


Introduction
Anxiety disorders are the most common mental health condition among children and adolescents, with a global prevalence of 6.5% (Polanczyk et al., Reference Polanczyk, Salum, Sugaya, Caye and Rohde2015), and cause problems with low self-esteem and social and academic performance in this population (de Lijster et al., Reference de Lijster, Dieleman, Utens, Dierckx, Wierenga, Verhulst and Legerstee2018; Peñate et al., Reference Peñate, González-Loyola and Oyanadel2020). Furthermore, research suggests that anxiety disorders are highly co-morbid with major depression and alcohol/substance use disorders, which can severely reduce quality of life (Bartoli et al., Reference Bartoli, Carretta and Carrà2021; Kalin, Reference Kalin2020). Anxiety disorders are preventable, and taking a preventative approach is both advantageous for enhancing children and adolescents’ mental health and cost-effective (Andrews and Wilkinson, Reference Andrews and Wilkinson2002). Considering these outcomes, the significance of early intervention in anxiety disorders during childhood and adolescence has been emphasised.
Childhood and adolescence are periods of heightened environmental sensitivity when individuals are especially susceptible to negative parental influence (Lionetti et al., Reference Lionetti, Klein, Pastore, Aron, Aron and Pluess2022; Pluess, Reference Pluess2015). Numerous studies elucidate parents’ role in the development of anxiety in children and adolescents. For example, frequent inter-parental conflict and parental over-involvement can increase the likelihood that children will experience anxiety problems (Lei et al., Reference Lei, Wang, Wan, Patel and Li2023; Yap et al., Reference Yap, Pilkington, Ryan and Jorm2014). Over-protective and coercive parental attitudes can also play a crucial role in increasing children’s anxiety (Laurin et al., Reference Laurin, Joussemet, Tremblay and Boivin2015). Furthermore, research shows that pediatric anxiety disorders have an intergenerational effect, as children with anxious parents are twice as likely to experience anxiety as those with non-anxious parents (Lawrence et al., Reference Lawrence, Murayama and Creswell2019). Anxious parents frequently demonstrate reduced autonomy, more criticism, and decreased warmth in their interactions with their children (Ballash et al., Reference Ballash, Leyfer, Buckley and Woodruff-Borden2006); however, research suggests that parental warmth can mitigate children’s anxiety symptoms by reducing their brain responses to criticism (Butterfield et al., Reference Butterfield, Silk, Lee, Siegle, Dahl, Forbes and Ladouceur2021). Therefore, to successfully alleviate children’s and adolescents’ anxiety, changes in parents’ attitudes and behaviours and active parental involvement are important to encourage.
Although anxiety disorders are common among children and adolescents, many do not receive treatment (Ghandour et al., Reference Ghandour, Sherman, Vladutiu, Ali, Lynch, Bitsko and Blumberg2019). Reasons why children and adolescents and their families do not seek professional help for mental health issues include a lack of time and cost barriers (Horwitz et al., Reference Horwitz, Storfer-Isser, Kerker, Szilagyi, Garner, O’Connor and Stein2015; Rowan et al., Reference Rowan, McAlpine and Blewett2013). In addition, fear of negative social consequences often makes it difficult for children and adolescents to disclose their issues to others, while the parents of such children may also face stigmatisation (Hansen et al., Reference Hansen, Telléus, Mohr-Jensen and Lauritsen2021; Radez et al., Reference Radez, Reardon, Creswell, Orchard and Waite2021). Interventions delivered through the internet can help address these problems and close the gap in service use. Internet-delivered interventions reduce wait times and are not restricted to a particular physical place. Moreover, concerns over stigma can be allayed by the assured anonymity and remote accessibility. Research has demonstrated that internet-based interventions can be a successful therapeutic approach for mitigating anxiety in young patients (Domhardt et al., Reference Domhardt, Steubl and Baumeister2018; Khanna and Carper, Reference Khanna and Carper2022).
Research on alleviating anxiety symptoms in children and adolescents emphasises parental participation, and interventions provided using internet technology are increasingly being studied. Previous reviews have considered research on parent-involved and parent-only interventions for childhood and adolescent anxiety (Cardy et al., Reference Cardy, Waite, Cocks and Creswell2020; Jewell et al., Reference Jewell, Wittkowski and Pratt2022). According to previous studies, interventions that directly target anxiety symptoms, such as training parents to manage their child’s anxiety and apply these techniques, have been found to be effective (Lebowitz et al., Reference Lebowitz, Marin, Martino, Shimshoni and Silverman2020; Yin et al., Reference Yin, Teng, Tong, Li, Fan, Zhou and Xie2021). In contrast, the effectiveness of interventions focusing on general parenting strategies and the home environment remains inconclusive. For example, one study indicated that while such interventions may be effective in improving parenting behaviours and family functioning, they did not produce significant changes in adolescent mental health outcomes. Another study highlighted the need for further research to validate the effectiveness of these parenting strategy programs (Fulgoni et al., Reference Fulgoni, Melvin, Jorm, Lawrence and Yap2019; Khor et al., Reference Khor, Fulgoni, Lewis, Melvin, Jorm, Lawrence and Yap2022). Building on this trend, internet-delivered interventions have gained increasing attention, with studies providing evidence of their effectiveness in treating anxiety in children and adolescents (Eilert et al., Reference Eilert, Wogan, Leen and Richards2022). Internet-delivered parent-led interventions emphasise the active role of parents while also offering the potential to enhance treatment accessibility.
However, there are currently very few reviews on internet-delivered, parent-led interventions for anxiety in children and adolescents. Grajdan et al. (Reference Grajdan, Etel, Farrell and Donovan2025) examined the impact of parental involvement in cognitive behavioural therapy (CBT) interventions. In their review, studies were included even when parents participated in only a single session. In contrast, the present review focuses on interventions in which parents take the lead and play an active role throughout the program. Furthermore, this review extends beyond CBT to explore a broader range of parent-led, internet-delivered programs, aiming to better understand the characteristics and effectiveness of these interventions. This study offers a valuable perspective by clearly distinguishing between limited parental involvement and parent-led approaches, and by evaluating the effectiveness of the latter. It examines the potential of parent-led internet-delivered interventions as accessible and flexible treatment options in contexts where access to services is limited, child engagement is low, or parental factors play a significant role.
Accordingly, this review aims to examine studies on the effects of internet-delivered parent-led interventions on anxiety in children and adolescents. It also explores whether these interventions can effectively reduce anxiety symptoms in children and adolescents while minimising therapist time and direct involvement. Specifically, it investigates the effectiveness of internet-delivered, parent-led interventions by classifying them based on intervention type, whether telephone consultation with a therapist is included, parental change measurements used, and treatment completion rate.
Method
Searches
All searches were limited to publications published between 2013 and 2024. To reflect the significant increase in both the number of studies and research interest in internet-delivered parent-led interventions, this study focused on studies published from 2013 onwards. While there were some studies prior to 2013, research on both internet-delivered interventions and parent-led approaches was quite limited before this period. However, around 2013, there was a noticeable increase in research on the use of digital technologies for delivering health services (Hollis et al., Reference Hollis, Morriss, Martin, Amani, Cotton, Denis and Lewis2015), which aligns with the focus of the present study. Therefore, the search was limited to studies published from 2013 onwards to capture the most relevant research trends in internet-delivered, parent-led interventions. Electronic database searches were conducted using PubMed, PsycArticles, Cochrane Library, and Google Scholar. The searches included studies conducted in various countries and reported in English. The search strategy was constructed using a combination of keywords categorised into five domains. The approach included the following search terms:
(a) child OR adolescent OR infant OR teen OR youth OR preschool;
(b) anxiety OR ‘anxiety disorder’ OR phobia OR ‘specific phobia’ OR ‘panic disorder’;
(c) ‘parent led’ OR ‘parent based’ OR ‘parent focused’ OR ‘parent guided’ OR ‘parent training’ OR ‘parent mediated’ OR ‘parent particip*’ OR ‘parent involve*’ OR ‘parent coached’ OR ‘parent manage*’ OR ‘parent engage*’ OR parenting;
(d) ‘internet-delivered’ OR ‘web based’ OR online;
(e) intervention OR program OR education OR therapy OR treatment.
These terms were combined using Boolean operators (AND, OR) to construct a range of search strings, such as ‘child AND anxiety AND parent-led AND internet delivered AND intervention’. To focus specifically on parent-led internet-delivered interventions targeting anxiety in children and adolescents, the study used a restricted set of search terms, and MeSH terms were not used in the search strategy. A publication date filter was applied to restrict the search to studies published after January 2013. Although some grey literature may have been identified in the initial search, only published, peer-reviewed papers were included in the final selection.
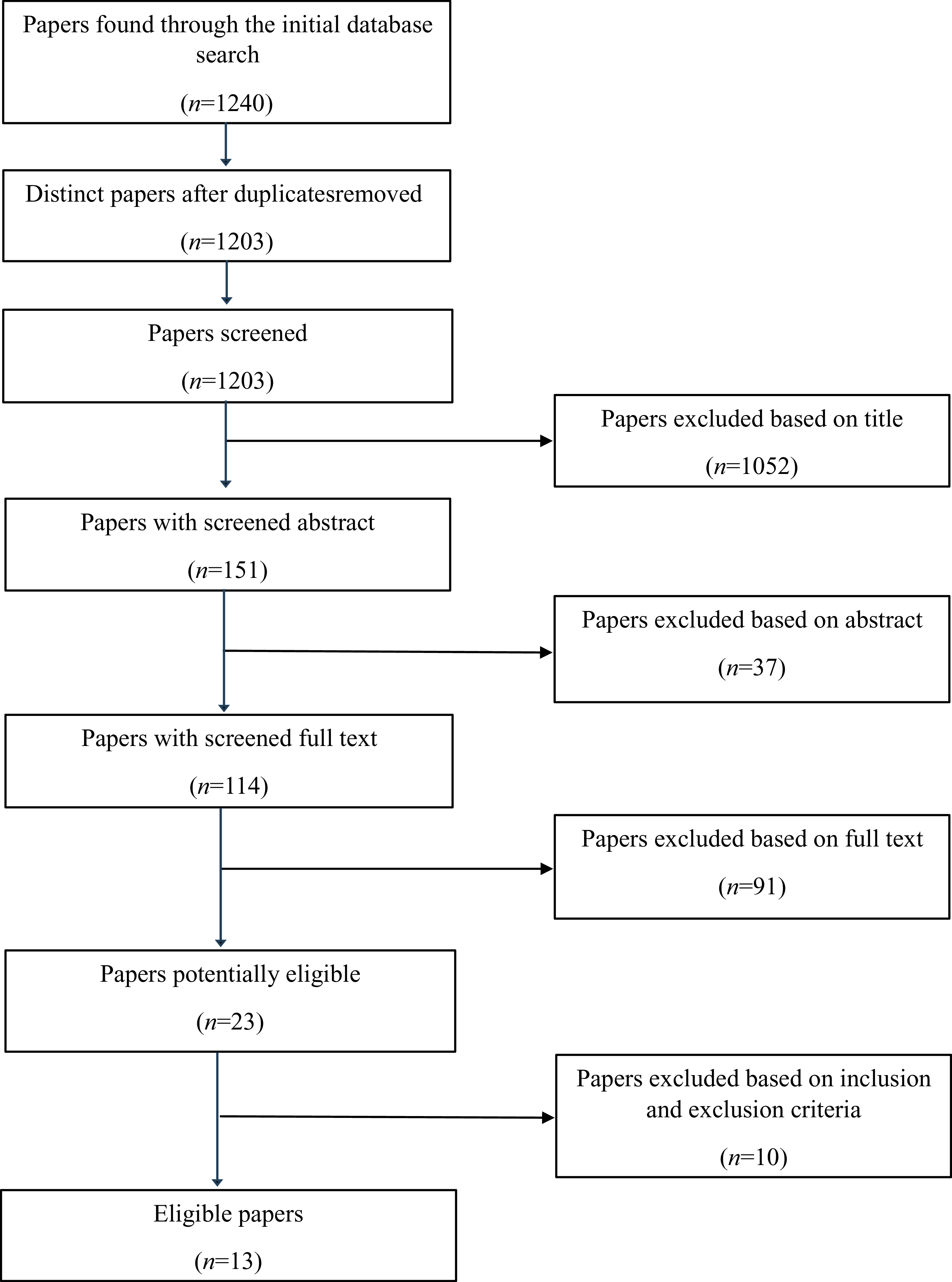
Zotero software was used to organise and screen references. All stages of the review process, including title and abstract screening, full-text review, and data extraction, were conducted independently by two reviewers (S.K. and H.S.K.). The second rater independently screened all records identified through the database searches (n=1240). Inter-rater agreement at the screening stage was assessed using Cohen’s kappa and demonstrated high agreement (κ=0.93). Data extraction was also conducted independently by two reviewers, with high inter-rater agreement for key categorical extraction variables (e.g. intervention type and comparator). Any discrepancies were resolved through discussion until consensus was reached. Additionally, the references listed in papers that met the inclusion criteria were manually searched and closely scrutinised to identify additional studies. The comprehensive searches were completed on 7 April 2024. This review was not pre-registered in any publicly accessible database. The literature search resulted in 13 papers meeting the inclusion criteria from the 1240 papers initially identified through the electronic database search. Due to substantial differences among the included studies in terms of intervention types, outcome measurement methods, and baseline anxiety levels of participants, it was deemed inappropriate to statistically integrate the findings. Therefore, a narrative synthesis was employed to qualitatively compare the characteristics and effects of the interventions. Figure 1 displays a flowchart showing the search and selection procedure.
Flowchart of displaying the search and selection procedure.

Study selection
The selected studies included research on parent-led interventions provided via the internet for anxiety in children and adolescents. Parent-led interventions were defined in this review as those with goals that involved changing parents’ knowledge, attitudes, and behaviours while also helping them apply what they had learned to their children. In addition, the number of intervention modules targeting parents should be equal to or greater than those targeting children and adolescents. Furthermore, the studies needed to meet the following requirements to be considered for inclusion in the review: (a) the goal of the intervention was to reduce anxiety in children or adolescents; (b) at least one parent of a child or adolescent under 18 years of age experiencing anxiety problems participated in the intervention directly, with or without the children or adolescents also participating; (c) the intervention content led to changes in parental knowledge, attitudes, and behaviours and provided strategies and skills parents could apply with their children; (d) the number of parental modules in the intervention matched or exceeded that of the modules designed for children or adolescents; (e) the primary intervention content was required to be delivered entirely online, and the core intervention did not include face-to-face interactions or offline content; (f) the outcomes of children or adolescents included changes in anxiety levels or diagnosis status; (g) the study included quantitative outcome data assessing the effects of the intervention.
The exclusion criteria were as follows: (a) the intervention targeted anxiety reduction in children or adolescents in specific disability groups such as those with autism spectrum disorder (ASD) and attention deficit hyperactivity disorder (ADHD); (b) other caregivers such as grandparents or relatives were the primary participants rather than at least one parent; (c) face-to-face elements were incorporated into an internet-delivered intervention; (d) focus was on changes in parents’ mental health symptoms, such as alleviating parent anxiety; and (e) no measurement results were provided for child anxiety.
Risk of bias assessment
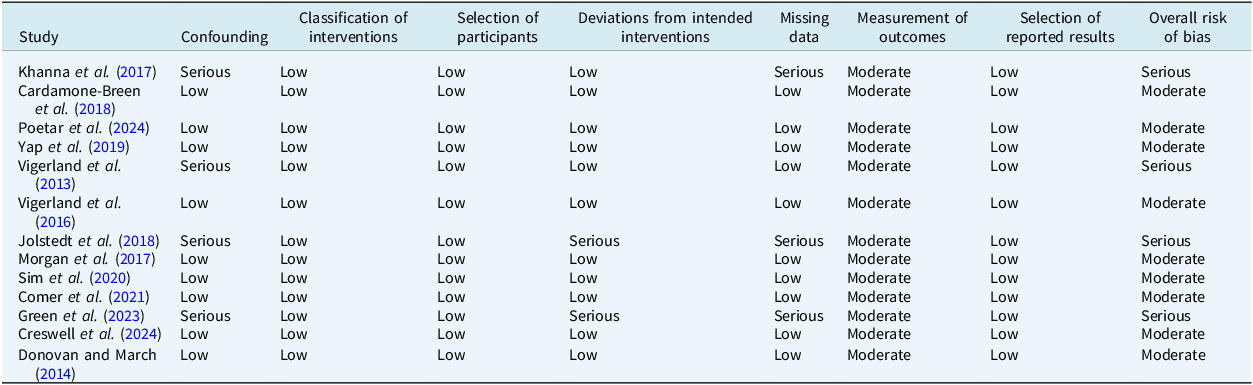
The risk of bias in the included studies was independently assessed by a single reviewer using the ROBINS-I-V2 tool. The tool evaluates the risk of bias across seven domains: confounding, classification of interventions, selection of participants, deviations from intended interventions, missing data, measurement of outcomes, and selection of reported results. Each domain is rated as having low, moderate, serious, or critical risk of bias. Overall risk of bias for each study was determined by the highest risk rating across the seven domains (Sterne et al., Reference Sterne, Hernán, Reeves, Savović, Berkman, Viswanathan and Higgins2016).
Results
Study characteristics
A total of 13 studies were ultimately included. Across the 13 studies, five were conducted in Australia, three in Sweden, two in the United Kingdom, two in the United States, and one in Romania. Sample sizes ranged from 19 parents and 19 children and adolescents to 443 parents and 443 children/adolescents. Parents’ mean age ranged from 35.9 to 45.2 years, while children and adolescents’ mean age ranged from 4.1 to 13.7 years. The interventions varied in duration from 3 weeks to 6 months. The total number of modules ranged from 7 to 24, with the average being 10.6. Ten studies only included parent modules, with intervention content delivered only to parents. A total of four studies used active control conditions. Among them, three used bibliographic materials or educational factsheets, while the remaining study used treatment as usual. Most studies included follow-up assessments, with time points ranging from 3 months to 12 months after the intervention. The most commonly reported follow-up period was 3 months, with several studies also including longer-term assessments at 6 or 12 months. Table 1 provides a detailed summary of the characteristics of the 13 studies.
Summary of study characteristics

CSQ, Client Satisfaction Questionnaire; CEQ, Computer Experience Questionnaire; CBCL-A, Child Behavior Checklist-Anxiety Subscale; SCAS-P, Spence Children’s Anxiety Scale-Parent Version; PRADAS-A, Parenting to Reduce Adolescent Depression and Anxiety Scale-Adolescent; SMFQ, Short Mood and Feelings Questionnaire; SDQ-P, Strengths and Difficulties Questionnaire-Parent Version; PSES, Parental Self-Efficacy Scale; SCAS-C, Spence Children’s Anxiety Scale-Child Version; CSR, Clinician Severity Rating; CGAS, Children’s Global Assessment Scale; FSSC-R C/P, Fear Survey Schedule for Children-Revised-Child Version and Parent Version; QOLI-C, Quality of Life Inventory-Child Version; CSS, Client Satisfaction Scale; CDI, Child Depression Inventory; ADIS-C/P, Anxiety Disorders Interview Schedule for Children and Parents; SAI-C, Separation Anxiety Inventory for Children; SPAI-C/P, Social Phobia and Anxiety Inventory for Children/Parents; PSWQ-C, Penn State Worry Questionnaire for Children; CGI-S/I, Clinical Global Impression-Severity/Improvement; CSDS, Child Sheehan Disability Scale; STSC, Short Temperament Scale for Children; PAS-R, Preschool Anxiety Scale-Revised; OAPA, Online Assessment of Preschool Anxiety; CALIS, Children’s Anxiety Life Interference Scale; OI/P, Over-Involved/Protective Parenting Scale; K10, Kessler 10 Psychological Distress Scale; PaRCADS, Parenting to Reduce Child Anxiety and Depression Scale; RCADS, Revised Child Anxiety and Depression Scale; CRPBI, Children’s Report of Parent Behavior Inventory; PCS, Psychological Control Scale; CHU9D, Child Health Utility 9D; AQoL-8D, Assessment of Quality of Life-8 Dimensions; GF, General Functioning Subscale; CBQ, Parent-report Children’s Behavior Questionnaire Short Form; CAIS, Child Anxiety Impairment Scale; DASS-21, Depression, Anxiety, Stress Scale-21-item version; FASA, Family Accommodation Scale-Anxiety; CORS, Child Outcome Rating Scale; GBO, Goal Based Outcome; EQ-5D-5L-P, EuroQol-5 dimensions, 5 levels; RCADS-P/C, Parent/Child-reported Child Anxiety Symptoms. CBCL-Int, Child Behaviour Checklist (1.5-5)-Internalising Subscale.
Risk of bias assessment
The overall risk of bias across the included studies was mostly moderate, with serious risk identified only in a few specific domains across four studies. All studies were assessed as having low risk of bias in the domains of classification of interventions, Selection of participants, and Selection of reported results. A detailed summary of the risk of bias assessment is provided in Table 2.
Risk of bias assessment

Psychological outcomes
More than two-thirds of the studies (n=9) reported finding a significant intervention effect (Comer et al., Reference Comer, Furr, Del Busto, Silva, Hong, Poznanski and Puliafico2021; Creswell et al., Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024; Donovan and March, Reference Donovan and March2014; Green et al., Reference Green, Reardon, Button, Williamson, Halliday, Hill and Creswell2023; Jolstedt et al., Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018; Morgan et al., Reference Morgan, Rapee, Salim, Goharpey, Tamir, McLellan and Bayer2017; Poetar et al., Reference Poetar, Dobrean and Andersson2024; Vigerland et al., Reference Vigerland, Thulin, Ljotsson, Svirsky, Öst, Lindefors and Serlachius2013; Vigerland et al., Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016), reporting improvements in anxiety symptoms in children and adolescents in the intervention group. One study demonstrated that the internet-delivered parent-led intervention was not inferior to treatment as usual (Creswell et al., Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024).
Parent-rated child/adolescent anxiety outcomes
In all the studies, parents assessed the anxiety symptoms of the children or adolescents. The most widely used measurement was the parent version of the Spence Children’s Anxiety Scale (SCAS-P; Spence, Reference Spence1998), which was used in six studies. In Poetar et al. (Reference Poetar, Dobrean and Andersson2024), the intervention group showed significantly greater improvements in parent-reported child anxiety symptoms compared with the control group, with a large effect size. Vigerland et al. (Reference Vigerland, Thulin, Ljotsson, Svirsky, Öst, Lindefors and Serlachius2013) showed that parent-reported improvements in child anxiety symptoms were observed after the intervention and were maintained at follow-up. Vigerland et al. (Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016) found that parents reported significantly lower symptoms of child anxiety in the intervention group than in the waitlist control (WLC) group. Jolstedt et al. (Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018) reported substantial reductions in child anxiety symptoms with large effect sizes across all parent-reported measures. In Morgan et al. (Reference Morgan, Rapee, Salim, Goharpey, Tamir, McLellan and Bayer2017), the intervention group showed greater improvements in anxiety symptoms, with small-to-moderate effect sizes, and a higher number of children who did not meet the criteria for anxiety disorder after showing significant improvement. In Comer et al. (Reference Comer, Furr, Del Busto, Silva, Hong, Poznanski and Puliafico2021), not only did parent-evaluated anxiety symptoms in children decrease significantly, but 60% of the children were classified as responders at 6-month follow-up. Green et al. (Reference Green, Reardon, Button, Williamson, Halliday, Hill and Creswell2023) reported substantial changes throughout the measurements made during the intervention, and the intervention was effective in alleviating children’s anxiety symptoms. Creswell et al. (Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024) reported that an internet-delivered parent-led intervention was as effective as other treatments in decreasing parent-reported anxiety symptoms in children. Donovan and March (Reference Donovan and March2014) found that parents in the intervention group reported greater reductions in their children’s clinical anxiety over time compared with the WLC group. In Cardamone-Breen et al. (Reference Cardamone-Breen, Jorm, Lawrence, Rapee, Mackinnon and Yap2018), parent-reported anxiety symptoms in children decreased over time; however, no significant differences were observed between groups. Sim et al. (Reference Sim, Fernando, Jorm, Rapee, Lawrence, Mackinnon and Yap2020) also showed a decrease in children’s anxiety symptoms over time in both groups. Yap et al. (Reference Yap, Cardamone-Breen, Rapee, Lawrence, Mackinnon, Mahtani and Jorm2019) found no significant intervention effect on parent-reported anxiety symptoms in adolescents. In Khanna et al. (Reference Khanna, Carper, Harris and Kendall2017), SCAS-P scores increased over time in the bibliotherapy, WLC, and intervention groups, while Child Behavior Checklist scores showed inconsistent results, decreasing in all three groups.
Child/adolescent-rated child/adolescent anxiety outcomes
Seven studies included anxiety symptoms reported by children or adolescents. The child version of the SCAS (Spence, Reference Spence1998) was applied in five studies, making it the most widely used measurement. Vigerland et al. (Reference Vigerland, Thulin, Ljotsson, Svirsky, Öst, Lindefors and Serlachius2013) reported that 35% of the children no longer met the criteria for a specific phobia diagnosis according to a self-reported measure of children’s anxiety symptoms. Of the children in Vigerland et al. (Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016), 20% no longer satisfied their principal diagnostic criteria after treatment, which increased to 50% in follow-up. Jolstedt et al. (Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018) also showed a significant improvement in children’s self-reported anxiety symptoms; 68% of the children reported no longer meeting diagnostic criteria at 3-month follow-up. Creswell et al. (Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024) showed that the studied intervention was as effective as other treatments for children’s anxiety symptoms as shown in children’s self-report measurements. Cardamone-Breen et al. (Reference Cardamone-Breen, Jorm, Lawrence, Rapee, Mackinnon and Yap2018) found no significant intervention effect on children’s self-reported anxiety symptoms. Sim et al. (Reference Sim, Fernando, Jorm, Rapee, Lawrence, Mackinnon and Yap2020) reported similar patterns in parent-reported and self-reported anxiety symptoms in children, resulting in no significant intervention effect. Yap et al. (Reference Yap, Cardamone-Breen, Rapee, Lawrence, Mackinnon, Mahtani and Jorm2019) found no intervention effects based on children’s self-reported anxiety symptoms, which were similar to those reported by their parents.
Directly vs indirectly targeting child anxiety
Most studies (n=10) directly addressed anxiety in children or adolescents. Educating parents to effectively manage anxiety in children or adolescents, empowering them to support their children, and enabling them to provide direct training to children or adolescents based on what they learned were the main components of the intervention (Comer et al., Reference Comer, Furr, Del Busto, Silva, Hong, Poznanski and Puliafico2021; Creswell et al., Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024; Donovan and March, Reference Donovan and March2014; Green et al., Reference Green, Reardon, Button, Williamson, Halliday, Hill and Creswell2023; Jolstedt et al., Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018; Khanna et al., Reference Khanna, Carper, Harris and Kendall2017; Morgan et al., Reference Morgan, Rapee, Salim, Goharpey, Tamir, McLellan and Bayer2017; Poetar et al., Reference Poetar, Dobrean and Andersson2024; Vigerland et al., Reference Vigerland, Thulin, Ljotsson, Svirsky, Öst, Lindefors and Serlachius2013; Vigerland et al., Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016). Parents received various types of anxiety-related education mainly on the nature and symptoms of anxiety, guiding principles or core components of CBT, psychoeducation and training in exposure techniques, the use of coping skills, and strategies to overcome and manage barriers. Less than one-quarter of the studies (n=3) provided interventions to evaluate parenting styles and improve parenting environments accordingly, rather than teaching skills to understand, resolve, and cope with anxiety in children (Cardamone-Breen et al., Reference Cardamone-Breen, Jorm, Lawrence, Rapee, Mackinnon and Yap2018; Sim et al., Reference Sim, Fernando, Jorm, Rapee, Lawrence, Mackinnon and Yap2020; Yap et al., Reference Yap, Cardamone-Breen, Rapee, Lawrence, Mackinnon, Mahtani and Jorm2019). In these three studies, parents completed a parenting scale evaluating current caregiving beliefs and practices to reduce anxiety in children and adolescents and subsequently received individually tailored feedback reports. The feedback reports focused on content such as their relationships with their children, continued interest and participation in their children’s lives, managing conflicts with their children, and encouraging good habits for their mental health, emphasising their current parenting strengths and areas of improvement.
Telephone calls for clinical consultation support
The majority of studies (n=8) provided parents with support using telephone consultations from therapists or psychologists. Telephone calls to simply encourage participation or consultations without individual treatment support were not included. Six studies included telephone sessions with therapists as an essential component of the intervention. Vigerland et al. (Reference Vigerland, Thulin, Ljotsson, Svirsky, Öst, Lindefors and Serlachius2013) and Vigerland et al. (Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016) provided each family with three telephone calls from therapists at the beginning, middle, and end of their treatment. Telephone calls were conducted for feedback, prompts, and task-related Q&A and encouragement during the exposure focus week. In Vigerland et al. (Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016), additional telephone calls were provided if it was determined that more telephone calls were needed to help solve the problem. Donovan and March (Reference Donovan and March2014) provided parents with telephone consultations lasting between 15 and 30 minutes with therapists during the exposure hierarchy phase to support intervention process. In Green et al. (Reference Green, Reardon, Button, Williamson, Halliday, Hill and Creswell2023) and Creswell et al. (Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024), parents received a telephone call from a therapist lasting approximately 20 minutes for each online module. Weekly telephone calls with therapists provided parents with support to better apply and customise their interventions. In Comer et al. (Reference Comer, Furr, Del Busto, Silva, Hong, Poznanski and Puliafico2021), interventions utilised webcam sessions where therapists provided remote live coaching to parents using Bluetooth earpieces. Parents broadcast real-time interactions with their children via webcam, enabling therapists to provide live guidance. based on these interactions. In two studies, parents were able to call a therapist when needed by asking for telephone support (Jolstedt et al., Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018; Morgan et al., Reference Morgan, Rapee, Salim, Goharpey, Tamir, McLellan and Bayer2017). In Jolstedt et al. (Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018), parents and therapists were mainly in contact through messages or worksheet comments within the program; however, telephone calls were also provided when necessary. In Morgan et al. (Reference Morgan, Rapee, Salim, Goharpey, Tamir, McLellan and Bayer2017), support calls were provided to assist with psychoeducation, technical practice, and the design and implementation of stepladders for addressing common difficulties.
Parental transition
Fewer than half of the studies (n=6) measured parent-related changes. Three of the studies measured changes in parenting (Cardamone-Breen et al., Reference Cardamone-Breen, Jorm, Lawrence, Rapee, Mackinnon and Yap2018; Sim et al., Reference Sim, Fernando, Jorm, Rapee, Lawrence, Mackinnon and Yap2020; Yap et al., Reference Yap, Cardamone-Breen, Rapee, Lawrence, Mackinnon, Mahtani and Jorm2019), evaluating whether concordance with parenting guidelines increased for parents who received the parenting intervention. Two studies measured changes in parental distress. Comer et al. (Reference Comer, Furr, Del Busto, Silva, Hong, Poznanski and Puliafico2021) assessed whether the intervention was effective in reducing parents’ negative effects such as life impairment on their children’s anxiety. Poetar et al. (Reference Poetar, Dobrean and Andersson2024) measured parental distress pre- and post-intervention to examine whether teaching parents skills to manage their psychological distress resulted in a reduction of anxiety in children. One study investigated changes in parental knowledge (Khanna et al., Reference Khanna, Carper, Harris and Kendall2017), determining whether parental knowledge on how to manage adolescents with anxiety improved after intervention.
Non-completion of assessment rates
In this review, non-completion rate was defined as the absence of participation in the first assessment conducted after the intervention among participants in the intervention group, as a way to assess the feasibility and adherence of each program. Regardless of the specific terminology used in the original studies, such as ‘post-intervention’ or ‘follow-up’, the first post-intervention assessment was consistently used as the reference point for determining whether participants had completed the intervention. Additional follow-up assessments conducted beyond the initial post-intervention evaluation were not included in the calculation of non-completion rates. In studies with multiple informants, such as parents, children, or clinicians, non-completion was determined based on parent-report data. This decision was made to enhance comparability across studies, as parent reports were most commonly used as the primary outcome measure of treatment effects. As a result, the non-completion rates reported in this review may differ from those reported by the original authors, who may have used different definitions or sources of information.
Non-completion rates varied across studies. Of the 13 studies reviewed, two showed non-completion rates of approximately 10% or lower. Vigerland et al. (Reference Vigerland, Thulin, Ljotsson, Svirsky, Öst, Lindefors and Serlachius2013) showed a 10% non-completion rate, while Cardamone-Breen et al. (Reference Cardamone-Breen, Jorm, Lawrence, Rapee, Mackinnon and Yap2018) showed a rate of 7%. Five studies had non-completion rates ranging from 10% to 20%. Comer et al. (Reference Comer, Furr, Del Busto, Silva, Hong, Poznanski and Puliafico2021) showed a 20% non-completion rate, Khanna et al. (Reference Khanna, Carper, Harris and Kendall2017) reported 16%, Yap et al. (Reference Yap, Cardamone-Breen, Rapee, Lawrence, Mackinnon, Mahtani and Jorm2019) had 13%, Sim et al. (Reference Sim, Fernando, Jorm, Rapee, Lawrence, Mackinnon and Yap2020) showed 18%, and Donovan and March (Reference Donovan and March2014) reported 17%. Donovan and March (Reference Donovan and March2014) defined completion as participants who completed both outcome assessments conducted during the first post-intervention evaluation. Participants who missed either assessment were classified as non-completers. This criterion was adopted to ensure the completeness of outcome measurement. Six studies showed non-completion rates exceeding 20%. Creswell et al. (Reference Creswell, Taylor, Giles, Howitt, Radley, Whitaker and Yu2024) reported 21%, Morgan et al. (Reference Morgan, Rapee, Salim, Goharpey, Tamir, McLellan and Bayer2017) showed 27%, and Jolstedt et al. (Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018) had a 53% non-completion rate. In Jolstedt et al. (Reference Jolstedt, Ljótsson, Fredlander, Tedgård, Hallberg, Ekeljung and Vigerland2018), the number of participants increased in later follow-up assessments compared with the post-intervention phase. However, the non-completion rate was still calculated based on the first post-intervention assessment, in accordance with the pre-defined criteria. Vigerland et al. (Reference Vigerland, Ljótsson, Thulin, Öst, Andersson and Serlachius2016) showed a 28% non-completion rate; although the original article stated that no families dropped out, as all completed at least part of the intervention, this review applied a consistent definition based on the absence of parent-report data at the first post-assessment. Poetar et al. (Reference Poetar, Dobrean and Andersson2024) also showed a 29% non-completion rate. Finally, Green et al. (Reference Green, Reardon, Button, Williamson, Halliday, Hill and Creswell2023) showed a non-completion rate of 45%. In this study, ‘Module 6’ was defined as the post-intervention phase by the authors, so non-completion was calculated based on completion status at that stage.
Discussion
This study was a narrative review of internet-delivered parent-led interventions to reduce anxiety symptoms in children and adolescents. The results show that these types of interventions may be effective in reducing anxiety symptoms in children and adolescents and that the effects may persist post-intervention.
The current review shows that interventions are more effective when they target anxiety symptoms directly rather than indirectly. Studies in which the interventions focused directly on anxiety in children and adolescents, such as by providing education on anxiety symptoms and teaching coping methods and skills, showed significant reductions in anxiety symptoms compared with the control group. In studies that only included a treatment condition, statistically significant decreases in anxiety were observed from pre- to post-treatment. One study demonstrated that internet-delivered parent-led interventions directly targeting anxiety symptoms were not inferior to treatment as usual. Only one study showed that the intervention group’s knowledge of CBT principles improved significantly compared with the control group; however, it did not have a decisive effect on child anxiety (Khanna et al., Reference Khanna, Carper, Harris and Kendall2017). Other studies also demonstrated significant intervention effects in targeting anxiety symptoms directly. Salza et al. (Reference Salza, Giusti, Ussorio, Casacchia and Roncone2020), who provided an intervention addressing anxiety management, reported that symptoms were significantly alleviated in all groups post-intervention. Levy et al. (Reference Levy, O’Bryan and Tolin2021) showed that this type of intervention was effective in maintaining treatment effects, as recurrence occurred in only 14% of patients. However, none of the three studies on parenting interventions that focused on modifying parenting environments rather than directly alleviating anxiety symptoms demonstrated significant intervention effects compared with control groups in improving anxiety symptoms in children and adolescents. Although these interventions were effective in reducing risk factors and improving protective factors for parenting, they did not demonstrate significant short-term effects in alleviating anxiety in children and adolescents. Considering that changes in the parenting environment may take longer to affect symptoms in children and adolescents compared with other interventions, the long-term effects require further investigation.
Clinical consultations with a therapist via telephone may have had a positive impact on reducing anxiety symptoms. Interventions directly targeting anxiety symptoms were somewhat effective on their own; however, the inclusion of telephone support led to consistent outcomes. Interventions that directly targeted anxiety and included clinical counselling through telephone calls with therapists, such as addressing questions related to intervention content and problem-solving, showed a decrease in anxiety symptoms in children and adolescents in the intervention group, with treatment effects persisting through follow-up. This suggests that active communication with therapists can enhance the effectiveness of interventions that directly target anxiety. This is consistent with the meta-analysis of Andersson et al. (Reference Andersson, Carlbring, Titov and Lindefors2019), which investigated internet-delivered CBT interventions for anxiety disorders and found that intervention support provided by a therapist when needed was particularly effective for treating anxiety disorders. Active interaction with therapists may lead to better treatment outcomes by not only engaging participants more fully in the therapeutic process but also discussing changes and conceptualising a shared understanding of the problems with them (Malins et al., Reference Malins, Moghaddam, Morriss, Schröder, Brown and Boycott2022). These findings also highlight the advantages of internet-delivered interventions. In situations where access to treatment is limited due to a shortage of therapists or delays in early intervention (Holmes et al., Reference Holmes, Ghaderi, Harmer, Ramchandani, Cuijpers, Morrison, Roiser, Bockting, O’Connor, Shafran, Moulds and Craske2018), such programs can offer an effective alternative by improving both the accessibility and efficiency of mental health services.
Discrepancies were found between self-reported anxiety symptoms in children and adolescents and those reported by their parents about their children, indicating the need to consider including both parent- and child-report measures. This pattern aligns with the findings of Orchard et al. (Reference Orchard, Pass, Cocks, Chessell and Reynolds2019). Parents cannot directly perceive their child’s emotional state; thus, they must use the child’s behaviour to infer the degree of anxiety their children experience. Moreover, children or adolescents experiencing anxiety focus on their inner self, making it easier for them to recognise the symptoms compared with noticing them from the outside (Pereira et al., Reference Pereira, Muris, Barros, Goes, Marques and Russo2015). Furthermore, in children and adolescents, anxiety symptoms that can only be perceived internally may have decreased after anxiety symptoms that can be observed externally, such as behaviour, had been reduced (Wood et al., Reference Wood, Piacentini, Southam-Gerow, Chu and Sigman2006). Therefore, not only measurements of anxiety in children and adolescents as reported by their parents but also those reported by the children and adolescents themselves are important to include in studies on intervention effects (Bowers et al., Reference Bowers, Reider, Morales, Buzzell, Miller, Troller-Renfree and Fox2020). The scales for measuring anxiety symptoms and severity in children and adolescents also varied. In future studies, it may be helpful to include anxiety symptoms reported by children and adolescents together, and considering standardised methods to facilitate the ease of comparing different measurement tools and severity levels at baseline would be beneficial.
Some limitations should be considered when drawing conclusions from the current review. First, by limiting the studies included in this review to those published after 2013, there is a possibility that important earlier research, which could broaden the understanding of internet-delivered parent-led interventions for anxiety in children and adolescents, was excluded. Additionally, although efforts have been made to capture all relevant literature through various keyword combinations, some eligible studies may have been inadvertently excluded due to limitations in the search strategy. Furthermore, the exclusion of grey literature from the final selection may have limited the scope of the review. Second, both children and adolescents diagnosed with anxiety disorders and those not diagnosed were included, resulting in varying severity levels at baseline. Also, some studies did not include assessments of anxiety symptoms reported by children and adolescents, instead using only parent-report measurements. These factors make accurate comparisons between studies difficult and indicate the need to interpret the findings carefully. Third, this review was not pre-registered in a publicly accessible database. In addition, main review procedures, such as screening and data extraction, were conducted by a single author. While efforts were made to maintain methodological rigor, the possibility of bias or error cannot be entirely excluded. Finally, this review only included papers published in English, which may have resulted in a language bias.
Conclusions
This review provides evidence that internet-delivered parent-led interventions can be effective in reducing anxiety symptoms in children and adolescents, and this effect can be maintained through follow-up. However, various intervention forms and methods centred on parents, and some studies relied only on parental reports regarding decreased anxiety in children and adolescents. These results are noteworthy in that they demonstrate that internet-delivered parent-led interventions can be a promising alternative to treating anxiety in children and adolescents from the perspective of increasing the accessibility and efficiency of mental health services for children and adolescents.
Data availability statement
No new data were generated or analysed in this study. All data supporting the findings of this review are derived from previously published studies and are cited within the article.
Acknowledgements
None.
Author contributions
Sujin Kim: conceptualization, investigation, writing-original draft; Hyo Shin Kang: conceptualization, writing-review & editing, supervision.
Financial support
None.
Competing interests
The authors declare none.
Ethical standards
This study is a literature review and did not involve the collection of primary data from human participants or animals. Therefore, ethical approval was not required.


 Open access
Open access
Comments
No Comments have been published for this article.