


Introduction
Context and conflict
From its onset in the 1990s, the Karabakh conflict caused widespread suffering and loss in the region, and the surrounding humanitarian situation has remained unresolved and unpredictable for decades. Repeated escalations have shaped the region for over thirty years, creating a persistent sense of insecurity among civilians. Communities living along the international border between Armenia and Azerbaijan have been particularly affected, facing challenges in terms of the safety, security and mental well-being of civilians.
The escalations of the conflict, particularly one in the autumn of 2020, generated profound psychological suffering and long-lasting mental health consequences on the population. Border residents not only faced loss and grief but were also exposed to a significant weakening of individual and collective coping mechanisms. The 2023 escalation triggered the rapid and large-scale movement of more than 100,000 ethnic Armenians from Karabakh to Armenia within a matter of days. This situation increased pressure on already fragile border communities that were struggling with insecurity, uncertainty and scarce resources; at the same time, the people that moved to Armenia arrived in these villages with psychological distress and the potentially traumatic experience of leaving their homes.
ICRC MHPSS interventions in Armenia
Mental health and psychosocial support (MHPSS) is one of the key intervention areas of the International Committee of the Red Cross (ICRC). Through its MHPSS projects, the ICRC aims to address the specific mental health and psychosocial consequences of conflict and different types of violence by promoting individual, family and community coping mechanisms as well as resilience.Footnote 1
Since 2021, the ICRC and the Armenian Red Cross Society (ARCS) have been supporting populations affected by the Karabakh conflict, and those residing in border villages, through a community-based MHPSS programme designed to strengthen coping mechanisms, enhance resilience and reduce vulnerability to mental health problems. The intervention is designed as a comprehensive, multilayered MHPSS programme with a cycle of group sessions at its core, complemented by activities across all levels of the International Red Cross and Red Crescent Movement’s MHPSS pyramid,Footnote 2 including awareness-raising initiatives, psychosocial group activities for children, individual counselling, and referrals for specialized mental health care. These services are delivered by thirteen trained and continuously supervised ARCS counsellors, all of whom come from the very communities they serve. To date, the programme has reached more than 6,000 individuals in over 100 communities.
Need for research
MHPSS interventions addressing the mental health and psychosocial effects of humanitarian crisis have gained greater recognition throughout the past three decades.Footnote 3 There is broad international consensus that multilayered systems of care represent best practice for addressing the wide range of MHPSS needs among people affected by humanitarian crisis.Footnote 4 MHPSS interventions range from the treatment of existing mental health disorders to the prevention of such disorders, as well as the promotion of positive aspects of mental health, including psychological well-being, psychosocial functioning, coping, quality of life and resilience.Footnote 5
Research shows that psychological therapies are effective in decreasing post-traumatic stress disorder, depressive symptoms and anxiety symptoms in adults, adolescents and children facing humanitarian crisis in low- and middle-income countries.Footnote 6 Evidence from ICRC programmes in the Democratic Republic of the Congo, Mali and Nigeria shows that receiving community-level MHPSS was associated with increased well-being among most beneficiaries, with reported reductions in distress and improved daily functioning.Footnote 7
Mental health is increasingly recognized as being more than the absence of disease. The World Health Organization (WHO) defines mental health as “a state of well-being in which every individual realizes his or her own potential, can cope with the normal stresses of life, can work productively and fruitfully, and is able to make a contribution to his or her community”.Footnote 8 While this widely accepted definition aligns with mental health promotion activities, much of the research in humanitarian settings has focused narrowly on post-traumatic stress disorder, depression, anxiety and symptom reduction.Footnote 9 This gap is particularly evident in post-conflict settings such as Armenia, where the absence of standardized, State-regulated MHPSS systems and limited research on community-based psychosocial interventions restricts the understanding of broader outcomes beyond symptom reduction, including well-being, functioning and resilience.Footnote 10 This focus on the treatment of mental health disorders contrasts with the knowledge priorities of MHPSS practitioners and policy-makers, who emphasize the need for more rigorous evaluation of community-based psychosocial support programmes as a key research priority.Footnote 11
In a 2023 article, Tol and colleagues outline the top twenty global research priorities identified by practitioners, policy-makers and researchers.Footnote 12 These emphasize practice-oriented questions related to the impact of MHPSS interventions in humanitarian settings, the comparative effectiveness, efficiency and safety of various MHPSS approaches, and strategies to ensure the sustainability of MHPSS services across diverse sectors and contexts. The agenda also incorporates broader analytical questions aimed at strengthening foundational knowledge, including the identification of key risk and protective factors associated with mental health and well-being in humanitarian environments, as well as the correlates of resilience in these settings.
Several definitions of resilience have emerged within a body of literature that has been growing since the 1970s. Today, the understanding of resilience as a dynamic process of adaptation to adversity is widely accepted.Footnote 13 These resilience processes emerge from interactions among multiple overlapping systems and ecologies across the course of life, including individual traits and behaviours, family and household structures, socio-cultural norms, historical contexts, and policy frameworks.Footnote 14 Although this multi-systemic definition of resilience is of growing interest, psychological research continues to focus on a limited number of systems, often prioritizing individual coping strategies.Footnote 15
Wagnild defines personal resilience as the capacity of individuals to bounce back from life’s challenges, learn from them, and grow. She identifies five underlying characteristics that together form the resilience core: purpose, perseverance, equanimity, self-reliance and existential aloneness (authenticity).Footnote 16 MHPSS interventions can play an important role in building resilience, particularly in settings where persistent stressors cannot be altered;Footnote 17 in line with this, the MHPSS programme discussed in this article aims to contribute to strengthening resilience through multiple components that serve as important supportive factors.
The present study is unique in Armenia, where large-scale investigations on this topic are rare. It examines a community-based MHPSS approach and resilience in a context characterized by recurrent violence. By focusing on implementation and outcomes beyond symptom reduction (including well-being, coping, quality of life and resilience), it directly addresses high-priority questions in the field and aims to provide insights to support practice and strengthen the evidence base for MHPSS programmes in conflict settings.
Primary research objective and research questions
The main objective of the research is to explore how this community-based MHPSS intervention contributes to strengthening the resilience of individuals residing in border communities in Armenia, in the aftermath of conflict and within a context of recurrent violence. To achieve this, the study aims to address the following questions:
• To what extent has participation in MHPSS group sessions helped participants strengthen their resilience?
• Are there positive correlations between perceived changes (in participants’ well-being, family relationships and community support), perceived quality of life and participants’ levels of resilience?
• Is this community-based MHPSS intervention effective, and could it be replicated in other humanitarian contexts?
• What are the programme’s weaknesses, and how could it be improved to enhance effectiveness and impact?
Methodology
Study design
This study employed a quantitative, cross-sectional research design to evaluate the impact of MHPSS group sessions on participants’ well-being, quality of life and resilience. One locally developed questionnaire and two validated standardized measurement tools were administered.
Perceived changes questionnaire
A locally developed instrument was used to assess participants’ self-reported perceptions of change resulting from their participation in MHPSS sessions. The instrument captured perceived improvements across three domains: individual, family and community.
The questionnaire used a five-point Likert scale ranging from “strongly disagree” to “strongly agree”, allowing participants to indicate the extent to which they experienced specific changes. At individual level, items focused on well-being, including reduction of negative feelings, capacity to cope with difficult emotions and situations, self-care practices, mental health awareness and help-seeking behaviours. The family level assessed changes in communication, relationship quality, and the ability to support relatives, including children. The community level explored social connectedness, perceived support, and participants’ capacity to have an active role in their community and help others.
Participants were asked to reflect on their experiences before and after participating in the MHPSS sessions, enabling the assessment of perceived changes over time. They were also encouraged to respond as honestly as possible, with the clarification that there were no right or wrong answers, as the purpose was to understand their personal experiences and perceptions.
The WHO Quality of Life – Brief (WHOQOL-BREF) instrumentFootnote 18
The WHOQOL-BREF is widely used in research and humanitarian settings to assess individuals’ well-being across four life domains: physical health, psychological health, social relationships and environment. It possesses strong cross-cultural validity and strong psychometric properties, and provides a comprehensive overview of individuals’ perception of well-being and functioning.
The original Resilience Scale™ (RS™)Footnote 19
The RS™ is a validated instrument used to evaluate psychological resilience. The construct of resilience was selected as the central focus of this research because it represents a relatively enduring but dynamic construct, reflecting adaptive capacity over time and extending beyond the specific coping strategies that individuals employ in response to situational stressors.Footnote 20 Resilience is understood as a holistic concept shaped by personal traits, life experiences and environmental factors, reflecting an individual’s capacity to adapt, recover and grow from adversity. As such, it functions as a protective factor against life stressors, making it especially relevant to examine and strengthen in contexts of sustained violent environments.Footnote 21 The RS™ assesses five underlying characteristics that together form the resilience core: purpose, perseverance, equanimity, self-reliance and existential aloneness (authenticity). A strong resilience core will support the individual’s capacity to develop and sustain adaptive responses to adversity.
All research tools were translated into Armenian using the WHO standardized translation methodology.Footnote 22 This included forward translation by bilingual experts, back-translation into English by a professional translator, and comparison with the original version to identify discrepancies. A review committee then discussed differences, resolved ambiguities, and adapted culturally sensitive terms to ensure conceptual equivalence. Finally, the Armenian versions were piloted with a small group of participants to test clarity, cultural relevance and comprehension before finalization. This process ensured that the instruments preserved both their linguistic accuracy and cultural validity, allowing reliable data collection across the study population.
To ensure adequate statistical power and representativeness, the sample size was determined using Cochran’s formula.Footnote 23 With a 95% confidence level (Z=1.96), an assumed population proportion of 0.50, and a 5% margin of error (e=0.05), the initial required sample size was calculated as 384.16 respondents. Because the study population was finite (N≈3,000 MHPSS group participants), the value was adjusted using the finite population correction, resulting in a final required sample size of approximately 341 participants. This sample size was selected to ensure precision while maintaining feasibility in field conditions.
Data collection was conducted by thirteen ARCS counsellors and occurred across multiple community settings where MHPSS groups had been implemented. The study relied on paper-based or interviewer-assisted questionnaires, depending on the literacy needs and accessibility constraints of each setting. All measures were administered at a single time point and collected anonymously to ensure confidentiality. The study design allowed systematic comparison across different measures and facilitated correlation analysis examining relationships between perceived changes, quality of life indicators and resilience.
Target population
The target population for this study consisted of adult men and women who had previously participated in structured MHPSS group sessions implemented in border communities. These groups were designed for individuals potentially experiencing elevated levels of stress due to conflict exposure, displacement or challenging socio-economic conditions. The overall accessible population consisted of approximately 3,000 former group participants across multiple regions.
A stratified sampling approach was applied to ensure balanced representation across geographic locations. First, the total population was divided into strata based on the regions and villages where group sessions had been conducted. The sample of 341 participants was then proportionally allocated across the strata, ensuring that participants in each region were represented in accordance with the region’s relative population size within the total population. Within each stratum, simple random sampling was applied to select groups and corresponding participants.
To address potential non-response or logistical barriers, such as incomplete surveys or the inability to reach selected individuals, backup groups and backup villages were pre-identified. These backups were used systematically to maintain the target sample size and minimize sampling bias. Eligibility criteria included prior participation in MHPSS group sessions and the ability to provide informed consent. There was no exclusion criteria based on gender, socio-economic status, ethnicity or psychological symptom severity.
Intervention: Content and delivery
The intervention evaluated in this study consisted of structured ICRC MHPSS group sessions delivered across multiple rural and border communities in Armenia. This community-based MHPSS intervention was implemented through a structured series of seven group sessions, consisting of one introductory information session followed by six thematic sessions. Groups included an average of ten participants and were conducted over a period of approximately seven or eight weeks, with sessions held on a weekly basis. Each session lasted approximately two hours and followed a standardized but adaptable manual developed in line with the ICRC’s Guidelines on Mental Health and Psychosocial Support.Footnote 24
The intervention was designed as a structured, manualized group programme combining psycho-education, psychosocial support and skills-building components. While a standardized curriculum ensured consistency across groups, facilitators were trained to adapt the delivery to participants’ needs, experiences and group dynamics, allowing for contextual responsiveness while maintaining core therapeutic elements. The intervention followed a progressive structure, moving from awareness-raising and normalization of psychological distress toward the development of coping strategies, interpersonal support and community-level resilience. Participation was voluntary, and sessions were offered free of charge as part of the broader community-based MHPSS programme.
Preparatory engagement, awareness-raising, and selection of participants
As an initial step, prior to the group sessions, preparatory engagement was conducted with regional and local authorities. Meetings were organized to present the potential ARCS–ICRC MHPSS intervention and to explore authorities’ perceptions of mental health and community needs. This process also aimed to ensure relevance of the intervention, foster local ownership and secure institutional support.
Mayors from the selected border villages were then requested to invite people from their communities to an introductory information session. They were encouraged to prioritize the inclusion of individuals with specific vulnerabilities, particularly those most affected by the conflict, individuals experiencing mental health difficulties, and people who had moved from Karabakh. In addition, key community members, such as teachers and health workers, were invited to participate given their close connection to the populations they serve and their important roles within their communities. Their involvement was considered essential for identifying and referring individuals in distress to ARCS counsellors, and for supporting sensitization and mental health awareness-raising initiatives.
The session introduced participants to key concepts of MHPSS, with a particular emphasis on destigmatizing mental health difficulties and promoting help-seeking behaviours. The role of the counsellors within the communities and the MHPSS intervention were explained. Individuals who expressed interest were then invited to enrol themselves in the group activities and take part in the initial session.
Throughout the presence of the counsellors in the villages, as well as during sensitization sessions and regular meetings with key community actors and organizations, community members strengthened their awareness of mental health issues, and misperceptions and barriers were reduced. Community members played an active role in identifying their own and others’ mental health support needs and referring individuals to ARCS counsellors for participation in the group sessions. At the same time, counsellors, drawing on their knowledge of the communities and their background in psychology, assessed whether individuals were suitable for participation in group sessions, required more specialized mental health care, or would benefit from the addition of individual counselling alongside group support.
The cycle of group sessions
The initial MHPSS session served to establish expectations, explain the purpose and structure of the programme, and initiate group cohesion. Participants were encouraged to reflect on their own perceptions of mental health and to recognize common reactions to stress in the context of conflict and displacement. The six subsequent sessions addressed specific thematic areas:
1. Stress and its manifestations. Participants were introduced to the concept of stress as a normal physiological and psychological response to challenging circumstances. The session included identification of stressors, recognition of emotional, cognitive and somatic symptoms, and discussion of when stress becomes problematic. Participants explored their own experiences and began to identify existing coping mechanisms.
2. Psychological consequences of armed conflict and loss. This session focused on trauma, grief and loss, including psycho-education on common reactions to traumatic events. Particular attention was given to normalizing emotional responses, understanding grief processes, and recognizing the impact of conflict on individuals, families and communities. Experiential exercises (e.g., expressive and reflective activities) supported emotional processing and identification of personal resources.
3. Coping strategies and resilience-building. Participants explored adaptive and maladaptive coping mechanisms and were supported in identifying and strengthening effective strategies. Practical techniques, such as problem-solving, cognitive reframing and relaxation exercises, were introduced. The session emphasized participants’ existing strengths and resources as a foundation for resilience.
4. Communication with children about conflict. This session addressed the specific challenges of discussing traumatic events with children. Participants learned age-appropriate communication strategies, ways to recognize children’s stress responses, and approaches to providing emotional support. The session aimed to strengthen caregiving capacities and intergenerational resilience.
5. Communication and mutual support. Focus was placed on interpersonal skills, including active listening, empathy, and non-judgemental communication. Participants engaged in role-play and group exercises to practice supportive interactions. The session also emphasized the importance of social connectedness as a protective factor for mental health.
6. Peer support and community-level resilience. The final session consolidated learning and encouraged participants to continue mutual support beyond the programme. The session took place in a leisure setting selected by participants, mostly in nature or at a religious site. It focused on strengthening peer networks, fostering collective coping and promoting community-based support mechanisms.
Each session followed a consistent structure, including (a) introduction and review of previous content, (b) psycho-educational input, (c) participatory exercises and group discussions, and (d) reflection and planning for application of learned skills in daily life. Between-session reflection and informal “home practice” were encouraged to facilitate integration of knowledge and skills.
Core intervention components (“active ingredients”)
The intervention was designed around several key mechanisms of change, based on ICRC and international standards for MHPSS implementation in humanitarian settings, as well as on evidence-based psychological interventions:Footnote 25
• Psycho-education and normalization: participants were provided with accessible information about stress, trauma and mental health, with the aim of reducing stigma, normalizing reactions and increasing self-awareness.
• Skills development: practical techniques such as breathing exercises, cognitive restructuring and problem-solving were introduced to enhance participants’ capacity to regulate emotional responses and manage stress.
• Emotional expression and processing: structured exercises created a safe space for participants to express and process difficult emotions related to conflict, loss and uncertainty.
• Social support and group cohesion: the group format facilitated peer connection, mutual understanding and the development of supportive relationships, which are critical protective factors in post-conflict settings.
• Strengths-based approach: the intervention emphasized identification and mobilization of individual and collective resources, reinforcing participants’ sense of agency and resilience.
• Community-oriented perspective: by encouraging peer support and dissemination of knowledge within communities, the intervention aimed to extend its impact beyond individual participants.
Role and qualifications of facilitators
Group sessions were facilitated by thirteen trained ARCS counsellors with a background in psychology, all of whom were recruited from the target communities. This community-based approach was intended to enhance trust, cultural relevance and accessibility. Facilitators underwent continuous capacity-building throughout the programme, including regular trainings on MHPSS principles, group facilitation skills, and the specific content of the intervention manual; in addition, they received ongoing supervision from senior mental health professionals at least twice per month. Supervision sessions provided technical guidance, ensured adherence to the intervention framework, and offered support in managing complex cases and group dynamics.
The involvement of trained psychologists was essential for several reasons. First, facilitators were required to deliver psycho-educational content accurately and to respond to participants’ questions regarding mental health and trauma. Second, they needed to manage potentially distressing disclosures and emotional reactions within the group setting, ensuring psychological safety. Third, facilitators were responsible for identifying participants who might require more specialized support and making appropriate referrals.
While the intervention was based on a standardized manual, facilitators were encouraged to adapt the delivery of sessions to the specific context and needs of each group. This included adjusting the pace of sessions, selecting or emphasizing particular exercises, and responding to emerging themes during discussions. Such flexibility was considered essential given the diversity of participants’ experiences and the evolving context of post-conflict recovery. At the same time, fidelity to the core components of the intervention was maintained through the use of structured session outlines, standardized materials and regular supervision. This balance between standardization and adaptability aimed to ensure both consistency and relevance.
A system for identifying and supporting participants with more severe mental health needs was integrated into the intervention. Prior to programme implementation, a mapping of available mental health and social services was conducted to establish referral pathways. During the sessions, facilitators monitored participants for signs of severe distress or vulnerability, and when necessary, they provided individual support or referred participants to specialized services. This ensured that the group intervention remained appropriate for its intended scope while enabling access to higher-level care when required.
The protocol of the current study was submitted to and approved by the ICRC Ethics Review Board (Ref: LDP_CORE25_016).
Results
The study population
The study included 341 participants, the vast majority of whom were women (98%). Most respondents were married (68%), and almost half were 30–44 years old (46%). The sample predominantly consisted of local residents (81%), with a smaller proportion of people having moved from Karabakh (19%). Regarding health status, while most reported no health issues (64%), a significant minority reported having at least one health problem (36%) (see Table 1).
Study population characteristics

Table 1 Long description
The table summarizes the study population by gender, marital status, age group, residency status, and self-reported health. Women account for 333 participants, or 98 percent, while men are 8 participants, or 2 percent. Most participants are married at 231 people, or 68 percent, compared with 110 people, or 32 percent, who are single or other. The largest age group is 30 to 44 years with 157 people, or 46 percent; other groups are 18 to 29 years at 59 people, or 17.3 percent, 45 to 59 years at 73 people, or 21.4 percent, and 60 years and older at 52 people, or 15.3 percent. Most are residents of border communities at 275 people, or 81 percent, while 66 people, or 19 percent, moved from Karabakh. Health status is mostly no reported issues at 219 people, or 64 percent, with 122 people, or 36 percent, reporting at least one health problem.
Perceived changes after participation in MHPSS group sessions
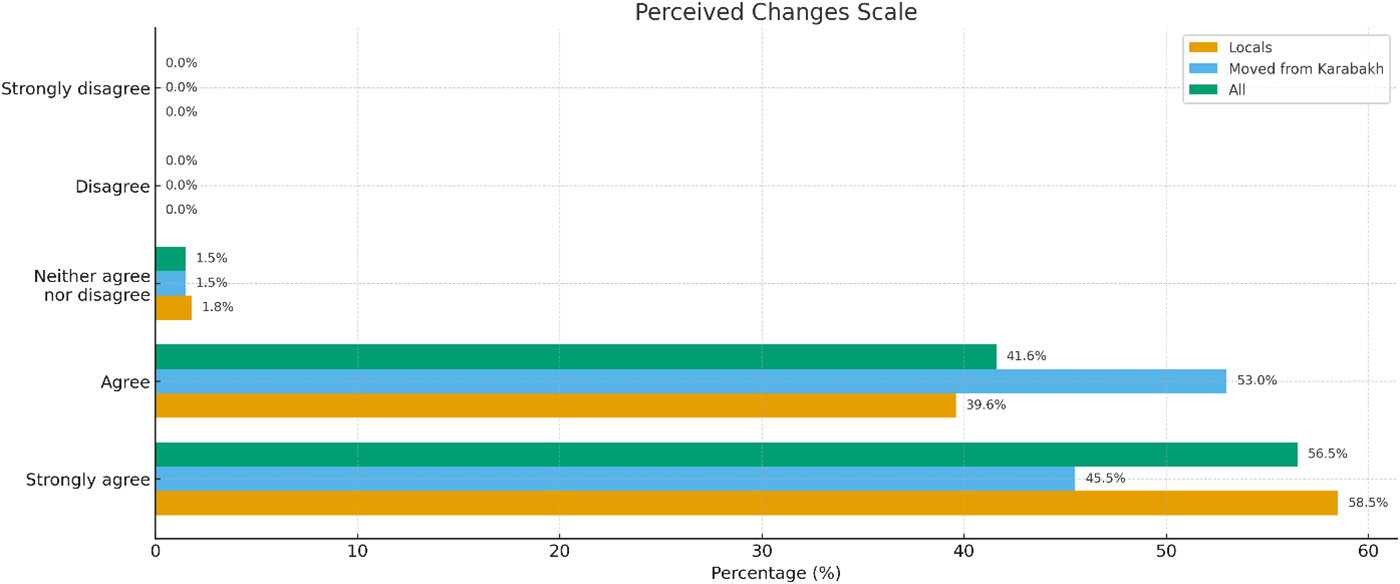
Responses on the perceived changes scale were categorized into five levels: strongly agree, agree, neither agree nor disagree, disagree, and strongly disagree. Among local participants, 58.5% strongly agreed and 39.6% agreed that they experienced positive changes following the intervention, while 1.8% selected neither agree nor disagree. None selected disagree or strongly disagree. Among participants moved from Karabakh, 45.5% strongly agreed and 53.0% agreed, with 1.5% selecting neither agree nor disagree and none selecting the two negative response options. In the total sample, 56.5% strongly agreed and 41.6% agreed, while 1.5% reported a neutral response and no participants selected disagree or strongly disagree. A direct comparison indicated that locals more frequently endorsed “strongly agree”, whereas participants moved from Karabakh more often selected “agree”. Neutral responses were minimal in both groups, and no participants reported negative perceptions of change (see Figure 1).
Perceived changes scale.

Figure 1 Long description
The title reads Perceived Changes Scale. A horizontal grouped bar graph is shown. The vertical axis lists response categories: Strongly disagree, Disagree, Neither agree nor disagree, Agree, Strongly agree. The horizontal axis label reads Percentage. The horizontal axis range is 0 to 60. A legend lists three series: Locals, Moved from Karabakh, Total. Strongly agree: Locals 58.5, Moved from Karabakh 45.5, Total 56.5. Agree: Locals 39.6, Moved from Karabakh 53.0, Total 41.6. Neither agree nor disagree: Locals 1.8, Moved from Karabakh 1.5, Total 1.5. Disagree: Locals 0.0, Moved from Karabakh 0.0, Total 0.0. Strongly disagree: Locals 0.0, Moved from Karabakh 0.0, Total 0.0.
Perceived quality of life
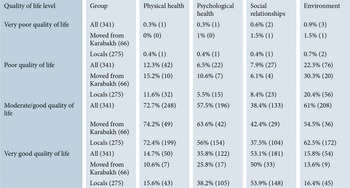
Across all four quality of life domains, displaced and local participants showed similar overall patterns, but with several notable contrasts. Participants moved from Karabakh reported higher rates of poor quality of life in physical health (15.2% versus 11.6%), psychological health (10.6% versus 5.5%) and environment (30.3% versus 20.4%). In contrast, local participants more frequently fell into the very good quality of life category across psychological health (38.2% versus 25.8%), social relationships (53.9% versus 50%) and environment (16.4% versus 13.6%). For moderate/good quality of life, differences between the groups were small across domains. Overall, participants moved from Karabakh showed higher representation in the lower quality of life categories, whereas local participants tended to appear more often in the higher categories (see Table 2).
Quality of life levels by participant group

Table 2 Long description
The table reports the share and count of participants rating four quality-of-life domains (physical, psychological, social relationships, environment) as very poor, poor, moderate or good, or very good, for all participants and by group (moved from Karabakh versus locals). In the full sample, moderate or good ratings are most common for physical health (72.7%, 248) and environment (61%, 208), while social relationships most often falls in the very good category (53.1%, 181). Very poor ratings are rare across domains, staying under 1% for the full sample (for example, environment 0.9%, 3). Poor ratings are highest for environment, especially among those moved from Karabakh (30.3%, 20) compared with locals (20.4%, 56). Psychological health shows more very good ratings among locals (38.2%, 105) than among those moved from Karabakh (25.8%, 17), while moderate or good psychological ratings are higher among those moved from Karabakh (63.6%, 42) than locals (56%, 154). For social relationships, both groups report high very good ratings (50%, 33 moved from Karabakh; 53.9%, 148 locals). Percentages are within each group and domain, and small counts in the very poor category mean minor differences should be interpreted cautiously.
Resilience
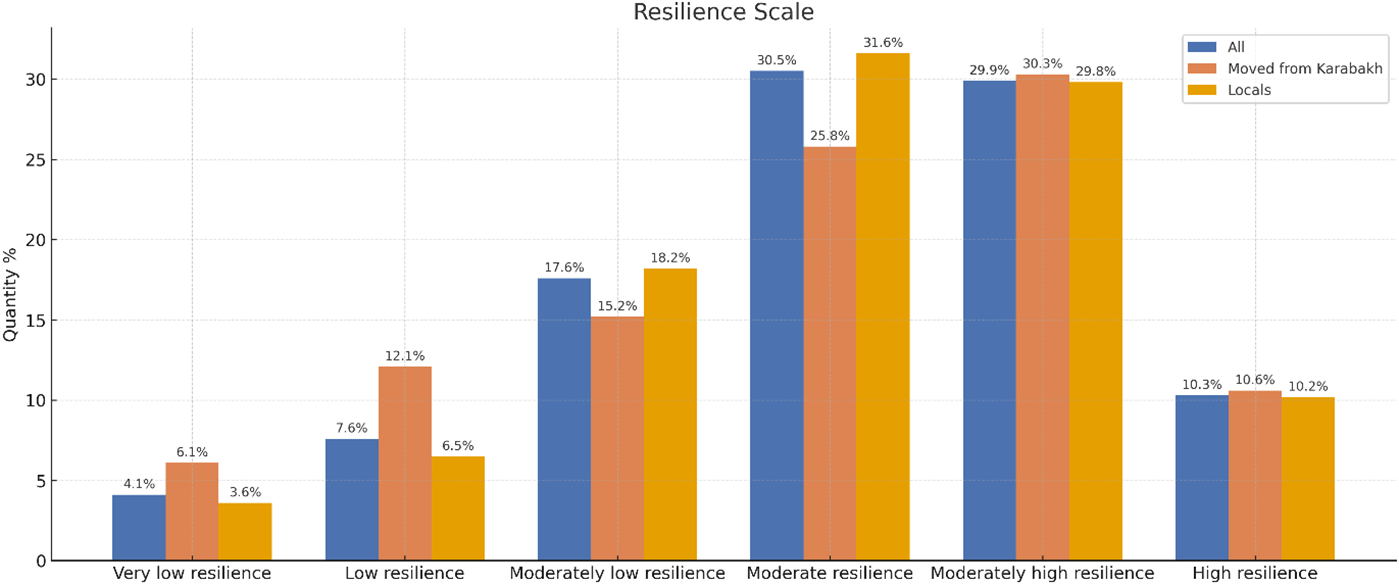
Resilience was assessed using the RS™ Footnote 26 and categorized into six levels: very low, low, moderately low, moderate, moderately high, and high resilience. Among all participants, 4.1% were classified as having very low resilience, 7.6% as low resilience, 17.6% as moderately low, 30.5% as moderate, 29.9% as moderately high, and 10.3% as high resilience. Among participants moved from Karabakh, 6.1% were categorized as very low resilience, 12.1% as low, 15.2% as moderately low, 25.8% as moderate, 30.3% as moderately high, and 10.6% as high resilience. Among local participants, 3.6% were classified as very low resilience, 6.5% as low, 18.2% as moderately low, 31.6% as moderate, 29.8% as moderately high, and 10.2% as high resilience.
The overall mean score was 138.4 (SD=18.71), indicating a generally moderate level of resilience within the sample; comparing the two subgroups, locals scored 139 (SD=18) while displaced individuals scored 136.1 (SD=22). Participants moved from Karabakh showed higher percentages than locals in the very low and low resilience categories, whereas locals showed higher percentages in the moderately low and moderate resilience categories. The proportions of local participants and participants moved from Karabakh in the moderately high and high resilience categories were similar, with only minimal differences across groups (see Figure 2).
Resilience levels by participant group.

Figure 2 Long description
The bar graph displays resilience levels by participant group, with categories ranging from very low to high resilience on the x-axis. The y-axis represents quantity, ranging from 0 to 35. The graph includes two groups: 'Moved from Karabakh' and 'Locals', differentiated by color. In the very low resilience category, 'Moved from Karabakh' is at 6.7 percent and 'Locals' at 3.6 percent. In the low resilience category, 'Moved from Karabakh' is at 11.1 percent and 'Locals' at 6.9 percent. For moderately low resilience, 'Moved from Karabakh' is at 22.2 percent and 'Locals' at 19.4 percent. In moderate resilience, 'Moved from Karabakh' is at 31.1 percent and 'Locals' at 33.3 percent. In moderately high resilience, 'Moved from Karabakh' is at 20 percent and 'Locals' at 26.4 percent. In high resilience, 'Moved from Karabakh' is at 8.9 percent and 'Locals' at 12.5 percent. The bars are vertical and grouped by category, illustrating differences in resilience levels between the two groups.
Correlations
Pearson coefficients were calculated to examine the associations among perceived changes (self-reported improvements related to participation in MHPSS group sessions), physical health (WHOQOL-BREF), psychological health (WHOQOL-BREF), social relationships (WHOQOL-BREF), environment (WHOQOL-BREF) and resilience (RS™).
Analyses indicated that perceived changes were significantly correlated with every other variable measured. Perceived changes demonstrated a positive correlation with resilience (r=0.24, t=4.61, p<0.001), indicating a statistically significant linear association between the two variables. Perceived changes were also significantly correlated with physical health (r=0.27, t=5.11, p<0.001) and psychological health (r=0.35, t=6.94, p<0.001). A statistically significant though smaller correlation was observed between perceived changes and social relationships (r=0.11, t=2.07, p<0.05). Additional significant correlations were identified between perceived changes and environment (r=0.29, t=5.63, p<0.001). All correlations involving perceived changes were positive and met the criteria for statistical significance.
Physical health was significantly correlated with multiple domains, showing a strong association with psychological health (r=0.61, t=14.31, p<0.001) and additional significant correlations with social relationships (r=0.28, t=5.44, p<0.001), environment (r=0.54, t=11.95, p<0.001) and resilience (r=0.34, t=6.59, p<0.001). All correlations were positive and statistically significant. Psychological health was also significantly correlated with social relationships (r=0.39, t=7.70, p<0.001), environment (r=0.58, t=12.94, p<0.001), and resilience (r=0.34, t=6.56, p<0.001), with all p-values below 0.001. Social relationships showed significant correlations with environment (r=0.33, t=6.40, p<0.001) and resilience (r=0.13, t=2.45, p<0.05), while environment was further significantly correlated with resilience (r=0.30, t=5.77, p<0.001).
Overall, all pairwise Pearson correlation coefficients among the six variables were positive. All t-values associated with these correlations exceeded the critical value required for statistical significance, resulting in p-values below 0.05 across the dataset. No non-significant results were identified, and no negative coefficients were observed. All reported statistics reflect the complete set of correlations calculated for the study (see Figure 3).
Pearson correlation matrix of perceived changes, quality of life domains and resilience.

Figure 3 Long description
The heat map displays a Pearson correlation matrix with labeled rows and columns: Perceived Changes, Physical Health, Psychological Health, Social Relationships, Environment and Resilience. The numerical values inside the cells represent correlation coefficients ranging from 0.00 to 1.00. The legend on the right indicates the gradient from 0.0 to 1.0, where lighter shades represent higher correlations. Key insights include strong correlations between Psychological Health and Physical Health (0.61) and between Environment and Resilience (0.30). The weakest correlation is between Social Relationships and Perceived Changes (0.11). All correlations are positive, with no negative values observed.
Discussion
The study results will now be discussed and explored according to the four research questions set out in the above section on “Primary Research Objective and Research Questions”.
To what extent has participation in MHPSS group sessions helped participants strengthen their resilience?
There is no universal standard or normative benchmark for the RS™, and reported scores vary widely across populations and study contexts. Nevertheless, previous studies provide several useful reference points that may help to situate the current findings, reflected in a mean score of 138.4 (SD=18.71). For instance, spouses of members of the armed forces showed RS™ scores around 142 and adults living in rural/frontier communities demonstrated scores around 136.8 (SD=21.2), while a recent study of Ukrainian migrants in the United States reported a substantially lower mean score of 105.9 (SD=18.46).Footnote 27
When comparing subgroups in the present study, locals scored 139 (SD=18) while people from Karabakh scored 136.1 (SD=22). Although the distribution across the higher resilience categories was relatively similar for both groups, the most important differences appeared at the lower end of the scale. Among Karabakh participants, 6.1% fell into the very low resilience group and 12.1% into the low group; in contrast, among locals these proportions were 3.6% and 6.5%, respectively. Thus, in the two lowest resilience categories, the share of individuals from Karabakh was nearly double that of non-displaced residents. This pattern suggests that although many individuals who moved from Karabakh demonstrated resilience levels comparable to the general population, a small yet distinct subgroup remained in the lower resilience range, indicating heightened vulnerability.
According to the American Psychological Association, resilience is both the process and the outcome of successfully adapting to challenging life experiences.Footnote 28 Displaced people face several additional risk factors that may negatively affect their mental health and overall adaptation: as outlined in a 2023 WHO report on the mental health of migrants and refugees, these risks include demographic factors (country of origin, education, religion), socio-cultural factors (language, cultural practices), economic factors (poverty, living conditions, employment), health-related factors, neighbourhood-level factors (social support, social isolation, social exclusion, racism and discrimination), environmental factors, country-level factors, and migration-related factors and migration trajectory.Footnote 29 In Armenia, many of these WHO-identified risk factors are mitigated because people who have moved from Karabakh share the same culture, religion and language as the host population and generally receive social acceptance and support.Footnote 30 These similarities likely help sustain resilience and explain why overall mean scores between the two groups do not differ substantially. Despite these protective factors, however, displaced individuals still face economic insecurity, unstable housing, disrupted social networks, and psychological distress linked to displacement and uncertainty about their long-term situation.Footnote 31
The study also found a positive correlation between perceived changes and resilience (r=0.24). The MHPSS programme includes several elements widely recognized in the literature as promoting resilience, such as providing a safe space,Footnote 32 addressing psychological and psychosocial needs, strengthening coping mechanisms,Footnote 33 enhancing social support,Footnote 34 fostering meaning-making and promoting hope.Footnote 35 Moreover, during the final psychosocial event, participants often chose to visit religious sites, which can also serve as a meaningful resilience-supporting practice.Footnote 36 Taken together, these components and the fact that almost all respondents (97.36%) reported perceived improvements (scoring in the “agree” or “strongly agree” categories) suggest that the programme likely contributed to strengthening resilience.
Are there positive correlations between perceived changes, perceived quality of life and participants’ levels of resilience?
As noted earlier, resilience is influenced by a wide range of factors, including health status, available social support and broader environmental conditions. Analyzing the correlations between resilience, perceived changes and the various components of perceived quality of life may help to clarify how these elements are interconnected within the context of this community-based MHPSS intervention.
Resilience showed one of its strongest correlations with the quality of life psychological domain (r=0.34); this aligns with evidence identifying resilience as a protective factor against mental health disorders such as depression and anxiety, while at the same time, psychological functioning enhances resilience.Footnote 37 In the specific context of this study, individuals living in border communities are exposed to recurrent violence, uncertainty about the future and a diminished sense of control, and resilience may play a crucial role in helping them to adapt to these challenging circumstances. Moreover, participants’ strong sense of belonging to their communities and their perceived responsibility to protect those communities reflect a sense of purpose and perseverance,Footnote 38 both of which are key elements of the resilience core.Footnote 39 At the same time, the perceived changes scale showed the strongest association with psychological health, which is consistent with the intervention’s focus on mental health and well-being.
Physical health showed the same correlation with resilience as psychological health (r=0.34). Notably, 36% of the 341 participants reported being currently ill in the quality of life questionnaire. The strongest association observed in the analysis is the correlation between physical and psychological health (r=0.61), a finding supported by scientific literature which widely documents the links between physical health and mental health, particularly stress.Footnote 40 Individuals living in the context addressed by this study are at higher risk from chronic stress, trauma and acute stress reactions, which by itself may predispose them to long-term physical health problems.Footnote 41 The existing correlation between physical health and perceived changes (r=0.27) may indicate the contribution of the group sessions in helping participants to understand the links between their physical and psychological distress. Throughout the sessions, psycho-education was provided on the links between cognitive, emotional, behavioural and physical components, emphasizing how stress can manifest through physical discomfort and health problems. In addition, techniques such as relaxation and breathing exercises were incorporated to reduce physical symptoms of stress and anxiety.
The environment domain of quality of life also correlated positively with resilience (r=0.30) and showed moderate to high associations with both physical health (r=0.54) and psychological health (r=0.58). According to WHO’s 2014 Social Determinants of Mental Health study, greater exposure and vulnerability to adverse social, economic and environmental conditions significantly increases the risk of developing mental health disorders and physical health problems.Footnote 42 The findings of the WHO study highlight the relevance of environmental factors in shaping both well-being and resilience. Likewise, a positive correlation exists between perceived changes and environment (r=0.29). Participants in the MHPSS intervention live in a particularly challenging environment marked by insecurity, isolation and limited access to essential services; the loss of territory during the conflict and the resulting disruption of livelihoods, especially those related to livestock and agriculture, which constitute many participants’ primary means of subsistence, further aggravates these difficulties. Linking the programme to the positive association with the environment, the continuous presence of ARCS counsellors in the communities facilitated participants’ access to MHPSS services. Additionally, the intervention extended beyond MHPSS provision by facilitating linkages to other forms of support provided either by ARCS, the ICRC or other governmental or non-governmental organizations – this included services related to health, livelihoods and education. This integrated approach, together with the sustained presence of ARCS counsellors, may have helped reduce participants’ sense of isolation while strengthening their connection to available resources and improving their perceived environmental conditions.
Surprisingly, the social relationships dimension of the quality of life scale exhibited only a very low, though significant, positive correlation with resilience (r=0.13) and perceived changes (r=0.11). This finding contrasts with existing evidence highlighting social connections as a critical factor in fostering resilience; it also diverges from the central role that social and peer support play in promoting well-being within the MHPSS group sessions that are part of the intervention under study. Notably, data from the perceived changes questionnaire indicate that 95% of participants reported “strongly agree” or “agree” when asked whether the intervention had helped them to improve their social relationships. One possible explanation for this discrepancy is that the quality of life questionnaire includes only three items related to social relationships, one of which addresses satisfaction with sex life – a complex construct influenced by multiple dimensions.Footnote 43 Almost one third of participants answered “neither satisfied nor dissatisfied” for this item, possibly as a way of avoiding a direct response. In Armenia, particularly in rural areas, social norms tend to be conservative, and questions about sex life may be sensitive or uncomfortable, even when mitigating measures are in place. Consistent with the present finding, studies examining the psychometric properties of the quality of life questionnaire used in the present research have reported that the social relationships domain demonstrates comparatively weaker psychometric performance, exhibiting lower internal consistency than the other domains.Footnote 44 Indeed, given that this domain comprises only three items, its brevity may limit its comprehensiveness and reduce its ability to fully capture the complexity of social relationships.Footnote 45 The sexual satisfaction item has also been identified as particularly difficult to answer, further affecting the sensitivity of the domain.Footnote 46
Is this community-based MHPSS intervention effective, and could it be replicated in other humanitarian contexts?
Although the core component of the programme consists of a cycle of group sessions, the full intervention follows a multilayered approach across the continuum of care, from basic psychosocial support to specialized mental health care delivered through referrals. To evaluate its effectiveness and explore which specific elements contribute most to its impact, the intervention was examined as a whole.
First, the intervention addresses barriers related to accessibility and stigma.Footnote 47 ARCS counsellors are present within remote communities, conduct group sessions in spaces convenient for all participants, and provide support for referrals to MHPSS and other services. In Armenia, based on the authors’ experience and existing studies, stigma stemming from limited knowledge and misinformation about mental health represents a significant barrier, particularly in rural and remote areas.Footnote 48 To address this, counsellors carry out awareness-raising activities with community members to prepare the ground before involving people in the group sessions, aiming to normalize mental health and reduce stigma. Psycho-education delivered during the group sessions further enhances participants’ understanding of mental health. Additionally, the fact that the counsellors themselves are from the communities of intervention and share the same cultural and social norms contributes to building trust and improving access to these services.
Armenia is still in the process of transitioning from a mental health model inherited from the Soviet period, heavily centralized and dominated by hospital-based psychiatry, towards a more diversified and accessible mental health system. Despite important reform efforts, the mental health sector continues to face significant limitations, including underfunding, marked rural–urban disparities and workforce shortages, with relatively few trained psychologists and limited availability of resources outside major urban centres.Footnote 49 In rural contexts with limited mental health resources, such as the remote villages targeted by the intervention, working with motivated local community members who have a basic background in psychology or social work – and who receive regular training and supervision from ICRC and ARCS mental health specialists – may be an effective, literature-supported strategy, provided that certain requirements are met.Footnote 50 This is known as a task-sharing approach, in which specific tasks traditionally performed by highly specialized professionals, such as psychiatrists or psychologists, are redistributed to trained non-specialist providers, including community workers, lay counsellors, nurses and peers. When appropriately implemented, task-sharing requires continuous support, ongoing capacity-building, clear role definition and safeguards to prevent overburdening of workers. This approach helps expand access to mental health care and is widely identified as a facilitating factor in the implementation of global mental health interventions in humanitarian settings.Footnote 51
Furthermore, using culturally adapted interventions that incorporate important cultural, religious and spiritual elements is known to strengthen coping strategies, social connectedness and psychological well-being, and is widely identified as a key factor in building resilience.Footnote 52 Highlighting the importance of religion in Armenian culture, the final group session, in which a social event was organized, often involved visiting a religious site. Going further, and in line with global mental health strategies,Footnote 53 the growing movement to decolonize mental health offers a critical lens on the use of imported Western models in humanitarian and development settings, underscoring the need to design interventions grounded in local understandings, cultural practices and community knowledge of mental health.Footnote 54
In the ARCS–ICRC intervention, although the content is culturally adapted and tailored to the specific dynamics of each village, the group sessions still follow clear guidelines that support counsellors in delivery and facilitate the scaling up of the intervention. The sessions integrate evidence-based components that are widely used in psychological interventions for common mental health disorders and in the promotion of well-being. This aligns with the transdiagnostic or common elements treatment approach, which aims to help with the dissemination, scaling up and, ultimately, sustainability of MHPSS interventions.Footnote 55 These evidence-based components include both specific and common factors. The specific factors addressed within the group sessions comprise psycho-education, management of stress symptoms, behavioural activation, cognitive restructuring, problem-solving, communication skills and social support. The common factors include empathy, alliance, establishment of a safe environment and cultural adaptation, and are critical to the effectiveness of psychological interventions.Footnote 56
A systematic review of twelve studies on MHPSS programmes in humanitarian contexts and in low- and middle-income countries recommends integrating interventions into existing community and health delivery systems in order to promote vertical expansion – not just horizontal or geographical scaling – as a strategy to enhance sustainability.Footnote 57 Long-term investment and commitment to building strong relationships with key community actors is another important element of sustainability;Footnote 58 in line with this, the MHPSS intervention is implemented jointly with ARCS, a key local organization that responds to emergencies and crises, operates across all regions and works in a variety of sectors, thereby contributing to the scaling up and sustainability of the programme.
Furthermore, research highlights the need for in-depth, multilayered assessments of causal and contributing factors, along with a thorough understanding of the local socio-cultural and economic context, in order to plan effective and comprehensive MHPSS actions. Such an approach supports the design of integrated, multisectoral interventions that employ a diverse range of strategies across ecological levels.Footnote 59 For instance, in some selected communities, our MHPSS intervention with children was complemented by group sessions with adults which focused on parenting skills and family communication, contributing to a more multilayered and comprehensive approach to promoting children’s well-being. Indeed, robust evidence indicates that stand-alone interventions with children often have limited impact because of chronic stress on parenting, which in turn influences children’s mental health.Footnote 60
What are the programme’s weaknesses, and how could it be improved to enhance effectiveness and impact?
The intervention under study clearly demonstrates efforts to move towards a comprehensive, multilayered approach. All levels of the MHPSS continuum of care are addressed through implementation of specific activities or referrals. Additionally, initial MHPSS assessments were carried out within a multidisciplinary process that incorporated food security, health, and water and habitat in order to enable integrated planning and thereby maximize the impact. However, important gaps remain in this area, and it is thus necessary to discuss the programme’s weaknesses and potential areas for improvement.
With regard to the environment domain of quality of life, results showed the highest percentage of respondents rating this domain as poor or very poor, followed by the health domain. Indeed, structural problems remain, such as insufficient government support, limited access to basic services and gaps in the health-care system.Footnote 61 In addition, insecurity, closeness to military positions and exposure to recurrent waves of violence are part of respondents’ reality. Furthermore, the continuum of care is far from perfect, as finding quality, accessible and affordable more specialized mental health services is often a real challenge. Intervening at all levels of the different ecosystems is undoubtably necessary, but it remains difficult, requiring an in-depth and rigorous understanding of context-specific needs as well as dedicated space for continuous reflection and adaptation of humanitarian action.Footnote 62 Nevertheless, resilience plays a crucial role in conserving individuals’ proper psychological functioning even when their quality of life is compromised. A study examining the associations between quality of life, depressive symptoms and hopelessness among Palestinians living under extremely difficult conditions found that resilience functions as a protective factor against ongoing potentially traumatic experiences. At the same time, improving quality of life helped to mobilize natural resources and skills linked to resilience that can protect people’s mental well-being.Footnote 63
When engaging new communities, regular awareness-raising sessions were implemented to reduce stigma, normalize MHPSS reactions to crisis and introduce the ARCS–ICRC MHPSS intervention, whose core component was the cycle of group sessions. Despite these efforts, some vulnerable individuals were unable to participate in the group sessions, including older adults and people with disabilities and limited mobility, as well as persons experiencing more severe mental health difficulties. By maintaining a continuous presence in the communities and fostering trusting relationships, counsellors were able to reach out to these individuals and offer them the opportunity to benefit from counselling sessions. At the same time, within the group sessions, participants, as part of the peer support component, learned to identify signs of distress in others, provide support and refer affected persons to ARCS counsellors for individual counselling or onward referrals to more specialized care.
Men’s participation in the MHPSS group sessions was limited, as reflected in the gender distribution of research participants (2% men). Several factors may help to explain this disparity. The MHPSS programme was initially implemented as an emergency response targeting vulnerable populations in general, without the development of tailored strategies specifically aimed at engaging men. At the time of programme initiation, stigma and misperceptions surrounding mental health issues were strong among community members and particularly among men, for whom expressions of distress were often perceived as a sign of weakness and inconsistent with prevailing norms of masculinity. Literature regarding MHPSS interventions in humanitarian settings highlights this common pattern, influenced by gender norms and perceptions that mental health is primarily a concern for women,Footnote 64 even though men are also affected by stressors linked to displacement and conflict. Moreover, considering that men’s mental health and behavioural problems – in particular substance abuse and interpersonal violence – have a strong adverse impact on women’s mental health, it is relevant to also target men in MHPSS programming.Footnote 65
Over time, a gradual process of awareness-raising and normalization about psychological distress and help-seeking behaviour, alongside the progressive development of trust between counsellors and community members, has taken place. Based on counsellors’ experience and feedback from participants in group sessions, this process appears to have played a significant role in strengthening community engagement with MHPSS. Furthermore, women participants may have played a key role in sensitizing male family members, contributing to a slow but ongoing shift in attitudes toward MHPSS. Although men-only group sessions are not examined in the present study due to their later implementation, it is plausible that this dynamic of trust-building and sensitization has fostered increased openness to engaging with the intervention among men.Footnote 66
On the other hand, as evidenced in the literature, to effectively engage men, interventions need to be gender-sensitive and culturally adapted.Footnote 67 This involves incorporating, at the beginning, an in-depth understanding of men’s specific MHPSS needs and the most appropriate modalities for addressing them. Actions may include offering separate group sessions for men and ensuring that activities and topics are relevant to them and presented in ways that are acceptable for them.Footnote 68 In the MHPSS intervention under review, men and women participated together in the same group sessions, and this may have contributed to lower male participation. The more recently implemented approach of conducting men-only sessions, tailored to address men’s specific needs, is showing encouraging levels of engagement and appears to be reducing the participation gap observed in the present study. These efforts reflect an adaptive learning process whereby the programme has evolved based on field experience while also adjusting to operational constraints inherent in the humanitarian context.
Strengths and limitations of the study
This study was made possible by the extensive participation of individuals residing in border communities who attended the MHPSS group sessions, allowing for a large sample to be included in the research. Furthermore, the broad network of trained and experienced ARCS counsellors facilitated the effective data collection process.
The main limitation of the study is the absence of baseline data prior to the intervention, which limited the study’s ability to accurately compare pre- and post-intervention outcomes and raised questions about the participants’ resilience levels before attending the group sessions. Additionally, due to ethical considerations, the study did not include a control group.
To address these limitations and strengthen the reliability of the findings, several mitigation measures were implemented. First, a robust and representative sample was drawn to ensure both representativeness and statistical reliability. Second, three scales, including two standardized and validated instruments, were employed to identify statistical tendencies and strengthen the robustness of the analysis. Third, an MHPSS survey on perceived changes was locally developed to capture and measure participants’ self-reported progress after their participation in the MHPSS group sessions.
Since the counsellors conducting the data collection interviews were the same individuals who implemented the MHPSS group sessions, there was a potential risk of bias due to participants’ tendency to provide responses they believed would please the interviewers. To mitigate this risk, counsellors were assigned to interview participants from groups that they did not facilitate.
An additional limitation is that due to the gender imbalance and low representation of men in the study population, the results may be applicable only to women and cannot be generalized to men.
Conclusions
Resilience is a complex and dynamic process of adapting to challenges and life difficulties, shaped by the interaction of multiple factors, including individual biological and psychological aspects, available social support, and broader social environmental conditions.Footnote 69 Despite the multiple elements influencing the study findings and the above-mentioned limitations, the results across the three instruments (the perceived changes survey, RS™ and WHOQOL-BREF), as well as the positive correlations identified, suggest that the ARCS–ICRC community-based MHPSS intervention most likely contributes to strengthening resilience.
Key components of the MHPSS programme, supported by existing literature, may contribute to resilience-building and to its overall effectiveness. Jointly implemented by International Red Cross and Red Crescent Movement partners through a network of local ARCS counsellors empowered to support their communities, the programme represents a cost-effective, sustainable and culturally adapted approach. It also has potential to be tailored and applied in other settings facing conflict and persistent violence.
Nevertheless, further research is recommended to more clearly demonstrate the effectiveness of this approach, including baseline data and analysis exploring the causal relationships between the intervention, resilience and quality of life. Additionally, future studies within the same context should consider including a more in-depth analysis of men and of people who moved from Karabakh.
Recommendations related to the programme include further advancing the implementation of rigorously designed MHPSS interventions within a comprehensive, integrated approach in order to respond, as fully as possible, to the multiple evolving needs emerging from humanitarian crisis. Achieving this requires investment in research activities that generate rigorous evidence and practical learnings. This will enable humanitarian workers to strengthen and adapt the support provided to people affected by conflict and violence, in line with the specific needs of each context.



 Open access
Open access