


Key points
-
• Older adults living in retirement homes are at increased risk for antibiotic-related harms, yet antimicrobial stewardship (AMS) efforts are limited in this setting.
-
• While this study of a pharmacist-led prospective audit and feedback intervention in retirement homes did not significantly reduce antibiotic use, it identified important barriers, facilitators and potential strategies to support AMS in retirement homes.
-
• The pilot helped to advance an AMS program in participating retirement homes by building on organizational support, pharmacist motivation and local capability to conduct AMU surveillance.
Introduction
Antimicrobial stewardship (AMS) programs are associated with reduced antibiotic use and lower risk of antimicrobial resistance and Clostridioides difficile infection. Reference Baur, Gladstone and Burkert1 While most formalized AMS efforts historically focused on hospitalized populations, the vast majority of antibiotics are prescribed to outpatients.
Older adults are a particularly important population given both their elevated risk of infection but also the risk of harm associated with antibiotic overuse includingadverse events, antimicrobial resistance and C. difficile infection. Reference Daneman, Bronskill and Gruneir2 AMS programs aiming to mitigate this harm in LTC homes are relatively nascent, but should include at least one strategy to improve antimicrobial use (AMU), along with tracking and reporting on AMU and other outcomes to providers. 3 Where they exist, programs tend to use multi-modal approaches including education, collaborative training, guidelines and protocols to improve antibiotic prescribing. Reference Pasay, Guirguis and Shkrobot4 Systematic reviews have shown AMS programs in LTC settings are effective and can reduce antibiotic use by approximately 14%. Reference Wu, Langford, Daneman, Friedrich and Garber5
However, the role and optimal model of AMS in retirement home settings is less clear. Older adults residing in retirement homes are typically more independent, receive fewer medical visits and require less nursing care than residents of LTC homes, but may still be at elevated risk of harm from antibiotic overuse. Reference Poss, Sinn, Grinchenko, Blums, Peirce and Hirdes6 Additionally, regulatory and accreditation standards may not provide the same level of oversight of these retirement homes compared with LTC homes, 7 which could lead to variations in prescribing and missed opportunities for AMS.
Prospective audit and feedback (PAF) is an evidence-based AMS strategy that involves review of individual antimicrobial prescriptions by a trained expert (pharmacist or physician) and provision of advice directly to prescribers to improve antibiotic prescribing. However, PAF is not established outside of the hospital setting. Reference Langenstroer, Jolles and Hossin8 High and variable antibiotic use in retirement home settings for older adults may provide an opportunity for PAF.
Our objective was to describe the development and evaluate the early implementation of a pharmacist-driven PAF intervention as part of an emerging AMS program to improve antibiotic use in seniors residing in retirement homes.
Methods
Study design
This was an observational quasi-experimental study with a control group that aimed to evaluate the implementation of an antibiotic PAF pilot project in retirement homes.
Setting
The study took place in Ontario, Canada’s most populous province, from June 2022 to December 2024. There are 781 licensed retirement homes in Ontario, housing over 60,000 residents. 9
Participating retirement homes
Retirement homes in Ontario served by CareRx (n = 405 of approximately 770 licensed homes in Ontario), 10 a contracted pharmacy service provider for seniors in communal care settings, were eligible for inclusion. Homes were invited to participate based on their interest in piloting an AMS program and if they had physicians with dedicated in-person rounds. Care teams and prescribers of these homes were provided with a one hour educational webinar on AMS principles for retirement home residents. Non-participating homes were considered controls. While the number of retirement homes serviced by CareRx varied over time, analyses at each evaluation point included only those homes that were actively serviced at that time.
Intervention
We reported intervention details in alignment with the Template for Intervention Description and Replication (TIDieR) checklist. Reference Hoffmann, Glasziou and Boutron11 Prior to implementation of the intervention, an education session was offered to retirement home staff and prescribers by an Infectious Diseases physician (ND) and pharmacist specialist (BL) focusing on AMS principles and resources, particularly on shorter durations of therapy for older individuals. 12,13 The PAF intervention was then carried out remotely, initially by one pharmacist (DD) with training in geriatrics and LTC and then by 2 additional CareRx staff pharmacists starting in July 2024 on a weekly rotating basis. On weekdays, the pharmacist received an email notification for each new antibiotic order dispensed the previous day for a resident in participating homes. During our initial data analysis, we identified that process for notifying pharmacists of new antibiotic prescriptions was incomplete, resulting in some prescriptions being missed; this was corrected after completing the pilot study. The profile of the patient receiving antibiotics was reviewed using Consultant Tools, a proprietary software platform integrated with the pharmacy software system (Kroll) for reviewing clinical information and documenting interventions. While reviewing each antimicrobial prescription, potential opportunities to improve the appropriateness of antimicrobial use were identified (eg, duration of therapy, dose, antibiotic selection). Antibiotic appropriateness was assessed based on local best practice recommendations and drug reference tools. 14,15 If necessary, the nursing care team was contacted by phone to obtain additional information (eg, indication), provide education, and discuss an intervention. All recommendations to optimize therapy were documented in Consultant Tools and faxed to the retirement home and the prescriber according to usual procedures. Prescribers were asked to review interventions and provide new orders following standardized facility procedures. There was an assessment 5 days later by the pharmacist to determine if the recommendation was accepted, not accepted or not received. As the PAF intervention was launched in June 2023, the preintervention period was June 2022 to May 2023 and the postintervention period was June 2023 to December 2024.
Data sources
All antimicrobial use and intervention data were captured from a pharmacy-maintained database integrated with Kroll and Consultant Tools. Demographic data about residents (eg, number of residents, resident days, age and sex) were collected from this internal database.
Outcome measures
Antibiotic use
The primary outcome was antibiotic days of therapy (DOT) per 1,000 resident days per month. Systemic antibiotics in The World Health Organization Anatomic Therapeutic Chemical classification J01 antibacterial were included in this definition. 16 Days of antibiotic therapy (DOT) were estimated based on the days supplied from pharmacy dispensing data. Resident-days were calculated using the number of occupied beds in each facility at the time of each monthly data extract, multiplied by the number of days in the corresponding month.
Process measures
Indication documentation
We evaluated the proportion of all antibiotic orders with indications included on the prescription, in both the intervention and control homes, before and after the intervention.
PAF recommendations
We evaluated the number of PAF interventions each month and the proportion of recommendations that were accepted. Recommendations were classified by suggestion type including discontinue therapy, change dose or agent, reduce duration. The drugs and reasons for use were captured for each recommendation.
Analysis
We presented data descriptively for resident demographics, PAF interventions, and antibiotic and indication outcomes. We conducted a difference-in-differences (DiD) analysis to estimate the effect of the intervention on AMU. The DiD analysis compared the difference between the pre and post intervention periods in the intervention compared to the control homes. We evaluated outcomes over a 31-month period, 12 months before (June 2022 to May 2023) and 19 months after (June 2023 to December 2024) the intervention. To model antibiotic DOT, we used negative binomial regression with an offset for patient volume (logarithm of resident days). To account for clustering of residents within homes we included a random intercept for the home. The model included terms for the intervention group, postintervention period, their interaction, the random intercept for the home. To estimate the average risk difference (RD) between the intervention and control groups in the postintervention period, a fitted model was used to simulate predictions under both scenarios. A model matrix was applied to generate 5,000 simulations of predicted values using a multivariate normal distribution defined from the estimated coefficients and variance-covariance matrix of the model. The RD was calculated as the mean difference between simulated rates in the intervention and control scenarios with 95% confidence intervals. Proportions of prescriptions with an indication documented were also evaluated using an analogous approach except using a binomial regression model with a logit link to account for the outcome. Differences in indication documentation were expressed as absolute percentage change. Analyses were carried out in R (version 4.5.0) (R Foundation for Statistical Computing, Vienna, Austria),
Barriers and facilitators analysis
After the intervention, barriers and facilitators to the implementation of pharmacist-driven PAF were identified via informal email consultations with the pharmacists delivering the feedback. Questions posed to pharmacists are included in the supplement. Determinants were categorized by one author (BL) and validated by a second author (VL) according to the Theoretical Domains Framework. Based on these determinants, opportunities for iterative improvement in future initiatives in this setting were identified using the StrategEase tool. Reference Atkins, Francis and Islam17 This tool has been used in other studies to facilitate identification of behavior change strategies. Reference Craven, Holmes, Kettlewell and Radford18
Ethics
This evaluation was approved by Public Health Ontario’s Ethics Review Board (# 2024-020.01)
Results
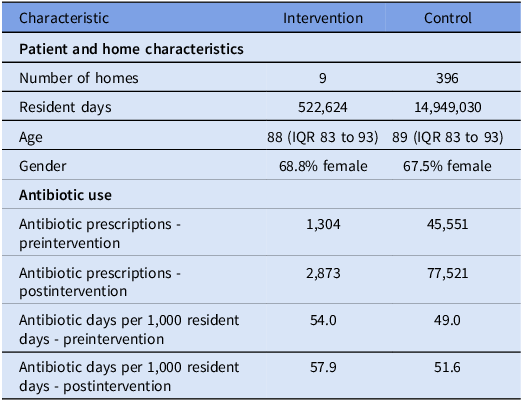
Nine intervention homes and 396 control homes were included in the analysis. The demographics were similar between groups. Median resident age in intervention homes was 88 years and in control homes was 89 years. The gender makeup was also similar with 68.8% female in the intervention homes and 67.5% female in the control homes. The total number of resident days was 522,624 in the intervention group and 14,949,030 in the control group (Table 1).
Retirement home and resident characteristics

IQR, interquartile range.
PAF recommendations
During the intervention period, across intervention homes, of 2,873 antimicrobial prescriptions, pharmacists assessed 794 new prescriptions for oral antibiotics, and made a total of 89 recommendations. Among these interventions, urinary tract infection was the most common indication (n = 26, 29%), followed by skin and soft tissue infection (n = 11, 12%), and respiratory tract infection (n = 9, 10%). Thirty-six prescriptions were for an unclear indication (40%). Of the recommendations made, 27 (30%) were accepted. Recommendations resulted in reduced antimicrobial duration (n = 24), switch to another agent (n = 2) and dose change (n = 1).
Antibiotic use
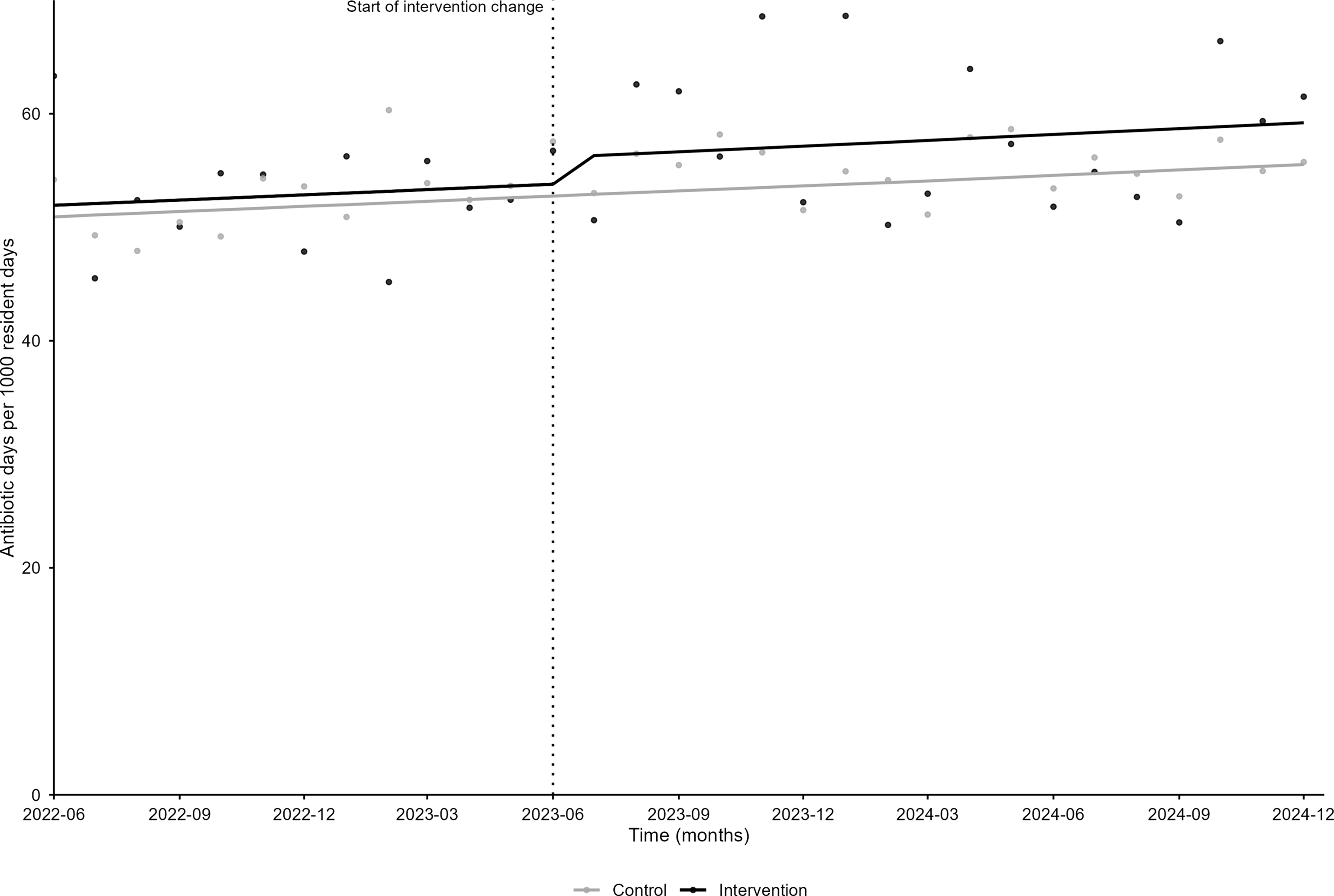
Total antibiotic use measured in DOT per 1000 resident days in intervention homes was similar before and after PAF (54.0 before vs 57.9 after). Similarly, usage in the control group was relatively stable (49.0 before vs 51.6 after). The difference-in-difference analysis showed no statistically significant association between the intervention and antibiotic usage when comparing intervention to control homes +2.4 DOT/1000 resident days (95% CI: −7.8 to 12.3, P = .6) (Figure 1).
Difference-in-differences analysis of antibiotic days (days of therapy) per 1,000 resident days from June 2022 to December 2024 between the intervention and control groups before and after the intervention.

Indication documentation
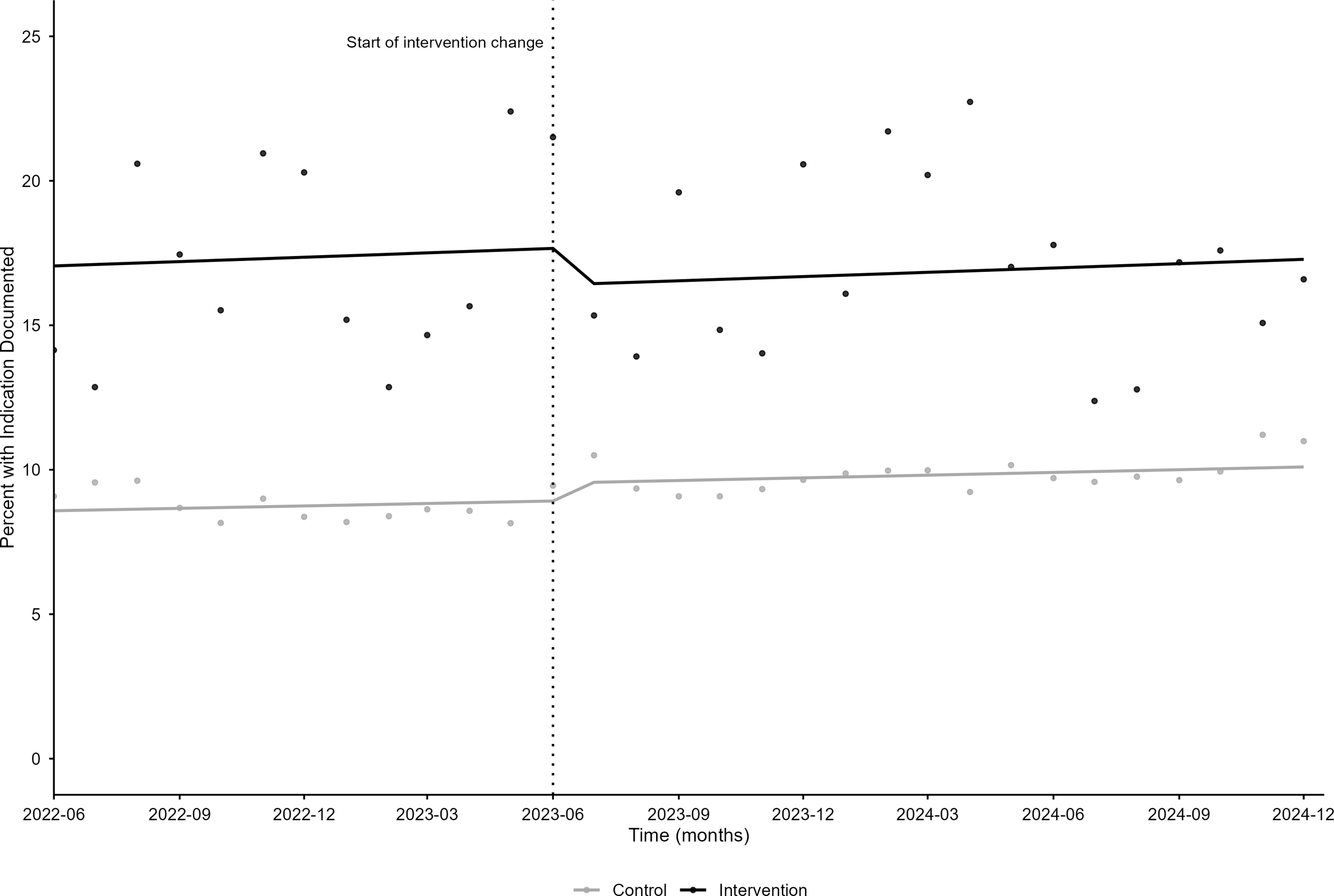
Documentation did not change substantially in the intervention group (before: 17.2%, after 17.0%) or the control group (before: 8.8%, after 9.8%). The difference-in-differences analysis showed a 1.9% (95% CI: −4.4 to 0.5) decrease in documentation of indication in the intervention group compared to the control group (Figure 2).
Antimicrobial indication documentation before and after a pilot prospective audit and feedback program.

Barriers and facilitators
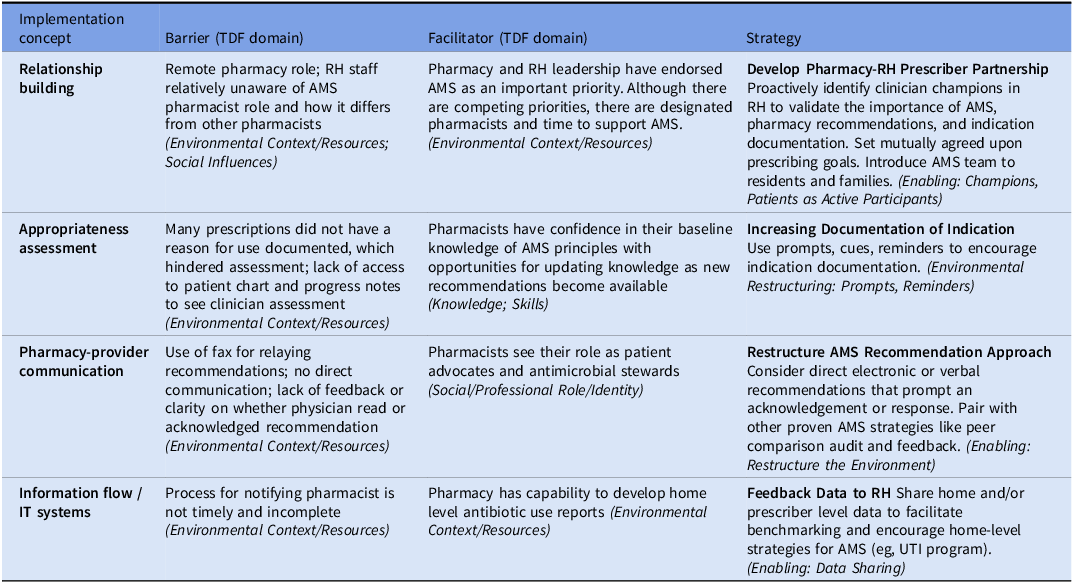
Several barriers and facilitators in the context of PAF implementation were identified based on discussion with pharmacists involved in the pilot (n = 3). Barriers were mapped to the current workflow and were mainly in the domain of environmental context/resources. Potential strategies to support AMS interventions in the future were generated based on these barriers and facilitators (See Table 2).
Barriers, facilitators and potential strategies to support antimicrobial stewardship in retirement homes

Note: Barriers and Facilitators were mapped to the Theoretical Domains Framework, shown in italics. Potential strategies identified via the StrategEase Tool. 21
RH, retirement home; AMS, antimicrobial stewardship; UTI, urinary tract infection.
Discussion
In this pilot of pharmacist-led PAF in the retirement home setting, there appeared to be no association between the intervention and AMU when comparing intervention to control homes. Similarly, indication documentation did not appear to improve significantly after the intervention.
Only 89 recommendations were made across 794 antimicrobial prescriptions assessed and 2,873 prescriptions overall, which may be an insufficient volume to effect meaningful overall change. This low proportion suggests greater resourcing or strategies to identify high yield interventions may be required to generate measurable impact. Additionally, limited access to clinical information including lack of indication for antibiotic prescriptions were also barriers to PAF and may have explained the relatively low proportion of prescriptions with recommendations. Documenting an indication for antibiotic prescriptions is a recommended practice that supports patient safety and appropriate antibiotic use, however it is not routine. Reference Saini, Leung and Si19 A previous study of antibiotic prescriptions from over 200 LTC homes found that 23% included an indication, the most common being urinary (45%), skin and soft tissue (19.9%) and respiratory infections (15.0%); however, there was also substantial variability in prevalence between homes with the overall median being 19.6% (IQR: 10.8%–31.4%). Reference Champaneria, Langford and Allen20 In this study, the prevalence of indication was lower for intervention and control homes at baseline and postintervention however this could be due to differences between the retirement home and LTC settings amongst other factors.
Several barriers related to implementation of PAF into the current workflow were identified and may have contributed to limited impact of the intervention. Most notably, indirect communication using fax to relay recommendations greatly limited the timeliness of recommendations reaching their intended audience because it relies on staff at the retirement home flagging the message to the prescriber. The lack of documented indication limited pharmacists’ ability to evaluate appropriateness and provide recommendations. Furthermore, when recommendations were made, the AMS pharmacist lacked a mechanism to determine whether the recommendation was acknowledged by the prescriber and if action was taken unless a new order was generated.
We identified organizational support and pharmacist motivation, knowledge, skills and expertise as facilitators to PAF in this pilot. Prior to implementation of the PAF intervention, AMU was not routinely monitored at the home level and there was no mechanism for benchmarking. Prior to this pilot, the number of new antibiotic prescriptions per month was sometimes used as a proxy for AMU however this does not account for duration of therapy which is crucial for determining overall exposure. During this project, CareRx established new capabilities and processes to capture DOTs at the home level for total antibiotics and by class. This represents a significant step toward establishing a comprehensive AMS program because these data are needed to support AMU surveillance as well as inform future local and overarching regional quality improvement interventions.
A strength of this study is its multi-facility sample with over 15,000,000 resident days and difference in difference design, minimizing the risk of bias. This study includes some potential limitations. The pharmacy dispensing data may have obscured some impacts of the intervention. In the absence of an electronic medication administration record, DOTs were calculated based on days supplied. Any changes in the duration of therapy as the result of the intervention would not have been reflected once the prescription was dispensed. For example, if nitrofurantoin was prescribed for 10 days and the PAF recommendation to decrease the duration to 5 days was accepted, the DOT captured for that resident would remain as 10 as that was the original days supplied even if that resident only ends up receiving 5 days of therapy. However, if PAF is successful in changing prescriber behavior then DOT should theoretically decrease over time. Additionally, there is potential for selection bias in that intervention homes may be already higher performing (eg, intervention homes had almost double the proportion of prescriptions with indication documentation), hence there could have been a lower opportunity for improvement in these homes. Further, since data on barriers and facilitators to stewardship in retirement homes was limited to the three pharmacists involved in the intervention, there is opportunity for a more in-depth qualitative analysis including a higher number and range of respondents to better understand these challenges and devise appropriate strategies. An additional limitation was that the barrier and facilitator assessment occurred after the conclusion of a relatively long pilot. An opportunity for improvement would have been to include earlier evaluation of implementation effectiveness, and implement iterative improvements based on these assessments.
Despite the lack of uptake and no association with improved AMU outcomes or indication documentation, this pilot revealed key barriers and facilitators for conducting PAF in the retirement home setting and increased local capabilities to conduct surveillance of AMU. To advance this and other AMS program interventions in this setting, future initiatives should consider direct, electronic communication for recommendations, strategies to improve indication documentation for antibiotic prescriptions and feedback of home and/or prescriber level data to facilitate benchmarking.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/ash.2026.10744.
Acknowledgements
None.
Author contribution
Study concept and design: Dan Dalton, Denis O’Donnell, Valerie Leung, Bradley J. Langford, Kevin Brown. Acquisition of data: Dan Dalton, Denis O’Donnell. Analysis and interpretation of data: Dan Dalton, Denis O’Donnell, Bradley J. Langford, Valerie Leung, Kevin Brown, Michelle Wong, Nick Daneman, and Kevin Schwartz. Preparation of manuscript: Dan Dalton, Denis O’Donnell, Bradley J. Langford, Valerie Leung, Kevin Brown, Michelle Wong, Nick Daneman, and Kevin Schwartz.
Financial support
This study was carried out as part of the authors’ routine work.
Competing interests
Dan Dalton, Denis O’Donnell, and Stephana Hung are employees of CareRx Pharmacy. Valerie Leung, Bradley J Langford, Kevin Brown, Michelle Wong, Nick Daneman, and Kevin Schwartz have no conflicts to declare.
Sponsor’s role
None.



 Open access
Open access