


Introduction
Heart disease and cancer are among the leading causes of death world-wide. 1 In Europe, cardiovascular disease (CVD) was responsible for 1.7 million deaths in 2021. Reference Luengo-Fernandez, Walli-Attaei and Gray2 In this context, it is crucial for health care professionals to be prepared to perform cardiopulmonary resuscitation (CPR) on patients with CVD. The American Heart Association (AHA; Dallas, Texas USA) defined CPR as a combination of chest compression and artificial ventilation to maintain circulation and oxygenation. Reference Merchant, Topjian and Panchal3 During the last decades, advances in resuscitation science led to the development of effective CPR protocols, increasing survival from cardiac arrest. Reference Nolan, Soar and Smith4 Prompt initiation of CPR is essential to maintain and restore function to the heart and brain. Reference Perkins, Handley and Koster5 Maintaining CPR knowledge and skills are crucial for health care professionals to respond promptly and effectively to patients experiencing cardiopulmonary arrest. The AHA states that knowledge retention tends to decline more slowly than practical skills. Reference Merchant, Topjian and Panchal3
Education and training in CPR increase the knowledge and competence of health care professionals. Nurses are usually the first responders after cardiac arrest in health care settings, and competence in CPR is the cornerstone of resuscitation. Reference García-Suárez, Méndez-Martínez, Martínez-Isasi, Gómez-Salgado and Fernández-García6 Therefore, it would be beneficial for nursing students to have adequate knowledge in CPR to enhance their skills for future application. Reference Madden7 Research indicates that nursing and medical students’ skills are reported to be poor and they require better CPR knowledge. Reference Baldi, Contri and Bailoni8,Reference Mäkinen, Axelsson, Castrén, Nurmi, Lankinen and Niemi-Murola9 To address this, the European Resuscitation Council (ERC; Niel, Belgium) has issued a guidance note aimed at enhancing CPR training for health care students. Reference Baldi, Savastano and Contri10 Studies highlight the benefits of incorporating innovative training approaches, and researchers recommend exploring new and alternative methods to improve CPR knowledge and skills among this group. Reference Pour, Aliyari, Farsi and Ghelich11 Since 2015, the AHA has recommended the use of high-fidelity manikins, simulators, and online training courses as tools for CPR education and training. Reference Bhanji, Donoghue and Wolff12 Manikin-based simulation training has proven effective for educating nursing and medical students. It enables learners to actively participate in their education and practice patient care within a controlled and safe setting. Reference McCoy, Rahman and Rendon13
Previous research has shown that knowledge and skills acquired through CPR training may decline over time. A study evaluating the long-term effects of CPR education based on theoretical lectures and training found a significant decline in knowledge after three months, highlighting the importance of on-going education and training. Reference Partiprajak and Thongpo14 Researchers have started exploring alternative teaching and learning methods, such as self-instructional videos, to support the development of resuscitation skills. Reference Lynch, Einspruch, Nichol, Becker, Aufderheide and Idris15 Several studies have demonstrated that CPR e-learning has proven effective in teaching knowledge and techniques, and, in some cases, has been reported to be more effective than instructor-led CPR education in enhancing knowledge and performance. Reference Mundell, Kennedy, Szostek and Cook16–Reference Tobase, Peres, Gianotto-Oliveira, Smith, Polastri and Timerman18 However, other studies have reported comparable outcomes between e-learning and face-to-face education. Reference Lynch, Einspruch, Nichol, Becker, Aufderheide and Idris15,Reference Horiuchi, Yaju, Koyo, Sakyo and Nakayama19 These differences in findings may be attributed to variations in study design, learner populations, the degree of interactivity in the digital platforms used, and whether e-learning was implemented as a standalone method or as part of a blended learning approach.
Despite numerous studies on Basic Life Support (BLS)/automated external defibrillation (AED) knowledge retention, several gaps remain. Most research has focused on initial CPR training, with relatively few studies examining the effectiveness of post-qualification refresher training for nursing students, a critical period when knowledge and skills may decline. Additionally, while e-learning and face-to-face methods have both been shown to improve knowledge, previous findings are inconsistent, particularly regarding long-term retention and skill performance. Moreover, few studies have directly compared these educational approaches in the same cohort of nursing students, assessing both knowledge and practical competence over time. By addressing these gaps, the present study aims to provide evidence on which training modality is most effective in sustaining CPR competence and to inform strategies for integrating refresher training into nursing curricula.
Thus, this study aims to examine whether: (1) CPR post-qualification training is needed in maintaining knowledge and skills, and (2) face-to-face or video-based online training is more effective as an educational method in preserving CPR knowledge and skills in nursing students. While the primary focus of the study is to evaluate CPR knowledge and skill retention following different educational interventions, positioned within Level 2 (learning) of the Kirkpatrick model, the study was also designed with the broader goal of informing future impacts at Levels 3 (behavior) and Level 4 (results). In this context, behavioral change refers to the consistent and correct application of CPR procedures in real clinical situations, including the timely recognition of cardiac arrest, initiation of high-quality chest compressions, and adherence to resuscitation guidelines. By examining which educational approach better supports the retention of CPR competence over time, the findings may help identify training strategies that are more likely to translate into improved performance in clinical practice (Level 3), particularly among nurses who are frequently the first responders to in-hospital cardiac arrest.
Furthermore, embedding effective CPR training methods into nursing education has the potential to enhance organizational preparedness and, ultimately, contribute to improved patient outcomes (Level 4), including increased survival rates from cardiopulmonary arrest. The structured design of the study and the inclusion of both traditional and e-learning approaches also enhance the generalizability of the findings to a wide-range of educational and clinical settings, making them relevant for curriculum planners, clinical educators, and health care systems aiming to strengthen resuscitation readiness. It was hypothesized that first, nursing students who receive post-qualification CPR training will demonstrate significantly better retention of CPR knowledge and skills compared to those who do not receive additional training, and second, the retention of knowledge and skills related to CPR would be significantly improved in the face-to-face or the e-learning group.
Methods
Study Design and Setting
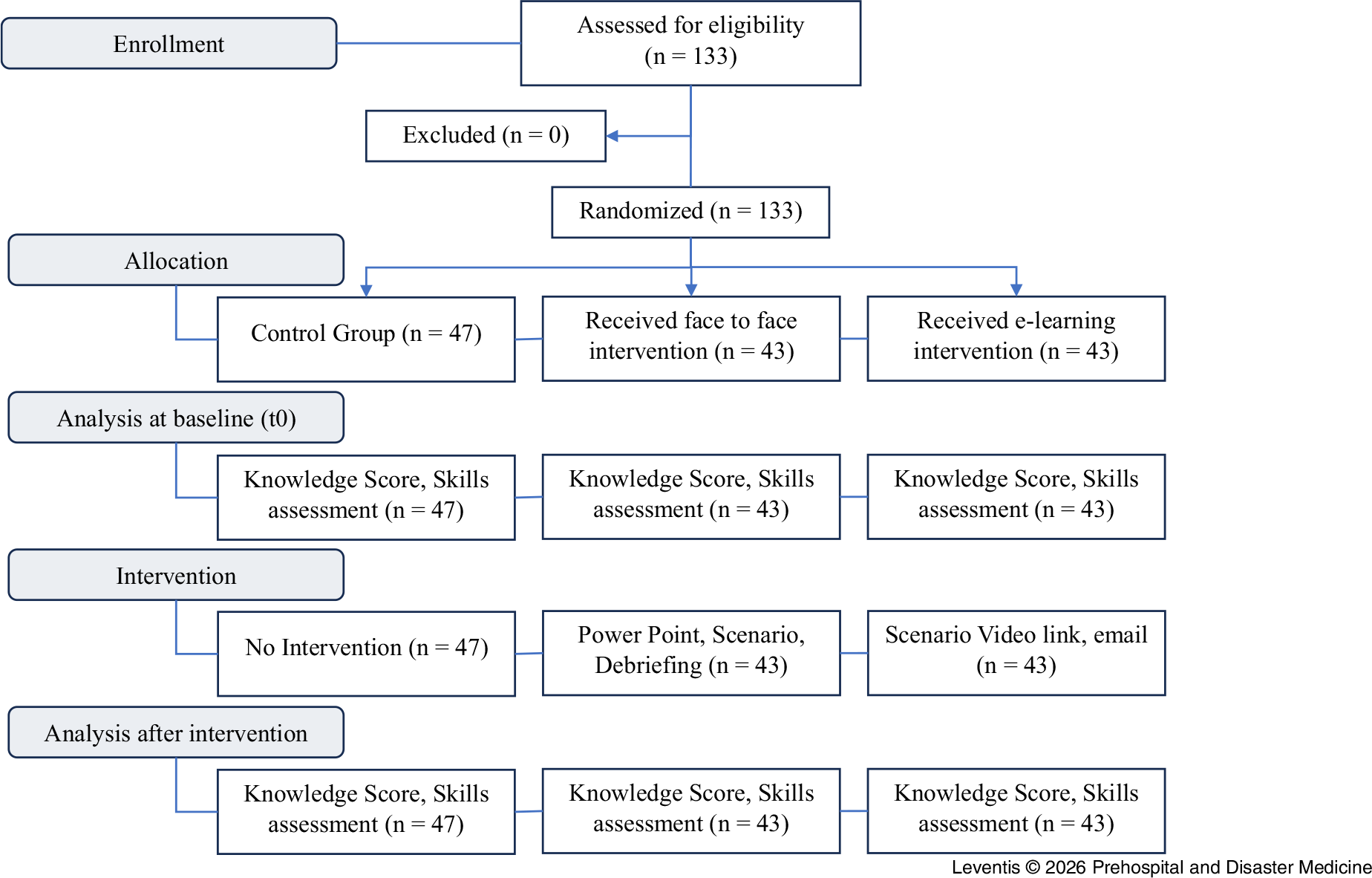
This study was conducted from December 2022 through December 2023 at the Department of Nursing of School of Health Rehabilitation Sciences, University of Patras (Greece), in the Nursing Simulation Laboratory. It utilized a three-group, parallel randomized-controlled, single-blind design and followed the CONSORT guidelines for the reporting of randomized controlled trials (Figure 1).
CONSORT Flow Diagram of the Present Randomized Controlled Trial.
Note: CONSORT = Consolidated Standards of Reporting Trials.

Participants and Sampling
This randomized controlled trial was conducted with a study population consisting of all the second-year nursing students at the Department of Nursing of the University of Patras who voluntarily participated in the study. The eligibility criteria required participants to provide informed consent and have no prior CPR training experience. Participants were excluded if they chose not to continue with the study or had a valid ERC certificate in a BLS/AED course. Students were invited to participate during their mandatory laboratory classes. Informed consent was obtained from all participants involved in the study.
Participants who met the inclusion criteria were randomly assigned with a simple randomization type to three groups, two intervention groups (face-to-face and e-learning training), and one control group, using a computer-generated random number sequence prepared by a researcher with no involvement in the trial. This approach ensured both random and blind assignment, fulfilling the essential criteria for randomization. Participants were unaware of the groups in which they were allocated. The study included 133 participants in total, 43 in the face-to-face group, 43 in the e-learning group, and 47 in the control group.
Effect sizes for calculations used the ratio of standard deviations to compare among three groups or between two points in time within each group. The statistical power analysis was presumed to calculate desired sample size, for the comparison between the three groups in the same time and for comparison within groups over time. Type I error rate was set to be five percent in all considered cases, and approximately 120 subjects (40 per group) were used in total as input to power calculations. Regarding the intergroup comparisons (under an analysis of variance [ANOVA] design with the null hypothesis being: f2 = 0), an effect size of 0.25 illustrated power of 99%. Regarding all intragroup comparisons through time (under a paired standardized mean differences [SMD] scenario with SMD = 0.5 and null hypothesis of “being equal” or “no change through time”), the anticipated power was 85%. The control of the interaction condition with an effect size of 0.25 is similarly expected to be characterized by power of 99% (under a repeated-measures ANOVA design with the null hypothesis being: f2 = 0, and two repeated measures considered). Reference Bulus and Jentschke20
The study was approved by the Ethics Committee of the University of Patras (Reference Number 3390/30-12-2021) and all procedures were in accordance with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All participants took part in the research voluntarily. Before starting the study, written informed consent was obtained from the students who agreed to participate in the study. The purpose of the study was explained to all participants, who were also informed of their right to decline participation or withdraw from the study at any point.
Data Collection: Interventions and Instruments
Before randomization, all participants (n = 133) successfully completed the ERC standard five-hour BLS/AED course (adjusted to COVID-19 guidelines) by accredited ERC instructors in the Simulation Laboratory of the Department of Nursing, University of Patras, using the manikin Little Anne QCPR model (Laerdal Medical; Stavanger, Norway) which includes electronic verification of proper CPR operation. The instructors had more than 10 years’ experience in emergency care. Students were divided into six groups of approximately 22 participants and training was completed in three days. Each student practiced and performed CPR on the simulator until they achieved proficiency. They were encouraged to ask the instructor questions both during and after the training. After the successful completion of the course by all participants, one of the instructors, who also was the principal investigator, administered a questionnaire to assess participants’ theoretical knowledge about CPR. This baseline time point (completion of the BLS/AED course by all the participants) will be referred to as t0.
The questionnaire initially included socio-demographic variables (age, gender, education level) and 13 multiple-choice close-ended questions assessing knowledge of BLS/AED procedures. The questionnaire was developed based on the 2021 guidelines of the ERC and was adapted to the requirements of the present study. The total score ranged from zero to 13, with higher scores indicating greater knowledge. Content validity was assessed by a panel of five emergency medicine experts, using the Content Validity Index (CVI) to evaluate item relevance. Reliability was evaluated through a test–re-test procedure in a separate sample of 30 participants who were not included in the main study. The questionnaire was administered twice with a 20-day interval between administrations, and stability was assessed using the intraclass correlation coefficient (ICC). Internal consistency was assessed using Cronbach’s alpha coefficient based on the responses of the total study sample. Construct validity was examined using exploratory factor analysis (EFA). Item analysis was performed by calculating item difficulty indices. For statistical analysis, the total score was converted into a percentage format and was defined as the Knowledge Score.
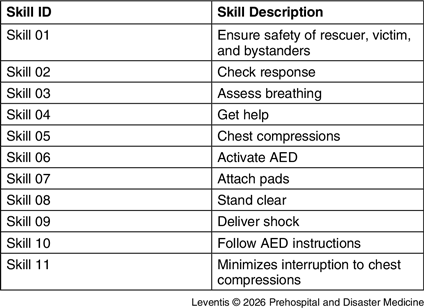
Moreover, the skills that were assessed throughout the course were derived from the ERC CPR/AED 11-item checklist (Table 1). Hence, with ERC certification, it is accepted that all certified participants have proficiency in CPR skills at t0. Numerically, the last fact denotes that all participants possessed with success all 11 skills at t0 which were converted into percent format and from now on will be referred to as Skill Score.
Set of Skills Used to Calculate the Skill Score

Abbreviation: AED, automated external defibrillator.
After a six-month period, Group A received face-to-face training, Group B received e-learning training, and Group C received no intervention. Group A was given at first a ten-minute briefing (using PowerPoint [Microsoft Corp.; Redmond, Washington USA]) on the basic CPR guidelines and then a demonstration of one of the scenarios (ten minutes) of cardiopulmonary arrest that were used during the initial BLS course, under the supervision of the same ERC instructors as in t0. The scenario included space safety, assessment of level of consciousness, airway and breath, call for help, the application of an AED, and the evaluation of high-quality chest compressions. More specifically, when the student entered the simulation room, they encountered a manikin lying on the floor, simulating a person in a public setting who collapsed. The manikin was unresponsive, showing no signs of breathing or pulse. The instructors simulated the resuscitation as follows: (1) assess the situation to ensure it was safe to approach; (2) verify unresponsiveness and assess breathing and pulse; (3) call for help and bring an AED; (4) initiate high-quality chest compressions and perform rescue breaths; and (5) continue for at least two cycles or until the AED was ready to use. The simulation had a six-minute time limit to emphasize quick action and efficient response in a time-critical situation. After the end of the simulation, a ten-minute reflective debriefing of the simulated resuscitation took place to discuss and analyze the performance between participants. Group B received by email a ten-minute video-recorded lecture (the same as Group A) and a video demonstrating the same resuscitation procedure as above (ten minutes). Afterwards, all participants replied with an email that they had watched the video and asked any potential questions to imitate the debriefing stage of Group A.
After one year (point t1) of the initial BLS/AED course and six months after the interventions, all participants (n = 133) were re-assessed individually for their theoretical knowledge on the same questionnaire with no previous notice. They were also given the same ten-minute simulated scenario of cardiopulmonary arrest with the intervention, using the same manikin, to assess the set of 11 skills. No feedback was provided during or after the scenario. The skills test was stopped after completing two cycles of CPR and shock delivery. For assessing the skills, two examiners/instructors applied the ERC CPR/AED 11-item checklist and calculated the Skill Score.
Statistical Analysis
Composite normality of data was tested with Shapiro-Wilk test. According to its outcome, non-parametric descriptive statistics included median (Q1 – Q3) for quantitative variables and count (%) for qualitative variables. Regarding the second ones, there was considered as base level: the control level for the group variable, male for gender, 18-19 years old for age, the general high school type, and urban for the area. Inferential “among group” analysis involved Kruskal-Wallis’s test (and Dunn’s test with Bonferroni correction for post-hoc pairwise comparisons) for quantitative variables and Pearson’s Chi-Squared test of independence (including multiple pairwise replications for post-hoc comparisons) for qualitative variables. Inferential “within group” analysis included Wilcoxon’s Signed-Rank test for quantitative variables and McNemar’s test for qualitative variables. All the P values are considered statistically significant when P < 0.05, and all statistical tests are considered as two-sided. Finally, multiple linear regression was applied to connect outcomes with a set of demographic independent variables and the group as well. Associating the “% of the correct skills at point t1” was held in an ANOVA manner. On the other hand, associating the “% Knowledge Score at point t1” was performed in an analysis of covariance (ANCOVA) manner (ie, by also utilizing as a predictor the “% Knowledge Score at point t0”). Again, all the P values are considered statistically significant when P < 0.05. The widths of the 95% confidence intervals have not been adjusted for multiplicity, and the intervals should not be used in place of hypothesis testing.
Results
Validation of the Knowledge Questionnaire
The content validity assessment demonstrated a satisfactory level of agreement among experts, with a CVI of 0.86. The test–re-test analysis indicated strong stability, with an ICC of 0.82. Internal consistency of the questionnaire was satisfactory, with a Cronbach’s alpha coefficient of 0.79. Exploratory factor analysis (EFA) supported a uni-dimensional structure, with an eigenvalue greater than 1.5, explaining 61% of the total variance. Item difficulty indices ranged from 0.40 to 0.85, indicating appropriate discriminative capacity of the items.
Demographic Characteristics
Regarding available demographic evidence, data from 133 subjects (47 controls, 43 of the face-to-face intervention group, and 43 of the e-learning intervention group) showed that 84.21% were female. Participants were primarily aged 18–19 years, with 49.62% in the 20+ age group. In terms of educational background, 8.27% had attended a professional high school (Professional Lyceum), which in Greece focuses on technical and vocational training rather than the academic curriculum of general high schools. Additionally, 33.83% of participants originated from rural areas, with the remainder from urban areas. Table 2 illustrates the overall statistics, as well as their distribution among groups.
Demographic Variables of the Cohort and Descriptive Evaluation

Note: N denotes total count. Any statistic is provided as a count (% of the respective total) of the non-base level of any qualitative demographic variable.
Univariate Inferential Analysis
The mean performance scores of students on the theoretical and practical tests performed at t1 are shown in Table 3, which focuses on evaluating all variables of interest among groups. Based on pairwise differences, the e-learning and the face-to-face group Knowledge Score and Skills Score were higher and dissimilar at t1 to controls. The face-to-face and e-learning teaching methods had comparable statistical outcomes in terms of knowledge and skills. Table 3 also evaluates the retention of Knowledge Score and Skills Score at t1 compared to t0, within groups. Although the Knowledge Score decreased over time in all groups, there was no statistically significant difference in its decrease in any of the three groups. On the other hand, there was a statistically significant change (decrease) in the Skill Score over time in control group, but not in the rest of the groups. Due to the significant reduction in the Skill Score in the control group, it was decided to proceed with additional analysis for each skill separately, which is presented later in the results.
Group-Wise Descriptive and Inferential Statistics of the Quantitative Variables of Interest

Note: N denotes total count. Τhe median (Q1 – Q3) describes each distribution, and Kruskal-Wallis’s test is used to extract p. Superscripts are used to imply post-hoc pairwise significant differences via Bonferroni method with a multiplicative factor of 3. Particularly, similar paired superscripts (that is, $ or *) disclose pairwise significant differences. Also, paired analysis of the quantitative variables of interest between t0 and t1. P values are extracted via Wilcoxon’s Signed-Rank test. A P value denotes statistical significance if P <.05.
Multivariate Analysis
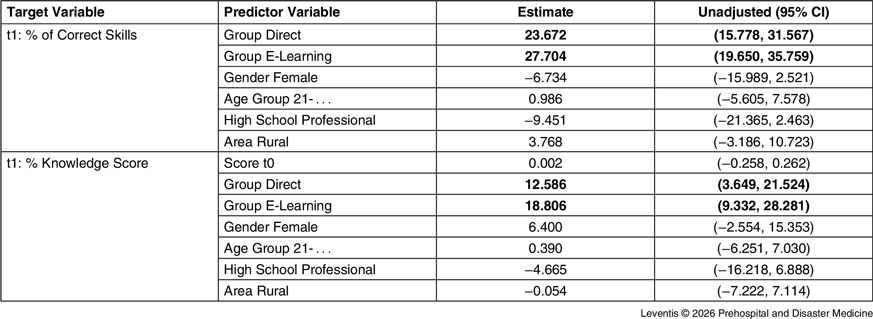
Using linear regression, the effect of demographics and t0 performance on participants’ performance at t1 was examined. Table 4 illustrates the linear regression models on the quantitative targets of % Skill Score and % Knowledge Score. As for already mentioned reasons, the % of Skills Score at t0 was left out from the modeling process; this was not the case when considering the % Knowledge Score. The outcome of this modeling process was that both variables were contingent statistically significantly only of the group variable, regardless of the demographic variables, or the t0 value in the case of the Knowledge Score. The performance of the participants at t1, and considering both dependent quantitative variables, was better for each one of the intervention groups compared to controls, if adjusted by each present demographic variable (and the t0 point variable in the case of the Knowledge Score).
Linear Regression Modeling that Utilizes Performance Quantitative Variables at Point t1 as Targets and All Demographic Variables as Predictors
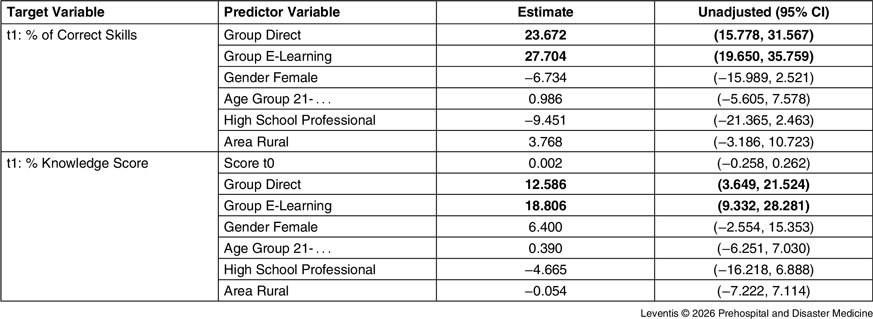
Note: A positive sign of an estimate suggests a positive correlation between the target and the predictor (while a negative one, negative correlation). The widths of the 95% confidence intervals have not been adjusted for multiplicity, and they should not be used in place of hypothesis testing.
More analytically, and with respect to the % Skills Score as a dependent variable, face-to-face had approximately 24%, on average, of larger retainment at t1 (decreased less when compared to t0), and e-learning had approximately 28%, on average, larger retainment compared to the control group. Finally, with respect to % Knowledge Score as a dependent variable, the face-to-face group had approximately13%, on average, higher score than controls at t1, and the e-learning group had approximately 19%, on average, higher score than controls at t1. Average denotes the situation that all demographic variables were considered as joint affecting or contributing factors in the multivariate association. No demographic feature, nor the % Knowledge Score at t0 (whenever applicable), were shown to be significant predictors. Indirectly, also, there seemed to be a marginal increase in participants’ performance at t1 when switching from face-to-face to e-learning mode, but this was not yielded statistically significantly, both when considering the % of correct skills variable and the % Knowledge Score variable.
Univariate Inferential Analysis per Skill
Subsequently, specific skill comparisons among the three groups at t1 was performed, as well as per specific skill comparisons within each group, between t0 and t1. Regarding the performance at t1, both intervention groups performed statistically significantly (P < 0.05) better for almost all skills than controls, except for skills four and nine. Regarding retention, in the control group, there existed a statistically significant reduction (P < 0.05) in all skills. On the other hand, both intervention groups retained all skills, except skills four and nine.
Discussion
This study aimed to investigate if CPR post-qualification training is needed in maintaining knowledge and skills and whether face-to-face or video-based online training (e-learning group) is more effective as an educational method in preserving CPR knowledge and skills in nursing students. After the completion of the BLS/AED course, participants exhibited a similar Knowledge Score and a Skill Score of 100% as it was prerequisite in order to get the certificate. The present study found that after one year, there was a statistically significant difference in Knowledge Score and Skill Score between both intervention groups in relation to the control group, with the intervention groups performing better. This aligns with the findings of previous studies, where participants who attended post-qualification resuscitation training demonstrated significantly higher levels of knowledge and expressed greater confidence in their resuscitation skills. Reference Mohamed Elsayed, Gamal Mahdy and Abdalla Elbiaa21–Reference Marzooq and Lyneham23
This study revealed that although the Knowledge Score decreases over time in all groups, there is no statistically significant difference in its decrease within any of the three groups between t0 and t1. This finding is supported by the AHA which states that knowledge retention tends to decline more slowly than practical skills. Reference Merchant, Topjian and Panchal3 This has been also demonstrated by Garcia, et al Reference Castillo García, Cerdà Vila, de Balanzó Fernández, Quintana Riera, Ferrés-Amat and Rodríguez Higueras24 who found that participants’ knowledge had decreased at nine months without significant between-group differences. However, a study evaluating the long-term effects of CPR education based on theoretical lectures and training found a significant decline in knowledge after three months, highlighting the importance of on-going education and training. Reference Partiprajak and Thongpo14
In the present study, there was a statistically significant decrease in the Skill Score in the control group after one year. These findings align with several studies which reported that participants’ skills performance was dramatically lowered one year after training. Reference Mohamed Elsayed, Gamal Mahdy and Abdalla Elbiaa21,Reference Castillo García, Cerdà Vila, de Balanzó Fernández, Quintana Riera, Ferrés-Amat and Rodríguez Higueras24 However, identifying the exact point at which participants’ skills begin to decline remains difficult, as the literature does not provide a consistent threshold. Notably, one study has shown that adolescents who received technology-based training retained their resuscitation skills for up to eight months, suggesting that the use of innovative training methods may contribute to prolonged retention. Reference Nord, Svensson and Claesson25
Additional analysis for each skill separately showed that the number of students who performed each one of them correctly was significantly higher, in nine out of the eleven skills, in both intervention groups compared with the control group. Previous studies have similarly confirmed the effectiveness of post-qualification education. Reference Cho26,Reference Semeraro, Frisoli and Loconsole27 In the present study, the e-learning group had the best performance in skill one, which was to ensure safety of the rescuer, victim, and bystanders. This is identical to the finding of another study which showed that the video-based group performed better scene safety as compared to the standard instructor-based group. Reference Chien, Tsai and Huang28
On the contrary, the performance in skill four (get help) and skill nine (deliver shock) did not differ significantly between all groups after one year. Furthermore, overtime, inferential analysis for these skills showed significant decrease within all three groups. Calling for help was the most forgotten step in all groups. In the light of these findings, it can be recommended that the importance of calling for help and delivering shock, in a right safe way, should be emphasized during both face-to-face and online training interventions. As mentioned above, the literature does not identify a precise point at which skill retention begins to decline, though guidelines generally suggest this occurs between three and six months. Reference Hernández-Padilla, Suthers, Granero-Molina and Fernández-Sola29
To the best of the authors’ knowledge, no other published study has conducted a multivariate analysis comparing Knowledge Score and Skill Score towards demographic factors, except for Toner, et al Reference Toner, Connolly, Laverty, McGrath, Connolly and McCluskey30 who found that male students showed relatively greater improvements in post-training Knowledge Scores compared to female students. In this study, despite the overall decrease in the performance of the participants one year after baseline, the decrease is not as high in the e-learning (primarily) and the direct (secondarily) groups as it is in control. This property remains irrelevant to demographic characteristics of the participants (gender, age group, high school type, and area of origin) and to their baseline (t0) knowledge and skills’ status. Both types of interventions had similar success, with the e-learning group demonstrating a non-significant trend toward greater retention. In numerous studies, it has been shown that e-learning is more effective than instructor-led CPR education in enhancing knowledge and performance. Reference Mundell, Kennedy, Szostek and Cook16–Reference Tobase, Peres, Gianotto-Oliveira, Smith, Polastri and Timerman18,Reference Mohamed Elsayed, Gamal Mahdy and Abdalla Elbiaa21,Reference Chien, Tsai and Huang28,Reference Hernández-Padilla, Suthers, Granero-Molina and Fernández-Sola29 However, similarly to the present study, several studies have found that e-learning does not yield significantly better results than traditional in-person education. Reference Lynch, Einspruch, Nichol, Becker, Aufderheide and Idris15,Reference Horiuchi, Yaju, Koyo, Sakyo and Nakayama19,Reference Castillo García, Cerdà Vila, de Balanzó Fernández, Quintana Riera, Ferrés-Amat and Rodríguez Higueras24,Reference Nord, Svensson and Claesson25
The divergent results reported in the literature regarding the effectiveness of e-learning versus face-to-face CPR training may be influenced by several factors. Differences in participant characteristics, such as age, baseline knowledge, prior exposure to CPR training, and motivation, could affect skill acquisition and retention. Regional educational standards and curriculum structures may also play a role, as the intensity, frequency, and methods of CPR instruction vary across institutions and countries. Furthermore, the design and interactivity of e-learning platforms differ widely, which can impact learner engagement and outcomes. These contextual factors may explain why some studies report superior performance with e-learning, while others find no significant differences compared to traditional instructor-led approaches. Recognizing these variations is important for interpreting these findings and considering their generalizability to other student populations and educational settings.
Limitations
This study has several limitations. First, the knowledge and skills of nursing students from a specific academic institution in one country were examined, and the sample may not be representative of the wider population of nursing students, which limits the generalization of the results. Therefore, additional and broader studies seem necessary to confirm the current findings. Second, the effect of human factor in BLS/AED teaching cannot be neglected as the skills, knowledge, and experience of instructors may vary. Finally, the study was conducted using a single scenario involving a manikin and simulation video to replicate a cardiac arrest event, which can only partially mimic real-life conditions.
Conclusion
In Greece, undergraduate nursing education is a four-year program. This study suggests that additional post-qualification training may help support the retention of CPR knowledge and skills among nursing students, while face-to-face and e-learning training appear to produce comparable outcomes. Consistent with previous evidence, knowledge retention declined more gradually than practical skills, with a notable deterioration in CPR skills observed approximately one year after the initial qualification course. These findings should be interpreted cautiously and do not imply a modification of certification intervals recommended by international resuscitation organizations such as the AHA or the ERC. Rather, they highlight the potential value of reinforcement or refresher educational activities to support long-term retention. Further research is needed to explore effective long-term retention strategies and optimal approaches to maintaining CPR competence.
Author Contributions
Conception and Design: AB, NS, CL, MI, AT, PK, JL, and CM.
Drafting Manuscript or Revising it Critically: AB, NS, CL, MI, AT, PK, JL, and CM.
Final Approval of the Document: AB, NS, CL, MI, AT, PK, JL, and CM.
Agreed to be Accountable for All Aspects of the Work: AB, NS, CL, MI, AT, PK, JL, and CM.
Conflicts of interest
Charalampos Leventis declares none; Angeliki Bistaraki declares none; Michael Igoumenidis declares none; Anastasios Tzenalis declares none; Panagiotis Kiekkas declares none; John Lakoumentas declares none; Christos Marneras declares none; Nikos Stefanopoulos declares none.



 Open access
Open access