


Introduction
The first case of COVID-19, the infections disease associated with SARS-CoV-2 was identified in Ireland on February 29th, 2020, with the World Health Organisation (WHO), declaring COVID-19 a global pandemic on March 11th, 2020 (Yuki et al. Reference Yuki, Fujiogi and Koutsogiannaki2020). Robust public health restrictions were subsequently enforced in many countries, including Ireland, to mitigate the potential impact of the COVID-19 pandemic on health service delivery. Restrictions of varying severity were in place for almost two years (based on the advice of the National Public Health Emergency Team (NPHET), with the most stringent of these implemented for approximately half of this time. These included social gatherings of no more than six people, a ban on indoor dining, a restriction on people’s movements to within five kilometres of their home and the closure of many facilities deemed as “non-essential“ including those attended by individuals with both physical and mental health disorders such as day and training centres. Consequently, many therapeutic interventions normally available for individuals with mental health difficulties both within and outside mental health services were unattainable including group psychotherapeutic activities during this time. Where such services continued, most had to adapt to a range of public health measures, with for example face-to-face interactions often replaced by tele-consultations (Kopelovich et al. Reference Kopelovich, Monroe-DeVita, Buck, Brenner, Moser, Jarskog, Harker and Chwastiak2021; Li et al. Reference Li, Glecia, Kent-Wilkinson, Leidl, Kleib and Risling2021). Social isolation, a putative risk factor for a variety of mental disorders (Beutel et al. Reference Beutel, Klein, Brähler, Reiner, Jünger, Michal, Wiltink, Wild, Münzel, Lackner and Tibubos2017) was expected to place an additional strain on mental health services with the President of the Royal College of Psychiatrists in the United Kingdom warning of a “tsunami” of referrals to mental health services (Torjesen Reference Torjesen2020).
The impact of these prolonged periods of restrictions and lockdowns for individuals’ mental well-being is somewhat unclear with contrasting data available to date. For example, early research documented an initial increase in the prevalence of anxiety and depressive symptoms amongst individuals attending mental health services and in general population cohorts during 2020 (Santomauro et al. Reference Santomauro, Mantilla Herrera, Shadid, Zheng, Ashbaugh, Pigott, Abbafati, Adolph, Amlag, Aravkin, Bang-Jensen, Bertolacci, Bloom, Castellano, Castro, Chakrabarti, Chattopadhyay, Cogen, Collins and Dai2021), although this was not a universal finding (Plunkett et al. Reference Plunkett, Costello, McGovern, McDonald and Hallahan2021; McLoughlin et al. Reference McLoughlin, O’Grady and Hallahan2022), with longer-term veracity of this assertion challenged on the grounds that data were collected during the nascent phase of COVID-19 (early 2020), with anxiety symptoms related to an acute stress reaction or “shock effect” (Sun et al. Reference Sun, Adamis and McNicholas2024). A number of longitudinal studies conducted in Ireland have noted a relatively low level of symptoms and a modest impairment on functioning for individuals with pre-existing, anxiety, bipolar and psychotic disorders 6, 12, 24 and 48 months after the onset of the COVID-19 pandemic respectively (McLoughlin et al. Reference McLoughlin, Abdalla, Gonzalez, Freyne, Asghar and Ferguson2023; McLoughlin et al. Reference McLoughlin, O’Grady and Hallahan2022; Rainford et al. Reference Rainford, Moran, McMahon, Fahy, McDonald and Hallahan2023; Hennigan et al. Reference Hennigan, McGovern, Plunkett, Costello, McDonald and Hallahan2021; O’Gorman et al. Reference O’Gorman, Rainford, Devaney, O’Mahony, McLoughlin and Hallahan2024; O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024). However, significant individual variation has been noted within these studies, with studies including individuals diagnosed with emotionally unstable personality disorder (EUPD) demonstrating significant symptomatology (anxiety and depressive symptoms) at baseline and at several follow-up time periods with impaired functioning and reduced quality of life additionally noted (McLoughlin et al. Reference McLoughlin, O’Grady and Hallahan2022; O’Gorman et al. Reference O’Gorman, Rainford, Devaney, O’Mahony, McLoughlin and Hallahan2024; O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024).
Variable findings and opinions have been noted pertaining to rates of both self-harm (Reger et al. Reference Reger, Stanley and Joiner2020; McIntyre et al. Reference McIntyre, Tong, McMahon and Doherty2021; Steeg et al. Reference Steeg, John, Gunnell, Kapur, Dekel, Schmidt, Knipe, Arensman, Hawton, Higgins, Eyles, Macleod-Hall, McGuiness and Webb2022; O’Malley et al. Reference O’Malley, McIntyre, McGilloway, Doherty and Hallahan2023) and suicide (Leaune et al. Reference Leaune, Samuel, Oh, Poulet and Brunelin2020; Pirkis et al. Reference Pirkis, John, Shin, DelPozo-Banos, Arya, Analuisa-Aguilar, Appleby, Arensman, Bantjes, Baran, Bertolote, Borges, Brečić, Caine, Castelpietra, Chang, Colchester, Crompton, Curkovic, Deisenhammer, Du, Dwyer, Erlangsen, Faust, Fortune, Garrett, George, Gerstner, Gilissen, Gould, Hawton, Kanter, Kapur, Khan, Kirtley, Knipe, Kolves, Leske, Marahatta, Mittendorfer-Rutz, Neznanov, Niederkrotenthaler, Nielsen, Nordentoft, Oberlerchner, O’Connor, Pearson, Phillips, Platt, Plener, Psota, Qin, Radeloff, Rados, Reif, Reif-Leonhard, Rozanov, Schlang, Schneider, Semenova, Sinyor, Townsend, Ueda, Vijayakumar, Webb, Weerasinghe, Zalsman, Gunnell and Spittal2021; Mannix et al. Reference Mannix, Holleran, Cevikel, McMorrow, Nerney, Phelan, McDonald and Hallahan2024) after the onset of the COVID-19 pandemic. Some researchers have suggested that rates of self-harm in the early stages of the COVID-19 were under-reported, with individuals who did not perceive their episode of self-harm as severe enough to require immediate medical attention not presenting to hospital/emergency department(s) for support; this was further reflected by a greater lethality of method employed in those who did present with self-harm episodes (McIntyre et al. Reference McIntyre, Tong, McMahon and Doherty2021; Kar et al. Reference Kar, Menon, Yasir Arafat, Rai, Kaliamoorthy, Akter, Shukla, Sharma, Roy and Sridhar2021).
As it is now over two years since the WHO declared the end of the COVID-19 global pandemic (May 5th, 2023), it is likely that attributing current symptoms to the COVID-19 pandemic would be associated with significant confounders and thus new studies ascertaining the impact of the COVID-19 pandemic on various mental health disorders or self-harm presentations are unlikely. A systematic review ascertaining the impact of the COVID-19 pandemic across a range of mental health disorders and rates of self-harm and suicide would thus be timely and potentially informative, particularly if public health restrictions are needed for a future local or global pandemic. Consequently, we aimed to conduct a systematic review examining (i) the putative impact of the COVID-19 pandemic across a range of mental health disorders in relation to both symptoms and functioning; (ii) rates of referral and presentation to mental health services and emergency departments (EDs) for probable mental health disorders, self-harm and suicidal ideation; and (iii) any potential impact of COVID-19 on suicide rates. These questions were formulated after three meetings between the authors (RVA, SL, BH) with consensus attained form all authors. Given the vast differences in health services and delivery of mental health services globally, we have included research conducted solely in Ireland in this systematic review.
Methods
Data sources and study selection
We conducted a systematic bibliographic search for studies evaluating the impact of the COVID-19 pandemic on a range of mental health disorders, self-harm, and suicide within Ireland from the following databases: CINAHL, Medline, PsycINFO, PubMed and EMBASE. We searched for articles published between March 12th, 2020 (date NPHET first mandated public health restrictions) and December 20th, 2024 written in English, using medical subject heading key words: “COVID*” OR SARS-CoV” AND “mental health” OR “mental illness” OR “mental disorder” OR “psychiatric” OR “psychological” OR “depression” OR “depressive” OR “mania” OR “manic” OR “manic-depressive” OR “bipolar” OR “BPAD” OR “mood” OR “anxiety” OR “psychosis” OR “schizophrenia” OR “psychotic” OR “schizophreniform” OR “delusion*” OR “hallucination*” OR “OCD” OR “obsessive–compulsive” OR “obsessive compulsive” or “compulsive” OR “obsessions” OR “obsessive” OR “obsessional” OR “eating disorder” OR “anorexia” OR “bulimia” OR “binge eating” OR “bulimic” OR “personality disorder” OR “posttraumatic” OR “post-traumatic” OR “PTSD” OR “dissociative” OR “adjustment disorder” OR “suicidal” OR “suicide” OR “self-harm” OR “self-injury” OR “self-mutilation” AND “Ireland”. We also searched by hand, references from the research articles identified. The study was pre-registered on PROSPERO (ID: CRD42025626954) and conducted in accordance with “Preferred Reporting Items for Systematic Reviews and Meta-Analyses” (PRISMA) guidelines.
Prospective and retrospective cohort studies, analytical cross-sectional studies, randomised control trials, case–control studies, case series, and case reports were included in the systematic review. Studies were excluded if they (1) consisted of incomplete patient data, (2) were letters to the editor or did not include novel data in the study, (3) were conducted in individuals without a pre-existing mental health disorder or included individuals with neurodevelopmental disorders, substance use and addiction disorders, or neurocognitive disorders without the presence of other co-morbid mental health disorders and (4) were conducted in another jurisdiction.
Data extraction
Titles and abstracts of articles were independently screened by two reviewers (R.V.A. and S.L.). The full texts of remaining articles were assessed according to inclusion and exclusion criteria independently by the two reviewers, utilising Covidence Software (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org). Selected variables extracted included relevant outcomes (psychometric instrument measurement and qualitative comments pertaining to symptoms, functioning and quality of life), study characteristics (design, timeframe since onset of COVID-19 pandemic, psychometric instruments employed, population studies) and demographic characteristics (sample size, age and gender). Any disagreements were resolved with discussion with unresolved differences discussed with the senior author (B.H.)
Risk of bias was assessed utilising the Newcastle Ottawa Scale (NOS), which generates a score based on sample selection, comparability of groups and adequacy of exposure/outcome (Wells et al. Reference Wells, Shea, O’Connell, Peterson, Welch, Losos and Tugwel2011), with the Joanna Briggs Institute utilised for case reports (Munn et al. Reference Munn, Barker, Moola, Tufanaru, Stern, McArthur, Stephenson and Aromataris2020).
Results
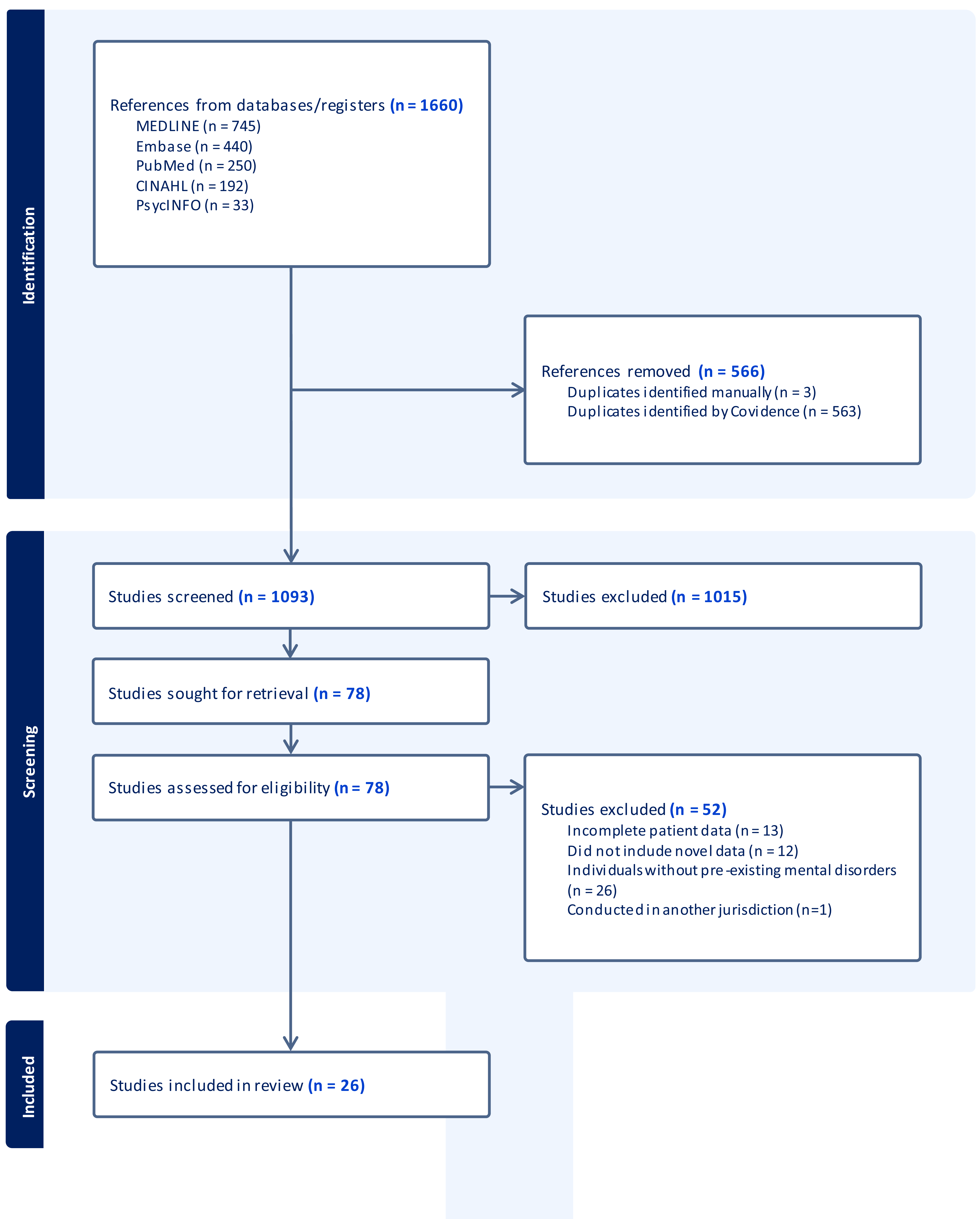
The PRISMA diagram summarising the literature search strategy is presented in Figure 1. A total of 1659 articles were identified, with 566 duplicates removed, with the remaining 1,093 screened. Seventy-eight full texts were reviewed, and 26 studies were included in the final systematic review. Excluded studies consisted of those with incomplete patient data (n = 13), included no novel data in their study design (n = 12), were conducted in individuals without a pre-existing mental health disorder (n = 26), with one study conducted in another jurisdiction.
Literature search.

Study design, socio-demographic and clinical characteristics, and findings of all included studies are provided in Table 1. There were 21 cross-sectional, four longitudinal cohort studies, and one case report included. Self-harm and suicide was the most-explored patient cohort (n = 12), with anxiety disorders (N = 11), psychotic disorders (n = 9), bipolar disorder (n = 7), major depressive disorder (n = 6), eating disorders (n = 6), OCD and related disorders (n = 4), EUPD (n = 4), and adjustment disorders (n = 1) also examined, with several studies examining more than one disorder. Eighteen studies examined referral or incident rates, with seven cross-sectional or longitudinal studies examining changes in clinical variables. The studies were equally divided between outpatient (N = 13) and inpatient (N = 13) settings.
Study characteristics and key findings

ADHD = Attention Deficit Hyperactivity Disorder; ASD = Autism Spectrum Disorder; BAI = Beck Anxiety Inventory; BD = Bipolar Disorder; BDI = Beck Depression Inventory; BHS = Beck Hopelessness Scale; CAMHS = Child and Adolescent Mental Health Services; CMHT = Community Mental Health Team; DUP = Duration of Untreated Psychosis; ED = Emergency Department; EUPD = Emotionally Unstable Personality Disorder; FEP = First-Episode of Psychosis; GAF = Global Assessment of Functioning; HARS = Hamilton Anxiety Rating Scale; IBW = Ideal Body Weight; ICD = International Classification of Diseases; MMSE = Mini-Mental State Examination; OSFED = Other specified Feeding or Eating Disorder; POLL = Psychiatry of Later Life.
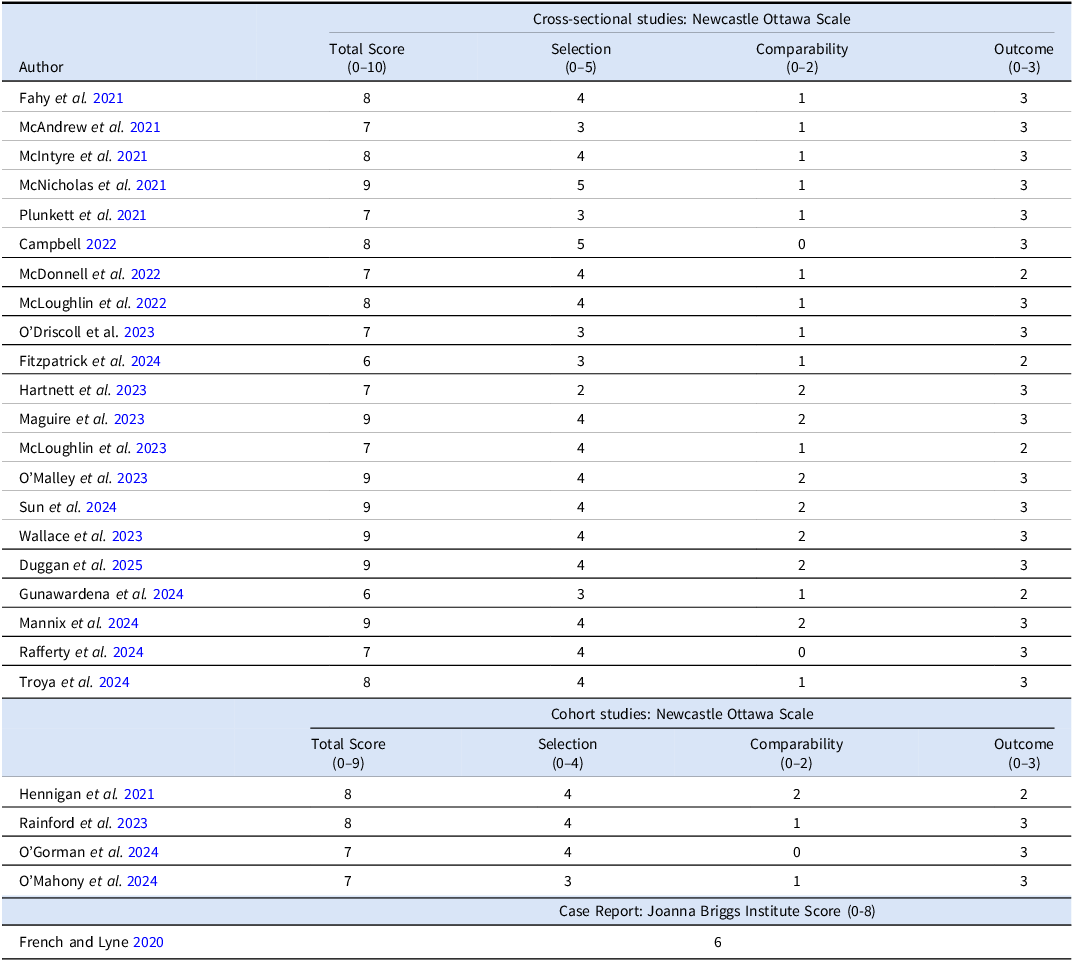
Risk of bias data for each study is presented in Table 2. Most studies fulfilled criteria to be denoted as either “good” (n = 15, 57.7%) or “very good” quality (n = 7, 26.9%) with four studies (15.4%) of “fair” quality and no “poor quality” studies included.
Risk of bias assessments

Very good quality = 9/10 score on Newcastle Ottawa Scale or 7/8 on Briggs Institute Score.
Good quality = 7/8 on Newcastle Ottawa Scale or 5/6 on Briggs Institute Score.
Fair quality = 5/6 on Newcastle Ottawa Scale or 4 on Briggs Institute Score.
Poor quality ≤ 5 on Newcastle Ottawa Scale or <4 on Briggs Institute Score.
Anxiety disorders and OCD
Of the eight studies examining rates of anxiety disorders, three noted an increase in presentations during the COVID-19 pandemic, with this increase noted in a CAMHS and liaison setting (McAndrew et al. Reference McAndrew, O’Leary, Cotter, Cannon, MacHale, Murphy and Barry2021; McDonnell et al. Reference McDonnell, Conlon, McNicholas, Barrett, Barrett, Cummins, Hensey, McAuliffe and Nicholson2022; Fitzpatrick et al. Reference Fitzpatrick, George, Lynch and McNicholas2024). Greater symptomatology was noted for females only in one study (McDonnell et al. Reference McDonnell, Conlon, McNicholas, Barrett, Barrett, Cummins, Hensey, McAuliffe and Nicholson2022). One cross-sectional study (Plunkett et al. Reference Plunkett, Costello, McGovern, McDonald and Hallahan2021) noted that individuals diagnosed with anxiety disorders observed a greater deterioration in their symptoms (50% reported a deterioration in symptomatology) compared to clinicians’ observations (27% noted as having a deterioration in symptomatology). Longitudinal follow-up of this cohort at three time-points noted no significant deleterious impact on psychometric measures of anxiety with modest mean anxiety symptoms evident, albeit a variable impact on social functioning was evident with significant variation in individuals’ symptoms and functioning noted (Hennigan et al. Reference Hennigan, McGovern, Plunkett, Costello, McDonald and Hallahan2021; O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024).
Self-harm/probable suicide
Twelve cross-sectional studies examined rates of self-harm and suicide. Seven studies noted increased rates of self-harm during the COVID-19 pandemic, including when this trend was not evident in the first 3-6 months of the COVID-19 pandemic period (O’Malley et al. Reference O’Malley, McIntyre, McGilloway, Doherty and Hallahan2023; Troya et al. Reference Troya, Corcoran, Arensman and Kavalidou2024). Increased presentations of self-harm were particularly evident in adolescents (Sun et al. Reference Sun, Adamis and McNicholas2024; Troya et al. Reference Troya, Corcoran, Arensman and Kavalidou2024). Data from the largest study in this patient cohort (National Clinical Programme for Self-Harm and Suicide-Related behaviours) noted that substance use likely contributed to presentations of self-harm for young males and people of Irish Traveller ethnicity (Maguire et al. Reference Maguire, Kavalidou, Bannan, Doherty and Jeffers2023). No difference in rates of probable suicide was demonstrated in the one study examining rates in a 2-year period pre and post the onset of the COVID-19 pandemic (Mannix et al. Reference Mannix, Holleran, Cevikel, McMorrow, Nerney, Phelan, McDonald and Hallahan2024).
Psychotic disorders
In studies examining individuals with diagnosed schizophrenia, including longitudinal follow-up studies (Fahy et al. Reference Fahy, Dineen, McDonald and Hallahan2021; Rainford et al. Reference Rainford, Moran, McMahon, Fahy, McDonald and Hallahan2023), no significant deleterious impact of the COVID-19 pandemic was evident although a minor impact on anxiety symptoms and social functioning was noted. A potential increase in FEP or presentations with psychosis to ED was noted in two studies (Duggan et al. Reference Duggan, Buckley, Fletcher, O’Keefe, Naughton, O’Connor and Clarke2025; Gunawardena et al. Reference Gunawardena, Godavarthi and Gethins2024), with a longer duration of untreated psychosis in women and increase in rates in an urban not rural area noted (Duggan et al. Reference Duggan, Buckley, Fletcher, O’Keefe, Naughton, O’Connor and Clarke2025).
Eating disorders
Five out of six studies noted an increase in either referral or presentation rates to ED or mental health services of individuals with eating disorders. Contrasting findings were noted in relation to metrics of eating disorder severity with higher ideal body weight (IBW) percentage loss noted in one (Campbell et al. Reference Campbell, Maunder, Lehmann, McKeown and McNicholas2022) but not another study (Rafferty et al. Reference Rafferty, O’Donnell, Campbell, Sun, King, Ali, Lynch, Barrett, Richardson, Clifford and McNicholas2024) during the COVID-19 pandemic. A shorter illness duration prior to referral to mental health services, was also noted in some studies (Campbell et al. Reference Campbell, Maunder, Lehmann, McKeown and McNicholas2022; Rafferty et al. Reference Rafferty, O’Donnell, Campbell, Sun, King, Ali, Lynch, Barrett, Richardson, Clifford and McNicholas2024).
Mood disorders
Five cross-sectional and two longitudinal cohort studies examined individuals with bipolar disorder. Studies noted minimal depressive or anxiety symptoms in this patient cohort with two longitudinal studies demonstrating no deterioration in mood or anxiety symptoms with improvements in quality of life and social functioning over time demonstrated (O’Gorman et al. Reference O’Gorman, Rainford, Devaney, O’Mahony, McLoughlin and Hallahan2024; O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024). Studies evaluating ED presentations demonstrated no increase in presentations of individuals with mood disorders.
An increase in individuals presenting with subjective symptoms of low mood (transient feelings of sadness and anhedonia) without a corresponding increase in major depressive disorder was noted in one study (Sun et al. Reference Sun, Adamis and McNicholas2024).
Emotionally unstable personality disorder (EUPD)
Two cross-sectional studies and two longitudinal cohort study examined personality disorders, with each of these studies evaluating EUPD and at least one other patient cohort. No other personality disorders were evaluated. An EUPD cohort was found to experience significant anxiety symptoms, with impairments in quality of life and functioning noted, with qualitative data noting that limited mental health supports secondary to the COVID-19 pandemic had a deleterious for their health and quality of life. A cross sectional study (McLoughlin et al. Reference McLoughlin, O’Grady and Hallahan2022) and subsequent longitudinal studies of the same patient cohort (O’Gorman et al. Reference O’Gorman, Rainford, Devaney, O’Mahony, McLoughlin and Hallahan2024; O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024) demonstrated that individuals attending an outpatient clinic with emotionally unstable personality disorder had significantly higher anxiety, depression, impulsivity and hopelessness scores, and greater impairment in social functioning and quality of life, than individuals with either bipolar disorder (O’Gorman et al. Reference O’Gorman, Rainford, Devaney, O’Mahony, McLoughlin and Hallahan2024; O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024) or anxiety disorders (O’Mahony et al. Reference O’Mahony, Aylward, McLoughlin, McLoughlin and Hallahan2024). One study examining rates of self-harm noted both pre- and post-COVID-19 that EUPD and substance use were the most common disorders present.
Discussion
Overall, there was no evidence of a large and widespread increase in, or exacerbation of mental disorders during the COVID-19 pandemic. However, there were nuanced and disorder-specific findings, with increased presentations of self-harm and eating disorders to EDs or mental health services evident, as well as greater distress and reduced functionality for individuals diagnosed with EUPD. This review focuses upon diagnosable mental disorders and therefore does not seek to capture reports of pandemic-related deterioration in mental health (anxiety, self-image, social connectivity, gambling) which might potentially be identified by self-report or presentations to counselling services and disproportionately affect a younger cohort.
Several studies noted an increase in presentations of self-harm to EDs especially in comparison to the presentation of other mental or physical health conditions, albeit an initial reduction in self-harm presentations after the onset of the COVID-19 pandemic was noted (McIntyre et al. Reference McIntyre, Tong, McMahon and Doherty2021), a finding consistent with international cohorts and likely related to individuals having a higher threshold for help-seeking, only presenting to EDs with more severe cases of self-harm in the initial months following the onset of the COVID-19 pandemic (McIntyre et al. Reference McIntyre, Tong, McMahon and Doherty2021; Jollant et al. Reference Jollant, Roussot, Corruble, Chauvet-Gelinier, Falissard, Mikaeloff and Quantin2021; Kar et al. Reference Kar, Menon, Yasir Arafat, Rai, Kaliamoorthy, Akter, Shukla, Sharma, Roy and Sridhar2021; Steeg et al. Reference Steeg, John, Gunnell, Kapur, Dekel, Schmidt, Knipe, Arensman, Hawton, Higgins, Eyles, Macleod-Hall, McGuiness and Webb2022) or potentially using alternative sources of support post self-harm (i.e. engagement with other support services such as Pieta House (Irish Examiner 2021)). A fear of contracting COVID-19 was prevalent in the initial period of the pandemic and resulted in individuals with significant medical conditions (i.e. cardiac events) similarly avoiding hospitals (Kristoffersen et al. Reference Kristofferson, Jahr, Thommessen and Rønning2020; Mafham et al. Reference Mafham, Spata, Goldacre, Gair, Curnow, Bray, Hollings, Roebuck, Gale, Mamas, Deanfield, de Belder, Luescher, Denwood, Landray, Emberson, Collins, Morris, Casadei and Baigent2020). No difference in rates of probable suicide was demonstrated in a 2-year period pre and post the onset of the COVID-19 pandemic, however this was the only Irish study conducted and only examined one region in Ireland. However, the findings are consistent with a systematic review of 34 studies from 25 countries with pooled suicide rates pre COVID-19 pandemic (11.35 per 100,000, 95% CI 9.35–13.42) similar and not statistically different to those during the COVID-19 pandemic (10.65 per 100,000, 95% CI 8.61–12.68) (da Cunha Varella et al. Reference da Cunha Varella, Griffin, Khashan and Kabir2024).
Individuals with EUPD exhibited significant symptomatology and poor functioning, although this patient cohort was not extensively studied. However, it is probable that similar factors accounted for increased rates of presentations of self-harm and distress for individuals with EUPD. The public health measures enforced in many countries have been shown to most effect those who endorse a sense of isolation (Henssler et al. Reference Henssler, Stock, van Bohemen, Walter, Heinz and Brandt2021), and thus likely impacted a greater proportion of individuals who were already isolated or those with a diagnosis of EUPD, given their greater sensitivity to feelings of emptiness, fears of abandonment (Fonagy and Bateman Reference Fonagy and Bateman2008), and thwarted desired closeness (attachment) (Ikhtabi et al. Reference Ikhtabi, Pitman, Toh, Birken, Pearce and Johnson2022). Participants with EUPD described isolation and distress secondary to the COVID-19 pandemic and associated mandated restrictions, would likely exacerbate any pre-existing interpersonal difficulties experienced (Skodol et al. Reference Skodol, Pagano, Bender, Shea, Gunderson, Yen, Stout, Morey, Sanislow and Grilo2005). The deleterious impact of the COVID-19 pandemic on mental health delivery (both within and outside mental health services) likely had a disproportionate impact for individuals with EUPD, given that many of the evidence based therapeutic interventions are predominantly group-based in nature (i.e. Decider Skills Therapy, Dialectical Behaviour Therapy, Mentalisation Based). Voluntary and service-user led supports often involving group therapeutic sessions and supports linked to non-therapeutic activities (i.e. group sporting activities) were also largely unavailable. It is possible that these reduced supports available impacted rates of self-harm presentations for individuals already engaged in and in those unknown to mental health services.
There was a consistent and substantial increase in anorexia nervosa and other eating disorder presentations, which is consistent with data in other jurisdictions (Agostino et al. Reference Agostino, Burstein, Moubayed, Taddeo, Grady, Vyver, Dimitropoulos, Dominic and Coelho2021; Spettigue et al. Reference Spettigue, Obeid, Erbach, Feder, Finner, Harrison, Isserlin, Robinson and Norris2021). A meta-analysis of almost 5 million individuals (predominantly from the United States of America) noted an increase in prevalence of eating disorders with increased symptom severity of anorexia nervosa, but not other eating disorders demonstrated (Guzel et al. Reference Guzel, Mutlu and Molendijk2023). This may have reflected an increase in exposure to weight and body image messaging. For example, public health messages aimed at supporting health lifestyles including healthy eating and physical activity could for some individuals have had a deleterious effect. It has been argued that mandated restrictions secondary to COVID-19, aligned with limited primary care (and mental health services) and social supports added to public health messaging led to some people including adolescents becoming more pre-occupied with body-shape, and over-reliant on dieting following physical activity restrictions (Puhl et al. Reference Puhl, Lessard, Larson, Eisenberg and Neumark-Stzainer2020, Miniati et al. Reference Miniati, Marzetti, Palagini, Marazziti, Orrù, Conversano and Gemignani2021; Rafferty et al. Reference Rafferty, O’Donnell, Campbell, Sun, King, Ali, Lynch, Barrett, Richardson, Clifford and McNicholas2024). Additionally, it has been postulated that more limited access to food and grocery trip, may have resulted in food insecurity and hoarding resulting in increased urges to binge (Gao et al. Reference Gao, Bagheri and Furuya-Kanamori2022).
The COVID-19 pandemic appeared to have a limited deleterious impact on individuals with pre-existing psychotic and mood disorders, with other jurisdictions noting similar findings (Kunzler et al. Reference Kunzler, Lindner, Röthke, Schäfer, Metzendorf, Sachkova, Müller-Eberstein, Klinger, Burns, Coenen and Lieb2023). There are several putative reasons for this. Despite the presence of enduring mental disorders, many of these participants were predominantly stable from a mental health perspective. Even though there was a general limited availability of community and mental health supports, many continued to attain input from their mental health team with mandated face-to-face interactions often required unlike other cohorts (i.e. blood tests due to lithium and clozapine treatment). Unlike individuals experiencing symptoms of mental disorder de novo (and perhaps unlike those presenting with a first episode of psychosis (FEP)), these participants had a greater awareness of how to access supports and had likely learnt techniques to reduce their distress due to their prior engagement with mental health services. Reports of an increase of FEP presentations (Duggan et al. Reference Duggan, Buckley, Fletcher, O’Keefe, Naughton, O’Connor and Clarke2025), has previously been noted in some international studies (Esposito et al. Reference Esposito, D’Agostino, Osso, Fiorentini, Prunas, Callari and Brambilla2021; Valdes-Florida et al. Reference Valdés-Florido, López-Díaz, Palermo-Zeballos, Garrido-Torres, Álvarez-Gil, Martínez-Molina, Martín-Gil, Ruiz-Ruiz, Mota-Molina, Algarín-Moriana, Guzmán-Del Castillo, Ruiz-Arcos, Gómez-Coronado, Galiano-Rus, Rosa-Ruiz, Prados-Ojeda, Gutierrez-Rojas, Crespo-Facorro and Ruiz-Veguilla2022; Kelbrick et al. Reference Kelbrick, da Silva, Griffiths, Ansari, Paduret, Tanner, Mann and Johnson2023), with pandemic related stress suggested as a major contributory factor (Bassiony et al. Reference Bassiony, Sehlo, Ibrahim, Zayed and Atwa2023), with stress known to constitute an independent risk factor for psychosis (Shah and Malla Reference Shah and Malla2015).
Some participants with psychosis as evidenced by qualitative comments (Fahy et al. Reference Fahy, Dineen, McDonald and Hallahan2021) noted no significant impacted on their occupational or social life, given that some had an existing limited repertoire of social activities. In addition, a diagnosis of a severe or enduring mental disorder does not mitigate against an individuals’ ability to be resilient. Many participants across the cohorts’ studied, demonstrated limited symptomatology and functioned well and likely engaged in appropriate coping mechanisms and demonstrated significant resilience.
Limitations and strengths
This systematic review has a number of limitations. The majority of included studies were cross-sectional in design, which limits the potential to draw causal relationships. Given the unanticipated nature of the onset of the COVID-19 pandemic, there was an absence of pre-pandemic psychometric data (i.e. measures of anxiety or depressive symptoms) limiting the ability to draw precise conclusions about the impact of the pandemic on symptomatology. However, the inclusion of both longitudinal studies and qualitative data in several of these studies supports findings of significant variability of symptoms for individuals, with certain cohorts of individuals (i.e. EUPD) experiencing reduced functionality secondary to the COVID-19 pandemic. There was a lack of detailed reporting of statistical data, including standard deviations, and consequently meta-analyses were not feasible. There was an under-representation of certain disorders, namely recurrent depressive disorder, obsessive compulsive disorder, post-traumatic stress disorder and personality disorders. We included studies that examined both children/adolescents and adult cohorts, with some studies including data pertaining to both groups (O’Driscoll et al. Reference O’Driscoll, Jennings, Clifford, Maher, Corbett, Wade, Dunne, Collins and McDevitt2023; Sun et al. Reference Sun, Adamis and McNicholas2024). Given there are often differences in symptoms and prognosis between children/adolescents and adults, caution is required in interpreting findings. A major caveat of the data is the pandemic-related reduction in healthcare utilisation and ED attendance. This could have masked changes in presentations of various mental disorders. Individuals with chronic and enduring mental illnesses who already have reduced healthcare engagement may have been particularly less likely to seek medical attention during the pandemic. Finally, given the vast differences in delivery of mental health services globally, we only included Irish data. Whilst many of our findings are consistent with other international studies, including only Irish data significantly impacts the generalisability of our findings.
Conclusion
Although there was not a widespread major exacerbation of symptoms for individuals with pre-existing mental disorders, certain cohorts including individuals with EUPD and eating disorders demonstrated greater symptomatology and impaired functioning during the COVID-19 pandemic. Our findings do not offer reasons for changes in mental health presentations during the pandemic but do provide an overview of the impact of COVID-19 on mental illness in Ireland. While the findings might not be generalisable to other countries, they are of interest for comparing with the pandemic impact on mental illness in other countries. Furthermore, this research highlights the potential future need for targeted interventions and supports in the event of future pandemics or public health restrictions.
Author contributions
All authors participated in the design of the study, data attainment and critical review of the manuscript.
Funding statement
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
None.
Ethical standards
Ethical approval was obtained for each individual study included in the systematic review. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committee on human experimentation with the Helsinki Declaration of 1975, as revised in 2008.
Disclosure statement
The authors declare that they have no conflict of interest. All authors have seen and approved the final version of the manuscript and believe that the manuscript represents work completed.


 Open access
Open access