


Introduction
Alcohol use problems are widespread, with an estimated 600,000 adults in England with alcohol use disorder (AUD) from 2018 to 2019 (Lewis et al., Reference Lewis, McCammond, Sood, Sritharan and McDougall2023). However, 82% of these individuals are unlikely to access treatment (Committee of Public Accounts, 2023), and AUD has gradually increased (Department of Health Improvements and Disparities, 2024). Defined by a ‘craving, tolerance, and a preoccupation with alcohol and continued drinking in spite of harmful consequences’ (National Institute for Health and Care Excellence, 2011), AUD can be influenced by factors such as social inequalities, financial insecurity, unemployment and stress from the cost-of-living crisis (Carpenter et al., Reference Carpenter, McClellan and Rees2017; Institute of Alcohol Studies, 2023; Lewis et al., Reference Lewis, McCammond, Sood, Sritharan and McDougall2023; Manthey et al., Reference Manthey, Hassan, Carr, Kilian, Kuitunen-Paul and Rehm2021). Social isolation related to stigmatisation and discrimination may further discourage individuals from seeking help (Earnshaw, Reference Earnshaw2020; Link et al., Reference Link, Struening, Rahav, Phelan and Nuttbrock1997; Livingston, Reference Livingston2020; Rwatschew et al., Reference Rwatschew, Langan and Dent2024), perpetuating the problem. The Coronavirus-19 pandemic potentially intensified these challenges, with increased alcohol use as a coping mechanism and disruptions to face-to-face treatment (Avena et al., Reference Avena, Simkus, Lewandowski, Gold and Potenza2021; Dubey et al., Reference Dubey, Ghosh, Chatterjee, Biswas, Chatterjee and Dubey2020a, Reference Dubey, Biswas, Ghosh, Chatterjee, Dubey, Chatterjee, Lahiri and Lavie2020b; Hulsey et al., Reference Hulsey, Mellis and Kelly2020; Roberts et al., Reference Roberts, Rogers, Mason, Siriwardena, Hogue, Whitley and Law2021). Moreover, alcohol-related deaths have risen sharply over the past two decades, with a 20% increase in 2020 and a further 8% rise in 2021 (Lewis et al., Reference Lewis, McCammond, Sood, Sritharan and McDougall2023; Public Health England, 2021).
Beyond fatalities, AUD contributes to chronic illness (NHS, 2017), increased healthcare costs (Manthey et al., Reference Manthey, Hassan, Carr, Kilian, Kuitunen-Paul and Rehm2021; Scarborough et al., Reference Scarborough, Bhatnagar, Wickramasinghe, Allender, Foster and Rayner2011), productivity losses due to unemployment (Luoma et al., Reference Luoma, Twohig, Waltz, Hayes, Roget, Padilla and Fisher2007; Nolte-Troha et al., Reference Nolte-Troha, Roser, Henkel, Scherbaum, Koller and Franke2023), and mental health struggles (Bell and Britton, Reference Bell and Britton2014). From 2022 to 2023, 71% of adults with a substance use problem also reported having a mental health need (Office for Health Improvement and Disparities, 2023), up from 53% in 2018 to 2019. The complex interplay of these factors creates a persistent and vicious cycle of struggle and mental health challenges, complicating efforts to address alcohol use effectively.
The biopsychosocial model of addiction can help conceptualise this and seeks to create a multi-faceted approach (Skewes and González (Reference Skewes and González2013). It addresses individual differences and social determinants of health (Marlatt et al., Reference Marlatt, Baer, Donovan and Kivlahan1988) by considering the interaction of biological (e.g. genetics), psychological (e.g. personality traits and cognitive processes) and social factors (e.g. socioeconomic status).
Biological interventions (e.g. medically assisted detoxification and medications for cravings, such as Acamprosate, Nalmefene and Naltrexone) provide one line of support (National Institute for Health and Care Excellence, 2007; National Institute for Health and Care Excellence, 2011). However, psychosocial interventions are essential for addressing broader factors and combining medical with psychosocial interventions improves outcomes (Anton et al., Reference Anton, O’Malley, Ciraulo, Cisler, Couper, Donovan, Gastfriend, Hosking, Johnson, LoCastro, Longabaugh, Mason, Mattson, Miller, Pettinati, Randall, Swift, Weiss and Williams2006; Wenzel et al., Reference Wenzel, Thomas, Carrano, Stidham and Fishman2024). A review and meta-analysis found psychosocial interventions were associated with an improvement in abstinence rates by 28% in comparison with treatment as usual; however, the interventions were less effective for reducing drinking frequency or amount (Ghosh et al., Reference Ghosh, Morgan, Calvey, Scheibein, Angelakis, Panagioti, Ferri and Krupchanka2024).
Interventions widely evidenced for managing AUD are focused on CBT (National Institute for Health and Care Excellence, 2011), based on Beck’s CBT model of addiction, highlighting how negative thinking patterns and core beliefs can precipitate and perpetuate the addiction (Beck et al., Reference Beck, Wright, Newman and Liese2011). CBT interventions typically target skills linked to alcohol use (e.g. functional analyses – identifying and managing triggers, coping with craving, refusal skills, problem-solving skills, recognising and changing thoughts), but can also target emotional regulation and mood management skills (Peri et al., Reference Peri, Neppala, Shaik and Parvaz2024). Meta-analyses have shown positive outcomes for CBT helping manage alcohol use problems (Dutra et al., Reference Dutra, Stathopoulou, Basden, Leyro, Powers and Otto2008; Magill and Ray, Reference Magill and Ray2009). Similar results have been found when delivering CBT in a group setting for individuals with AUD (Chen et al., Reference Chen, Qian, Sun, Lin and Tang2019; Marques and Formigoni, Reference Marques and Formigoni2001; Peng et al., Reference Peng, Zhang, Yang, Wang, Kang, Zhu, Pan and Xu2022).
Dame Carol Black expressed that in many localities, psychosocial interventions are ‘limited’ and ‘substandard’ (Black, Reference Black2021) when she reviewed the sector, arising from funding cuts from 2014 to 2021 which led to a dearth of registered and trained professionals. On the other hand, peer-led groups such as Alcoholics Anonymous (AA) provide significant support for individuals in recovery (Boisvert et al., Reference Boisvert, Martin, Grosek and Clarie2008). There is an overlap between CBT and other interventions for AUD (Miller and Wilbourne, Reference Miller and Wilbourne2002). Social interventions are crucial with addiction due to the stigmatisation and discrimination faced by individuals. Best et al.’s (Reference Best, Beckwith, Haslam, Alexander Haslam, Jetten, Mawson and Lubman2016) model of social identity for recovery suggests the importance of individuals transitioning to pro-recovery social groups, with groups based on this model also addressing cognitive barriers to connection (Ingram et al., Reference Ingram, Dingle, Larance, Baker, Deane, Robinson, Beck, Leigh, Kontogiannis, Coleman, Degan, Nixon, Stirling, Hudson, Hides, Drummond, Breeze, Webber, Street and Kelly2025). Moreover, evidence has found peer-support and mutual aid groups, such as AA and Self-Management and Recovery Training (SMART), are important for reducing relapse and improving recovery (Boisvert et al., Reference Boisvert, Martin, Grosek and Clarie2008; Martinelli et al., Reference Martinelli, van de Mheen, Best, Vanderplasschen and Nagelhout2021; National Institute for Health and Care Excellence, 2011).
Engagement in drug and alcohol treatment remains a challenge. Dutra et al.’s (Reference Dutra, Stathopoulou, Basden, Leyro, Powers and Otto2008) review found that 35.3% of participants did not complete treatment. Similarly, Gilchrist et al. (Reference Gilchrist, Langohr, Fonseca, Muga and Torrens2012) reported that 21.5% of individuals self-discharged while going through alcohol detoxification. National data remain relatively consistent, with 33% of people seeking treatment for alcohol disengaging in 2023/24 (National Drug Treatment Monitoring System, 2024a, 2024b). High withdrawal rates may stem from difficulties in connecting with treatment programmes (Craig, Reference Craig1985). Dance et al. (Reference Dance, Brown, Bammer and Sibthorpe2004) emphasised the need for flexible approaches when working with marginalised individuals to ensure accessibility. Notwithstanding struggles with engagement, recovery rates tend to be modest. During 2023, 35.1% of adults successfully completed treatment for alcohol use and did not re-engage with services within six months (National Drug Treatment Monitoring System, 2024a, 2024b). This highlights the importance of integrating the evidence base, while evaluating the challenges within the local community context.
This project was conducted in a third sector drug and alcohol service within the South of England. The service adopts a biopsychosocial approach, delivered by a multi-disciplinary team, integrating medically assisted detoxifications, medication prescriptions, structured CBT groups, and individual motivational interviewing sessions (Rollnick and Miller, Reference Rollnick and Miller1995). Social support is provided through mutual aid groups (AA, SMART), community activities, access to gyms, cooking sessions and more. A small psychology team co-facilitates the structured CBT groups with recovery practitioners for the alcohol pathway.
This mixed-methods project aimed to evaluate a new structured CBT group, comparing outcomes with the previous unstructured psychosocial group by:
-
(1) Identifying whether self-reported data on alcohol consumption, psychological health, quality of life and physical health during two time-points in a six-month period, differed between groups, through quantitative data.
-
(2) Identifying whether attendance and completion rates differed between groups, through quantitative data.
-
(3) Exploring qualitative feedback from service-users who attended the structured CBT group.
Method
Intervention
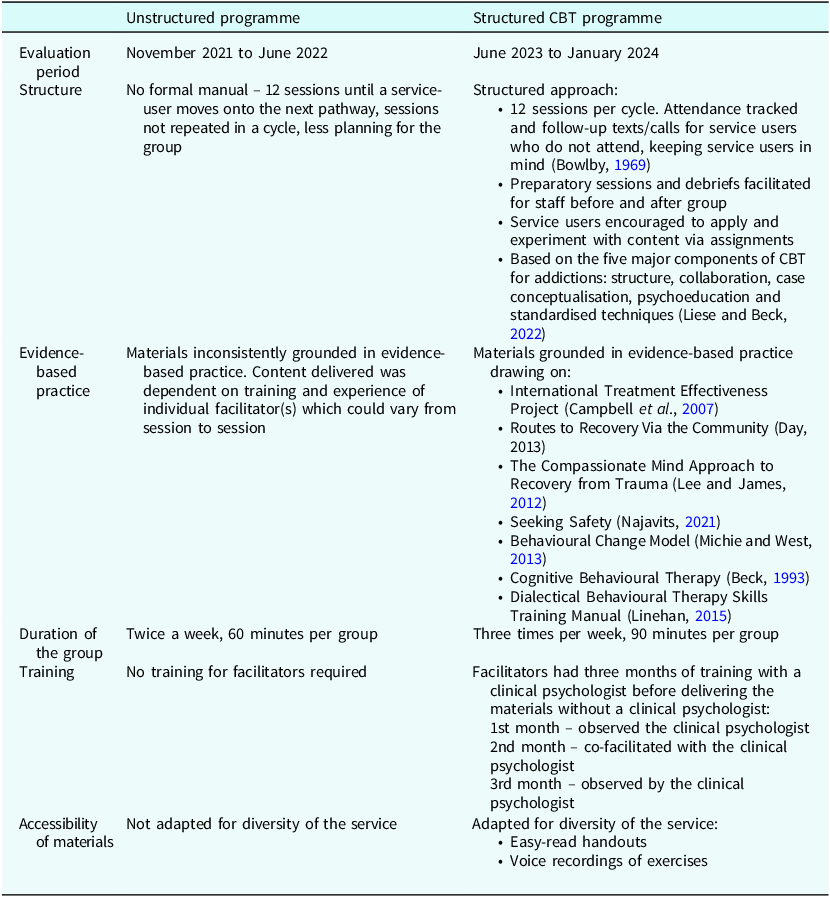
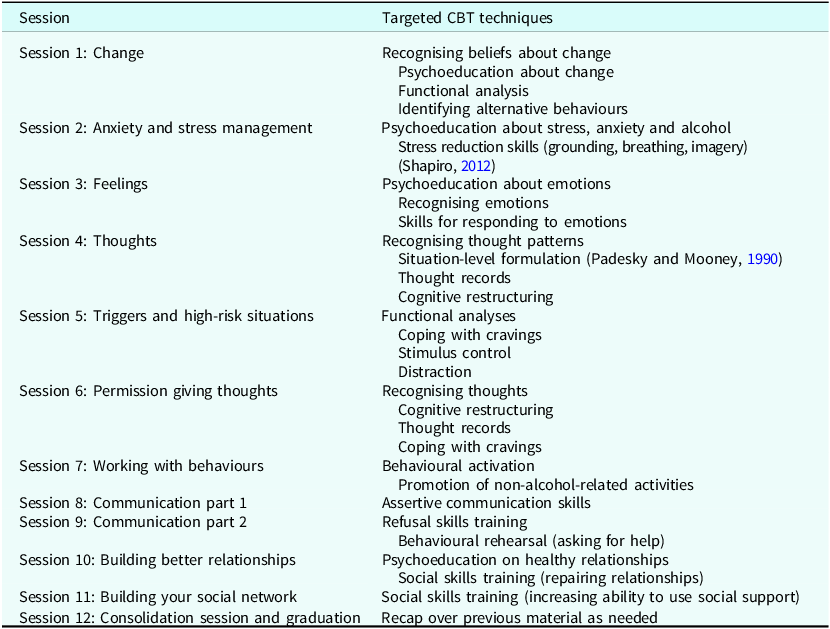
A structured CBT group was compared with an unstructured psychosocial group. Table 1 summarises the differences between the groups. Both groups were for people with AUD, now committed to an alcohol-free life. As the group was abstinence-based, attendees typically completed a medically assisted detoxification beforehand. The type of detoxification varied depending on the individual (for example, in-patient due to complex needs, or community-based when no significant risks were identified). The structured CBT group ran three times per week, for 90 minutes. The unstructured group ran twice per week, for 60 minutes. There were 12 sessions in each group. Therefore, service users would participate in the structured CBT group for one month and the unstructured group for six weeks. Data were collected over two 8-month time periods; consequently, six unstructured groups were evaluated and eight groups were evaluated within the structured CBT group. The specific CBT techniques used in each session in the structured CBT group are listed in Table 2. For the unstructured psychosocial group, no formal manual was used. Content was determined by the skills and experience of the individual practitioners and it was not systematic. Example of content covered during the period of data collection included:
-
What is aftercare, using mutual aid, and returning to work;
-
Tips for avoiding triggers;
-
Open discussion on where people were on their pathway, framework of care plans, reflecting on challenges within the week;
-
Harm reduction on Hepatitis A and B;
-
Reflective on recovery;
-
Open discussions about cravings and how to cope;
-
Relapse prevention;
-
Anger management;
-
Goal planning;
-
Decisional balance.
Specification of the unstructured and structured CBT programmes

Specific CBT techniques used in each session of the structured CBT programme (Beck et al., Reference Beck, Wright, Newman and Liese2011; Liese and Beck, Reference Liese and Beck2022)

Design
A mixed methods design was used to obtain subjective information from participants who attended the group, possibly providing more in-depth detail of their experiences, as well as data taken from outcome measures. This might enhance the understanding of the research problem, and corroborate the validity of the results (Hafsa, Reference Hafsa2019). Quantitative data were used to evaluate the change associated with the two different groups at two different time points. A mixed 2 × 2 design was used because there were two independent variables using different service users. One independent variable, unstructured and structured CBT, used between-subjects design as there were different service users in each group. The other independent variable, time (before and after the group), was a within-subjects design because the same service users were used. The dependent variables were the TOPs, and attendance and completion data. Qualitative data were used to explore service users’ feedback on the structured CBT group.
Inclusion and exclusion criteria
Service users were excluded if they only had one TOPs or were still in active treatment. Due to service users moving through the service and being discharged regularly, only service users who completed the structured CBT group within the last month were contacted for the qualitative evaluation.
Participants
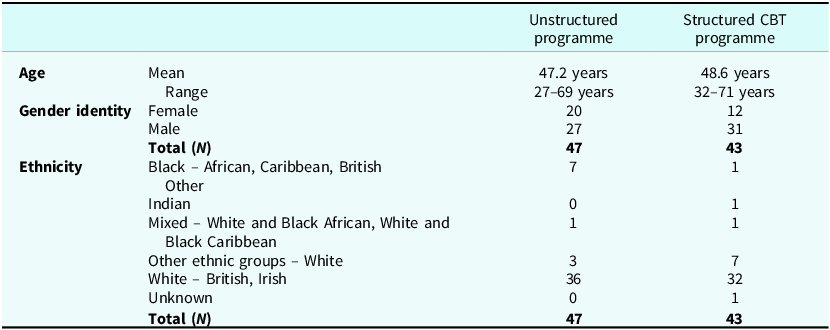
There were 90 service users included (unstructured group = 47, structured CBT group = 43). All service users received an information sheet and provided consent to use routine clinical outcomes data for research purposes when entering treatment. Table 3 summarises the demographic data: age, gender and ethnicity. A power calculation was not conducted as the data were already collected as part of routine clinical monitoring.
Age, gender and ethnicity of service users in (unstructured programme = 47, structured CBT programme = 43)

For the qualitative evaluation, those who completed the group within the last month were contacted via text (N=12). Four replied with interest and gave written and verbal consent. Table 4 shows the demographic data and their pseudonyms.
Pseudonyms and demographic data for service users in qualitative evaluation

Measures
The TOPs questionnaire is a government required standard that measures change and progress in different areas of the lives of drug and alcohol users (Public Health England, 2020). To assess change, the TOPs is completed every six months, as per government guidelines. Due to this, the TOPs data are not an accurate representation of a pre and post group measure, e.g. the pre-intervention TOPs could have been completed many weeks before the group and may not represent their functioning immediately at baseline. As this service evaluation was designed before the implementation of the CBT group but after the implementation of the unstructured group, the TOPs was the only outcome measure available for both interventions and was therefore used in the current analysis. The TOPs has 20 questions, and four statements were evaluated: ‘Client’s rating of psychological health (1), physical health (2), quality of life (3)’, and their alcohol consumption (average units per day). The client’s rating of psychological health, physical health and quality of life was scored on a scale of 0 (poor) to 20 (good). The TOPs has high inter-rater reliability and validity (Marsden et al., Reference Marsden, Farrell, Bradbury, Dale-Perera, Eastwood, Roxburgh and Taylor2008). The specific TOPs data being analysed were self-reported alcohol consumption (reported in units), psychological health, quality of life and physical health.
A semi-structured interview schedule was designed which included questions surrounding what the service users found helpful and unhelpful in the group, and anything in the group they would change.
Procedure and data collection
Keyworkers completed the TOPs with the service users and it was uploaded onto a secure sever where the researcher accessed, exported and anonymised the data. For the qualitative evaluation, four service users attended individual interviews with the lead researcher who was also on placement at the service. The interviews were approximately 10 minutes long.
Data analysis
Parametric data were analysed using mixed model ANOVAs: repeated measures and between subjects (psychological health and physical health). Where Box’s test of equality was highly significant and the assumption of homogeneity of variance was violated, non-parametric Mann–Whitney U and Wilcoxon matched pairs tests were used (alcohol consumption and quality of life). Attendance rates were analysed with independent samples t-tests. Withdrawal rates were analysed using chi-squared.
Thematic analysis (Braun and Clarke, Reference Braun and Clarke2021) was used to analyse the qualitative data. An inductive, semantic and latent approach was taken. A semantic and latent approach was taken due to recruitment difficulties and consequently limited data (Robertson et al., Reference Robertson, Zwolinsky, Pringle, McKenna, Daly-Smith and White2013). Initial codes were created, followed by emerging themes. The final two themes were developed from the four working themes. The lead researcher conducted the thematic analysis. The lead research had also co-facilitated the group the four participants attended. The emerging themes were discussed with the lead researcher’s external supervisor.
Results
Quantitative analysis
Table 5 shows alcohol consumption in both groups (alcohol units were average per day). Medians and interquartile ranges were used as non-parametric inferential statistics for this analysis due to the violation of homogeneity of variance. A Mann–Whitney U test indicated there was no significant difference between alcohol consumption in the unstructured and structured CBT groups, U (47,43)=792, z=–1.77, p=.08. Participants were required to be abstinent to attend the group, and likely completed a detoxification within the service or in an in-patient setting prior to attending the group. Therefore, group completion might act as a proxy measure of alcohol consumption. While there was a reduction in both groups’ alcohol consumption, it is important to consider that alcohol consumption is based on descriptive data from self-reports rather than statistical significance testing.
Pre and post descriptives for alcohol consumption and quality of life

Md, median; IQR, interquartile range.
Quality of life was assessed on a 20-point scale, where a score of 20 represents the highest self-reported quality of life. Similarly to above, medians and interquartile ranges were used for this analysis, followed by a Mann–Whitney U test due to the violation of homogeneity of variance. A Mann–Whitney U test was completed to evaluate whether self-reported quality of life differed by group. The results showed there was no significant difference, U=890, z=–.98, p=.33.
Another factor of the TOPs that was analysed was psychological health (scored out of 20). Higher scores indicate higher self-reported psychological health. Table 6 shows the descriptive statistics. A mixed ‘group type’ by ‘time’ ANOVA was conducted to examine the effects of intervention group and time on self-reported psychological health. The results showed a significant main effect of time indicating psychological health was significantly better after the intervention than before, F(1,88)=134.65, p<.001, η2 p=.61. There was no significant interaction between ‘group type’ and ‘time’, suggesting the increase in psychological health did not statistically differ between the two groups, F(1,88)=.18, p=.67.
Pre and post descriptive statistics for psychological health and physical health

M, mean; SD, standard deviation. *Significant main effect of time.
Physical health was evaluated through the TOPs. Higher values indicate higher self-reported physical health (scored out of 20). Another mixed model ANOVA was conducted to examine the effects of ‘group type’ and ‘time’ on self-reported physical health. There was a significant main effect of time, F(1,99)=36.57, p<.001, η2 p=.29. This indicates physical health had significantly increased after the intervention. The interaction between group and physical health was not significant, F(1,88)=.46, p=.50, suggesting the increase of physical health unlikely differed between groups.
To see whether there was a difference in engagement between the groups, attendance rates were compared using an independent samples t-test. Attendance was measured on the percentage of sessions the service user attended. On average, service users in the structured CBT group attended significantly more sessions (50.97% vs 25.53%), t 88=–5.10, p<.001, highlighting a possible association between the structured CBT group and greater attendance. The results showed significantly higher overall completion rates following the structured CBT group compared with the unstructured group (93.02% completion compared with 74.47%) (see Table 7). A chi-squared test of independence was conducted to determine a difference between the completion and withdrawal rates. The chi-squared showed there was a significant difference in proportion of those who completed the intervention (χ2(1,N=90)=5.57, p=.01).
Completion (%) and withdrawal (%) rate

* Chi-squared reported significant difference as proportion of those who completed the programme
** independent samples t-test demonstrated significantly better attendance.
Qualitative analysis
Two main themes were developed from the data.
Theme 1: A sense of belonging
Service users emphasised the significance of interpersonal dynamics within the group, noticing how these interactions helped cultivate a strong sense of belonging. For many, the group became a safe and understanding space and their connection eased their transition into further groups and the community.
Subtheme: Validation through shared understanding
Shared experiences played a role in helping the service users feel validated and understood. For some service users, the group potentially offered the understanding they wanted but did not receive elsewhere. For example, Davide spoke to the difference between his family’s expectations and the group’s: ‘My brother and family think I should still drink … but the group understand’.
Subtheme: Building confidence and easing engagement
Service users spoke of spending time together, knowing who would be in the group and how this eased them into feeling confident to share. Josie noted how the group dynamics helped ease interactions: ‘We were really fortunate to get a good group… we bonded well’.
Service users who initially expected to feel hesitant about sharing experiences found themselves surprised by how quickly they adapted, possibly due to the group’s support:
‘I would have thought I would be shy in the group but I felt comfortable and relaxed to get involved’ – Lucy.
Furthermore, service users described how the group helped increased confidence and engagement within the service:
‘The group has led me to do all those things… it builds confidence… it gets you to know the service and the people doing the course’ – Kate.
The quotes identified here highlight the role interpersonal relationships had throughout the group and how they affected a shared understanding, and in turn a sense of belonging. By sharing experiences and supporting one another, the service users established a foundation of trust and empathy.
Theme 2: Accessibility
Accessibility was explained through creating a greater understanding of the self and the flexibility of the group. Together, these subthemes highlight how the group was designed to be inclusive, adaptable and supportive of diverse needs and learning styles.
Subtheme: Developing a greater understanding of the self
Many service-users reflected on how they found the group content helpful in highlighting a wider understanding of their difficulties, particularly their emotions and triggers. This process was potentially integral to their journey and ability to engage with the group:
‘The emotions and how they work was quite helpful’ – Davide.
‘Learning about triggers and stuff was really helpful like I never really knew my triggers’ – Kate.
This indicated that the session materials were easy to understand and relevant. By making complex concepts approachable it potentially empowered the service users to develop a better understanding of their needs, supporting the idea that the group was accessible.
Subtheme: Flexibility
The flexibility of the group was commented on by some of the service users. Positively, they spoke to being able to re-do sessions they missed due to clashing appointments, potentially providing a sense of reassurance and continuity:
‘I missed a few sessions because of physiotherapy… but I have been able to re-do them’ – Davide.
‘I did an extra week because I couldn’t make my final week which I liked’ – Kate.
However, flexibility was not without its challenges. Davide mentioned the length of the sessions, potentially not being as flexible as he liked as it was quite long:
‘Sometimes maybe just too long … I am like a child and can’t sit for a long time’ – Davide.
This also highlighted perhaps the need to be re-engaged and further adjustments to be made for service users who may struggle with attention. Another service user occasionally had to leave early due to childcare but did not find this to be an issue, possibly highlighting the design of the group balancing inclusivity with practicality, and thus the flexibility of the group:
‘The only problem I had was when the kids were off school … or pick up time was quite tight … but I wouldn’t expect the group to be changed just for me’ – Lucy.
Josie spoke of the different ways of learning that were incorporated into the sessions – visual, auditory, and kinesthetics. These examples potentially highlighted the flexibility and accessibility of the group because there were multiple ways of learning:
‘I think the visual part, the writing on the board which was backed up with sheets and when people learn in different ways like visual audio kinesthetics it covered everything’ – Josie.
The reflections shared by service users demonstrated the accessibility of the group was multi-faceted by encompassing both practical flexibility and thoughtful content through relevant and easy-read materials. The balance of structure and adaptability was key to ensuring the group was inclusive and supportive for a wide range of participants.
Discussion
This evaluation demonstrated that while both group interventions increased treatment outcomes, a structured CBT group had significantly higher attendance rates and had 3.6 times fewer treatment withdrawals than the unstructured group, suggesting an association between the structured group and increased engagement. Alcohol consumption reduced in both the unstructured and structured CBT group, with no significant difference between groups, and all service users who completed the group were abstinent from alcohol, again bringing the reader’s attention to the self-report of these data. The TOPs showed self-reported psychological health, quality of life and physical health increased in both the groups, with no significant difference between groups, suggesting that the increased self-reported data might not be due to the difference in intervention. As discussed previously, the TOPs data were not collected at pre- and post-group timeframes and therefore the changes cannot be directly attributed to the group intervention. Of significance, attendance rates increased, with service users attending an average of 50.97% of sessions in the structured CBT group compared with 25.53% of sessions in the unstructured group. Significantly more participants completed the structured CBT group, compared with the unstructured group (93.02% compared with 74.47%).
Critically, as this was an abstinence-based group, engagement with the group may act as a proxy measure for abstinence. If service users had a relapse and were no longer committed to abstinence, the group was no longer appropriate for them and they were supported instead through one-to-one key working sessions and the option of alternative groups. The higher engagement rates may be associated with service users using the structured CBT group and subsequently who were more likely to remain abstinent. For both groups, self-reported abstinence was supported by random breathalysing. Typically, participants would be breathalysed twice over the 12-group programme. However, abstinence was predominantly self-reported, and therefore further work would be needed to confirm the relationship between abstinence and engagement. Moreover, in the structured CBT group, the facilitators sent reminder text messages and text messages if someone had not attended, which also might explain the difference in attendance. The qualitative analysis identified two emerging themes: a sense of belonging and accessibility. All service users commented positively on feeling understood by one another and creating a bond, alongside feeling the group was accessible and inclusive.
Engagement is important for quality improvement (McLellan et al., Reference McLellan, Chalk and Bartlett2007), especially since engagement and successful treatments are low within addictions (Gilchrist et al., Reference Gilchrist, Langohr, Fonseca, Muga and Torrens2012; National Drug Treatment Monitoring System, 2024a, 2024b). With higher attendance and completion rates demonstrated, this evaluation adds to the body of research that has found positive outcomes when working with individuals with alcohol use problems within a CBT framework (Chen et al., Reference Chen, Qian, Sun, Lin and Tang2019; Dutra et al., Reference Dutra, Stathopoulou, Basden, Leyro, Powers and Otto2008; Magill and Ray, Reference Magill and Ray2009; Peng et al., Reference Peng, Zhang, Yang, Wang, Kang, Zhu, Pan and Xu2022). Service users’ feedback valuing the flexibility mirrors the findings of Dance et al. (2004), demonstrating the need for flexibility when trying to reach marginalised individuals.
Further feedback from the service users encompassed a sense of belonging and a lack of judgement within the group. All four service users spoke about building relationships based on understanding and empathy, and how there was a relaxed and welcoming atmosphere. Previous research has highlighted barriers in accessing services might be due to stigmatisation and discrimination (Link et al., Reference Link, Struening, Rahav, Phelan and Nuttbrock1997; Livingston, Reference Livingston2020). The group may have provided an antidote to this. Service users demonstrated an emotional and physical connection to the group, which Craig (Reference Craig1985) has proposed could be linked to withdrawal rates. It may be that the experience of having their presence missed and receiving a message when they did not attend helped create a healthy attachment to the group. The sense of belonging and flexibility, alongside feeling connected to the structured CBT group, could have been associated with the difference in attendance and completion rates.
Limitations
This evaluation was limited by use of the TOPs. In line with government guidelines, the TOPs should be completed every six months, as change unlikely occurs quickly (Marsden et al., Reference Marsden, Farrell, Bradbury, Dale-Perera, Eastwood, Roxburgh and Taylor2008). Therefore, the TOPs completion in this project is not a representative pre and post measure for the group, rather a measure that was completed twice within a six-month time period during which the group will have occurred. We cannot be sure changes from the TOPs were due to the group and thus causation cannot be assumed. For future projects, it could be beneficial to complete the TOPs directly after the group. Measures such as the Penn Alcohol Craving Scale (Flannery et al., Reference Flannery, Volpicelli and Pettinati1999), or the Brief Situational Confidence Questionnaire (Breslin et al., Reference Breslin, Sobell, Sobell and Agrawal2000) could provide deeper insights into psychological outcomes. Future evaluations should measure how long abstinence was sustained following the group. Another potential limitation of the TOPs was that as it was used as a measure of service performance, it may be vulnerable to manipulation, impacting validity, and offering an alternative explanation for uniformly improved scores (Bevan and Hood, Reference Bevan and Hood2006).
The qualitative analysis was limited by short interviews, providing a small number of themes with minimal coded data. Additionally, the sample size was small and only representative of the structured CBT group and the results miss a comparative element with the unstructured group highlighting a further limitation of the qualitative aspect of this evaluation. Due to this, the results from the interviews may lack generalisability and the themes identified may be more situated as emerging themes, rather than concrete themes. The emerging themes appear more linked to group processes, rather than specifically related to CBT (Yalom and Leszcz, Reference Yalom and Leszcz2020). A further limitation with this analysis was that the lead researcher conducted the interviews as well as co-facilitated the groups the service user participated in, possibly increasing participant bias. In future research, it could be advantageous to interview a wider range of service users.
Absence of a formal measure of fidelity to the treatment manual represents a further limitation. While a formal measure of fidelity was not utilised, a registered clinical psychologist observed a full cycle of the structured group to help ensure fidelity. It is anticipated that this approach will have contributed to the outcomes; however, due to the study design, it was not possible to formally evaluate this.
A final limitation was the lack of insights into diversity. The structured CBT group was created with easy-read materials. It would have been beneficial to specifically explore whether these individuals felt their needs were met appropriately.
Conclusion
This evaluation has outlined two different approaches to facilitating groups for service users with AUD. It has demonstrated both groups showed positive outcomes for psychological health, quality of life and physical health. There was, however, greater engagement in the structured CBT group. Due to limitations in the study design, it was unclear whether increased engagement was attributable to the introduction of the CBT structure, or other factors such as greater follow-up with service users outside of group sessions; therefore, it remains an association. It might be beneficial for commissioners and those managing services to ensure sufficient registered psychological professionals are in place to establish and sustain structured groups and ultimately to support the recovery of service users with AUD.
Key practice points
-
(1) There is an increase in AUD across the UK, alongside co-occurring mental health needs, highlighting a need for effective treatment.
-
(2) A structured CBT group can double engagement with treatment and improve treatment retention 3.6-fold, over an unstructured approach. A group intervention can provide a sense of belonging, validation, build confidence, and act as a stepping stone to other interventions. A flexible approach is recommended to accommodate service users’ other needs.
Data availability statement
Data is available upon reasonable request to the corresponding author.
Acknowledgements
The authors wish to thank the service users and team at Via Greenwich who supported this project.
Author contributions
Rosie Delchiappo: Conceptualization (supporting), Data curation (lead), Formal analysis (lead), Investigation (lead), Methodology (lead), Project administration (lead), Resources (lead), Validation (equal), Visualization (equal), Writing - original draft (lead), Writing - review & editing (supporting); Michelle O’Sullivan: Conceptualization (lead), Data curation (supporting), Formal analysis (supporting), Investigation (supporting), Methodology (supporting), Resources (supporting), Supervision (lead), Validation (equal), Visualization (equal), Writing - review & editing (lead).
Financial support
The research did not receive any specific grant from funding agencies.
Competing interests
The authors declare none.
Ethical standards
All authors have abided by the Ethical Principles of Psychologists and Code of Conduct as set out by the BABCP and BPS. Ethical approval was obtained from Canterbury Christ Church University and Via. Informed consent from participants was obtained for data to be collected, and used to write the report.





 Open access
Open access
Comments
No Comments have been published for this article.