


Introduction
Antimicrobials are prescribed widely by providers in both subspecialty and general practice to treat infections. However, a significant proportion of antimicrobials prescribed are non-essential and contribute to resistance and adverse side effects. The CDC core elements of hospital antimicrobial stewardship programs (ASPs) were introduced in 2014 to improve prescribing, limit unnecessary use and patient harm, and combat resistance. 1 Education is a core element of an ASP and should be tailored to the actions most relevant to the target provider group to have a meaningful impact on prescribing practices.
Education for antimicrobial prescribing varies in the medical community despite having a high rate of overuse. Most published antimicrobial stewardship (AS) education interventions have focused on medical students, Reference Hsu2–Reference Wang, Degnan and Luther4 medical residents, and infectious diseases (ID) fellows Reference Alshengeti, Slayter, Black and Top5,Reference Spicer, Armstrong and Schwartz6 with few studies centered on advanced practice providers (APPs). Reference Lee and Stead7,Reference Parzen-Johnson, Toia, Sun and Patel8 APPs, including nurse practitioners (NPs) and physician assistants (PAs), represent a growing group of providers in pediatric inpatient and outpatient settings, and have varied backgrounds and educational experiences. Sym et al found that 66.3% of NP programs include only five hours or less of teaching on antimicrobials in a pharmacology course. Reference Sym, Brennan, Hart and Larson9 Lee et al demonstrated similar findings with 53% of neurocritical care and cardiac surgery APPs at a single center reporting less than 10 hours of antimicrobial education in master’s level training programs. Reference Lee and Stead7 There is even less known about education on AS in APP programs. Similarly, there have been limited studies investigating APP knowledge gaps and interests regarding AS to guide the development of educational initiatives. Reference Abbo, Smith, Pereyra, Wyckoff and Hooton10,Reference Hamilton, Merrill, Luthy and Nuttall11
Involving APP leadership in the development of education can allow educators to customize learning initiatives to fit the unique needs of the institution while also considering providers’ interests and varied backgrounds. Reference Swords, Weddle, Herigon, Stering and Lee12 While understanding the knowledge, attitudes and perceptions of APPs is vital to improving antimicrobial utilization long term, the perspective of key stakeholders of ASPs who help guide clinical decision-making is also necessary to identify target areas for educational interventions. Literature that considers the perspectives of APPs and ASP stakeholders is limited but necessary to optimize AS educational efforts. Our study aims to explore attitudes, prescribing practices, and knowledge deficits in AS, and barriers to learning among APPs through a qualitative needs assessment from the perspectives of APPs and ASP stakeholders to inform curriculum development at a large academic children’s hospital.
Methods
Setting
This single center qualitative study consisted of focus groups with APPs and ASP stakeholders at Children’s Hospital of Philadelphia (CHOP).
The ASP consists of three pediatric ID attending medical directors, three clinical pharmacists and several pediatric ID fellows. The ASP leads a prospective audit and feedback program where positive cultures and new antibiotic prescriptions are reviewed Monday through Friday, and recommendations are made directly to ordering providers. The ASP team participates in AS handshake rounds three times weekly in the general and subspecialty pediatrics units, pediatric intensive care unit (PICU), cardiac intensive care unit (CICU) and the cardiac care unit. Handshake rounds allow for in-person feedback and targeted education to be given to clinical teams caring for patients identified via prospective audit and feedback. Reference Hurst, Child, Pearce, Palmer, Todd and Parker13 The ASP also approves the use of restricted antimicrobials on a case-by-case basis from 7 AM–10 PM daily. Most antimicrobials require approval from the ASP to prescribe with exceptions for limited preapproved indications.
Recruitment
Participants were recruited from October 9 to November 15, 2024. The project was discussed initially with APP clinical team leaders in the neonatal intensive care unit (NICU), PICU, CICU, and Division of Oncology to characterize the need for AS educational initiatives. APPs from these divisions were deliberately recruited given their higher usage of antimicrobials and frequent interactions with the ASP when prescribing restricted antimicrobials. Once a clear need for this education was identified, potentially eligible APPs were notified of the project in various ways: (1) APP clinical team leaders informed APPs in their divisions through word of mouth and electronic newsletters, (2) flyers with information for registration were posted in APP workrooms, (3) direct verbal communication from the study lead (N.H.) while conducting AS handshake rounds, and (4) individual informational emails to APPs with a registration link. Nine ASP key stakeholders were invited to participate via e-mail based on level of interaction with APPs through the AS pager by study lead (N.H.). This study was considered exempt by the CHOP Institutional Review Board.
Focus groups
Focus groups were chosen for their ability to facilitate the exploration of perceptions, attitudes and feelings while allowing for clarification of views, reflection and rich group discussion. Reference Kevern and Webb14,Reference Woods-Hill, Xie and Lin15 APP focus groups were hosted virtually to improve accessibility for maximal participation.
Four focus groups were comprised only of APPs, in which 11 open-ended questions were asked, including questions about education, training, influences on prescribing practices, knowledge gaps, and desired topics for education in AS, as well as general barriers to ongoing learning (Supplement 1). Questions were reviewed by a study team member (K.M.) and a NICU attending and piloted on a third-year internal medicine resident. Additional probing questions were iteratively added to the focus group guide as themes began to emerge through constant comparison for subsequent focus groups. One focus group included 1 ASP medical director, 3 ASP pharmacists and 2 first-year pediatric ID fellows hosted as a hybrid virtual/in-person meeting. The guide for this focus group included 5 open-ended questions about teaching initiatives, knowledge gaps, and high yield teaching topics for APPs from their perspective (Supplement 2).
Verbal consent was obtained from all participants prior to participation. Four to six participants were included in each focus group. Focus groups were facilitated by one study team member (N.H) who ensured all participants were given a chance to answer each question and moderated discussions. Focus groups continued until thematic saturation was achieved with no new themes or topics emerging during the discussion. Only one focus group was held with ASP stakeholders due to limited overlapping availability of participants. All participants in the study were given remuneration in the form of a $10 gift card for completion.
Data collection
Focus groups were audio recorded via Microsoft TeamsTM and a voice recorder. Audio recordings of focus groups were transcribed by Microsoft TeamsTM, validated and edited to ensure accuracy of transcription, and de-identified by one study member (N.H.).
Analysis
Conventional content analysis with an inductive coding approach was used to develop the initial codebook after completion of all focus groups. Reference Hsieh and Shannon16 Two focus group transcripts were double coded each by two team members (N.H. and J.R. or M.E.) using the Dedoose web application. 17 Study team members discussed discrepancies with assigned codes, used axial coding to develop connections between codes, and refined the codebook.
An inter-rater reliability was calculated across 9 codes with a median κ of .78 (.76–1) and median percent agreement of 95%. The remaining transcripts were coded by one study member (N.H, J.R or M.E) and reviewed by another study member, with disagreements in applied codes discussed as a group.
Results
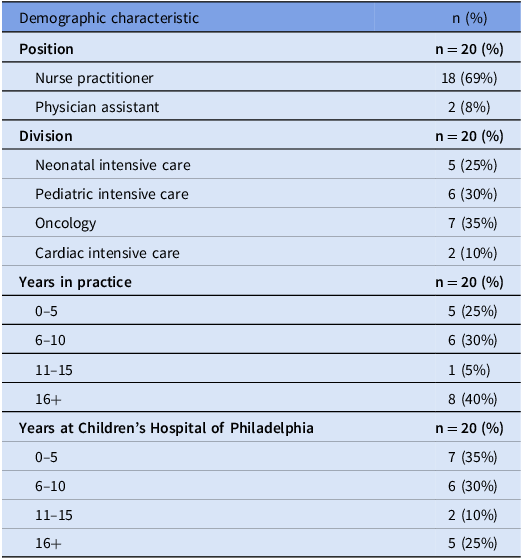
In total, 20 APPs participated in four focus groups (Table 1). 6 ASP key stakeholders participated in one focus group, including one medical director, two pediatric ID fellows and three pharmacists. Focus groups lasted 34 to 56 minutes (average time 47 mins). Four domains were generated with eight themes (Figure 1) with additional representative quotations included in Table 2.
Demographic characteristics of advanced practice providers

Domains and themes identified for antimicrobial stewardship curriculum development.

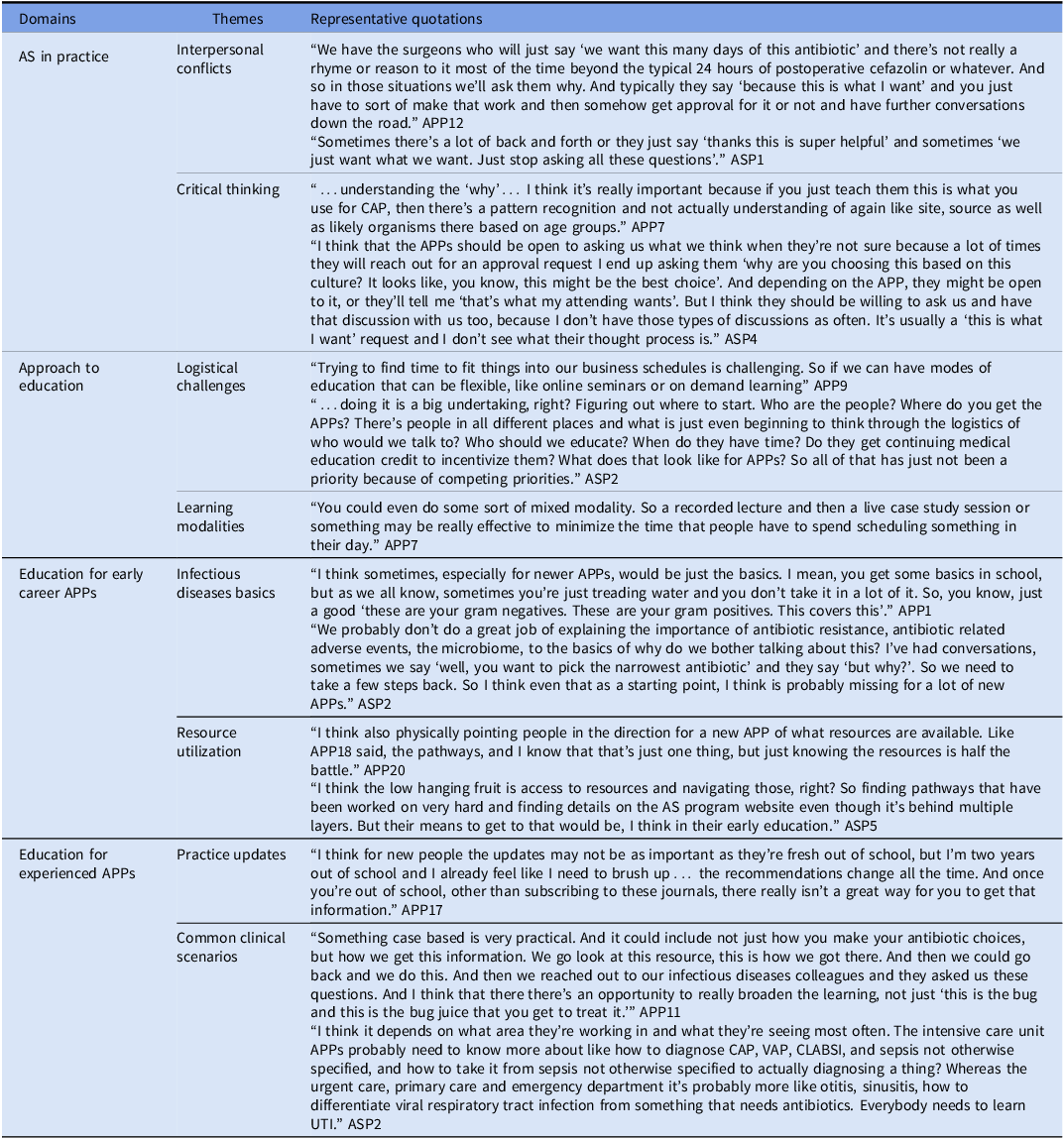
Representative quotations of domains and themes

AS, antimicrobial stewardship; ASP, antimicrobial stewardship program; APP, advanced practice provider; CAP, community acquired pneumonia; VAP, ventilator associated pneumonia; CLABSI, central line associated bloodstream infection; UTI = urinary tract infection.
Barriers to AS in practice
Several barriers to implementing AS into clinical practice were emphasized by participants. Two themes were identified, including interpersonal conflicts and critical thinking.
APPs frequently recounted being given instructions regarding use of antibiotics by their primary attending or a consulting team where they did not understand and/or agree with the recommendations. They highlighted tension with the ASP when requesting approval for use of antibiotics in these situations and described being “between a rock and a hard place” (APP11, APP13) or “the middle man” (APP12, APP17, ASP1). Similarly, ASP stakeholders recalled interactions with APPs requesting approval for antimicrobials that they felt were inappropriate and sensed a lack of openness from APPs to discussing alternatives. APPs report there is no education on how to navigate these types of disagreements despite frequent situations where APPs, the ASP, and consulting teams are “fighting over antibiotics” (APP16). Additionally, APPs also felt that having restrictions in place for prescribing antimicrobials hindered efficiency, and in some cases the depth to which they considered treatment options for their patients. One participant stated, “if I’m lazy I’ll just take whatever infectious diseases tells me to do. But it would be nice to grow and learn” (APP6).
APPs described in detail the various patient, microbiological, and medication factors they consider and how they incorporate them into patient care decisions. However, many APPs expressed discomfort when caring for patients whose clinical presentation did not fall under a standard operating procedure or pathway. Similarly, they noted that their less experienced APP colleagues inappropriately relied largely on pattern recognition for clinical decision-making, stating, “I think we have to learn to think beyond just pathways” (APP7). ASP stakeholders noted that there are significant knowledge gaps among APPs in consideration of a patient’s clinical context, and ordering and interpretation of diagnostic testing that AS practices. As one participant commented, “interpretation of diagnostics is also a problem. They say, ‘this test is positive, it needs treatment’. And that’s not really how that works” (ASP2).
Approach to education
Logistical challenges and preferred learning strategies for effective education were identified by APPs. The most frequently cited barrier was lack of time. Specifically, APPs expressed that their schedules have limited flexibility, making in-person lessons difficult to arrange for larger groups. They also reported numerous interruptions related to patient care during education that took place during regular work hours. APPs expressed that offering options for distance learning, including participating virtually in real time, or having access to recorded lessons, could mitigate this challenge. Pros and cons of preferred learning formats were discussed. There was widespread dissatisfaction with module-based learning, which is a dominant form of APP Continuing Medical Education (CME). When discussing module-based education, one participant said, “I just want to click through, complete it and move on because I’m busy” (APP10). Many participants favored education that is case-based given its promotion of rich discussion among small and large groups that resulted in both deeper understanding and lasting change.
Participants also described the importance of being taught topics related to their specialty, interests, and level of education as crucial for engagement. Incentives to engage meaningfully with education were also highlighted. Many APPs expressed that education qualifying for CME credit, specifically in pharmacotherapeutics for NPs, is a significant incentive for participation.
The ASP stakeholders highlighted several reasons why a formal curriculum has not been developed for APPs thus far. Lack of time and knowledge of how to develop and implement such a curriculum were discussed as the main barriers. ASP stakeholders also felt unsure of the educational background and interests of APPs, noting that APP training is “obviously very different from Doctor of Medicine/Doctor of Osteopathic Medicine training and Doctor of Pharmacy training and it definitely varies by APP” (ASP2).
Education for early career APPs
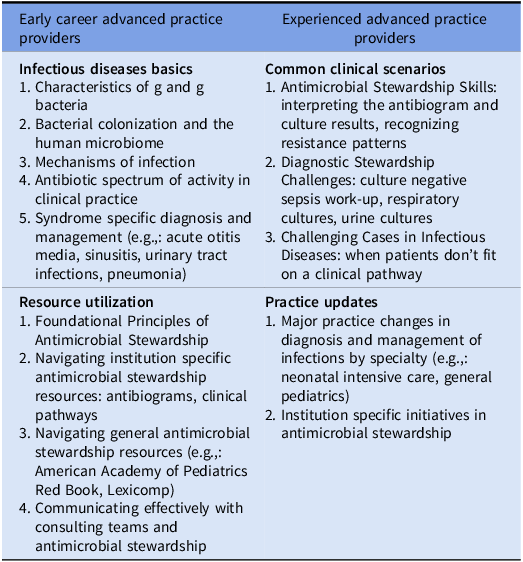
Participants highlighted that the learning needs of early career APPs are different from those of experienced APPs. Specific topics identified are outlined in Table 3. Notably, difficulty with identifying and utilizing resources that are widely available and specific to CHOP for treatment of infections and AS was described by many participants. The CHOP ASP intranet web page contains the antibiogram, institution specific guidelines, diagnosis-specific pathways, and AS decision-making tools, but was described by APPs as “overwhelming” (APP12, APP13) and “not very satisfying” (APP11). Similar concerns were raised by APPs about lack of knowledge regarding which general resources were most appropriate to use to aid in decision-making. The ASP team emphasized a similar need for APPs to learn how to use published resources and highlighted the underuse of the ASP team as a resource. ASP stakeholders expressed that they “want APPs to know who we are when they are onboarding…we are here to help them with any antibiotic questions” (ASP4).
Major topics of interest by level of experience for advanced practice providers

Both APPs and ASP stakeholders expressed a need for early career APPs to learn basic principles in the clinical application of microbiology, antimicrobials, and ID before learning about AS practices. ASP stakeholders noted that teaching AS principles to new-to-practice APPs is difficult because “there’s a lot of missing general infectious diseases knowledge, which makes it hard to teach stewardship” (ASP2). APPs also reported significant variation in their early training when learning about microbiology, antimicrobials, and ID. One APP recalled feeling “really well prepared…it sounds like there’s not much that has changed about antibiotics over the last 20 years” (APP19). Another APP reported their formal training “minimally prepared me…I’m not comfortable with these decisions” (APP16). Several APPs reported their training in antimicrobials was limited within their pharmacology classes, and most reported no dedicated education on AS. APPs specifically expressed a desire to learn about characteristics of g and negative bacteria, and antimicrobial spectrum of activity for treatment. One participant described struggling with “when you have a bug that’s susceptible to multiple antibiotics, figuring out what is more narrow, especially for the cephalosporins because they all look the same” (APP9). Focusing on syndrome-based teaching, particularly for commonly encountered, uncomplicated conditions was highlighted by participants as important earlier in APP education.
Education for experienced APPs
APP participants emphasized the need to learn several AS skills and expressed a desire to incorporate them into practice, including how to use antibiograms, interpret culture results, recognize resistance patterns, narrow antibiotics for definitive therapy and select durations of treatment. Specific topics of interest are listed in Table 3. One participant stated, “if you’re susceptible to several antibiotics, understanding why did you choose antibiotic A or B or C” (APP6) as important to understand. Similarly, ASP6 noted, “being able to interpret cultures would be a very useful skill to reinforce…at least general overviews of what type of susceptibility profiles we might expect for certain organisms, what should we be on the lookout for, and when a susceptibility pattern indicates having to broaden.”
Participants discussed many desired education topics for experienced APPs relating to general and specialty-specific practice. Exploring the nuances of clinical decision-making using case examples was highlighted as valuable for understanding the ID team perspective, and “guiding the critical thinking” for complex patients (APP6). ASP stakeholders endorsed a need for APPs to conceptualize patients’ clinical syndromes and consider “what am I actually worried about? Which is the right test for that…If you don’t have the syndrome right, you’re never going to be able to get the right antibiotic either” (ASP2). Specific clinical scenarios were brought up by APPs and ASP stakeholders as particularly important, including culture negative sepsis, pneumonia, sinusitis, acute otitis media, and urinary tract infections. All participants agreed that targeting cases to the audience and their specialty of practice would be most engaging.
Several participants expressed a desire for education to help keep their practice up to date. Many APPs expressed difficulty with learning about advances in CHOP-specific practices, antimicrobial treatment options, durations of therapy, emerging pathogens, resistance patterns, and geographic updates in the local region.
Discussion
This study is the first of its kind to assess education needs from the perspectives of both APPs and ASP stakeholders and makes important contributions to the consideration of APP education in AS. First, we identified numerous knowledge gaps and delineated important topics for education based on APP level of experience and scope of practice. This allows for the creation of multiple novel curricula that are learner centered. There was overall agreement among APP and ASP stakeholders that emphasis should initially be placed on development of curriculum specific to new-to-practice APPs. Prior survey-based assessments of APPs and AS demonstrated general education needs, particularly in using antibiograms, understanding antibiotics, de-escalating therapy, and identifying resistant organisms. Reference Abbo, Smith, Pereyra, Wyckoff and Hooton10,Reference Hamilton, Merrill, Luthy and Nuttall11,Reference Salsgiver, Bernstein and Simon18 Needs assessments of pediatric physicians identified a wide range of important topics for education including understanding antimicrobial spectrum of activity and local antibiotic resistance patterns, selecting empiric antibiotic, using clinical decision support tools, therapeutic drug monitoring, interpreting culture results, and determining durations of therapy. Reference Salsgiver, Bernstein and Simon18–Reference Sattler, Greer, Lockowitz, Newland, Facer and Wolfe20 Broader assessments of a range of providers have also demonstrated a need for education on diagnostic stewardship. Reference Baker, Hyun, Neuhauser, Bhatt and Srinivasan21 While several of these topics and more were also identified as knowledge gaps for APPs in our study, we additionally clarified the educational background and practice environment of APPs, as well as ASP stakeholders’ understanding of APP practice, providing valuable context for creating educational materials that meet the unique needs of this group of learners.
Second, we identified key elements of the social learning environment as they relate to AS that must also be addressed in curricula development. Social interactions, the community, and desired behaviors of the institution that are often invisible provide valuable context to individual prescriber decisions regarding antimicrobials and must be addressed to promote meaningful changes in prescribing practices. Reference Mukhalalati, Elshami, Eljaam, Hussain and Bishawi22–Reference Szymczak and Linder24 This “prescribing etiquette” of unwritten yet widely accepted cultural rules regarding antimicrobials is strongly influenced by social norms that emerge from unit-based and organizational subcultures. Reference Szymczak, Newland and Barlam25 Pressure from attendings to prescribe antibiotics that a provider does not think are necessary is prevalent, particularly among junior staff. Reference Bashir, Gray, Bashir, Ahmed and Theodosiou26 Senior physician preferences, expectations and prescribing norms also shape junior doctors’ prescribing decisions and they risk facing social sanctions if they make decisions that do not align with these norms. Reference Szymczak, Newland and Barlam25,Reference Krockow, Colman and Chattoe-Brown27 Interestingly, there is a paucity of literature discussing interpersonal issues between primary providers, including APPs, and multiple subspecialty teams. Participants of this study highlighted this as having a significant influence on prescribing habits and a source of tension in relationships with members of consulting teams. This is an important area of future investigation to thoroughly explore the cultural influences of the institution as it relates to provider identity, autonomy, education, and clinical decision-making.
Interpersonal relationships and communication between providers and members of the ASP is also a complicated issue that can hinder AS in practice. The ASP approval process for restricted antimicrobials has been found to decrease efficiency. Reference Salsgiver, Bernstein and Simon18,Reference Rynkiewich23,Reference Szymczak, Kitt and Hayes28 Many providers engage in workarounds, particularly to satisfy demands of their attending or specialty consult service when there are disagreements, which is a phenomenon that was frequently reported by APPs and ASP stakeholders in this study. Reference Salsgiver, Bernstein and Simon18,Reference Szymczak, Newland and Barlam25,Reference Szymczak, Kitt and Hayes28 There are conflicting reports on how restricting antimicrobials and AS handshake rounds impact the relationship between providers and the ASP. Some studies report these interventions have bred antagonism between the ASP and providers, invoked threats to autonomous prescribing, and undermined teamwork, while others had opposite results. Reference Salsgiver, Bernstein and Simon18,Reference Szymczak, Newland and Barlam25,Reference McCreary, Tse-Chang, Forbes and Foulds29 This phenomenon was discussed among participants, and interestingly, some APPs also noted that these measures, particularly the requirement for preapproval to prescribe antimicrobials, led them to defer critical thinking about antimicrobial choices to the ASP.
Third, we identified incentives, barriers and facilitators for learning for APPs with diverse experiences. There is significant variability in teaching resources that APPs find most useful for ID and AS education. Live/virtual recorded lectures (93%) and medical journals (85%) have been rated as most useful for continuing education on antibiotics, with ASPs as a resource ranked slightly lower (77%) by NPs. Reference Hamilton, Merrill, Luthy and Nuttall11 Survey-based studies showed lower utilization of the ASP as a source for education. Reference Abbo, Smith, Pereyra, Wyckoff and Hooton10,Reference Fabian30 In contrast, APPs participating in a pilot AS education program cited lectures as the least utilized source for education and relied primarily on peer-reviewed point of care resources. Reference Lee and Stead7 Participants of this study expressed a need to educate APPs on the utility of the ASP as a resource for clinical decision-making. This lack of awareness could be due to many factors including low exposure to the ASP on certain clinical units and poor explanation of the role of the ASP as a resource for AS practices. The variability in resources for learning may exist because AS education is typically targeted toward medical students and residents with different educational backgrounds and roles. Reference Swords, Weddle, Herigon, Stering and Lee12 Interestingly, despite the rise in popularity of online asynchronous education for time-limited learners, participants in this study unanimously expressed dissatisfaction with online module-based learning in overall engagement and retention. Teaching strategies that incorporate desired elements for learning could include role-playing, guided discussions, gamification, simulated clinical scenarios and concept mapping. Given time constraints highlighted by all participants, other modalities that rely on participation outside of teaching time such as problem based learning and flipped classroom may be less feasible.
This study is not without limitations. First, this needs assessment was conducted in a single center and thus may have unique findings relevant to the specific context of our hospital. This study also included APPs from specific divisions with higher rates of antibiotic use and thus the results may be less generalizable to APPs in all clinical settings. Additionally, most APP participants had more than five years of experience in practice and as such, results may favor those with more experience. However, many comments did consider the perspective and needs of new-to-practice APPs.
Overall, this needs assessment identified several important topics for a comprehensive AS curriculum for APPs with a focus on area of practice and level of experience. Both APPs and ASP stakeholders recognized that further education on AS is important for diagnosing and treating infections and educational content that considers the culture of the institution is essential for enabling true behavior changes. Next steps include developing an engaging curriculum to meet these described local needs utilizing recommended modalities of delivery. Given similar educational needs described in the literature, this curriculum can also be disseminated widely, impacting prescribing practices and improving antibiotic use far beyond the walls of our own institution.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ash.2025.10278.
Acknowledgements
None.
Financial support
This work was funded by the Children’s Hospital of Philadelphia’s Center for Leadership and Innovation in Medical Education.
Competing interests
All authors report no conflicts of interest relevant to this article.




 Open access
Open access