


Introduction
Understanding the impact of CHD on family functioning has become increasingly important as advances in paediatric cardiology and cardiac surgery have substantially improved survival rates among children with life-threatening heart defects. Reference Stephens, Morris and Benjamin1 In Slovakia, approximately 450 children are born with CHD each year, with around 300 requiring surgical intervention. Of these, nearly 85% survive into adulthood, yet many require long-term, multidisciplinary care. 2,Reference Vršanská3 Despite these medical successes, children with CHD often face persistent health challenges, frequent hospitalisations, and ongoing therapeutic needs that place considerable physical, emotional, and financial demands on their families. Reference Mastorci, Ait-Ali and Festa4,Reference Baumgartner, De Backer and Babu-Narayan5
Parents play a central role in the daily care and management of children with CHD, often assuming complex caregiving responsibilities that go beyond routine parenting. Although supported by multidisciplinary healthcare teams, families must navigate chronic stress, uncertainty, and disruptions to everyday life. Numerous studies have shown that parents of children with CHD report lower quality of life across multiple domains, including mental health, vitality, emotional well-being, and social functioning. Reference Sood, Karpyn and Demianczyk6–Reference Gaskin11 The emotional burden is frequently accompanied by physical exhaustion, organisational challenges, and financial strain. Reference Gaskin, Barron and Wray8–Reference Knight Lozano, May and Clarkson10
Recent literature increasingly emphasises the need to understand the broader psychosocial impact of CHD on the family system. Reference Grunberg, Geller, Hoffman and Patterson12 While existing research has addressed areas such as parental stress, Reference Sood, Karpyn and Demianczyk6 coping and resilience, Reference Sanayeh, Nourian and Tajalli13 depression, Reference Kolaitis, Meentken and Utens14 and quality of life, Reference Gaskin11,Reference Cole, Ridings and Phillips15 one important area remains relatively underexplored: spirituality. Spirituality—broadly understood as a source of existential meaning, faith, or belief system—has been recognised as a critical coping resource in the context of chronic illness. Reference Nayeri, Roddehghan, Mahmoodi and Mahmoodi7 Cultural and religious beliefs may significantly influence how families interpret illness, seek meaning, and make care-related decisions. Reference Sood, Karpyn and Demianczyk6,Reference Nayeri, Roddehghan, Mahmoodi and Mahmoodi7,Reference Dalir, Heydari, Kareshki and Manzari16 However, despite its potential relevance, the spiritual dimension of caregiving remains insufficiently examined, particularly in Central Europe.
In Slovakia and other Central European countries, spirituality is often deeply interwoven with cultural identity and community life, predominantly shaped by Christian traditions. Nonetheless, spiritual support is rarely integrated into routine clinical care. Parents of children with CHD frequently report unmet needs related to emotional counselling, spiritual guidance, and family-centred communication, revealing a persistent gap between holistic care recommendations and real-world practice. Reference Kondrla, Leskova and Durkova17,Reference Woolf-King, Anger and Arnold9
As de Morais et al. Reference de Morais Almeida, de Carvalho and Araujo Júnior18 emphasise, cultural and spiritual factors play a crucial role in how families cope with stress and illness. Understanding these dimensions is essential for tailoring support to the unique socio-cultural contexts of each family. Therefore, research is needed to explore how parents of children with CHD in Slovakia experience their caregiving role, what sources of psychological, spiritual, and material support they rely on, and how socio-demographic and clinical variables influence their daily functioning.
This study aims to address these gaps by examining the psychosocial functioning, emotional experiences, and spiritual coping of parents caring for children with CHD in Slovakia. Specifically, it investigates (1) the life situations and support systems of these parents, (2) the associations between parental socio-demographic factors and child clinical characteristics with family functioning, and (3) the role spirituality plays in coping with the demands of caregiving. Through this culturally grounded perspective, the study seeks to inform more holistic, family-centred approaches to care that better reflect the lived realities of families affected by CHD.
Materials and methods
This study was conducted as a web-based survey using a cross-sectional design, in accordance with the STROBE checklist for observational studies Reference von Elm, Altman and Egger19 and the CHERRIES checklist for reporting internet-based surveys. Reference Eysenbach20 The study adhered to the principles of the Declaration of Helsinki, developed by the World Medical Association, as well as the guidelines of Good Clinical Practice. 21,Reference Guerra-Farfan, Garcia-Sanchez and Jornet-Gibert22 The study protocol was approved by the Bioethics Committee of the Medical University of Silesia in Katowice, Poland (No.: BNW/NWN/0052/KB/288/24) and the Ethics Committee of Constantine the Philosopher University in Nitra, Slovakia (No.: UKF/1460/2024/191013:001). Prior to participation, respondents were informed about the anonymous and voluntary nature of the survey. Informed consent was obtained from each respondent before the study began.
Participants
The study sample included a targeted group of parents (n = 118), selected based on predefined inclusion and exclusion criteria. The inclusion criteria were being a parent of a child with a medically confirmed CHD diagnosis, fluency in spoken and written Slovak, provision of informed consent and being the parent of a minor child with CHD. Exclusion criteria were lack of consent to participate, having more than one child with CHD (to limit confounding emotional and logistical variables), inability to comprehend or complete the questionnaire due to language limitations, and being a parent of an adult with CHD (aged 18 years and older).
A purposive sampling method was used to ensure the minimum required sample size, which was calculated to be 116 participants. This calculation was based on statistical estimation of the population of paediatric CHD patients and their families in Slovakia, using a confidence level of 80%, a fraction size of 0.5, and a maximum allowable margin of error of 5%, in line with national data. 2 The final sample (n = 117) met the target, fulfilling the inclusion criteria and providing sufficient statistical power for the planned analyses.
Data collection
Data collection was conducted between December 2024 and January 2025 and focused on parents of children diagnosed with CHD in the Slovak Republic. Participants were recruited through a closed social media support group specifically dedicated to families of children with CHD. This group was recommended by nurses from a specialised paediatric cardiology unit at a major children’s hospital in Slovakia, where these families receive regular care. The recruitment strategy may have contributed to the relatively high response rate. Additionally, the online format enabled flexible participation and may have facilitated wider dissemination through peer sharing within the support community (i.e., a snowball effect). The questionnaire was administered online via a secure platform, and participation was both voluntary and anonymous. Due to the anonymous nature of the survey, it was not possible to determine whether responses originated from both parents within the same family unit. Consequently, each response was treated as an independent observation. A brief description of the study’s aim, along with an informed consent statement, was provided at the beginning of the survey. Respondents were informed that they could withdraw from the study at any point without consequence.
Instruments
Data were collected using the Life Situations of Caregivers/Parents of Children with CHD and/or Other Cardiac Diseases Questionnaire, which was developed by Polish authors. Reference Kolarczyk, Morka, Barański and Szydłowski23 The Slovak version of the questionnaire was prepared using a forward–backward translation process to ensure linguistic and conceptual equivalence. Two independent translators completed the initial translation into Slovak, which was then synthesised and back-translated by two other translators blinded to the original. Discrepancies were resolved through expert consensus. Face validity was evaluated through cognitive interviews with four parents of children with CHD, leading to minor wording adjustments for clarity. Content validity was assessed by a panel of six experts who rated each item for relevance and clarity. The resulting item-level CVIs were ≥0.85, and the scale-level CVI exceeded 0.90, confirming strong content validity and suitability for use in the Slovak context.
The Life Situations of Caregivers/Parents of Children with CHD and/or Other Cardiac Diseases Questionnaire is a self-report tool consisting of 10 items designed to assess caregivers´ life situation across two primary domains: personal functioning and the influence of spirituality on life functioning, as well as overall life situation. Responses are rated on a five-point Likert scale, with higher scores on subscales indicating a better perceived life situation, higher levels of daily functioning, and a greater influence of spirituality on the caregiver´s life circumstances.
Furthermore, the questionnaire includes six additional multiple-choice items that explore parents´ emotional experiences related to the child’s illness, as well as perceived psychological, spiritual, and material support, beliefs about the causes of the illness, and identification of the primary caregiver. The questionnaire has demonstrated reliability and internal consistency in measuring parental functioning in the context of a child’s illness. The Cronbach alpha coefficients (α) in the original study were as follows: α = 0.72 for the personal domain, α = 0.83 for the spiritual domain, and the overall α = 0.66. Reference Kolarczyk, Morka, Barański and Szydłowski23 In the Slovak version of the questionnaire, internal consistency was acceptable, with a Cronbach’s alpha of 0.78 for the overall scale, 0.70 for the personal functioning domain, and 0.84 for the spirituality domain.
Along with the main questionnaire, a self-designed sociodemographic and clinical questionnaire was also administered, which included items on the parent’s age, marital status, education, place of residence, employment status, and religious affiliation, as well as the child’s age, gender, type of heart defect, history of cardiac surgery, and the time elapsed since the most recent procedure.
Statistical analysis
A significance level of p < 0.05 was used for all statistical analyses. Descriptive analysis of the questionnaire and related items included the calculation of the mean (M), standard deviation (SD), median (Md), frequencies (%), quartiles, and range. Multiple linear regression was employed to examine the potential impact of predictors on the outcome variable. Regression coefficients were reported along with their 95% confidence intervals. All statistical analyses were conducted using R software (version 4.5.1) 24 and IBM SPSS Statistics (version 25.0). Regression analysis offers important advantages when exploring relationships between multiple predictors and a single outcome, compared to conducting separate univariate tests. By including all predictors in a single model, regression allows for a more accurate estimation of each variable’s unique contribution while controlling for the influence of others. This approach not only improves interpretability but also reduces the risk of Type I errors associated with multiple comparisons. Reference Ali and Younas25
Results
Characteristics of the study group
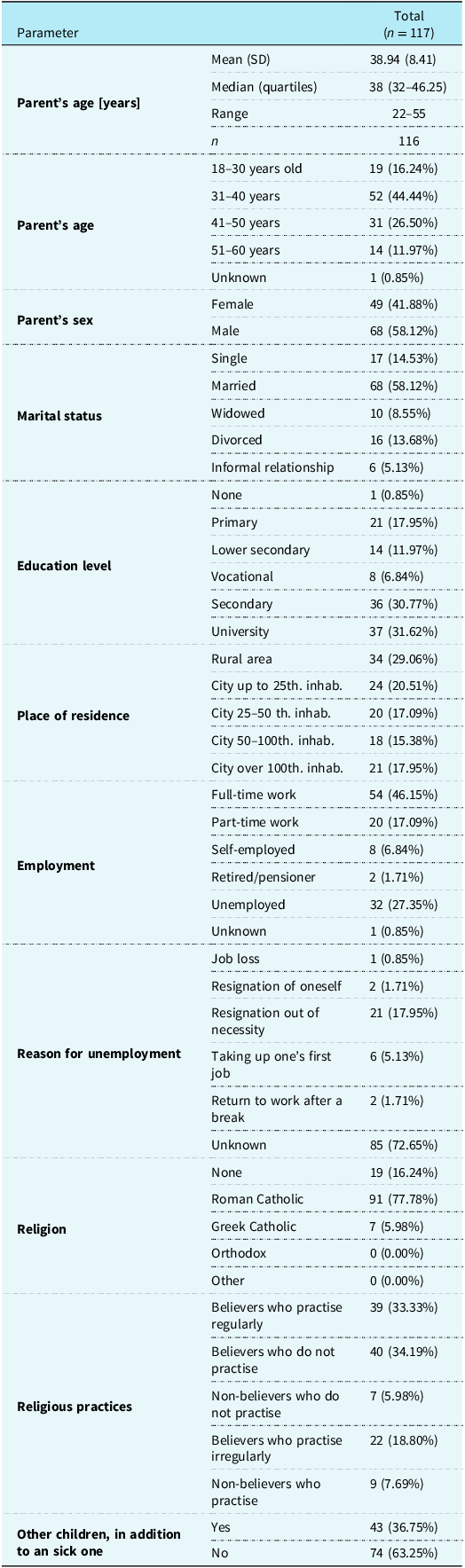
The sample consisted of 49 mothers (49.88%) and 68 fathers (58.12%), with a mean age of 38.94 ± 8.41 years. An overview of the participants´ sociodemographic characteristics is presented in Table 1.
Sociodemographic characteristics of the study group

Table 1. Long description
The table presents sociodemographic characteristics of a study group with 117 participants. It includes columns for various parameters such as parent’s age, parent’s sex, marital status, education level, place of residence, employment, reason for unemployment, religion, religious practices, and other children in addition to a sick one. The table has 12 columns and 18 rows, including headers and grouped rows. Each row provides specific data points for the parameters listed. For example, the parent’s age is divided into categories like 18-30 years old, 31-40 years old, and so on, with corresponding counts. The table also includes detailed information on employment status, reasons for unemployment, and religious practices.
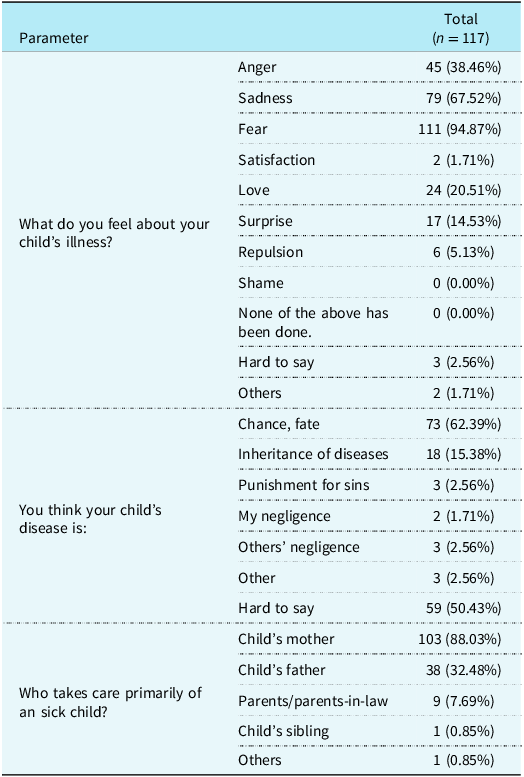
The most reported emotions related to the child’s illness were fear (94.9%), sadness (67.1%), and anger (38.46%). Most parents (62.39%) believed the illness occurred by chance, while 15.38% considered it hereditary. Mothers were most often identified as the primary caregivers (88.03%), compared to fathers (32.48%). The mean age of the children was 7.26 ± 4.98 years, with an equal gender distribution (49.57% boys and 49.57% girls). Further details on parental characteristics, child demographics, and the psychological, spiritual, and material support available to families are presented in Tables 2–4.
Parents’ feelings about the child’s illness, its perceived cause, and the main caregiver

Table 2. Long description
A table with three columns and twelve rows. The columns are labeled ’Parameter’, ’Total’, and ’N = 117’. The table is divided into three sections: feelings about the child’s illness, perceived causes of the illness, and primary caregivers. Row 1: Parameter, Total, N = 117. Row 2: What do you feel about your child’s illness?, Anger, 45 (38.46%). Row 3: Sadness, 79 (67.52%). Row 4: Fear, 111 (94.87%). Row 5: Satisfaction, 2 (1.71%). Row 6: Love, 24 (20.51%). Row 7: Surprise, 17 (14.53%). Row 8: Repulsion, 6 (5.13%). Row 9: Shame, 0 (0.00%). Row 10: None of the above has been done, 0 (0.00%). Row 11: Hard to say, 3 (2.56%). Row 12: Others, 2 (1.71%). Row 13: You think your child’s disease is:, Chance, fate, 73 (62.39%). Row 14: Inheritance of diseases, 18 (15.38%). Row 15: Punishment for sins, 3 (2.56%). Row 16: My negligence, 2 (1.71%). Row 17: Others’ negligence, 3 (2.56%). Row 18: Other, 3 (2.56%). Row 19: Hard to say, 59 (50.43%). Row 20: Who takes care primarily of an sick child?, Child’s mother, 103 (88.03%). Row 21: Child’s father, 38 (32.48%). Row 22: Parents/parents-in-law, 9 (7.69%). Row 23: Child’s sibling, 1 (0.85%). Row 24: Others, 1 (0.85%).
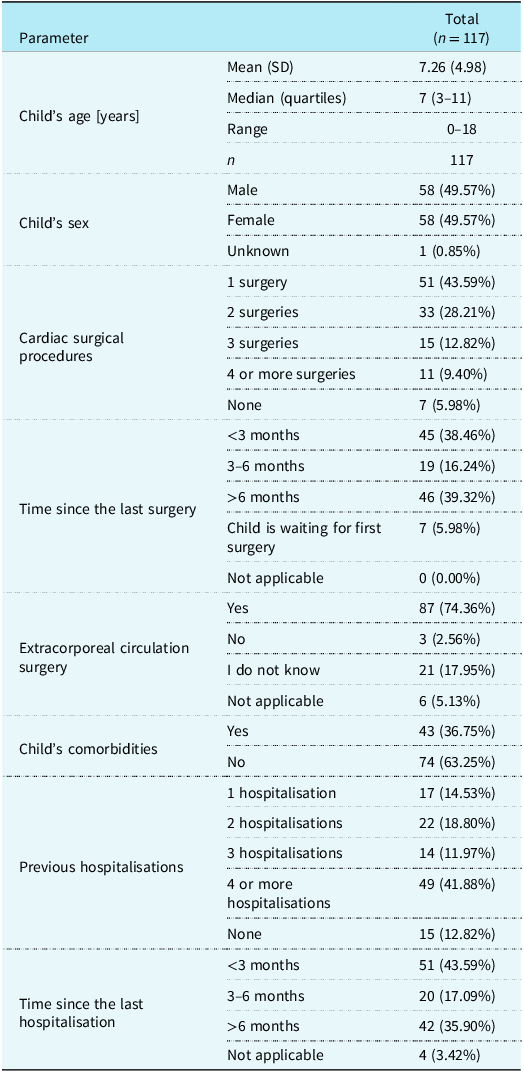
Characteristics of children with congenital heart defects as reported by their parents

Table 3. Long description
The table presents characteristics of children with congenital heart defects as reported by their parents. It has 12 rows and 2 columns. The columns are labeled ’Parameter’ and ’Total (N=117)’. The rows include various parameters such as child’s age, sex, cardiac surgical procedures, time since the last surgery, extracorporeal circulation surgery, child’s comorbidities, previous hospitalizations, and time since the last hospitalization. Each parameter is detailed with specific values and percentages. For example, the mean age is 7.26 years with a standard deviation of 4.98 years. The sex distribution shows 58 males and 58 females. Cardiac surgical procedures range from 1 surgery to 4 or more surgeries, with 7 children having none. Time since the last surgery is categorized into less than 3 months, 3-6 months, and more than 6 months, with 7 children waiting for their first surgery. Extracorporeal circulation surgery is reported by 87 children, with 3 not having it and 21 unsure. Comorbidities are present in 43 children, and previous hospitalizations range from 1 to 4 or more, with 15 children having none. Time since the last hospitalization is also categorized similarly to the time since the last surgery.
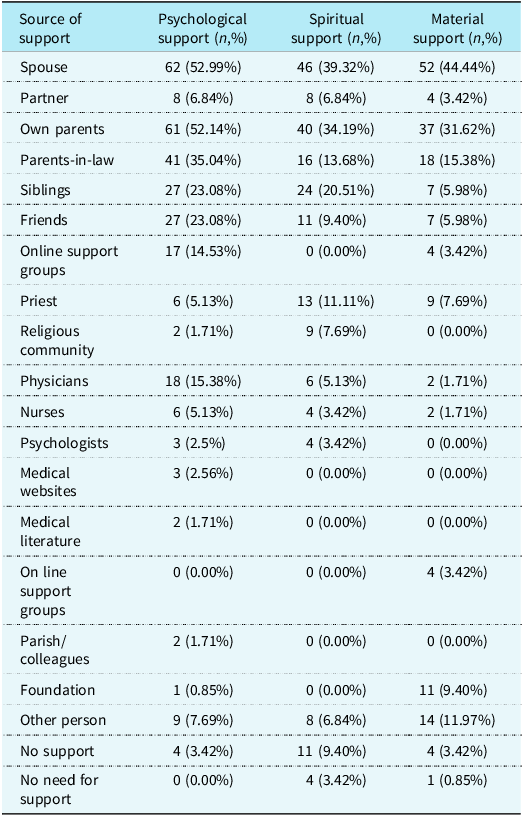
Sources of support for parents of children with CHD

Table 4. Long description
The table presents data on various sources of support categorized into psychological, spiritual, and material support for parents of children with CHD. It includes 21 rows and 4 columns. The columns are labeled as Source of support, Psychological support (n,%), Spiritual support (n,%), and Material support (n,%). The rows list different sources of support such as Spouse, Partner, Own parents, Parents-in-law, Siblings, Friends, Online support groups, Priest, Religious community, Physicians, Nurses, Psychologists, Medical websites, Medical literature, On line support groups, Parish/colleagues, Foundation, Other person, No support, and No need for support. Each row provides the number and percentage of parents who receive each type of support from the listed sources. For example, Spouse provides psychological support to 62 parents (52.99%), spiritual support to 46 parents (39.32%), and material support to 52 parents (44.44%). The table highlights the varying levels of support from different sources across the three categories.
Sociodemographic and clinical factors of family functioning in daily life
Multivariable linear regression showed that parental employment status and the child’s hospitalisation history were significantly associated with parents’ likelihood of giving up personal plans and career ambitions. Compared to full-time employed parents, those retired or on disability reported lower scores (B = −2.854, p = 0.026), while unemployed parents reported higher scores (B = 0.795, p = 0.018). Parents of children with four or more hospitalisations also scored lower (B = −1.341, p = 0.027).
The number of cardiac surgeries and time since last hospitalisation were significantly linked to perceived limitations in parents’ social life. One procedure increased scores by 2.224 points (p = 0.022), two by 2.463 (p = 0.014), three by 2.594, and four or more by 2.498 (p = 0.017). Recent hospitalisations reduced scores: within 3 months (B = −3.835, p = 0.012), 3–6 months (B = −3.252, p = 0.029), and over 6 months ago (B = −3.481, p = 0.019).
Unemployed parents also reported greater limitations in vacation, rest, and leisure (B = 1.064, p = 0.007). Parents with more children perceived fewer limitations in attention to their other children (B = −0.717, p = 0.024). No significant predictors were found for the impact of the illness on family bonding or conflicts (p > 0.05).
Sociodemographic and clinical factors of the impact of spirituality on living situations
The multivariable analysis showed that none of the examined sociodemographic or clinical characteristics were significant independent predictors of parents’ responses related to faith and religious practices (e.g., whether faith and prayer could restore their child’s health, whether they had lost belief in God, or whether they prayed and participated in religious rituals more frequently because of the child’s illness), as all p-values exceeded 0.05.
Results of the life situation questionnaire among parents of children with CHD
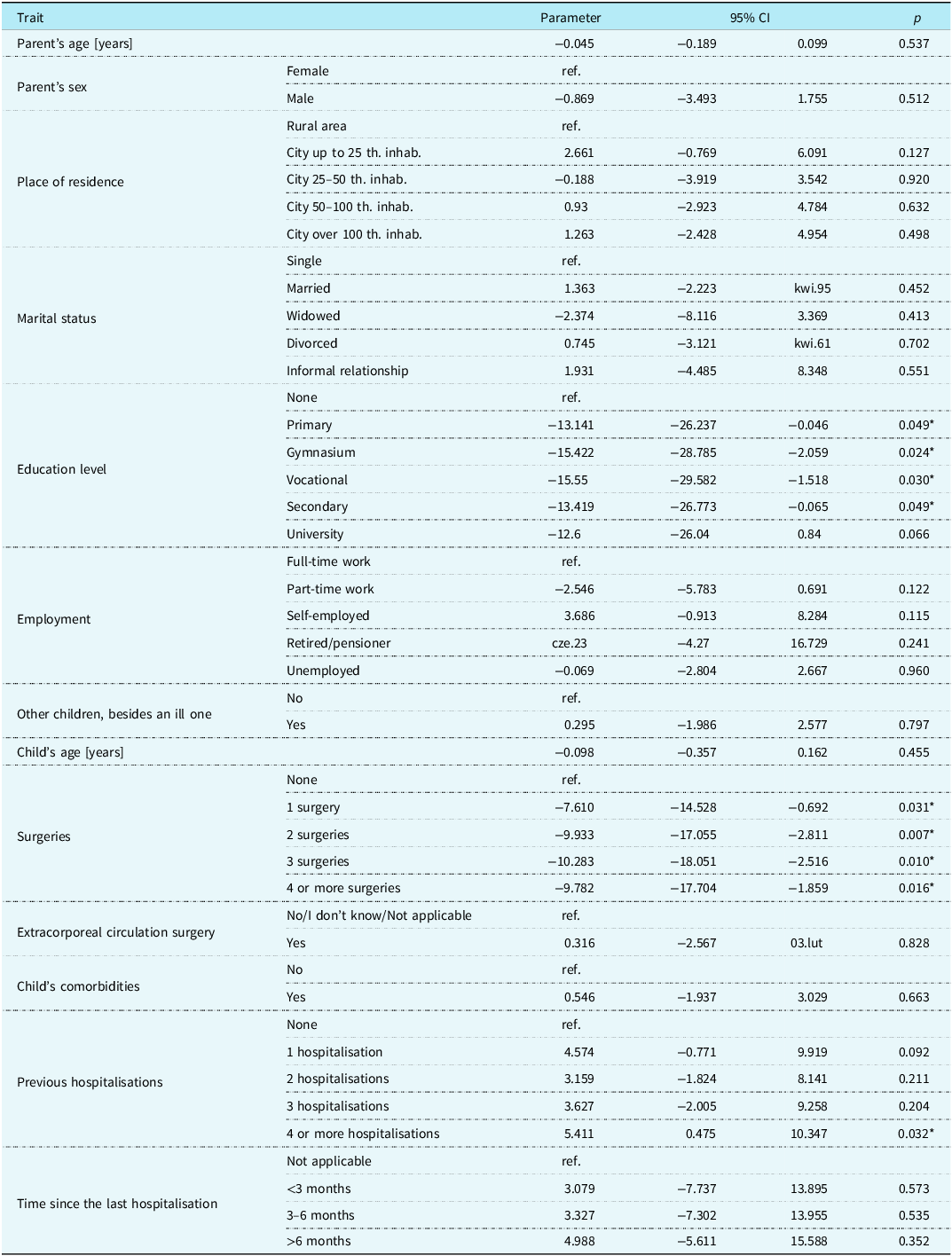
The mean score on the Life Situation Questionnaire among parents of children with CHD was 31.09 ± 5.58. Regression analysis revealed that parental education and the child’s clinical history significantly influenced these scores. Compared to parents without formal education, those with primary (B = −13.141, p = 0.049), gymnasium (B = −15.422, p = 0.024), vocational (B = −15.550, p = 0.030), and secondary education (B = −13.419, p = 0.049) had significantly lower scores. Similarly, parents of children who had undergone one (B = −7.610, p = 0.031), two (B = −9.933, p = 0.007), three (B = −10.283, p = 0.010), or four or more cardiac surgeries (B = −9.782, p = 0.016) scored lower compared to those whose children had no procedures. Conversely, having a child with four or more prior hospitalisations was associated with a higher score (B = 5.411, p = 0.032) (Table 5).
Multivariate linear regression model

Table 5. Long description
The table presents a multivariate linear regression model with parameters for various traits affecting life situation scores. It has 10 columns and 30 rows. The columns are labeled Trait, Parameter, 95% CI, and p. The rows are grouped by different traits such as Parent’s age, Parent’s sex, Place of residence, Marital status, Education level, Employment, Other children, besides an ill one, Child’s age, Surgeries, Extracorporeal circulation surgery, Child’s comorbidities, Previous hospitalisations, and Time since the last hospitalisation. Each row lists the trait, parameter value, 95% confidence interval, and p-value. Notable trends include significant p-values for certain education levels and the number of surgeries, indicating their influence on life situation scores.
* Statistically significant difference: p < 0.05.
Discussion
The study found that repeated hospitalisations of the child were associated with a more favourable parental assessment of their life situation, possibly reflecting adaptation to the child’s illness or strengthened coping mechanisms. In contrast, lower parental education and the child’s history of cardiac surgery were linked to less favourable assessments, suggesting increased psychological and social stress in these groups.
Chang et al. demonstrated that frequent hospitalisations and a higher number of surgical procedures in children with CHD significantly increase parental stress and reduce their ability to cope effectively with the illness. However, they also noted that longer hospital stays can foster stronger, partnership-orientated relationships between mothers and nurses. Reference Chang, Lim and Yoon26 Frequent hospitalisations are further linked to financial strain, contributing to material hardships within the household. Reference Hummel, Ludomirsky and Burgunder27 These factors help explain why parental evaluations of their life situation are closely tied to the frequency of hospitalisations. The impact of parental education is supported by Delaney et al., who found that lower education levels are associated with reduced psychological resilience in coping with the challenges of raising a child with CHD. Reference Delaney, Fu and McTernan28
As noted in the literature, having a child with CHD often requires parents to adapt to the child´s specific needs, frequently at the expense of their social and family life. Reference Hummel, Ludomirsky and Burgunder27,Reference Arafa, Zaher, El-Dowaty and Moneeb29 Studies also report that following the diagnosis, some parents withdraw from social interactions, experience isolation, and face significant restrictions in social activities due to caregiving responsibilities and the concerns about the child’s health. Reference Nayeri, Roddehghan, Mahmoodi and Mahmoodi7
In the present study, the number of cardiac surgical procedures was positively associated with parents´ perception that the illness limited their social life—the more procedures, the stronger this perception. In contrast, recent hospitalisations had the opposite effect: parents of children hospitalised in recent months reported fewer social limitations compared to those whose children had not been hospitalised. The greatest decrease in this perception was observed when hospitalisation occurred within the last three months. This may reflect a sense of relief following successful treatment and reassurance from the close medical supervision provided during hospitalisation. Reference Jackson, Frydenberg and Liang30 Additionally, these findings suggest that surgical interventions may intensify caregiving demands, prompting parents to withdraw from social activities and focus more intensely on their child’s needs. Conversely, recent hospitalisations may offer a temporary sense of stability and security, contributing to reduced perceptions of social restriction. Reference Woolf-King, Anger and Arnold9
The study also revealed that unemployed parents were more likely to feel deprived of opportunities for rest and vacation due to their child´s illness compared to those employed full-time. However, the absence of work-related obligations may simultaneously allow for greater involvement in caregiving. Reference Koerber, Mack and Seefeld31 Unemployed parents may have more flexibility and time to adjust to the demands of caring for a child with CHD. Although this often requires a substantial reorganisation of daily routines, those less burdened by external responsibilities may be better equipped to cope with the associated challenges. Reference Chen, Chen and Lo32 Thus, while unemployment may intensify perceived losses in leisure and rest, it may also facilitate adaptation to the caregiving role.
This study also found that parents with more than one child were less likely to feel that their child´s illness limited the attention given to their other children. This may be due to the fact that parents with more children often develop effective time management and responsibility-sharing strategies, enabling them to more easily divide their attention between the child with CHD and their healthy siblings. Reference Gregory, Prouhet and Russell33 Additionally, the presence of siblings may help maintain balance in family dynamics, as parents are compelled to consider the needs of all their children, which may reduce feelings of neglect. However, existing literature indicates that siblings of children with CHD often experience significant disruptions in daily life, with negative consequences across various domains. Evidence on protective or mitigating factors remains limited and inconclusive, highlighting the need for further research in this area. Reference Parker, Houghton, Bichard and McKeever34
In the present study, fear was the most commonly reported emotion among parents of children with CHD (94.87%), followed by sadness (67.52%) and anger (38.46%). Similar findings were reported by Ahn et al., who observed that although 83.3% of mothers of children with CHD received positive support from their husbands, they also experienced feelings of abandonment, anxiety about the potential loss of their child, and a strong need for reassurance. These emotional responses evolved over time, influenced by the child´s clinical status and psychosocial development. Reference Ahn, Lee and Choi35 Consistent with these findings, our study also found spouses were most frequently identified as the primary source of psychological, material, and spiritual support.
Traumatic stress is recognised as the most common psychological consequence experienced by parents of children with heart disease, Reference Jones, Cameron, Lee and McNelis36 with symptoms often emerging at the time of diagnosis, during hospitalisation, and continuing after discharge. Reference Currie, Anderson and McCarthy37 The findings of this study suggest that such may be alleviated if support for parents extends beyond the immediate family and includes structured assistance from healthcare professionals, such as access to psychologists, chaplains, and supportive nursing care. However, only 15.38% of parents reported receiving psychological support from a physician, 5.13% from a nurse, and just 2.56% from a psychologist. These results are consistent with the findings of Kalánková et al., who reported that psychological and emotional support is among the most frequently rationed aspects of nursing care in Slovakia. Reference Kalánková, Bartoníčková, Kolarczyk, Žiaková and Młynarska38
The present study also revealed an aspect related to the relatively high participation of fathers. One possible explanation may be the online and fully anonymous format of the survey, which may have provided participants with a greater sense of privacy and comfort when sharing personal experiences and emotions. Furthermore, this finding may reflect a broader cultural and social context concerning parental roles, in which contemporary fathers are increasingly involved in the daily care of their children and in medical decision-making processes concerning their children. Reference Sood, Karpyn and Demianczyk6,Reference Nayeri, Roddehghan, Mahmoodi and Mahmoodi7,Reference Knight Lozano, May and Clarkson10,Reference Gaskin11 This observation may suggest a growing willingness among fathers to actively participate in research related to child health and family experiences.
Religious and spiritual beliefs play a central role in helping parents cope with the burden of caring for a child with CHD. Previous research has shown that religious resources are more frequently used in stressful caregiving situations. Reference Dalir, Heydari, Kareshki and Manzari16 Consistent with these findings, our study demonstrated that, regardless of socio-demographic or clinical factors, parents emphasised the importance of spirituality and religious practices in their daily lives. Ahn et al. found that parents who professed a belief in God had significantly higher emotion-oriented coping scores than nonbelievers. Reference Ahn, Lee and Choi35 Similarly, Liu et al. reported that parents of infants with CHD who held strong religious beliefs and relied on spiritual support experienced lower levels of depression and reported a higher quality of life compared to nonbelieving parents. Reference Liu, Xie and Lei39
This study aimed to assess the role of spirituality in how parents of children with CHD cope with the challenges of their child’s illness. Existing literature suggests a significant relationship between religious beliefs and the mental health, caregiving burden, and quality of life of parents of infants with CHD. Reference Liu, Xie and Lei39 A study conducted in China found that parents with strong beliefs in God who received religious support were less likely to experience depression and reported a higher quality of life compared to non-believing parents. Some parents view their child’s illness as a “divine test” and place their hope in God’s will, believing that the child’s survival or death lies in His hands. Reference Nayeri, Roddehghan, Mahmoodi and Mahmoodi7 According to Dalir et al., religious and spiritual beliefs deeply influence the lives of families of children with CHD, with the use of religious resources becoming particularly pronounced during highly stressful caregiving. Reference Dalir, Heydari, Kareshki and Manzari16
Spiritual practice and religious support represent an important link between spirituality and the core disciplines of psychological and health research. According to López-Tarrida, it is important to integrate psychological knowledge—particularly in areas such as stress management, cognitive processes, family dynamics, and emotional regulation—into spiritual care. This interdisciplinary approach, including collaboration with psychologists and medical staff, can offer more comprehensive support to families of children with complex heart disease. Reference López-Tarrida, Suárez-Reina and de Diego-Cordero40 In line with this perspective, our findings suggest that spirituality plays a meaningful role in the lives of many parents of children with CHD. Regardless of their sociodemographic or clinical background, parents reported varying degrees of spiritual influence on their life situation. While spiritual support was most commonly received from family members, some parents also found support through religious communities, friends, or healthcare professionals. However, a notable proportion reported limited or no access to such support, highlighting potential gaps in holistic care. These findings highlight the relevance of spirituality in the lives of parents of children with CHD and emphasise the need for holistic, interdisciplinary approaches that integrate spiritual support into clinical practice.
This study further highlights several areas that warrant further in-depth exploration, particularly the role of spirituality in coping, gender differences in caregiving experiences, and the influence of cultural context on parental adaptation. Future research should consider a mixed-methods approach, incorporating qualitative interviews to provide a more nuanced understanding of these complex psychosocial processes.
Study limitations
This study has several limitations, including a relatively small sample of respondents (n = 117) and the use of a cross-sectional, web-based design. Another limitation of the study may be that parents of children with CHD who did not have access to digital technologies or sufficient digital literacy skills may have had limited opportunities to participate. Therefore, the study group may have been somewhat selective and composed primarily of individuals who actively use the internet and online platforms. Additionally, the absence of a comparison group limits the ability to draw broader conclusions; however, such a group is not required within the observational research framework. The authors plan to address this in future research by including a comparison group of parents of children with other cardiac conditions.
Conclusions
This study highlights that lower parental education and a child’s history of cardiac surgeries are associated with greater psychosocial strain among parents of children with CHD, while repeated hospitalisations may facilitate adaptive coping. Fear, sadness, and anger were the most reported emotions, with family members serving as the primary source of support. Although spirituality played an important role in coping, structured psychological and spiritual support from healthcare professionals was limited. These findings underscore the need for targeted psychosocial interventions and the integration of spiritual care within multidisciplinary paediatric cardiac services to enhance family-centred care.
Data availability statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
The authors extend their sincere thanks and gratitude to Dr Alina Zimna, from the Center for Foreign Languages of the Academy of Applied Sciences in Raciborz, for support in linguistic translation of the survey. The authors also wish to thank all the parents who participated in this study.
Author contribution
All authors listed confirm that they participated in the development of the manuscript in the following ways: conception and design or analysis and interpretation of the data; drafting the article or reviewing it critically for important intellectual content; and final approval of the version to be published.
Financial support
This research received no external funding.
Competing interests
The authors declare no conflict of interest.

 Open access
Open access