


Introduction
The World Health Organization has referred to spirituality as an important dimension of quality of life (World Health Organization 2003). In Japan, hospice and palliative care have expanded discussions on end-of-life care to include spiritual pain care. However, there is no equivalent Japanese term for “spiritual pain,” and the concept has not been clearly defined.
For cancer patients, documented spiritual pain includes despair, loss of autonomy, loss of control, loss of a sense of self-continuity, issues with relationships/isolation, a sense of meaninglessness, and loss of a sense of dignity. Consistent with many empirical studies in Western cultures, Morita et al. (Reference Morita, Sakaguchi and Hirai2004) conducted a study on spiritual challenges among end-of-life cancer patients receiving specialized palliative care in Japan, categorizing them as: “relationship distress,” “loss of control,” “a sense of being a burden on others,” “loss of a sense of continuity,” “distress over unaccomplished life tasks,” “hope/hopelessness,” and “acceptance/readiness”, clearly defining spiritual pain as an important dimension when discussing spiritual care for end-of-life cancer patients. Murata defined spiritual pain among end-of-life cancer patients as, “pain arising from the disappearance of one’s own existence and a sense of meaning,” and clarified the formation and construct of spiritual pain experienced by such patients (Murata Reference Murata2003). Using the conceptual framework of Murata (Reference Murata2003), Tamura et al. (Reference Tamura, Ichihara and Maetaki2006) developed an evaluation sheet, Spiritual Pain Assessment Sheet (SpiPas), to measure spiritual pain experienced by cancer patients, and demonstrated that this could be an appropriate assessment tool.
As with cancer patients, caregivers also often experience spiritual pain after the patient’s death. Studies have reported that bereaved caregivers experience spiritual pain, such as a loss of purpose and a loss of identity as a couple (Ikuta Reference Ikuta2011; Miyabayashi Reference Miyabayashi2016). Caregiving for an end-of-life family member can lead to psychological distress and spiritual pain, which may persist even after the patient’s death (Murray et al. Reference Murray, Kendall and Boyd2010). To provide appropriate care for caregivers, it is crucial to continuously assess their spiritual pain (Huang et al. Reference Huang, Tai and Longcoy2021).
However, to our knowledge, no quantitative scale has been developed to assess the unique spiritual pain experienced by bereaved caregivers of cancer patients in Japan. Therefore, this preliminary scale development aims to explore and clarify the structure of spiritual pain among bereaved caregivers of cancer patients using data from the J-HOPE4 survey.
Methods
Study population
Certain caregivers were excluded from the study: (1) Caregivers who, at the time of discharge, were considered unable to complete the questionnaire due to cognitive impairment, psychiatric disorder, visual impairment, or other similar conditions; (2) caregivers who were judged to be in a markedly unstable psychological condition at the time of discharge or at present, such that participation in the study was deemed inappropriate; (3) caregivers for whom participation was considered inappropriate based on a comprehensive multidisciplinary assessment (including physicians and nurses), particularly in cases of strong dissatisfaction with medical care, significant misunderstanding of treatment, or severely impaired relationships with healthcare professionals. We acknowledge that this exclusion criterion may have introduced selection bias by excluding caregivers with potentially different experiences of spiritual pain.
All regular members of the Japan Hospice and Palliative Care Association (as of July 1, 2017) were asked to participate. General and palliative care wards of various hospitals that agreed to participate were included in this study. The study was restricted to participants meeting the following eligibility criteria: (1) Bereaved family members (primary family caregiver or legal representative) of patients who died of cancer at the participating institutions; (2) patients aged 20 years or older at the time of death; (3) bereaved family members aged 20 years or older.
At the medical personnel’s discretion, we excluded cases involving: (1) Patients whose caregivers could not be identified; (2) patients who died from treatment-related or ICU complications; (3) caregivers who, at the time of hospital discharge, were deemed unable to complete the survey because of impairments such as dementia or mental or visual disabilities; (4) caregivers who were judged to be in a markedly unstable psychological condition at the time of discharge or at present, such that participation in the study was deemed inappropriate; (5) cases involving patients who were severely dissatisfied, did not understand the medical care received, or had extremely poor relations with medical personnel.
Questionnaire for the survey
Previous studies by Ikuta (Reference Ikuta2011) on older bereaved spouses and Miyabayashi (Reference Miyabayashi2016) on bereaved individuals participating in family bereavement care have shown that bereaved individuals experience a loss of meaning, value, and purpose. We define spiritual pain among caregivers of cancer patients as “the various distresses that arise when the caregiver becomes aware of the ‘finiteness’ of the patient’s life.” The SpiPas developed by Tamura et al. (Reference Tamura, Ichihara and Maetaki2006) comprises categories used to assess the presence or absence of spiritual pain and the nature of distress manifested by spiritual pain. The SpiPas evaluation sheets for cancer patients include 14 conceptual categories. Additionally, as the multifaceted suffering of cancer patients affects family members’ psychological and spiritual aspects, bereaved caregivers also have spiritual needs (Murray et al. Reference Murray, Kendall and Boyd2010; Huang et al. Reference Huang, Tai and Longcoy2021). A pilot survey was conducted with 5 bereaved caregivers, before the study. The established questions were then administered in person to the caregivers, who were asked to rate the validity and ease of understanding. We formulated 35 items to assess spiritual pain among bereaved caregivers of cancer patients, based on prior qualitative studies and the conceptual framework of spiritual pain, including reference to the SpiPas framework. A complete list of the questionnaire items is presented in Figure 2.
Study methods and statistical analysis
A self-administered questionnaire, the Spiritual Pain Questionnaire for Bereaved Caregivers of Cancer Patients, was sent out to participants between July and September 2018, and no reminders were sent out to those who did not respond. The participants were asked to rate the relative significance of spiritual pain on a 7-point Likert scale (from 1: strongly disagree, to 7: strongly agree). The weighted average factors of the question groups were used to evaluate spiritual pain, with factors of 4 or higher classified as “yes,” and factors below 4 as “no.” To clarify the nature of spiritual pain among caregivers, we created a questionnaire and conducted exploratory factor analysis (EFA). The EFA was conducted using the Promax rotation method, and confirmatory factor analysis was performed for each construct. All analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
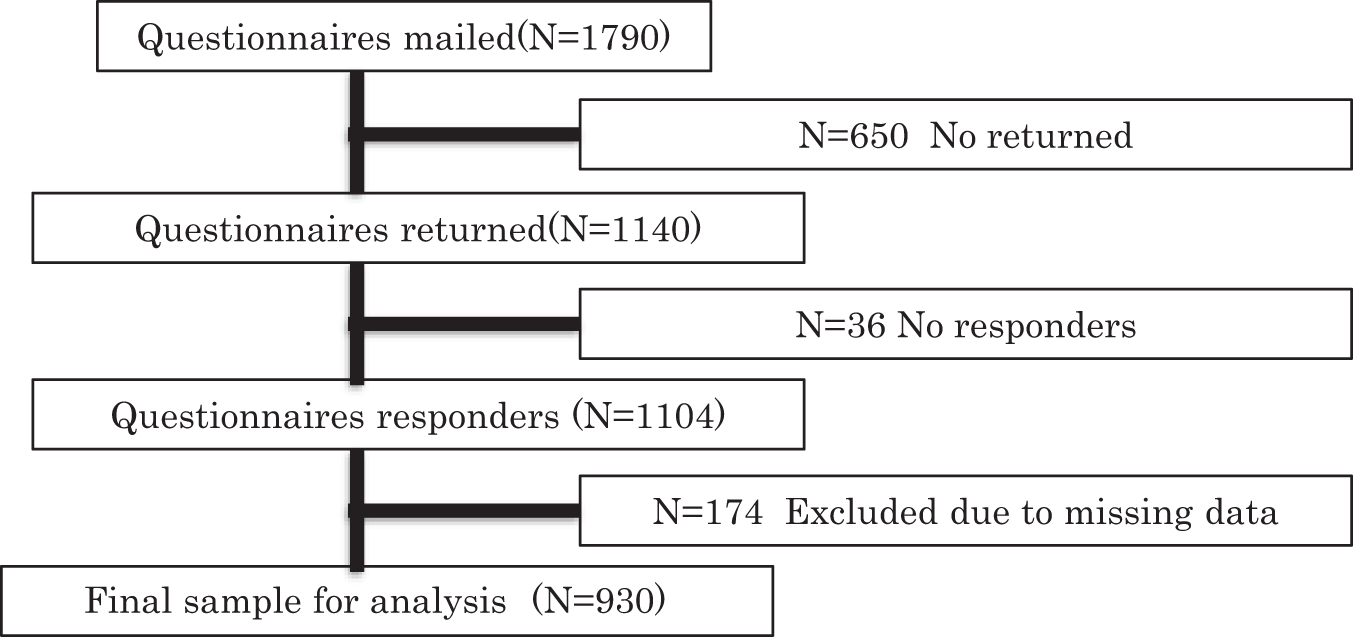
A total of 1790 questionnaire packets, including background information forms, were mailed to potential participants. Of these, 1140 responses were returned, of which 174 were excluded due to missing data. This resulted in a final sample of 930 individuals in the analysis, for whom both patient and caregiver information were available (Figure 1). Table 1 shows caregiver and patient backgrounds.
Flowchart of the study participant selection process, including the number of questionnaires mailed, returned, and excluded, resulting in the final sample sizes for groups.

Figure 1 Long description
The flowchart illustrates the study participant selection process. It begins with 'Questionnaires mailed (N=1790).' From this, 'N=650 No returned' is noted. Next, 'Questionnaires returned (N=1140)' is shown, followed by 'N=36 No responders.' The next step is 'Questionnaires responders (N=1104),' with 'N=174 Excluded due to missing data.' The final step is 'Final sample for analysis (N=930).' Each step is connected sequentially, showing the reduction in sample size at each stage.
Caregiver and patient’s background

Table 1 Long description
The table summarizes demographic and clinical background characteristics for caregivers (930 respondents) and patients (1104 respondents), reporting counts and percentages for categories and average age with standard deviation. Among caregivers, 62.3% were female and 37.7% were male, with an average age of 63.0 years. Caregivers were most often spouses (48%) or adult children (36%), with very small numbers in other relationship categories and a small no-response group. Among patients, 58% were male and 42% were female, with an average age of 73.3 years. Patients were split between palliative care units (58%) and general wards (42%). The most common primary cancer sites were “others” (26%) and lung (21%), followed by gastric or esophageal (13%), colorectal (12%), and liver, biliary tract, or pancreatic (11%). Patient marital status was most often married (54%), with widowed (17%) and no response (20%) also notable; percentages may not sum to 100 due to rounding or missing responses.
N indicates the number of participants, and % indicates the percentage of the total number of respondents for each item. Continuous variables (age) are presented as mean ± standard deviation (SD), and categorical variables are presented as number (N) and percentage (%). Percentages may not total 100% due to rounding or missing responses.
Spiritual pain
Table 2 summarizes the results of the EFA into question items with an effect size of 0.3 or greater. In the main factor analysis, a scree plot was created, and 7 constructs with effect sizes of 1 or greater were determined appropriate. The spiritual pain of the caregivers was categorized into the following constructs, along with the corresponding question items. Loneliness (1: I wondered what would happen to me if the patient died; 2: I thought there would be nothing left for me if the patient died; 3: I thought about what would happen to me in the future; 4: I was afraid of being alone; 5: I felt all alone; 6: I thought I would lose my sense of belonging; 7: I questioned what my life had been all about; 8: I thought death was approaching for me, too; 9: I found that my future was not what I had envisioned; 10: I felt helpless), Life’s heartlessness (11: I felt life was impermanent; 12: I felt that life was unfair; 13: I felt the vanity of human life; 14: I felt the absence of God or Buddha; 15: I found it hard to resist fate), A sense of unfinished business (17: I wished I could talk to the patient about unresolved issues and putting personal matters in order; 18: I wished I could spend more time with the patient; 19: I was pained because I felt the patient had unfinished business; 20: I was pained knowing the patient would not see his/her children and grandchildren grow up; 21: I found that I would no longer be able to care for the patient; 22: I wished I had discovered the patient’s disease earlier), Distress over patient deterioration (23: It was painful to see the patient deteriorate; 24: It was painful to see the patient lose the ability to tend to his/her own matters; 25: It was painful to see the patient trying to act strong, Remorse (26: I felt I was to blame for the patient’s ailment; 27: I felt remorse over what has happened to the patient), Regret (30: I felt frustrated because my job, role, hobbies, etc., were restricted; 31: I thought my efforts to help the patient get better were futile), A sense of loss (33: I felt I would lose the history I shared with the patient; 34: I felt I would lose a part of me). The Cronbach’s α reliability coefficients were as follows: Overall (0.94); Loneliness (0.90); Life’s heartlessness (0.83); A sense of unfinished business (0.77); Distress over patient deterioration (0.84); Remorse (0.74); Regret (0.36); and A sense of loss (0.65).
Exploratory factor analysis of spiritual pain for bereaved caregivers of cancer patients

Table 2 Long description
The table reports an exploratory factor analysis of a spiritual pain questionnaire for bereaved caregivers, listing 35 items with factor loadings on seven factors, plus communality, sample size, item mean, and standard deviation. The seven factors are labeled Loneliness, Life’s heartlessness, Unfinished business, Distress over patient, Remorse, Regret, and Sense of loss. Loneliness items show very strong loadings, including worry about what happens to oneself if the patient dies and fear of being alone, with loadings around 0.78 to 0.89 and communalities up to about 0.80. Distress over patient is the most sharply defined factor, with two items about seeing the patient deteriorate or lose independence loading around 0.87 to 0.95 and high communalities around 0.77 to 0.87. Life’s heartlessness also loads strongly, especially feeling life is impermanent or unfair, with loadings around 0.83 to 0.88. Unfinished business items load moderately to strongly, including wishing for more time and unresolved issues, with loadings around 0.52 to 0.67. Remorse includes self-blame and remorse items with loadings around 0.84 to 0.86, while Regret has weaker and more mixed loadings and the lowest internal consistency among factors. Sense of loss includes losing shared history and part of oneself, with the strongest item loading around 0.67; overall scale reliability is high, but some items show cross-loadings and lower communalities, so factor labels should be interpreted cautiously.
Bold values indicate the primary factor loading (i.e., the highest factor loading) for each item and were used to identify the factor to which each item was assigned.
The 35 Items of the Spiritual Pain Questionnaire for Bereaved Caregivers.

Figure 2 Long description
1. I wondered what would happen to me if the patient died. 2. I thought there would be nothing left for me if the patient died. 3. I thought about what would happen to me in the future. 4. I was afraid of being alone. 5. I felt all alone. 6. I thought I would lose my sense of belonging. 7. I questioned what my life had been all about. 8. I thought death was approaching mecomma too. 9. I found that my future was not what I had envisioned. 10. I felt helpless. 11. I felt life was impermanent. 12. I felt life was unfair. 13. I felt the vanity of human life. 14. I felt the absence of God or Buddha. 15. I found it hard to resist fate. 16. I wondered why the patient got the disease. 17. I wished I could talk to the patient about unresolved issues and putting personal matters in order. 18. I wished I could spend more time with the patient. 19. I was pained because I felt the patient had unfinished business. 20. I was pained knowing the patient would not see hisdivided byher children and grandchildren growing up. 21. I found that I would no longer be able to care for the patient. 22. I wished I had discovered the patient’s disease earlier. 23. It was painful to see the patient deteriorate. 24. It was painful to see the patient lose the ability to tend to hisdivided byher own matters. 25. It was painful to see the patient trying to act strong. 26. I felt I was to blame for the patient’s ailment. 27. I felt remorse over what has happened to the patient. 28. I felt I could do nothing about the patient’s pain. 29. I thought the patient had been abandoned by the medical staff. 30. I felt frustrated because my jobcomma rolecomma hobbiescomma etc.comma were restricted. 31. I thought my efforts to help the patient get better were futile. 32. It was hard not being able to talk to the patient about my own predicament. 33. I felt I would lose the history I shared with the patient. 34. I felt I would lose a part of me. 35. It was painful to see the patient being hopeful.
Discussion
The constructs of spiritual pain among bereaved caregivers of cancer patients may include Loneliness, Life’s heartlessness, A sense of unfinished business, Distress over patient deterioration, Remorse, A sense of loss, and Regret. The following is a discussion on each of these constructs. Loneliness: The experience of losing the patient caused the bereaved to question their own existence or to experience spiritual pain, such as not knowing how to continue their lives. This is similar to a loss of the meaning of existence, as outlined in a study on older adult bereaved caregivers who lost spouses (Ikuta Reference Ikuta2011). Previous studies have shown that losing a loved one can lead to feelings of loneliness and isolation (Rokach Reference Rokach2000; Stroebe et al. Reference Stroebe, Schut and Stroebe2007). Our findings were consistent with these studies, but also revealed that loneliness was related to a loss of purpose and direction in life. Healthcare providers can support bereaved caregivers by acknowledging their loneliness and providing opportunities for social connection, such as bereavement support groups, and exploring ways to help them find new sources of meaning and purpose. Life’s heartlessness: When faced with the patient’s inevitable death, the bereaved were unable to accept reality, and seemed as if they were clutching at straws. This represents the caregiver’s feelings of resignation to the fact that fate cannot be resisted, despite their strong desire for the patient to live or recover even a little. The concept of spirituality originated from the religious background of Western countries. On the other hand, Japan may be unique in having little religious support for people to turn to when faced with the inevitability of death. Studies have shown that confronting the fragility of life and the inevitability of death can be a profound source of distress for caregivers (Adelbratt and Strang Reference Adelbratt and Strang2000; Sand and Strang Reference Sand and Strang2006). Our findings align with these studies, but also reveal that life’s heartlessness is associated with feelings of unfairness and a struggle to find meaning in loss. Healthcare providers can address this aspect of spiritual pain by providing opportunities for caregivers to explore their existential concerns, find ways to make meaning in their experiences, and develop resilience. A sense of unfinished business: Faced with the fact that the patient had no future, caregivers felt regret about what the patient had left undone, and about their own failure to confirm and discuss the patient’s wishes regarding matters after death. Bereaved caregivers may feel distressed when they perceive that the patient had a sense of having unfinished business. However, this may be alleviated by support from medical personnel. Studies have shown that a sense of unfinished business is a common source of distress for patients and caregivers at the end of life (Klingspon et al. Reference Klingspon, Holland and Neimeyer2015; Yamashita et al. Reference Yamashita, Arao and Takao2017). Our findings were not only consistent with these studies, but also revealed that caregivers experienced spiritual pain related to their own sense of unfinished business. Healthcare providers can help alleviate this pain by providing opportunities for life review and closure, such as facilitating discussions between patients and caregivers about end-of-life matters. Distress over patient deterioration: Witnessing the patient’s loss of autonomy is a definite component of spiritual pain. In Japan, it is said that patients feel an especially severe spiritual pain when they must depend on others to take care of their toileting needs. The caregivers also felt pained when the patient was unable to independently address personal needs. Studies have shown that witnessing the decline and suffering of a loved one can be a profound source of distress for caregivers (Proot et al. Reference Proot, Abu-saad and Crebolder2003; Grunfeld et al. Reference Grunfeld, Coyle and Whelan2004). Our findings were consistent with these studies, but also revealed that caregivers experienced specific distress related to the patient’s loss of autonomy and ability to perform self-care tasks. Healthcare providers can support caregivers by acknowledging this pain, providing education and support to manage the practical and emotional challenges of caregiving, and offering opportunities for respite and self-care. Remorse: Caregivers tended to blame themselves, wondering if things would have turned out differently, had they noticed a change in the patient, and prompted earlier treatment. They also considered that the patient’s predicament was in some way attributable to a failing on their part. Studies have identified remorse as a common source of distress for caregivers (Waldrop Reference Waldrop2007; Spillers et al. Reference Spillers, Wellisch and Kim2008). Our findings aligned with these studies, but also revealed that remorse was correlated with psychological distress. Healthcare providers can address this aspect of spiritual pain by providing opportunities for caregivers to express their emotions, challenge self-blaming thoughts, and find a sense of forgiveness and acceptance through bereavement counseling and support groups that incorporate cognitive-behavioral techniques. A sense of loss: In losing their relationship with the patient, bereaved caregivers felt pain, as if they were losing a part of themselves. Studies have established that losing a loved one to cancer can lead to feelings of emptiness, loneliness, and a struggle to find meaning in life (Kim et al. Reference Kim, Carver and Spiegel2017). Our findings were not only consistent with these studies, but also revealed that caregivers experienced spiritual pain related to losing their shared history and a part of themselves. Healthcare providers can support bereaved caregivers by acknowledging and validating their loss, providing opportunities to share their stories, express their grief, and find ways to maintain a connection with the patient’s memory through bereavement support groups and individual counseling. Regret: Bereaved caregivers felt as though the very foundation of their lives up to that point had been shattered, or that they had lost everything in life that they could rely on. They tended to lose hope and a sense of purpose, and experienced intense emotional turmoil (anxiety, fear, frustration, and grief). Caregivers felt a sense of regret upon seeing the patient become ill and were inevitably forced to change their lifestyle, in accordance with factors such as nursing requirements. Studies have shown that regret is a prevalent experience among bereaved caregivers (Waldrop Reference Waldrop2007; Spillers et al. Reference Spillers, Wellisch and Kim2008). Our findings were consistent with these studies, but also revealed that regret was associated with a loss and a shattering of life’s foundation. Healthcare providers can help address this pain by providing opportunities for caregivers to express their regrets, re-frame their experiences, and find a sense of forgiveness and acceptance through bereavement counseling and support groups that incorporate narrative therapy techniques. With regard to Regret, the influence of psychiatric disorders such as depression cannot be excluded. It should be acknowledged that, these factors may have been influenced by psychiatric disorders such as depression, and may not have precisely represented spiritual pain. When considering spiritual pain, depression is a factor that must necessarily be excluded. Future research should devise questionnaires that strictly distinguish spiritual pain from psychiatric disorders such as depression.
Although no previous studies have evaluated the spiritual pain of bereaved caregivers, it is interesting to note how the spiritual pain felt by cancer patients highlights the characteristics of their bereaved caregivers in comparison. Bereaved caregivers share the same categories of spiritual pain that Morita et al. (Reference Morita, Sakaguchi and Hirai2004) outlined for patients: Questioning the Meaning of Life; Anxiety about Death; Loss of Dignity; Guilt; Grief over the Reality of Oneself; Loss of Relation; and Desire for Transcendent Existence. However, A sense of unfinished business and Regret are not among Morita et al.’s constructs of spiritual pain, and can be understood as spiritual pain unique to the bereaved. Comparing the findings of Morita et al. with those of Tamura et al.’s (Reference Tamura, Ichihara and Maetaki2006), SpiPas suggests that spiritual pain among the bereaved caregivers of cancer patients is characterized by a strong correlation with relationship dimensions, such as Loneliness and Life’s heartlessness. When spiritual pain is recognized for the bereaved caregivers of cancer patients, it is likely that they would desire help from healthcare providers. It is thus imperative for providers to openly inquire about how they may respond and help. Depression and complicated grief in bereaved caregivers may reduce their quality of life and place them at risk of suicide and social challenges. Therefore, prudent support is needed for bereaved caregivers. It is of clinical advantage for healthcare providers to screen for spiritual pain to predict these issues. This 7-factor structure is similar to the factor structure of spiritual pain experienced by cancer patients, as identified in previous studies, suggesting commonalities in the spiritual pain experienced by cancer patients and their bereaved caregivers. However, A sense of unfinished business and Regret are not included in the factors of spiritual pain experienced by cancer patients and can be considered unique to bereaved caregivers. A strength of this study is that it is the first to clarify the spiritual pain of bereaved caregivers of cancer patients in Japan. This study revealed that the spiritual pain experienced by bereaved caregivers consists of 7 key constructs: Loneliness; Life’s heartlessness; A sense of unfinished business; Distress over patient deterioration; Remorse; Regret; and A sense of loss. While there are commonalities between the spiritual pain experienced by cancer patients themselves and that of their bereaved caregivers, the constructs of A sense of unfinished business and Regret appear to be unique to caregivers. This suggests that these aspects play a crucial role in their grieving process. In clinical settings, a systematic assessment of these factors is essential to ensure that bereaved caregivers receive appropriate support. Furthermore, preliminary scale development provides a foundation for the future of cancer patients and their caregivers. Specifically, it can serve as a basis study for developing effective intervention strategies to alleviate spiritual pain and improve the quality of life for both cancer patients and their bereaved caregivers.
Importantly, the present findings do not allow for a clear distinction between spiritual pain and depressive symptomatology. Several identified domains, such as loss, helplessness, and emotional burden, may conceptually overlap with general psychological distress, including depression.
Because depressive symptoms were not assessed in this study, the discriminant validity of the proposed construct remains uncertain. Future studies incorporating validated measures of depression (e.g., Patient Health Questionnaire-9 [PHQ-9]) will be essential to determine whether the identified factors capture aspects of spiritual pain that are distinct from depressive states.
Accordingly, the current findings should be interpreted as preliminary with respect to construct validity.
In addition, the internal consistency of the “Regret” factor was relatively low, suggesting potential limitations in its stability as a subscale. This may reflect heterogeneity in the underlying construct or insufficient item representation.
Further refinement of this factor is warranted in future scale development, including potential revision or expansion of items. Validation studies using independent samples will be necessary to confirm its robustness.
Limitations of the study
There are critical limitations to this study. First, the survey was conducted only once, and very little information was provided regarding the detailed background of participants. Longitudinal studies are needed to understand how spiritual pain evolves over time during bereavement.
Furthermore, the questionnaire items were created based on previous studies and a pilot survey, and both validity testing and the main survey were conducted using these same items. In other words, exploration and validation were performed using the same dataset, and the possibility of overfitting must be acknowledged. Hence, this study represents a preliminary scale development. The identified structure may reflect capitalization on chance, and requires replication in independent samples using confirmatory factor analysis.
Moreover, there is an absence of psychiatric assessment, particularly for depression. Depressive symptoms, including feelings of regret, guilt, and hopelessness, may overlap with or confound the experience of spiritual pain. Without controlling for this factor, it is difficult to determine whether the reported experiences reflect spiritual pain, depressive cognition, or a combination of both. Future studies should incorporate validated depression screening tools (e.g., PHQ-9, Center for Epidemiologic Studies Depression Scale [CES-D]) and conduct sensitivity analyses excluding participants with clinically significant depressive symptoms.
It should also be noted that bereaved caregivers may not have participated if they were in extremely poor physical or mental condition, or were suffering from severe grief or depression. Although the overall valid response rate for this study was 60.4%, the possibility of respondent bias cannot be ruled out. In addition, recall bias may have occurred because bereaved caregivers answered the surveys retrospectively. Another problem is that this study was conducted among the bereaved caregivers of cancer patients who died at full-member facilities of Hospice Palliative Care Japan, which may not be a representative sample of all cancer deaths and bereaved caregivers in Japan.
Also, as the survey was conducted with bereaved caregivers, its correlation with the distress felt by cancer patients remains unclear. Further studies are needed to clarify such correlations. Additionally, the Cronbach’s α coefficient for the Regret factor was relatively low, at 0.36, indicating insufficient internal consistency. This suggests that further refinement of the factor structure and survey items is necessary to develop a more reliable and valid scale. Furthermore, as the sample excludes individuals who had poor relationships with medical personnel, the results may be biased in terms of understanding the needs of caregivers. Finally, this study focused solely on the content of caregivers’ spiritual pain and did not explore its relationship with psychosocial factors. Understanding such connections could help healthcare providers develop more effective interventions.
Conclusions
This study conducted a preliminary scale development of the constructs of spiritual pain among bereaved caregivers of cancer patients. The findings contribute to a deeper understanding of the spiritual pain experienced by bereaved caregivers. Future studies should expand the population to explore appropriate responses and interventions for spiritual pain of bereaved caregivers, the correlation between spiritual pain of patients and their caregivers, and the relationship between caregivers’ psychosocial backgrounds and their spiritual pain. This study represents an initial step toward scale development and requires validation in independent samples. Future research should address the limitations identified, particularly the need to control for depression and employ confirmatory factor analysis.
Acknowledgments
The authors express their gratitude to the participants of the study.
Funding
This preliminary scale development was conducted as a specific study of the J-HOPE4 funded by the Japan Hospice Palliative Care Foundation.
Competing interests
The authors declare no competing interests.
Ethical approval
This study was approved by the Ethics Committee of Tohoku University Hospital. Subsequently, it was submitted to the participating institutions’ ethics committees for approval. If the participating institution did not have an ethics committee, a central review board at Tohoku University Hospital was used. Additionally, approval was obtained from the Medical Ethics Review Board of Kyoto University (Approval No. R1664). Data were strictly managed by the study office to protect personal information and ensure that the scores of each participating institution were not revealed to others.




 Open access
Open access