

Introduction
The co-occurrence of mental health and substance use disorders can present a dilemma to healthcare systems (Whiteford et al., Reference Whiteford, Degenhardt, Rehm, Baxter, Ferrari, Erskine and Vos2013). Individuals with co-occurring conditions often experience poorer outcomes, higher rates of hospitalisation, increased risk of relapse, and greater social and economic costs relative to those with single disorders (Esmaeelzadeh et al., Reference Esmaeelzadeh, Moraros, Thorpe and Bird2018; Pacek et al., Reference Pacek, Martins and Crum2013). Traditional service delivery models, typified by siloed approaches to co-occurring conditions, have been shown to be inadequate in addressing the multi-faceted needs of this population. Patients often report a ‘bouncing between’ effect, receiving care that is poorly coordinated and fails to address the interplay between their mental health and substance use (Lawrence-Jones, Reference Lawrence-Jones2010). Patients also report being told by each respective service to use the ‘other’ team prior to their own (Black, Reference Black2021) before starting any treatment.
NHS Talking Therapies (NHS TT) have in the past published a Positive Practice Guide in working with substance use (National Treatment Agency for Substance Misuse, 2012), but this guide appears to have gathered less traction than other similarly published positive practice guides.
Dame Carol Black’s Independent Review on Drugs (Reference Black2020, Reference Black2021) provides a stark reminder of the systemic issues in addressing substance use in England and Wales. The review highlights the significant harm caused by illicit drugs, the rising rates of drug-related deaths, and the profound impact of addiction on individuals, families, and society. Black (Reference Black2021) emphasises the urgent need for a ‘whole-system approach’ that integrates prevention, treatment, and recovery services, with a focus on inter-agency collaboration and coordinated care pathways mirroring recent guidance from the Royal College of Psychiatrists (2025).
Harris et al. (Reference Harris, Dalkin, Jones, Ainscough, Maden, Bate, Copello, Gilchrist, Griffith, Mitcheson, Sumnall and Hughes2023) further emphasise the adverse impact of unintegrated care on individuals with co-occurring disorders. They highlight the scarcity of practical frameworks to guide clinicians in delivering integrated care. The current service delivery system, as highlighted in the Black Review, is ill-equipped to meet the complex needs of individuals with co-occurring disorders.
Although existing literature points to the importance of integrated care, it should be noted that uni-disciplinary care in NHS TT can be sufficient for hazardous or harmful drinkers (Buckman et al., Reference Buckman, Saunders, Cohen, Barnett, Clarke, Ambler and Pilling2021). This is to say, integrated services are not necessarily indicated for every individual who drinks alcohol within NHS TT but should be determined on a case-by-case basis. This paper describes the development and implementation of an integrated service pathway designed to address the challenges of co-occurring mental health and substance use disorders within a primary care context.
The model, a collaboration between an NHS TT service and a local substance use service, uses a ‘reciprocal consultative’ approach, emphasising inter-professional collaboration and shared understanding. This paper will detail the key features of this model, the drivers involved in its establishment, and the mechanisms for ensuring continuity of care. The paper has a primary focus on the service model, with a small-scale summary on patient outcomes.
The integrated service model: a reciprocal consultation approach
The integrated service model was developed in response to the limitations of existing service delivery for individuals with co-occurring disorders. The primary aim was to create a more seamless and coordinated pathway, ensuring that patients received comprehensive support that addressed both their mental health and substance use needs. The model is underpinned by the following key principles:
-
(1) Reciprocal consultation: a core feature of the model is the emphasis on shared expertise and collaborative decision making between NHS TT therapists and substance use recovery workers. This involves a shift away from a traditional hierarchical model towards an approach where all professionals contribute their unique knowledge and skills to inform decision making. Concretely, this involved recovery workers sharing their expertise on substances and their effects on mental health whilst also allowing therapists to share their expertise of psychological mechanisms and how substances fit within a formulation.
-
(2) Patient-centeredness: the patient is placed at the heart of the integrated care process. Treatment planning and delivery are guided by the patient’s individual needs, goals, and preferences, with a strong emphasis on shared decision making and empowerment.
-
(3) Holistic assessment and care planning: the model promotes a comprehensive understanding of the patient’s situation, encompassing their mental health, substance use, social circumstances and physical health. This holistic assessment informs the development of a coordinated care plan that addresses the interconnected factors contributing to their difficulties.
-
(4) Continuity of care and information sharing: mechanisms are in place to ensure seamless transitions between services and effective communication between professionals. This includes the development of shared protocols and regular inter-agency meetings leading to a coordinated and consistent approach to patient care. Concretely, this might look like timing a therapy to begin following a patient completing a detox.
-
(5) Skills sharing and mutual learning: the model promotes ongoing professional development through knowledge exchange and skills sharing between NHS TT therapists and recovery workers. This enhances the competence and confidence of both professional groups in addressing the complexities of co-occurring disorders.
Model implementation
The implementation of the integrated service pathway involved several key processes:
-
Managerial buy-in: gaining support from clinical and operational service managers within both the NHS Talking Therapies service and the substance use service was crucial for the successful implementation of the pathway. This involved clearly articulating the rationale for integrated partnership care, highlighting the potential benefits for patients and services, and addressing any concerns or reservations. In this context, this was made simpler due to both services falling under the same NHS trust.
-
Establishing communication protocols: clear and effective communication protocols were developed to facilitate information sharing and coordination between the two services. This included the establishment of regular minuted inter-agency meetings.
-
Defining roles and responsibilities: the roles and responsibilities of different professionals within the integrated care team were clearly defined. NHS TT therapists provided specialist mental health assessment and therapeutic expertise, while substance use recovery workers offered expertise in substance use and recovery support. The reciprocal consultative approach ensured that both professionals contributed their unique perspectives and skills to the care plan.
-
Ongoing review and follow-up: mechanisms were established for ongoing review and follow-up of patients engaged in the integrated pathway. Regular meetings between the partnership care team allowed for monitoring of patient progress, adjustment of treatment plans as needed, and proactive management of any challenges or setbacks. Patients included in the collection of data in the pilot were marked as follow-ups in each meeting and progress was routinely discussed between the two services.
The integrated care pathway
The integrated care pathway consisted of two primary treatment options, offering flexibility to meet the diverse needs of individuals with co-occurring disorders:
-
(1) Co-facilitated emotion regulation skills group: this 8-week group intervention, facilitated by a therapist and a substance use recovery worker, targeted individuals identifying emotional dysregulation as a key factor or trigger preceding substance use. The group provided an environment for patients to learn and practise emotion regulation skills, with the facilitation model allowing for a blend of therapeutic expertise and practical recovery support. All patients completing this group were offered a post-group review and a route into one-to-one therapy should they wish to do this.
-
(2) Integrated one-to-one therapy: this option involved individual therapy sessions delivered by NHS TT practitioners, with the patient’s allocated recovery worker participating in the initial assessment and in subsequent review sessions (typically every sixth session). These triadic meetings provided a platform for collaborative assessment, treatment planning, and ongoing review, ensuring that both mental health and substance use needs were addressed in a coordinated manner.
Figure 1 illustrates the reciprocal consultative nature of the integrated one-to-one model. The overlapping circles represent the distinct but interconnected roles of the patient, NHS TT therapist, and substance use recovery worker. The areas of overlap highlight the shared focus on patient needs and goals, the integration of therapeutic interventions with recovery support, whilst also respecting that each professional would also have a one-to-one relationship with the patient that would not overlap.
Patient, NHS TT and substance use team overlap.

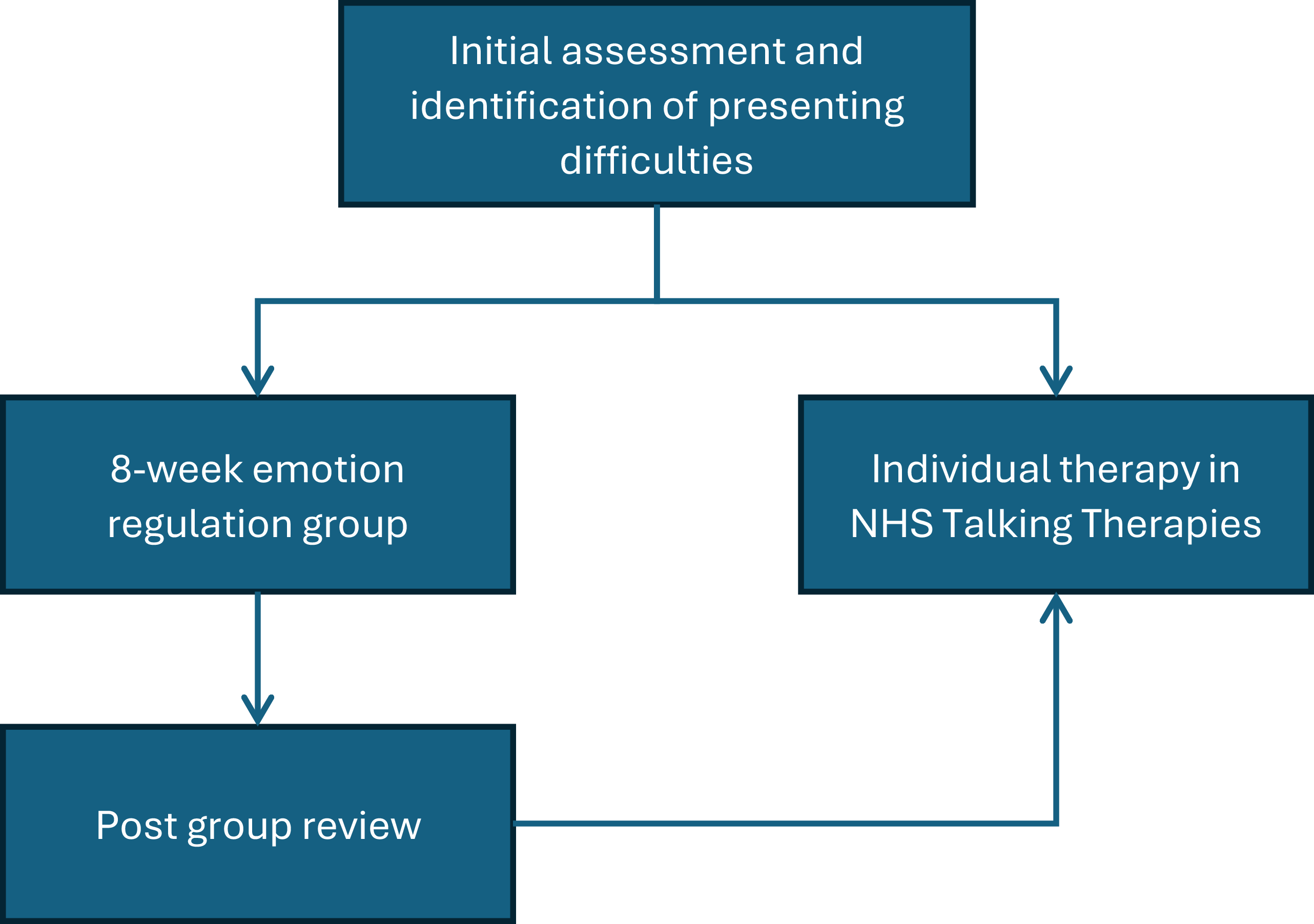
Figure 2 illustrates the pathway for individuals with co-occurring disorders. The figure highlights the two treatment options that follow initial assessment and identification of presenting problems. Patients were offered the choice of the emotion regulation group or one-to-one sessions. Patients completing the group were also given the choice of further one-to-one sessions with NHS Talking Therapies.
Integrated care pathway.

Supplementing the two aforementioned interventions, the pathway incorporated a fortnightly inter-agency multi-disciplinary team (MDT) meeting. This forum served several key functions: facilitating joint care planning for cases requiring inter-agency input, reviewing and approving referrals, and enabling proactive planning for anticipated patient needs (e.g. timely initiation of therapy following detoxification). Additionally, the MDT provided a valuable platform for senior practitioners to engage in reciprocal consultation and learning more about the ‘other’ service. Decision-making regarding patient suitability for therapy in instances of clinical uncertainty was guided by adapted readiness questions derived from Buckman et al. (Reference Buckman, Naismith, Saunders, Morrison, Linke, Leibowitz and Pilling2018), originally based on the Alcohol Use Disorders Identification Test-Concise (Bush et al., Reference Bush, Kivlahan, McDonell, Fihn and Bradley1998).
Service evaluation: a focus on model implementation
This service evaluation employed a mixed-methods approach to examine the development and implementation of the integrated care pathway. The principal aim was to describe the service model, outlining its structure, rationale and practical delivery. Quantitative and qualitative data were gathered to provide an indication on feasibility and acceptability, but are not the focus of this paper.
Method
The service evaluation consisted of the following components:
-
Service model description: a detailed description of the integrated pathway was developed, drawing on service protocols, meeting minutes, and interviews with key stakeholders (service managers, clinicians, and recovery workers). This description outlined the pathway’s key principles, components, and operational procedures. A central aspect of the pathway’s development was the implementation of collaborative assessments, conducted jointly by the NHS TT and substance use clinicians, alongside regular patient reviews.
-
Quantitative outcome data: routine outcome data collected within the NHS Talking Therapies service and the substance use service were analysed. This included scores on the Patient Health Questionnaire-9 (PHQ-9; Kroenke et al., Reference Kroenke, Spitzer and Williams2001), the Generalised Anxiety Disorder-7 (GAD-7; Spitzer et al., Reference Spitzer, Kroenke, Williams and Löwe2006), and the Treatment Outcome Profile Scale (TOPS; Marsden et al., Reference Marsden, Gossop, Stewart, Best, Farrell, Lehmann and Strang2000), administered at pre- and post-treatment.
-
Qualitative data: patient and staff interviews were audio-recorded, transcribed verbatim, and analysed thematically following Braun and Clarke’s (Reference Braun and Clarke2006) approach. For the purposes of this service evaluation, findings are presented at a summary level, focusing on high-level information most pertinent to the implementation of the integrated service model rather than an in-depth, qualitative analysis.
Results
The service evaluation revealed the following key findings.
Qualitative outcomes
-
Improved inter-service collaboration: the implementation of the integrated service pathway led to significant improvements in communication and collaboration between the NHS Talking Therapies service and the substance use service. Regular inter-agency meetings, the development of shared protocols, and improved information sharing facilitated a more coordinated and consistent approach to patient care. Therapists and recovery workers reported a greater understanding of each other’s roles, perspectives, and expertise, leading to more effective teamwork and a shared sense of purpose.
-
Reciprocal consultation practice: the reciprocal approach was viewed positively by both therapists and recovery workers. They reported that the model facilitated knowledge exchange and skill development. Attending therapists gained a better understanding of substances and recovery principles, while recovery workers enhanced their skills in mental health assessment and formulation. This mutual learning fostered a more holistic and integrated approach to patient care.
-
Patient-centred care: the integrated pathway was perceived as promoting a more patient-centred approach. Patients reported feeling that their needs were better understood and addressed through the coordinated efforts of the two services. The emphasis on shared decision-making and collaborative treatment planning empowered patients to take a more active role in their care. Patients reported improvements generally to their mental health in addition to specific coping strategies and overall wellbeing.
-
Improved continuity of care: the mechanisms for ensuring continuity of care, such as joint reviews and coordinated transitions, were seen as beneficial in providing a more seamless and consistent patient journey. Patients reported experiencing less fragmentation and a greater sense of being supported throughout their treatment.
Quantitative outcomes
Analysis of routine outcome data from NHS Talking Therapies found that seven of nine patients were discharged with scores that would meet the definition of recovery in Talking Therapies. It is important to note, however, that two patients who entered therapy did not meet caseness. The TOPS data indicated a reduction in substance use severity for six of nine participants.
Discussion
The findings of this evaluation highlight the potential of integrated care to enhance inter-agency collaboration, promote a more holistic approach to patient care, and improve communication and coordination between different teams. In addition, the model facilitated knowledge exchange and skill development among therapists and recovery workers, fostering a shared understanding of patient needs and a more joined-up approach to treatment planning and delivery. The positive feedback received from patients underscores the importance of a patient-centred approach that empowers individuals to take an active role in their care and promotes a sense of being supported throughout their treatment journey. Therapists reported feeling more confident in understanding different types of substances in addition to understanding the effects of different quantities of substances on a patient’s functioning. The outcomes from the evaluation underscore the recommendations outlined in the National Treatment Agency for Substance Misuse (2012) Positive Practice Guide, particularly highlighting the impact of more nuanced and interconnected working between NHS Talking Therapies and substance use services.
The initial patient outcome data, while limited by the small sample size, suggest that the pathway could be effective in improving both mental health and substance use outcomes. The improvement in symptoms, as measured by the NHS TT minimum dataset, provides some preliminary evidence of the pathway’s potential to alleviate mental distress. The feedback from patient and staff interviews further support these trends, with patients reporting improvements in their overall wellbeing and coping skills.
The pathway aligns with the recommendations of Dame Carol Black’s Independent Review on Drugs (Reference Black2021), which calls for a ‘whole-system approach’ to address the complex needs of individuals with co-occurring disorders within the primary care context. Black (Reference Black2021) emphasises the importance of breaking down inter-agency barriers, improving communication and coordination between services, and ensuring a more seamless and patient-centred care experience.
Recommendations
To improve access and flow, consideration should be given to implementing ‘fast track’ pathways for this cohort, potentially alongside adapting expected ‘Recovery’ targets for this group towards measures like ‘Reliable Improvement’. In addition, the authors wonder about instead of (or, in addition to) using an anxiety disorder-specific measure within the minimum data set, utilising the TOPS to contribute in assessing efficacy of treatment.
The current NHS TT assessment process could be enhanced by incorporating relevant screening questionnaires for substance use at initial contact (i.e. TOPS), building on the paper’s description of adapting readiness questions for assessment suitability. This measure could potentially be built in within integrated Artificial Intelligence onboarding services which many NHS Talking Therapies service employ. Furthermore, supplementing the NHS TT staff team with additional substance use top-up training akin to current Psychological Therapies for Serious Mental Health Problems (PT-SMHP) offers could further increase confidence and competence within the staff team.
The successful integration of substance use recovery workers in this model suggests the value of employing such roles more widely within NHS TT and primary/secondary care psychology services, and is in line with Black’s (Reference Black2021) recommendations.
To overcome systemic barriers, improving shared electronic patient record systems and inter-service information sharing is crucial to support coordinated care and facilitate vital follow-ups, which are currently often lacking. These systemic improvements, alongside the model’s emphasis on co-facilitated interventions and joint working, are essential steps towards a truly integrated system capable of meeting the complex needs of individuals with co-occurring disorders, as advocated by Black (Reference Black2021).
Adaptability and scalability
The integrated service pathway described in this paper demonstrates potential adaptability and scalability to other healthcare settings, particularly secondary or specialist services with co-located substance use teams. The core principles of reciprocal consultation, inter-professional collaboration, and patient-centred care are transferable to various contexts where individuals present with complex and co-occurring needs.
Further research is warranted to explore the feasibility and effectiveness of implementing this model in different settings and with larger and more diverse patient population. The current evaluation is based on a small sample, in a primary care setting which limits the generalisability of the findings. A pilot study in a secondary care setting, such as a community mental health team with an embedded substance use recovery worker, could be a valuable next step. Such a pilot could examine the specific adaptations required to implement the model in a different context, the impact on staff roles and responsibilities, and the potential benefits for patients with more severe and complex presentations. It would also be valuable to explore the long-term outcomes of this integrated pathway and to assess whether its impact is sustainable over time.
Finally, future research should take a closer look at staff experiences while delivering integrated care. This could lead to a better insight into how roles are defined, and how an integrated pathway impacts inter-agency dynamics and effectiveness for patients.
Learning and reflections
The implementation of this reciprocal consultation model yielded many learning opportunities, extending beyond individual skills acquisition to shape inter-service dynamics and inform future practice. Therapists gained valuable, practically oriented knowledge about substance use – the nuances of withdrawal, the impact of different substances on mental states, and indicators of readiness for psychological intervention. This demystification of substance use fostered greater confidence and reduced hesitancy in working with this population. Simultaneously, recovery workers developed an appreciation for the complexities of mental health conditions and the theoretical underpinnings of therapeutic interventions, enhancing their ability to support individuals navigating co-occurring difficulties and facilitating smoother transitions into talking therapies (i.e. substance use as a mechanism to cope with flashbacks in post-traumatic stress disorder). The shared learning environment fostered a culture of mutual respect and a more holistic understanding of patient needs, moving away from fragmented, single-agency perspectives towards a unified approach. The learning derived from this model underscores the importance of intentionally creating spaces for inter-professional dialogue and knowledge exchange to improve the quality and coordination of care for individuals with co-occurring difficulties.
How to foster inter-professional learning in integrated care
-
Establish regular joint meetings: schedule consistent inter-agency minuted meetings (e.g. MDTs, case consultation forums) with protected time for discussion and shared problem-solving.
-
Implement co-facilitated interventions: where appropriate, design and deliver joint interventions (e.g. groups, initial assessments) that necessitate active collaboration and shared expertise.
-
Create continuing professional development opportunities: arrange joint training sessions, workshops, or shadowing experiences where professionals can learn directly from each other’s disciplines.
-
Develop shared protocols and guidelines: collaboratively create integrated care pathways and protocols that reflect the combined knowledge with both services and service users.
-
Promote reciprocal consultation: embed a culture of seeking and offering consultation across services, valuing the unique perspectives and knowledge of each professional group. Explicitly name this in any Terms of Reference document for the joined-up inter-agency meeting.
-
Encourage cross-service communication and relationship building: foster informal communication channels and opportunities for social interaction to build trust and understanding between teams. If possible, sharing estates would be ideal to promote face-to-face relationships where possible.
-
Actively solicit feedback from both professionals and patients: regularly gather feedback on the learning process and the impact of collaboration on service delivery and patient experience. Embed the need for quantitative and qualitative evaluations on a regular basis within any joined-up service agreements reviewed by senior clinicians from both services. Invite service users to be a part of a forum that oversees the development of the pathway to gain additional insights.
Conclusion
This service evaluation describes the development and implementation of an integrated care pathway for individuals with co-occurring mental health and substance use disorders. The model, characterised by a reciprocal consultative approach and a strong emphasis on inter-professional collaboration, demonstrates potential as a framework for improving service delivery and enhancing patient care. While the patient outcome data are limited by the small sample size, the qualitative findings and the focus on a service model offer insights for service re-design and future research. The model’s adaptability to other settings, coupled with its alignment with several of the recommendations of Dame Carol Black (Reference Black2021) for greater integration and a more coordinated, patient-centred approach, suggests that this integrated care model has the potential to be a valuable framework for services.
Key practice points
-
(1) Support from clinical and operational leaders is required for the successful implementation of this integrated service pathway.
-
(2) Alongside joined-up sessions, successful delivery of integrated care includes regular inter-agency meetings, the development of shared protocols, and sharing of patient information (where consent is given) to strengthen collaboration across services.
-
(3) Regular joint reviews of patient progress allow for timely adjustments to care plans, shared decision making, and early identification of setbacks.
-
(4) Clearly defining roles and responsibilities between professionals enables more cohesive care planning and fosters mutual respect across disciplines.
Data availability statement
The data that support the findings of this study are available from the corresponding author (R.P.), upon reasonable request.
Acknowledgements
The authors would like to acknowledge how helpful it was to receive consultation, support and education from Samantha Bheenick, Mark Frost, Spencer Hempsted, Leanne Horwill, Alexander James, Paul Moorcraft, Sarah Stacey and Tom Sturman. It was tremendously helpful to be on the journey with you all on this from 2022 to 2024.
Author contributions
Richard Pione: Conceptualization (lead), Methodology (lead), Writing - original draft (equal), Writing - review & editing (lead); Patrice Adjovu: Data curation (supporting), Formal analysis (equal), Methodology (supporting), Writing - original draft (equal); Clare Dolan: Conceptualization (supporting), Data curation (equal), Formal analysis (lead), Investigation (equal), Resources (supporting), Writing - original draft (equal).
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare none.
Ethical standards
Authors abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BPS and BABCP. Ethical approval was not required for this research, according to the NHS Health Research Authority Tool (Health Research Authority). The project was approved by a NHS Research & Innovation department under the category of service evaluation. All participants gave informed consent for their anonymised data to be used in the service evaluation. Confidentiality was maintained in line with NHS Trust governance procedures, and all data were stored securely. The evaluation was registered with the Midlands Partnership NHS Foundation Trust, Research and Development team (references e2021-49 and e2021-52), and conducted in accordance with local governance approvals.


 Open access
Open access
Comments
No Comments have been published for this article.