemic. Three of the challenges, physician employment model, limited resources and therapeutic momentum, were challenges to ASP prior to the pandemic and continued to negatively impact ASP work during the pandemic. The other challenges, staff shortages due to illness, shift in priorities, increased workload and remote work, were new challenges that arose during the pandemic. Interestingly, the challenges to ASPs identified in this study were modifiable, suggesting they could be overcome by implementing the strategies described in this and other studies. Reference Chen, Hoang and Yaskina23–Reference Pierce and Stevens29
In future pandemics, it is critically important to maintain AMS activities. We hypothesize that the deprioritization of AMS activities, which was reported in this study as well as in prior work, Reference Mendelson, Sharland and Mpundu9,Reference Campbell, Borek and McLeod10,Reference Hashad, Stewart, Perumal, Abdulrazzaq and Tonna30,Reference Abdelsalam Elshenawy, Umaru and Aslanpour31 contributed to the overuse of antibiotics for viral acute respiratory infections Reference Pulia, Wolf, Schulz, Pop-Vicas, Schwei and Lindenauer3–Reference Pulia, Griffin and Schwei8 and the subsequent increase in bacterial antimicrobial resistant hospital-onset infections. Reference Witt, Howard-Anderson, Jacob and Gottlieb32,33 Prior work has highlighted how routine AMS activities such as prospective audit and feedback contributed to lower antibiotic use compared to usual care during the COVID-19 pandemic. Reference Chen, Hoang and Yaskina23,Reference Mbamalu, Surendran and Nampoothiri34 ASP and ID professionals are needed to support appropriate use of antibiotics, and their role may be even more essential during a pandemic where high levels of stress may contribute to increases in inappropriate use of antibiotics.
It is in the best interest of health systems to incorporate lessons learned from COVID-19 to enhance preparedness and enable a proactive response. Reference Cunningham and Hopkins25,Reference Williams, Jones, Welch and True35 Re-emerging infectious diseases such as Mpox, Marburg, and avian influenza highlight the threat of a future pandemic. Reference Sidik11–13 For ASPs, the preexisting strategies identified in this study included system-wide AMS, decentralized AMS, excellent interprofessional relationships, strong AMS culture and embracing incremental change. Four of these strategies are within the organization domain of the SEIPS model suggesting that the behavior of antibiotic prescribing is impacted by more than the patient and provider beliefs and attitudes. Reference Cosgrove, Ahn, Dullabh, Gordon, Miller and Tamma26,Reference Charani, Edwards and Sevdalis36–Reference Parker, Frost and Day39
Participants identified real-time response strategies that allowed their ASP to function effectively during the pandemic. Intensifying ID engagement, prioritization and consistency of AMS work, and reliance on automated tools and technology were strategies participants utilized in response to limitations on resources such as personnel and time. These findings are supported by prior work which has suggested that additional AMS resources and enhanced utilization of tools and technology are helpful during pandemics to mitigate increased workload. Reference Heil, Justo and Bork24,Reference Hashad, Stewart, Perumal, Abdulrazzaq and Tonna30,Reference Martin, Philbin, Hughes, Bergin and Talento40–Reference Davis, McManus and Koff42
Another important finding from this study was how personal dedication of the ID professionals throughout the pandemic contributed to ASP resiliency. This is an important finding for future periods of stress because healthcare leaders need to do a better job of recognizing the extraordinary efforts of individuals in real-time, providing resources and compensation to ensure this essential work is completed. Reference Billings, Ching, Gkofa, Greene and Bloomfield43
The study results should be considered in the context of the study’s limitations. The first limitation to consider is selection bias both because the recruitment strategy was opt-in, and because our sampling frame only recruited staff from hospitals with significant COVID-19 burden. Second, due to elapsed time since the start of the pandemic, the fluidity of recommendations during the pandemic and the traumatic nature of the pandemic, participants’ memories were not always clear on how certain events transpired.
Using a systems engineering informed qualitative approach, we characterized work system challenges to and strategies for resiliency during the COVID-19 pandemic specific to the ASP work system. Participants identified challenges to AMS resiliency, many of which were modifiable and could be addressed in future pandemics. Healthcare system leadership should utilize the identified preexisting and real-time response strategies as a roadmap to ASP preparedness and an effective, proactive response to future instances of operational stress.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ice.2026.10415.
Acknowledgments
We appreciate all of participants who took time out of their busy schedules to meet with us for this project. This work would not have been possible without their efforts. MSP received grant support from the Agency for Healthcare Research and quality grant R01 HS028669 and the Clinical and Translational Science Award (CTSA) program, through the NIH National Center for Advancing Translational Sciences (NCATS), grant UL1TR002373.
Competing interests
RJS, HI, MG, NW, APV, AK, SS, and MSP have no conflicts of interest to report. LS is employed by Cepheid.



 Open access
Open access