

The Australian Context
Australia is a settler-colonial State, and its head of State is still a British monarch. Britain established six colonies on the continent of Australia, and these colonies negotiated the establishment of a federal commonwealth in 1901. (Reference Grimshaw1) The colonies became states, retaining sole legislative jurisdiction over some areas, including health, while others, such as immigration, became the sole responsibility of the federal government. (Reference Healy2) Australia is now formally independent from Britain, but retains close cultural and legal similarities.
Australia is the sixth largest country in the world based on land area, but its population remains comparatively small, reaching just under twenty-six million in March 2022. (3) Rural industries, including mining and agriculture, loom large in the Australian cultural consciousness, but approximately 90% of Australians live in urban areas. (4) Australian rural and remote communities can be highly isolated, and lack essential services, with some remote communities hundreds of kilometres from their nearest neighbours. As with other Organisation for Economic Co-operation and Development (OECD) nations, service industries make up a large portion of the Australian economy. The small population can result in labour shortages in some industries, including health care, and skilled migrants are often treated as a solution to this issue. In 2023, 30.7% of Australians had been born overseas. (5)
Race and Gender
The Indigenous, or Aboriginal and Torres Strait Islander, communities that predated British colonial rule have been subject to continuing and brutal oppression and marginalisation by a colonial regime that has systematically eroded Indigenous individuals’ access and connection to culture, identity, land and their own ways of knowing and being. (5). Modern Australia has been imposed upon the traditional lands or Country of hundreds of Indigenous nations. Successive waves of immigration in Australia have led to complex cultural and racial dynamics. From the late eighteenth to the mid nineteenth century, migration to Australia consisted of a mix of British convicts and British ‘free settlers’. ‘White’ Australians descended from these and other generations of British migrants form the largest ethnic group of Australians to this day.
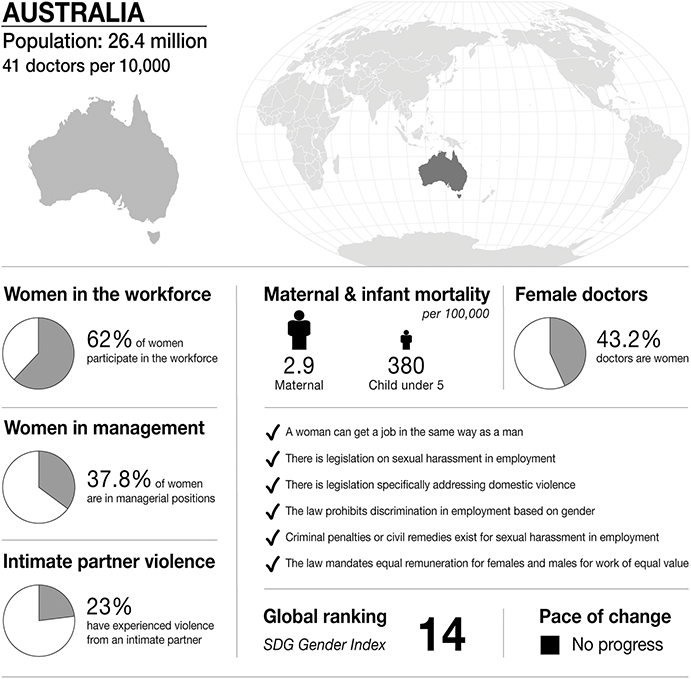
Infographic Australia. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.

Figure 18.1 Long description
The infographic provides information about Australia, with a population of 26.4 million and 41 doctors per 10,000 people. It highlights several gender-related statistics. 62 per cent of women participate in the workforce. 37.8 per cent of women are in managerial positions. 23 per cent of women have experienced intimate partner violence. Maternal mortality is 2.9 per 100,000. Infant mortality under 5 is 380 per 100,000. 43.2 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Australia:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– the law mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 14, and is stable.
In the later nineteenth century, growing agricultural and mining industries attracted more diverse migrants, including many from Asia and the Pacific Islands. (Reference McNeill and Marmo6; Reference Stead and Davies7) Non-white migrants experienced discrimination, abusive working conditions and exploitative labour practices, including indentured labour, and there has been race-based violence throughout Australian history. (Reference Stead and Davies7; Reference Mar8) For the first half of the twentieth century, the vast majority of non-white migrants were rejected, and some non-white residents were deported, in what is known as the ‘White Australia’ policy. The ‘White Australia’ policy was officially ended in 1973. Racism continues to be an unpleasant undercurrent in Australian culture and is a common political target. (Reference Elkin9)
Of note, ‘White Australia’ policies were never accepted by all Australians. Hodges describes the way Australian multiculturalism developed over time, and the complex race relations that have characterised Australian culture. He argues that although Australia had a series of policies, including ‘1901–1945 (bad white Australia policy); 1945–65 (not-quite as bad assimilationist policy); 1972–96 (trying-to-be-good multiculturalism policy); 1997–present (bad new regressive policy)’, these policies were continually challenged. The policies ‘ignore the complex connections people have always made in Australia, even before Federation’. (Reference Hodge10) Australians have a long tradition of championing diversity and human rights which runs in parallel to racist discourses. (Reference Tazreiter11–Reference Bottomley13)
There is a similar history of gender-based violence, with one in four Australian women experiencing intimate partner violence. (Reference Bottomley13) Aboriginal and Torres Strait Islander women are at higher risk. (Reference Bottomley13) Despite public protest, and a recent ‘Australian of the Year’ who championed this cause, (Reference Wheildon15) one woman dies every eleven days due to domestic homicide. (14) The prevalence appears to be rising.
Australia has important cultural myths that shape the experience and response to gender-based and race-based violence. Australians are generally proud of convict heritage, and the anti-establishment and anti-authority culture prevalent in Australia’s history and literature is represented in the so-called ‘tall poppy syndrome’, a description of the way high achieving or successful Australians are often seen as untrustworthy, arrogant and selfish opportunists who need to be ‘cut down to size’. (Reference Peeters16) This form of classist prejudice plays into rape myths, where doctor survivors may not be well supported or acknowledged because they are privileged, and therefore not seen as vulnerable. (Reference Krahé, Kury, Redo and Shea17) The narrative of ‘mateship’ and the myth of egalitarianism (a ‘fair go for all’) obscure the uncomfortable history of racism, sexism, harassment and interpersonal violence that shapes Australia’s history. (Reference Austin and Fozdar18)
Medical Workforce and Health Care Services
The so-called State–Federal divide in health care means financial and policy approaches to health can be confusing and contradictory. General Practitioner trainees are funded and managed through the Federal budget, while other doctors in training are funded and managed primarily in State government-run hospitals. The division between the two systems is one reason why cultural change is difficult.
GPs train and work in small community businesses, and their patients are partly or fully reimbursed through a fee for service insurance scheme called Medicare. Non-GP doctors generally train in salaried positions in State-run hospitals where patients are fully subsidised. Some service delivery models, and some kinds of health care workers, work with distinctive populations with distinctive needs in distinctive ways that are not necessarily encompassed by this description of the mainstream system. Aboriginal Community-Controlled Health Organisations (ACCHOs), for example, often offer salaries rather than fees for service.
The multiple management systems involved in health care make it challenging for doctors in training to understand their rights in any given workplace. Most doctors in training rotate through multiple workplaces, and may need to manage the policy environments of their workplaces, their training organisations and the civil and criminal legal systems of State and Federal courts. Understandably, this can be confusing and impede reporting of sexual harassment.
Australia has a long tradition of fly-in, fly-out (FIFO) services, including the Royal Flying Doctor Service, which has a century-long tradition of supplying health care to isolated communities; however, this does not fully compensate for a lack of rural services. Some remote communities, particularly those with high Aboriginal and Torres Strait Islander populations, have very poor access to health care services. Despite the narrative that Australia has ‘universal health care’, there is a deep divide between health experience access for rich and poor, and between urban, rural and remote populations. These divides exert a profound influence on the kinds of health care experiences an individual may have, and the kinds of experiences a health care worker may have in their ‘workplace’. There are also areas with their own microculture, such as mining communities and farming communities. Outer metropolitan communities are often highly racially diverse. Intersecting marginalisations can mean health care workers can have very different sociocultural experiences, depending on the location of their work.
International Medical Graduate Experience and Vulnerabilities
Over 40% of the rural medical workforce are International Medical Graduates. (19) International Medical Graduates who seek to obtain registration in Australia must complete an International Medical Graduate (IMG) programme to do so. (Reference Board20) In most medical disciplines, after attaining medical registration in Australia, IMGs must work for many years in a ‘priority area’ and obtain a permanent residents’ visa or citizenship in order to provide services covered by Medicare rebates. Theoretically, these conditions are designed to incentivise practising in locations, services, or communities that are under-served. In practice, these conditions appear designed to exploit skilled labour. (Reference Healey, Fakes and Nair21–23)
After undergoing the difficulty and expense of emigrating, IMGs face a range of personal challenges: they start on temporary residency visas, with limited rights, no access to Medicare for their own health care, and a future that is dependent on the immigration arm of the government and the medical training and regulation bodies working in concert with one another to facilitate their career. (Reference Healey, Fakes and Nair21) Doctors who previously held more senior positions must ‘prove themselves again’ under this system with little opportunity for recognition of prior professional expertise (23) and IMGs’ ability to continue to live and work in the country is partly contingent on continuing to work in services that, in rural and remote ‘areas of need’, often leave them profoundly isolated from formal and social systems to protect them from abuse by clients or colleagues. (Reference Board20–23)
Gender in Australian Medicine
Although women are evenly represented in medical graduates, they are not evenly represented across disciplines, or in leadership. (Reference Bismark24; Reference Shalit25) Sexual harassment has been an important dialogue in recent years, with several high-profile cases discussed in the national discourse and described in our discussion. (Reference White26–Reference Colenbrander, Causer and Haire32) High prestige disciplines are still seen as ‘boy’s clubs’, particularly in anaesthetics (Reference Carter33), surgery (Reference Lim34) and cardiology. (Reference Burgess35) Doctors from marginalised groups are at higher risk of discrimination and harassment. (Reference Pascoe36)
In surgery in particular, Australia follows the global trend of being relatively hostile to female surgeons, with less female representation in leadership, and persistent microaggressions towards female surgeons in practice. (Reference Sprow37) Qualitative research in this area suggests there are four types of implicit bias that restrict women from thriving in surgical training and practice: workplace factors such as access to parental leave and role models, epistemic injustices such as unfair assessments of women surgeons’ performance by patients and senior colleagues, objectification and the assumption that they will carry out more emotional labour in their work and life. (Reference Hutchison38)
There are assumptions about ‘Lady doctor’ work that are pervasive, and affect all disciplines. ‘Lady doctors’ are seen by the community to be more empathic, generous, self-sacrificial and interpersonally capable. (Reference West39) These widespread assumptions lead not only to shape the type of work women do, but also the remuneration. In Australia, the medical gender pay gap is wide, (Reference FitzGerald40; Reference Grossman41) and while procedural work is highly valued, cognitive and interpersonal work is not. (Reference Grossman41) Specialties characterised by high emotional labour extract a deep personal toll on contemporary doctors. (Reference Quadrio42–Reference Jenkins44) Doctors in high prestige disciplines, such as neurosurgery, often echo other forms of privilege, and these doctors are more likely to be white, male and Australian born. (Reference McAlpine and Drummond45)
Interestingly, there is often unease between female junior doctors and nurses, which has deep roots in Victorian history. (Reference McAlpine and Drummond45; Reference Heggie46) In our study, one of the participants commented that
Females and medicine are walking this tightrope between being strong and all those traditional male qualities, making decisions, getting on with it and solving problems. Not creating dramas, I guess being a good girl and then also being approachable and nice to the nursing staff.
The unease and fraught power relationships between female doctors and nurses alienates junior doctors from the women who could be their natural allies in the prevention of sexual harassment.
Women doctors also carry the burden of emotional labour outside of their profession. Professor Carolyn Quadrio, a child and adolescent psychiatrist in Melbourne, mentions in a podcast the legacy of domestic violence and emotional work carried by women. She describes her background in a Greek immigrant family, and the legacy of grief, pain and sorry women carry. ‘Women were the emotional organ of the family’, she says, ‘the work of grieving was done by the women’. (Reference Quadrio and Howpage48) She expresses concern that this generation of young doctors are busy managing immediate trauma and are therefore less able to manage longer term concerns around structural barriers: ‘You have to deal with the immediate wound before you think about the battle.’ (Reference Quadrio and Howpage48)
Law
Prosecuting sexual offences generally involves requiring the prosecution to prove the complainant did not consent, and while each state largely emphasises free or voluntary agreement in its definition of consent, each jurisdiction has slightly different definitions of consent as well as different legislation regarding the conditions under which consent may be considered ‘impossible’ or ‘non-existent’ (e.g. if the complainant was drugged or unconscious). (Reference Mathews and Bismark49)
In criminal cases, a jury must determine if the prosecution has proven beyond reasonable doubt that the complainant did not consent to the sexual behaviour in question, considering the complainant’s state of mind at the time. (Reference Mathews and Bismark49) Workplace sexual harms are comparatively rarely prosecuted in criminal court, (50) in part because workplace sexual harms often do not meet the threshold of ‘sexual offence’ definitions, and in part because criminal cases can be costly in relation to one’s time, energy, and finances. Cases often involve specific features that can be re-traumatising and difficult to endure for survivors.
The external bodies that may use civil courts or independent tribunals to receive and respond to allegations of workplace sexual harassment include anti-discrimination or human rights bodies, industrial relations or employment tribunals or the Fair Work Commission, or workplace health and safety bodies or regulators. (Reference Smith51)
Applications to the Fair Work Commission and Industrial Relations/Employment Tribunals
The Fair Work Commission (FWC) is a national workplace relations tribunal. Recent amendments to the Fair Work Act (2009) have empowered the FWC, from November 2021, to hear complaints of workplace sexual harassment and respond to applications for general protections, complaints of unfair dismissal and unlawful termination, and issue orders to stop workplace sexual harassment. (Reference Smith51) ‘Orders’ to stop specified behaviours are a kind of formal legal warning which, if violated, may be enforced by pursuing remedy through civil courts and may include a fine.
The Work Health and Safety Act 2011 (Cth) and Work Health and Safety Regulations 2011 (Cth) specify that employers or workplaces are obligated to prevent (or, if this is not possible, minimise) occupational risks and hazards that endanger the wellbeing of people in the workplace (employee or otherwise). The federal policy body responsible for developing workplace health and safety ‘model laws’, Safe Work Australia, interprets this obligation to include a duty to prevent workplace sexual harms, (Reference Smith51) including a duty for businesses to coordinate work health and safety responsibilities (and how they may be discharged) with other businesses with which they work or share premises.
Medical Education
Doctors in Australia train in universities, with extensive workplace-based learning occurring simultaneously in hospitals, community health centres and general practices. After an undergraduate degree, or an undergraduate and postgraduate degree, the medical students graduate and undertake a series of rotations as ‘junior doctors’, also known as interns in the first year, then residents. After a few years of generalist training, most residents apply to a specialty training scheme and become registrars.
Australian universities have a historical issue with sexual harassment on campus, particularly in residential colleges. In 2016, the peak body representing the thirty-nine universities of Australia (Universities Australia, or UA) launched the Respect. Now. Always. initiative to prevent sexual harms in universities and improve university responses to sexual harms, (Reference MacDermott52–55) including two national surveys of student safety (Reference MacDermott52–53) and culminating in agreements between universities on plans to address sexual harms of students over the next several years, including public accountability measures. (53–55)
Specialty training schemes are run by medical specialist colleges, where the profession is responsible for training and certifying doctors to practise in the discipline. On completing their requisite training, they become fellows of the relevant college, and are then registered by Australian Health Practitioners Regulation Agency as specialists in their relevant discipline.
Learning environments are accredited by the Australian Medical Council to ensure training occurs in high quality environments. General practice is a little different because GPs are funded through the federal government, and practice in private rather than public medical workplaces. Training is heavily subsidised by the federal government and is regulated differently to other medical disciplines. GP trainees are required to undertake some of their training in underserved communities to partially offset this cost, and form a significant workforce for rural and remote Australia. International Medical Graduates have additional training and certification requirements. (23)
Rapid turnover of placements means doctors rarely settle into teams, and may have difficulty acculturating to their context. Sexual harassment policies also overlap. A student, for instance, has a policy framework in their training hospital as well as their university, and a registrar reports to their college as well as their hospital or general practice. Add in legal options, and medical regulatory bodies, and doctors in training can be very confused about who to report to, and what will happen if they do.
Medical Regulation
Australian doctors, including medical students, are regulated by the Medical Board, a federal organisation that is managed by the Australian Health Practitioners Regulation Agency. This agency is responsible for registering health professionals, and the Board hears cases of potential professional misconduct. The Board can temporarily or permanently deregister a health practitioner, which means they are unable to practise their profession in Australia. There are a number of other less severe options for the Board, including education, remediation and supervision. (57)
The Medical Board’s aim is ‘to protect the public’. While the Board does hear cases where a doctor’s behaviour in their personal lives indicates a potential risk to patients (e.g. criminal behaviour, violence and fraud), reports of sexual harassment between colleagues have been relatively rare.
However, there have been some important decisions which shape our understanding of the Board’s stance on these issues. In one case, (58) a doctor had sexually harassed a patient and had consequently undertaken disciplinary action (including an educational course on professional boundaries), then two years later sexually harassed a nurse who worked with him in a hospital.
The Board took immediate action and suspended his licence during the investigation, and he appealed to the Tribunal, arguing that this action was too severe because his misconduct against a co-worker should not be considered equally as egregious as his misconduct towards a patient: ‘to equate conduct between a doctor and a colleague to a doctor and a patient erroneously diminishes the importance of the unique features of a doctor patient relationship’. The Tribunal rejected this argument, and responded:
We do not accept that the conduct of the Respondent to a nurse, working with him in a hospital, where the only reason for his employment in that place must be to apply his knowledge and skill to the medical care of patients in that venue, can be seen in any lesser way than if his conduct had been visited upon a patient he was treating. It was his position as a medical practitioner which gave him access to Person A. In the circumstance of the relationship the Respondent held with Person A in that place, he exercised authority over her and she was, in our opinion, a ‘vulnerable person’ because of that relationship.
In this response, the Tribunal indicated recognition that sexual harassment between colleagues in a medical workplace not only constitutes professional misconduct, but that it involves power dynamics through the hierarchy of the medical workplace that render workers vulnerable.
Case Study
In the foreword to this book, Yoo Young (Dominique) Lee tells us about the sexual assault that changed her career and her life. To our knowledge, hers is the first case in Australia where a doctor who has sexually assaulted another doctor is found guilty in a criminal court. In Australia, a victim of crime is invited to present an impact statement to the court. The following excerpts are from the victim impact statement for Dr Lee.
‘Before the assault, I was a confident, vivacious young thirty-two-year-old woman without a doubt in my mind about my abilities. I was loved by my friends and colleagues because of my fun-loving, caring and bubbly nature. November 22, 2013, everything changed. My whole belief system collapsed. For weeks, I could not comprehend what had happened. I could not understand why my trust was betrayed. I wondered how I could have so stupidly misunderstood the intentions of someone I considered a mentor. I called all other staff specialists in the department by their first name, but I always called the offender Prof because I viewed him as a well-rounded, high functioning clinician and a leader, I respected him so much.
The shock of the assault and the loss of memory haunted me every minute of the day and for the first time in my life, I forgot how to speak. I could not eat or sleep. I found myself avoiding people at work, and I could not hold a conversation with patients. The constant intrusive thoughts and questions about why I was chosen to be the victim of such a despicable crime have robbed me of my confidence and self-worth …
Time is supposed to heal all wounds, but I am still waiting … Every time I’m reminded of the incident, I still feel the same rage, shame, and desire to just disappear. I received a letter of apology from the offender many months ago. His words blame his actions on work stress, life stress, and alcohol and drugs. What I read in this letter are excuses and not an apology …
As doctors, we have a responsibility. As a child, I longed to be a doctor so I can help people. Not just patients but anyone who needs help. When we graduate from medical school, we all swear the Hippocratic Oath. Part of the oath states: “I will remember that I remain a member of society, with special obligations to all my fellow human beings.” I love that. I love that I have the privilege of working alongside people who feel the same way, about how precious life is as I do. I have always respected and looked up to my senior colleagues for the hard work they do, the sacrifices they make for our patients and future generations …
I knew that by informing the authorities about what happened, I was at risk of being labelled a troublemaker. In a highly hierarchical world of medicine this is the most dreaded label. The impact on my career could be irreversible. I was told on several occasions that I would be the one to lose in this trial. I stood by my decision because even if he was not found guilty, it might prevent him from hurting other women. The offender told me himself that reporting the matter would not result in a good outcome in any way. There is an obvious imbalance of power and I couldn’t help but feel small. I am well aware of the resources and connections the offender has that I don’t have …
During the two years before the trial, I worried about how my going forward with the case would impact on my career. I decided few months after the assault that my career in radiation oncology is over, and that I would be left to pursue a career in a different speciality. I had even come to terms with the fact that I may have to leave medicine altogether …
The assault had a major impact on my view on self-worth and I am no longer able to socialize as I used to. My previous relationship drifted apart because of the distance I created. I still struggle to communicate my feelings freely with family and friends …
Although I am not left with physical scars, I am left with deep emotional scars. My world is broken and it will never be the same.’ (59)
Prelude
Before and immediately after the assault, Dr Lee viewed her relationship with John Kearsley as a mentor. However, as time passed, she came to realise that his behaviour was deliberate and predatory. When she reflected on the vulnerabilities experienced by junior doctors, she commented that attrition of self-esteem, hierarchical power relations and lack of respect for interpersonal boundaries was enculturated early in medical school.
When I went through med school, we got into theatre and I was told to stand in a corner and not speak. And it wasn’t surprising if the consultant who you’ve worked with for six weeks didn’t know your name. I think all of that (affects) your self-esteem and makes you think that they’re really important and you’re nothing … Medicine is very hierarchical … And I think that gives them the power to abuse that respect.
She also described the similarities between the supervisor–trainee relationship and other hierarchical and dependent relationships.
I think being a junior doctor is like being in an abusive relationship. … A lot of boundary transgressions, like expecting somebody to come in all weekend when they’re not paid for it. The controller and the controlled. You know how the relationship between your boss and the trainees is often like a weird parental relationship?
In retrospect, Dr Lee felt that medical training teaches junior doctors to suppress emotions, conceal problems, and strive for perfection, which ultimately makes them more vulnerable.
I think, as a profession, we’re not very good at recognising our own emotions, and I think most of us have very poor coping strategies for lots of different problems, and we’re supposed to somehow deal with problems by ourselves without asking people. And I think because, as doctors, we’re so busy focusing on other people all the time, we’re very poor at recognising our own issues. And often, when things are wrong, you don’t know what’s wrong. So I think that’s one of the reasons why people drink a lot and do have unhealthful behaviours … we learn to shut it down.
Assault
Dr Lee describes her experience in the foreword of this book, but in summary, she was invited to a professor’s home for dinner to discuss mentorship. He had a family, and as it is not unusual to have a dinner with a supervisor and their family in Australia, this was not an initial concern. Because she was drugged prior to the assault, she does not recall all of the evening, but she does recall waking up during the assault. She had difficulty putting on her shoes, so was obviously still cognitively impaired when she left his house.
The morning after the assault, she disclosed the situation to a medical friend, and this friend facilitated an appointment with a GP, advocating for her and insisting that they do a drug screen.
The incident happened on Friday night, and on Tuesday, the GP practice called me and said, ‘the urine toxicology’s come back and you have benzodiazepines in it’. The whole thing is no longer a mistake, and it shocked me he had criminal intent. And so, I thought about it for a while and I … I remember my friend and I even made an anonymous phone call to police and asked, what one should do, saying that this is the case that involves a friend. And police are going, you should tell your friend to come into the local police station.
And then, I called the victim helpline and I thought about it for a while and I thought, well, I just couldn’t imagine that this is a behaviour that somebody in his 60s would’ve suddenly developed. And if somebody else who had this done to them had reported it earlier, it wouldn’t have happened to me. And thereby, if I let it slide and something similar happened to somebody else …
I was actually extremely lucky that I didn’t crash my car on the way home and didn’t kill someone on the road or die myself.
Dissociation is a common response to trauma, and reduces the victim’s ability to think and respond appropriately. It also impacts on their ability to function professionally. In her victim impact statement, Dr Lee discussed how she had changed from being open and engaging to being quite withdrawn and isolated. It was difficult in this highly traumatised state to speak at all, let alone to report behaviour that is often experienced as shameful.
Limbo
In Australia, legal and organisational processes require prolonged periods of confidentiality, because court cases take many months and even years to be heard. Like other victims, Dr Lee had to endure many months of silence, isolation and self-doubt. Dr Lee managed to complete her training, but the trauma impacted her professional and personal life deeply.
Although Dr Lee had similar confusing reporting avenues to consider, the benzodiazepines she was given decided her course of action.
There was an obvious imbalance of power and I couldn’t help but feel small, (but) even if he was not found guilty, it might prevent him from hurting other women.
She did have support from friends, family and some senior colleagues, which was essential. No restrictions were placed on his medical licence until he pleaded guilty two years after the assault, leading to his suspension. It was not until 2019, over three years after his conviction, that he was finally deregistered.
When Dr Lee reflected on the situation, she commented on the expectation that she manage interpersonal conflict herself:
I think there are so many things along the way that could have gone wrong, so much more wrong than it did. I just didn’t think I could live with myself. It went beyond trying to protect myself and my line of work, because, obviously, you don’t want to be a trouble-maker and I’ve never been the sort of trainee to complain about things.
Exposure
Although Dr Lee chose to keep her name confidential in the court case, she was aware that many colleagues knew what had happened. That loss of anonymity and gossip were painful, and made her workplace feel quite unsafe. As a doctor who was used to having a high degree of control and agency, the lack of control over the perceptions of others was unsettling.
And I think one of the difficulties is that I feel like all the work that I put in during my medical career is ruined and now people are free to have an opinion about me based on this thing, and I have no control over that.
She was also deeply disturbed by the number of character references supplied by her colleagues for the perpetrator, even after he pleaded guilty to the assault.
On the trial day, the prosecutor asked me to go through the folder of – oh, it was huge – of character references, and tell me who I know and what I make of these people … One of them was written by a consultant who told me she feels terrible about what’s happened. I don’t know whether it’s poor judgement or a lack of information on how to handle these situations.
Aftermath
Dr Lee revealed that after the conviction, instead of feeling triumphant, she was engulfed by profound shame. She felt humiliated, believing that her own weaknesses had blinded her and made her vulnerable to being handpicked, groomed and victimised by a man she had trusted. Dr Lee found it difficult to re-establish her career and sense of self. She describes feeling vulnerable and exposed at work.
When I went back to work, I found myself hugging the walls because the floor no longer felt safe.
When she became a consultant herself, she questioned her role in supervising and mentoring junior staff. Do we teach in the hidden curriculum this sense of over compliance? Is professionalism about being unemotional, and in total control? Dr Lee sees her role as nurturing the next generation, arming them with the skills to self -protect. She is working on her biography, and continues to reflect on how this experience shaped her life as a doctor and a person.
The reason I went into medicine is to help people, and it’s not just inside a hospital or in your clinical room, if you see someone sick on the road, you will help. I think as doctors we have a duty to protect each other and patients. It’s a core thing that I can’t negotiate. A lot of people say to me oh, you’re really brave and lots of people wouldn’t have done what you’ve done, but to me, actually, there is no alternative.
Discussion
In 2014, when we first started working in this area, there was very little written about the issue of sexual harassment in medicine. Everything changed in 2015, when Gabrielle McMullin, an Australian vascular surgeon, launched her book on gender equity. (Reference McMullin and Matthews (ed.)60) In her speech at the launch, she discussed sexual harassment in her discipline of surgery. ‘What I tell my trainees is that, if you are approached for sex, probably the safest thing to do in terms of your career is to comply with the request’, she said, ‘If you complain … you’ll be exposed, you’ll be hung up to dry, you won’t be able to work … you absolutely would be seen as a liability moving forward.’ (Reference McMullin and Matthews (ed.)60)
Her comments sparked a cascade of disclosures, discussions, policy work and predictable outrage. (Reference Drummond61) There was fierce debate about the accuracy and advisability of her claims. ‘Of course I don’t condone any form of sexual harassment, and the advice that I gave to potential surgical trainees was irony’, Dr McMullin told the ABC, ‘but unfortunately that is the truth at the moment – that women do not get supported if they make a complaint’. (Reference Matthews62) The Royal Australian College of Surgeons initially denied the claims of sexual harassment in the profession, but soon pivoted to a public apology and a sustained campaign of education and policy reform they called ‘Operating with Respect’. (Reference Coopes63–65)
Almost a decade later, the impact of that intervention is still debated. There continues to be confusion around appropriate professional behaviour, interactions and approaches to teaching within surgical departments, (Reference Lim34) and surgery remains a highly gendered profession. (Reference Pascoe36) Dr Rhea Liang is a well-known voice for equity in the surgical profession, and has written extensively about the lived experience of being a woman surgeon, and sharing a conversation with female surgeons at a conference. ‘It is a privilege to be ordinary in a space’, she says. ‘To be ordinary means to be so normalised that it does not require additional comment. To belong so much that work arrangements are fashioned to fit around your needs and not those of a different, stereotyped norm.’ (Reference Liang, Anthony and Leditschke68; Reference Liang69) Lockhart and Blatt are much more blunt in their comments on women surgeons. ‘We have cracked the ceiling’, they say ‘but how long must we walk on broken glass?’ (Reference Lockhart and Blatt70)
Of course, sexual harassment in medicine is not limited to surgery or to women, and studies have now been performed on a number of disciplines within Australia. (Reference Braid71–Reference Herweck73) They make for sobering reading. But whenever we present our work on sexual harassment in medicine, we have been surprised that the same questions keep rising to the surface. Why is there so much silence around this issue? How can it be occurring in the light of day in our medical institutions? And why do survivors not report this criminal behaviour?
As we present this work in various forums, we have an extraordinary split experience. Survivors come to us, or write to us and tell us quietly about sexual abuse that occurred two or twenty or even fifty years ago that they have never disclosed. They thank as for our work and reveal how profoundly damaging the abuse has been, both personally and professionally. At the same time, senior members of our profession who are good, committed teachers, clinicians and leaders ask why it is that survivors don’t report the abuse. If they don’t tell us, they say, how can we possibly change this behaviour?
We believe there are several reasons for the silencing of survivors.
Cumulative Microaggressions: ‘We’re Just Too Used To It’
Junior doctors learn in a hierarchy and are expected to be compliant with the needs of the team. Many junior doctors, particularly those who live with intersectional disprivilege, learn to tolerate sexist and racist microaggressions, from the profession, their multidisciplinary colleagues and the community. (Reference Herweck73–Reference Wheeler76) In this environment, it is unsurprising that junior doctors can become tolerant of unacceptable conduct. It is also understandable that managing repeated microaggressions leaves less cognitive and emotional capacity for recognising and responding to harassment. (Reference Wheeler76) International Medical Graduates in Australia practise under a moratorium, which binds them to a decade of service in an underserved community. (Reference Healey, Fakes and Nair21–23) It is highly unlikely that an IMG will risk a complaint when their visas are dependent on their supervisors, their college or hospital, the Medical Board and the Australian Government.
The Role of Invalidation and Shame
Doctors are also part of a community, and the community continues to blame survivors for their own trauma. Rape myths invalidate survivor experiences, minimising the impact of trauma, and leading to underreporting of sexual harassment. (77–78) It is surprisingly difficult to break the perception that rape only happens to those who ‘deserve’ it, due to their choice of clothing, behaviour, location or even their body types. (77–78) These myths are pervasive, and are reinforced in the media, (79) the courts (80) and the broader social world. (81–82) The recent treatment of Brittany Higgins, who was sexually assaulted in our Australian Parliament House, has provided a clear warning for survivors. Being a survivor, and making a story public, comes with deep personal and reputational consequences that can destroy personal and professional wellbeing.
For a survivor in medicine, rape myths cause cognitive dissonance. Doctors are privileged, and therefore do not fit the public image of either a survivor or a perpetrator. Whenever we present this work, we inevitably face the question, ‘How can sexual harassment occur in the cold, hard light of day in a busy hospital?’, closely followed by a suggestion that young doctors may benefit from resilience training. The narratives that survivors are ‘sensitive snowflakes’ (Reference Haslop, O’Rourke and Southern83) who misinterpret the behaviour of their senior colleagues is often matched with a similar narrative that perpetrators are merely ‘bad apples’ and therefore should be managed individually. Thinking this way means they see no need for systemic change. (Reference Searle84)
Career Impact: ‘Does Anyone Ever Report These Things and Come Out on Top?’
Sexual abuse in the medical profession is not just a personal trauma, it is also a professional betrayal. When the workplace, the courts, the colleges or the collegiate community fail to respond appropriately, the personal trauma of sexual abuse is compounded by institutional betrayal that threatens recovery. (85–87) In the last ten years, there has been a concerted effort by Australian colleges, universities, hospitals and the Medical Board to address the issue of sexual harassment. Most now have policies and processes in place for reporting.
The Australian Human Rights Commission recently published their landmark report, Respect@work, (85) and it is this report that led to positive changes in national legislation. (Reference Nawaz86) Australian law now requires that all workplaces have a positive duty to report, ensuring hospitals, universities and other medical workplaces comply with the Sex Discrimination Act around sexual safety at work.
However, reporting sexual abuse in medicine has profound consequences, since young doctors rely on senior colleagues for support. Like the military, the hierarchy of medicine diminishes the likelihood of reporting abuse. (87) Young doctors fear ‘whistleblowing’, feeling it may bias fair assessment for training, and also their continued access to collegiate networks that will sustain their careers in the longer term. (87–88) There is also confusion about the process of reporting. Sexual abuse in the workplace is managed by a series of institutions with overlapping roles and responsibilities (89–90).
It is unrealistic to expect a junior doctor to navigate this complexity. In our study, we found time and time again that there was a difference between written policies and expected behaviour, so survivors distrust the institutional response to reporting. (Reference Healey, Fakes and Nair21; 50; Reference Braid71; 90) The anti-harassment posters on the walls reflect a law that is not always enforced, and the written policies around the reporting of abuse do not always reflect what they see happening in their working environments.
Personal Impact: ‘My World Is Broken and Will Never Be the Same’
In our study, we found that participants not only experience personal trauma, but they also experience a profound shift in their world view and their professional identity. Such a shift is likely to junior doctors to lose confidence and agency. The cost of a court case is also prohibitive for a junior doctor, especially as the hope of a successful outcome is slim. The risk of re-traumatising is high. Many doctors reflect the views of Judge Madgwick when sentencing a person for sexual assault: he described the victim as a ‘heroine of fortitude’ for surviving the hearing. (89) Many women believe that taking a sexual assault to court provides no benefit to the victim, even if it may forward the cause of justice for others by serving as a deterrent. Taking a case to court involves surviving ‘a theatre of shame’. (90)
Betrayal Blindness: ‘Was It Really Abuse?’
Betrayal trauma theory suggests that underreporting may also be linked to a purposeful, if unconscious, method of ‘not-knowing’. (91) Freyd and colleagues found that a close and dependent relationship between the perpetrator and victim predicted memory impairment for physical and sexual abuse. (92) After abuse, betrayal trauma theory suggests that victims may dissociate to maintain important relationships, by unconsciously not-knowing about information that would threaten it. (92; 93) Victims who have survived childhood trauma are more likely to suffer betrayal trauma and are more likely to dissociate, (93) reducing their capacity to register and respond to betrayal. (94; 95) Given prevalence estimates of 8–31% for girls, (96) it is likely that some victims of sexual trauma in medicine are also survivors of childhood trauma. In betrayal trauma, ‘the best way to keep a secret is not to know it in the first place; unawareness is a powerful survival technique when information is too dangerous to know’. (Reference Walton29)
‘Betrayal blindness’ can also be experienced by bystanders. This may involve consciously pretending not to know to avoid consequences in social relationships (the ‘Emperor’s New Clothes’ phenomenon) or may mean that bystanders remain truly unaware of the trauma. Bystander blindness protects the bystander by helping them avoid seeing and responding to risk. Acknowledging trauma threatens their own interpersonal, physical and moral security. (97)
Betrayal trauma has also been linked to poorer outcomes in mental health, including depression, anxiety, and PTSD. (98) This is particularly evident when institutions fail to protect victims or negatively respond to them. Therefore, it is essential that we understand how both abuse and betrayal influence the narratives of victims of sexual abuse in the medical profession – their understanding of causative factors, their initial response to the trauma, their experience of suffering, their decisions around reporting, and their longer term recovery. Survivors may not report because they genuinely have been consciously and unconsciously silenced. (99)
In Australia, the importance of bystanders was raised by the military. In 2013, an investigation was launched into sexual violence and gendered abuse in the Army. (100) The Chief of Army, Lieutenant General David Morrison gave a powerful speech that is still cited as a turning point in the national consciousness around sexual harassment and gendered workplace relations. Morrison was already known for his stance on gender equity, and this speech was written by his speech writer, Lieutenant Colonel Cate McGregor, who is transgender.
The speech was a masterclass in cultural leadership, with a visibly angry Morrison delivering a powerful directive. The most quoted phrase from this speech is the call to bystanders, where he stated, ‘the standard you walk past is the standard you accept’. However, there are other important messages in this speech that shaped not only the dialogue around sexual harassment, but also the role of men and male leaders in particular in eradicating it.
I have stated categorically, many times, that the Army has to be an inclusive organisation, in which every soldier, man and woman, is able to reach their full potential and is encouraged to do so. Those who think that it is ok to behave in a way that demeans or exploits their colleagues, have no place in this army …
If that does not suit you … then get out!!
You may find another employer where your attitude and behaviour is acceptable, but I doubt it. The same goes to those who think toughness is built on humiliating others.
Every one of us is responsible for the culture and reputation of our army and the environment in which we work. If you become aware of any individual degrading another, then show moral courage and take a stand against it.
I will be ruthless in ridding the army of people who cannot live up to it’s values … The standard you walk past is the standard you accept. That goes for all of us, but especially those, who by their rank, have a leadership role.
If we are a great national institution, if we care about the legacy left to us by those who have served before us, if we care about the legacy we leave to those who, in turn will protect and secure Australia, then it is up to us to make a difference. If you’re not up to it, find something else to do with your life. There is no place for you among this band of brothers and sisters.
Restorative Justice
Institutional trauma needs institutional healing. Part of this healing involves understanding and responding to failures in the system that contribute to vulnerability. In 2023, we held an Australasian Summit on sexual harassment in medicine, and focused on the trajectory of health promotion, from primary to quaternary prevention.
Australia has made a significant effort over the last ten years to eradicate sexual harassment, but the problem undoubtedly persists. In medicine, the greatest weapon a perpetrator has is the tendency of the survivor to shut down and be silenced. Until we understand how to enable the survivor to speak, we suspect the behaviour will continue, perhaps in more subtle ways that are difficult to challenge.

 Open access
Open access