


Significant outcomes
-
• Sequential tDCS significantly improved both mood symptom and motor symptoms in Parkinson’s disease patients with comorbid depression.
-
• Changes in apathy severity were strongly correlated with improvements in daily step counts.
-
• Smart device monitoring provided ecologically valid insights into real-world behavioural changes beyond clinical scales.
Limitations
-
• No sham-controlled group was included, limiting causal inference due to potential placebo effects.
-
• Follow-up data were not collected, making it unclear whether the observed results were sustained over time.
-
• Small sample size reduces generalizability and calls for larger-scale validation.
Introduction
Parkinson’s disease (PD) is a neurodegenerative disorder characterised by a spectrum of motor symptoms encompassing tremor, rigidity, and bradykinesia. In addition to these motor manifestations, people with PD frequently experience non-motor symptoms – most notably mood disturbances and sleep problem – which substantially contribute to reduced quality of life (Avanzino et al., Reference Avanzino, Lagravinese, Abbruzzese and Pelosin2018). Recent studies propose that individuals experiencing freezing episodes in PD exhibit heightened connectivity within the striato-limbic network and diminished connectivity within the fronto-parietal network (Reijnders et al., Reference Reijnders, Ehrt, Weber, Aarsland and Leentjens2008; Broeder et al., Reference Broeder, Nackaerts, Heremans, Vervoort, Meesen, Verheyden and Nieuwboer2015). Given that aberrant connectivity within the fronto-limbic system is associated with negative mood symptoms, neurobiological changes in the brains of PD patients may therefore affect not only motor function but also affective symptoms (Weintraub et al., Reference Weintraub, Moberg, Duda, Katz and Stern2004; Alamian et al., Reference Alamian, Hincapié, Combrisson, Thiery, Martel, Althukov and Jerbi2017). Mood disturbances can exacerbate motor symptoms, and conversely, the physical limitations imposed by motor symptoms can contribute to emotional distress (Schrag, Reference Schrag2006). Moreover, mood regulation is closely related to treatment engagement and adherence; individuals with better emotional well-being are more likely to follow medication regimens, participate in rehabilitation, and remain actively involved in their care. Effective management of mood symptoms may also enhance social functioning and reduce isolation, fostering a more supportive environment for coping with chronic illness (Getz & Levin, Reference Getz and Levin2017). Thus, mood regulation represents an important therapeutic target alongside motor symptoms, reflecting the close interplay between the neurological and psychological dimensions of the disease. Recognising and treating mood dysregulation in PD is integral to comprehensive care and may improve overall quality of life.
Even though dopamine replacement therapy has been the mainstay of PD treatment, the therapeutic benefit of dopaminergic medications often becomes less stable, with many patients developing motor fluctuations characterised by alternating periods of improved mobility (‘ON’ state) and worsening symptoms (‘OFF’ state) that can be increasingly difficult to predict and manage (Teymourian et al., Reference Teymourian, Tehrani, Longardner, Mahato, Podhajny, Moon, Kotagiri, Sempionatto, Litvan and Wang2022). In addition, long-term dopaminergic therapy is also associated with levodopa-induced dyskinesia, further complicating symptom control and daily functioning (Cornett et al., Reference Cornett, Novitch, Kaye, Kata and Kaye2017). Therefore, while dopamine replacement therapy may produce transient improvements in motor symptoms and, in turn, in non-motor symptoms that are reciprocally influenced by motor function, these benefits are likely to be short-lived; as long as motor symptoms fluctuate, non-motor domains, including mood, may be also prone to fluctuation. Accordingly, a treatment strategy for PD that relies solely on dopamine replacement therapy is inherently limited.
Recently, interest has grown in non-invasive neuromodulation techniques such as transcranial direct current stimulation (tDCS) as potential or alternative adjunctive therapies for PD. tDCS is simple to administer, well-tolerated, and generally associated with a low risk of adverse effects (Matsumoto & Ugawa, Reference Matsumoto and Ugawa2017), making it an attractive candidate for long-term or repeated intervention. While tDCS has already established its efficacy in treating depression and is widely utilised in clinical practice, its application in PD remains an area of ongoing research. (Jog et al., Reference Jog, Anderson, Kubicki, Boucher, Leaver, Hellemann, Iacoboni, Woods and Narr2023). Numerous studies have scrutinised the impact of tDCS on motor symptoms in PD, yielding mixed or inconclusive results (Benninger et al., Reference Benninger, Lomarev, Lopez, Wassermann, Li, Considine and Hallett2010; Doruk et al., Reference Doruk, Gray, Bravo, Pascual-Leone and Fregni2014; Simpson and Mak, Reference Simpson and Mak2020).
Parallel to advances in neuromodulation, wearable technology offers new opportunities to quantify PD symptoms in real-world settings. Smart band equipped with accelerometers and gyroscopes enable continuous or long-term monitoring of fluctuating motor features, including tremor, gait abnormalities, and changes in movement patterns (Maetzler et al., Reference Maetzler, Domingos, Srulijes, Ferreira and Bloem2013; Cancela et al., Reference Cancela, Pastorino, Tzallas, Tsipouras, Rigas, Arredondo and Fotiadis2014; Adams et al., Reference Adams, Dinesh, Snyder, Xiong, Tarolli, Sharma, Dorsey and Sharma2021). Wearables can also provide objective indices of daily activity and sleep, complementing clinic-based assessments and self-reported outcomes (Concheiro-Moscoso et al., Reference Concheiro-Moscoso, Groba, Martínez-Martínez, Miranda-Duro Mía del, Nieto-Riveiro, Pousada and Pereira2022; Concheiro-Moscoso et al., Reference Concheiro-Moscoso, Groba, Alvarez-Estevez, Miranda-Duro Mía del, Pousada, Nieto-Riveiro, Mejuto-Muiño and Pereira2023). Incorporating such digital measures may improve sensitivity to treatment-related changes and facilitate individualised assessment of symptom dynamics.
Patients with PD typically suffer from both motor and non-motor symptoms, which are closely interrelated. While conventional interventions have primarily targeted motor dysfunction, the present study sought to investigate whether targeting a non-motor domain, specifically mood, could be associated with favourable changes in motor function. Accordingly, we examined the effects of sequential bilateral dorsolateral prefrontal cortex (DLPFC) tDCS on both mood and motor symptoms in individuals with PD. Furthermore, we incorporated wearable smart devices to provide an objective, real-world evaluation of potential changes in daily activity levels and sleep patterns following the intervention.
Methods
Participants
Participants were recruited from the outpatient neurology clinic at Korea University Medical Center, Ansan Hospital. Participants comprised individuals diagnosed with PD based on the UK Brain Bank diagnostic criteria (Postuma et al., Reference Postuma, Poewe, Litvan, Lewis, Lang, Halliday, Goetz, Chan, Slow and Seppi2018). To increase diagnostic certainty, participants who have decreased dopamine transporters (DATs) in the posterior putamen on 123I-N-fluoropropyl-2β-carbomethoxy-3β-(4-iodophenyl) nortropane (FP-CIT) PET were included.
Inclusion criteria were: (1) age ≥19 years and <80 years; and (2) mild-to-moderate concomitant depressive symptoms as assessed using the Korean version of the Montgomery–Åsberg Depression Rating Scale (K-MADRS)(AHN et al., Reference Y-M, K-Y, J-S, M-H, D-H, J-L, Shin, H-K, YEON and J-H2005). Mild-to-moderate depression was defined as a K-MADRS score of 7–34, as evaluated by an experienced psychiatrist (Stuart A Montgomery and Åsberg, Reference Montgomery and Åsberg1979) (H.K. Yoon).
Exclusion criteria were: (1) severe depressive symptoms (K-MADRS ≥35) or clinical need for immediate treatment of depression; (2) cognitive impairment (K-MMSE < 24); (3) changes in antiparkinsonian medication within the past 6 months; (4) current use of psychotropic medications, including antidepressants, anxiolytics, hypnotics, or melatonin; and (5) systemic medical conditions or language disorders deemed likely to interfere with reliable scale assessments.
Study design
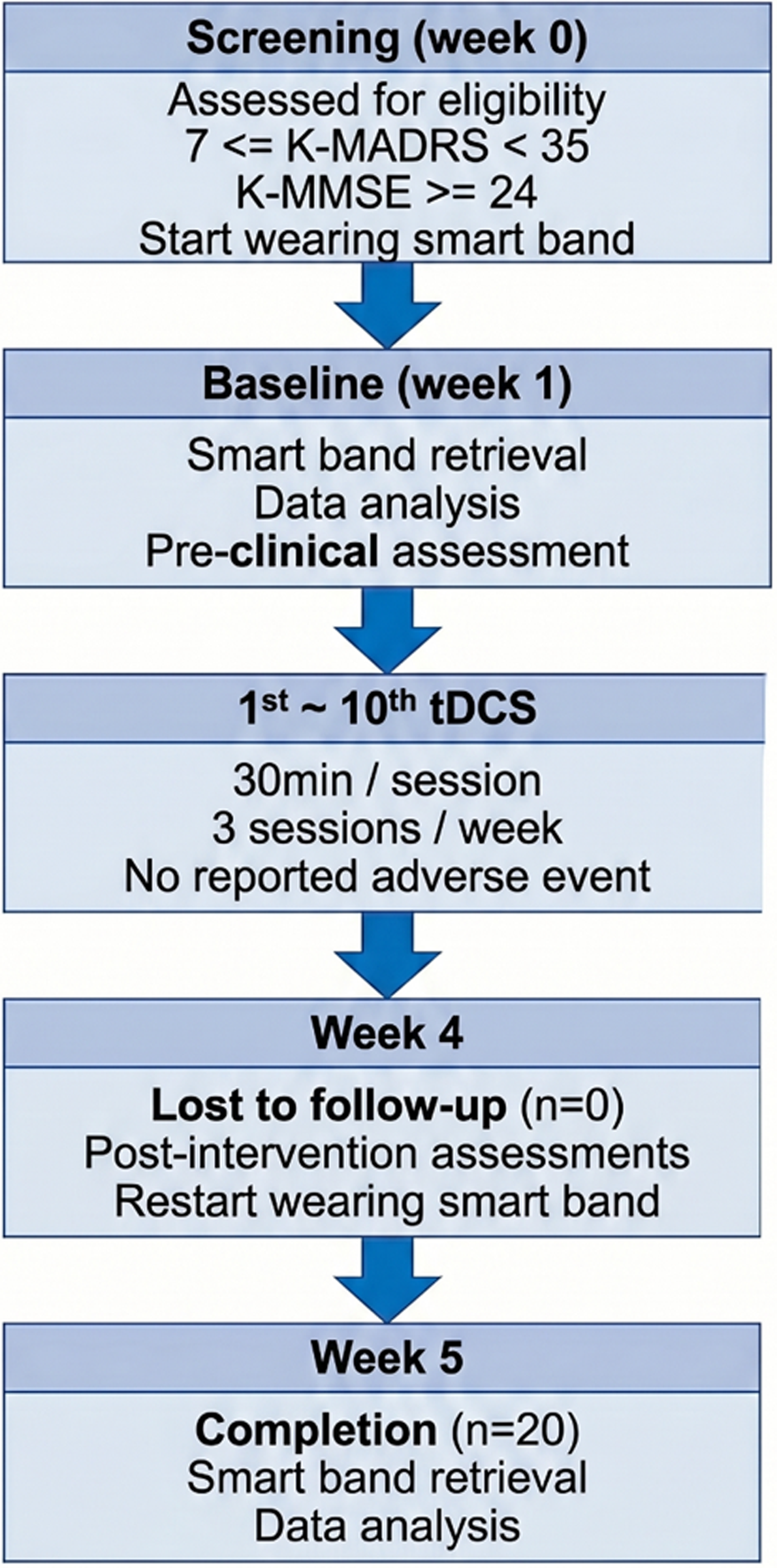
A longitudinal, single-arm design was employed. At screening (week 0), eligibility was confirmed (K-MADRS score 7–34 and K-MMSE ≥ 24). After enrolment, participants began wearing a smart band. At week 1, the smart band was retrieved for baseline data extraction, and participants completed the baseline clinical assessment (motor function, depressive symptom, anxiety, apathy, and quality of life). Participants then underwent a total of 10 tDCS sessions, administered three times per week on Monday, Wednesday, and Friday. Throughout the entire study period, all participants maintained their pre-existing antiparkinsonian medication regimens, and no changes in the type or dosage of drugs were permitted. Immediately following the completion of the final tDCS session, participants again completed the full set of clinical assessments and resumed smart device-based monitoring for an additional seven consecutive days to capture post-intervention changes in activity and sleep patterns (Figure 1).
Flowchart of the study design.

Clinical assessments
PD motor function was evaluated using the Hoehn and Yahr (HY) staging scale (Hoehn & Yahr, Reference Hoehn and Yahr1967) and the Unified Parkinson’s Disease Rating Scale (UPDRS) part III (Jankovic, Reference Jankovic2008). Depressive symptoms were measured using K-MADRS (S. A. Montgomery & Asberg, Reference Montgomery and Asberg1979). Anxiety symptoms were assessed using the State–Trait Anxiety Inventory (STAI) (Spielberger et al., Reference Spielberger, Gonzalez-Reigosa, Martinez-Urrutia, Natalicio and Natalicio1971). Apathy was evaluated using the Apathy Scale (AS) (Robert et al., Reference Robert, Onyike, Leentjens, Dujardin, Aalten, Starkstein, Verhey, Yessavage, Clement and Drapier2009). Quality of life was assessed using the Parkinson’s Disease Questionnaire-39 (PDQ-39) (Kwon et al., Reference Kwon, Kim, Ma, Ahn, Cho, Lee, Chung, Kim, Baik and Koh2013). Global cognitive function was assessed using the K-MMSE (Kang et al., Reference Kang, NA and Hahn1997). To ensure the standardisation of motor assessment and minimise the confounding effects of dopaminergic medication, all clinical evaluations, including the UPDRS Part III, were performed consistently in the medication ‘ON’ state. Specifically, assessments were conducted at the same time of day for each participant (e.g., approximately 1–2 h after the morning dose) to account for diurnal motor fluctuations and the peak effect of medication.
Smart device-based activity and sleep monitoring
Participants were instructed to wear a Xiaomi Mi Band 2 (Anhui Huami Information Technology Co., Ltd., Hefei, China) continuously for seven consecutive days before and after the tDCS intervention period. The Mi Band 2 is a commercially available wrist-worn activity tracker equipped with a triaxial accelerometer to monitor physical activity and an optical sensor to estimate sleep parameters (Xie et al., Reference Xie, Wen, Liang, Jia, Gao and Lei2018). Several previous studies have demonstrated the validity and acceptable accuracy of the Xiaomi Mi Band 2 for assessing both step counts and sleep parameters including sleep duration and sleep stages (Casado-Robles et al., Reference Casado-Robles, Mayorga-Vega, Guijarro-Romero and Viciana2023; Concheiro-Moscoso et al., Reference Concheiro-Moscoso, Groba, Alvarez-Estevez, Miranda-Duro Mía del, Pousada, Nieto-Riveiro, Mejuto-Muiño and Pereira2023; de la Casa Pérez et al., Reference de la Casa Pérez, Latorre Roman, Munoz Jimenez, Lucena Zurita, Laredo Aguilera, Párraga Montilla and Cabrera Linares2022; Pino-Ortega et al., Reference Pino-Ortega, Gómez-Carmona and Rico-González2021). We used this device to objectively record daily activity, quantified as the mean daily step count (steps per day), and sleep patterns, including total sleep time (minutes per day), duration of light sleep and deep sleep, and periods of wakefulness after sleep onset (WASO). Data were synchronised using the Mi Fit mobile application (Huami Technology), exported in CSV format, and processed using Microsoft Excel and IBM SPSS Statistics (version 27.0). Valid data were defined as at least 10 h of daytime wear per day for activity monitoring and complete overnight wear for sleep data collection. Days with incomplete data or technical errors (e.g., zero activity counts) were excluded from analysis. Due to the lack of an automated total recording time log in the wearable device, data validity was confirmed by cross-referencing activity logs with participant and family reports.
tDCS protocol
We used the MINDD STIM (Ybrain Inc., Seongnam, Republic of Korea), a tDCS device approved by the Ministry of Food and Drug Safety in Korea. The MINDD STIM employs circular electrodes with a diameter of 6 cm (surface area: 28.3 cm2), consisting of conductive rubber electrodes in contact with single-use sponge pads soaked in physiological saline (0.9% NaCl) to ensure adequate conductivity. In our study, stimulation was delivered at an intensity of 2 mA (current density: 0.07 mA/cm2) for 30 min per session, three times per week, for a total of 10 sessions over approximately 4 weeks. The system performs real-time impedance monitoring and initiates and maintains stimulation only when impedance is within the range of 500 Ω to 10 kΩ; if impedance falls outside this range or an electrode becomes detached, stimulation is automatically interrupted or terminated. A 30-s ramp-up and ramp-down procedure was used at the beginning and end of each session. Reported adverse effects of MINDD STIM are predominantly mild, transient local skin reactions, such as tingling, itching, and erythema at the electrode sites (Brunoni et al., Reference Brunoni, Amadera, Berbel, Volz, Rizzerio and Fregni2011; Matsumoto & Ugawa, Reference Matsumoto and Ugawa2017). We employed a montage widely used for the treatment of depression, placing the anodal electrode over the left dorsolateral prefrontal cortex (DLPFC; F3) and the cathodal electrode over the right DLPFC (F4), in accordance with the international 10–20 electroencephalography (EEG) system (Dedoncker et al., Reference Dedoncker, Brunoni, Baeken and Vanderhasselt2016; Lefaucheur et al., Reference Lefaucheur, Antal, Ayache, Benninger, Brunelin, Cogiamanian, Cotelli, De Ridder, Ferrucci, Langguth, Marangolo, Mylius, Nitsche, Padberg, Palm, Poulet, Priori, Rossi, Schecklmann, Vanneste, Ziemann, Garcia-Larrea and Paulus2017).
Statistical analyses
Statistical analyses were conducted using IBM SPSS Statistics (version 27.0). Continuous variables were reported as means ± standard deviations and 95% confidence intervals. Normality of distributions was assessed using the Shapiro–Wilk test. Pre- and post-tDCS measurements from both Xiaomi Mi Band 2.0 and clinical scales were compared using paired t-tests or Wilcoxon signed-rank tests, as appropriate. Associations between changes in Xiaomi Mi Band 2.0 data and clinical scale scores were assessed using Spearman’s rank correlation. In statistical analyses, a p-value less than 0.05 is generally considered statistically significant. However, in this study, five separate tests were conducted on the smart device data, which could increase the risk of Type I error. To control for this, a Bonferroni correction was applied, and the significance threshold was adjusted to p < 0.01.
Results
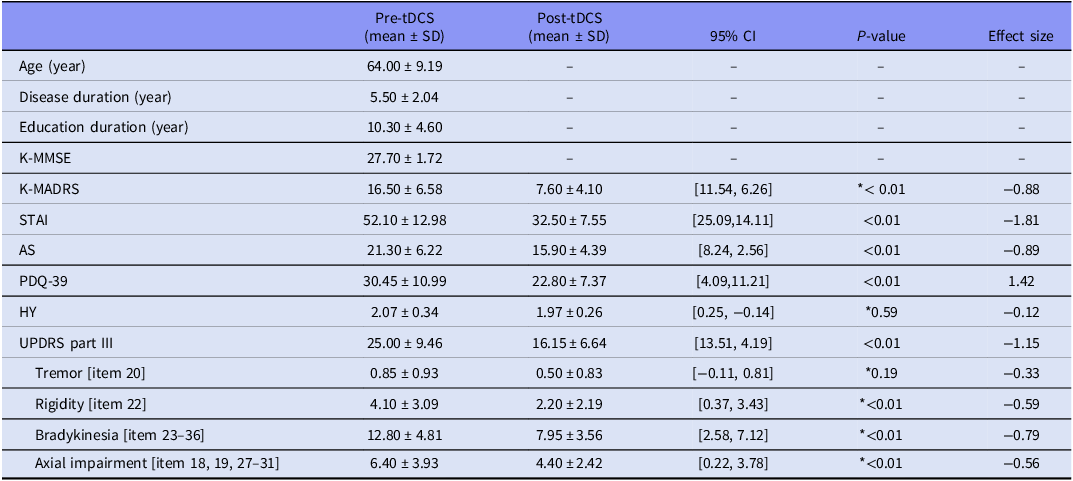
Twenty outpatients were enrolled and completed the study (Figure 1). The mean age of the sample was 64.00 years, with an average disease duration of 5.50 years. The mean duration of education at baseline was 10.30 years. Baseline clinical characteristics indicated mild-to-moderate depressive symptoms (K-MADRS: mean = 16.50, SD = 6.58), moderate anxiety levels (STAI: mean = 52.10, SD = 12.98), and moderate apathy (AS: mean = 21.30, SD = 6.22). The mean baseline UPDRS Part III score was 25.00 (Table 1). No adverse events by tDCS were reported during the study.
Descriptive statistics and analysis of clinical scales before and after treatment

P-values were calculated using either paired t-test or *Wilcoxon signed-rank test.
tDCS: transcranial direct current stimulation, SD: standard deviations, K-MADRS: Montgomery-Åsberg Depression Rating Scale, STAI: State–Trait Anxiety Inventory, AS: Apathy Scale, PDQ-39: Parkinson’s Disease Questionnaire-39items, UPDRS: Unified Parkinson’s Disease Rating Scale.
After the tDCS intervention, participants demonstrated significant improvements across all clinical assessments (Table 1). K-MADRS scores demonstrated a marked reduction (Wilcoxon signed-rank test, p < 0.01). STAI scores also decreased substantially (paired t-test, p < 0.01). AS scores were significantly lowered following the intervention (paired t-test, p < 0.01). PDQ-39 scores improved notably (paired t-test, p < 0.01), and UPDRS part III score improved significantly compared to baseline (paired t-test, p < 0.01). In addition to the UPDRS part III total score, we examined changes in the following UPDRS part III subscales: tremor (item 20), rigidity (item 22), bradykinesia (items 23–26), and axial impairment (items 18, 19, and 27–31). Significant improvements were observed in the UPDRS part III subscales of rigidity (Wilcoxon signed-rank test, p < 0.01), bradykinesia (Wilcoxon signed-rank test, p < 0.01), and axial impairment following tDCS (Wilcoxon signed-rank test, p < 0.01), whereas no significant change was detected in the tremor subscale (Wilcoxon signed-rank test, p = 0.19).
Comparing pre- and post-tDCS data from Xiaomi Mi Band 2.0, significant increases were observed in daily step count (p = 0.005). Although physical activity time tended to increase, this change did not reach statistical significance. Sleep time also showed increasing, but it was not significant (Table 2).
Comparison of smart band between before and after tDCS

P-values were calculated using Wilcoxon signed-rank test. *p < 0.01.
tDCS: transcranial direct current stimulation, SD: standard deviations, WASO: Wake after sleep onset.
Spearman’s rank correlation analysis was conducted to assess the relationships between changes in step count and changes in clinical scale scores. After setting the significance level at p < 0.01, a strong negative correlation was found between changes in step count and AS scores (rho = –0.73, 95% CI: –0.89 to –0.43, p < 0.001). Although negative correlations were also observed with K-MADRS (rho = –0.52, 95% CI: –0.78 to –0.10, p = 0.02), UPDRS part III (rho = –0.42, 95% CI: –0.72 to 0.04, p = 0.07), PDQ-39 (rho = –0.35, 95% CI: –0.71 to 0.07, p = 0.13), and STAI (rho = –0.35, 95% CI: -0.69 to 0.11, p = 0.13) scores, these did not reach statistical significance after correction.
To further verify the robustness of this relationship, a partial correlation analysis controlling for potential confounding variables, including age, years of education, disease duration, and baseline HY stage, was conducted. The negative correlation between changes in apathy and step count remained significant even after controlling for these factors, suggesting that the observed relationship was not attributable to demographic or disease-related covariates (rho = –0.76, p < 0.001).
Discussion
In this preliminary study, we aimed to investigate whether tDCS may be associated with changes not only in mood symptoms but also in physical activity levels in PD patients with accompanying depressive symptoms, using clinical scales and smart devices. When comparing pre- and post-tDCS assessments, significant changes were observed in K-MADRS, STAI, and AS scores. Comparing pre- and post-tDCS data from Xiaomi Mi Band 2.0, participants demonstrated significant improvements in the number of daily steps. However, only improvement in AS showed a significant correlation with increases in step count, and this relationship remained significant even after controlling for potential confounding factors such as age, education, disease duration, and baseline HY stage. This finding suggests that the reduction in apathy played a key role in enhancing physical activity levels following tDCS. Although both UPDRS part III and step count are measures of motor function and showed a negative correlation in our data, this association did not reach statistical significance and may be attributable to several factors. First, the small sample size and the use of Spearman’s rank correlation likely limited statistical power, reducing the ability to detect an existing association. Second, UPDRS part III captures multiple motor domains beyond gait, such as facial expression, finger tapping, rapid alternating hand movements, and resting tremor, so the total score only partially reflects gait-related performance, which can attenuate its correlation with step-based measures. Third, UPDRS part III is a clinician-rated scale that inherently incorporates rater subjectivity, and such measurement variability may further weaken its observable relationship with an objective metric such as step count.
Although tDCS has been primarily studied for its antidepressant effects (Bennabi & Haffen, Reference Bennabi and Haffen2018; Aktürk et al., Reference Aktürk, Agargün, Özdemir, Dalmizrak and Güntekin2025), our findings also suggest a potential benefit on apathy. Apathy commonly occurs across a wide spectrum of neurocognitive disorders (NCD), including PD (17–70%), frontotemporal dementia (50–100%), and Alzheimer’s disease (24–85%)(Lanctot et al., Reference Lanctot, Ismail, Bawa, Cummings, Husain, Mortby and Robert2023; Totuk & Sahin, Reference Totuk and Sahin2025). Although depression is also common among individuals with NCDs, research including patients with apathy without depression, and those with depression without apathy, provides clear evidence that these two syndromes are distinct (Marin et al., Reference Marin, Firinciogullari and Biedrzycki1994; Levy et al., Reference Levy, Cummings, Fairbanks, Masterman, Miller, Craig, Paulsen and Litvan1998; Landes et al., Reference Landes, Sperry and Strauss2005). Apathy is defined as a quantitative reduction of goal-directed activity in comparison to the patient’s previous level of in multiple dimensions including behaviour/cognition, emotion and social interaction (Fahed and Steffens, Reference Fahed and Steffens2021). Depression is typically characterised by negative emotions such as sadness and hopelessness. Investigators have reported that apathy – but not depression – is associated with aberrant motor behaviour and disinhibition, whereas depression – but not apathy – is associated with anxiety, agitation, irritability, and hallucinations (Levy et al., Reference Levy, Cummings, Fairbanks, Masterman, Miller, Craig, Paulsen and Litvan1998). A meta-analysis of 16 studies examining the relationship between behavioural and psychological symptoms of dementia and caregiver burden found that apathy ranked among the three most distressing symptoms, surpassed only by depression and agitation/aggression (Feast et al., Reference Feast, Moniz-Cook, Stoner, Charlesworth and Orrell2016). Therefore, an improvement in apathy may represent a particularly important therapeutic effect and underscores the significance of our results.
Early reviews drawing on data from individuals with various NCDs suggested that apathy arises from dysfunction within frontal–subcortical circuits (Cummings, Reference Cummings1998). Supporting this, reductions in grey matter density in medial frontal regions and across several prefrontal areas have been linked to different dimensions of apathy, including the DLPFC (involved in generating cognitive plans or goals for action), the dorsomedial prefrontal cortex (involved in self-initiated actions), and the orbito-ventromedial prefrontal cortex (involved in emotional evaluation) (van Dyck et al., Reference van Dyck, Arnsten, Padala, Brawman-Mintzer, Lerner, Porsteinsson, Scherer, Levey, Herrmann, Jamil, Mintzer, Lanctôt and Rosenberg2021). Furthermore, magnetic resonance imaging studies have shown reduced integrity of frontal white matter in patients with apathy, likely contributing to disruptions in frontal–subcortical pathways (Starkstein et al., Reference Starkstein, Mizrahi, Capizzano, Acion, Brockman and Power2009). Given that apathy is closely linked to frontal network dysfunction, prefrontal tDCS may modulate fronto–subcortical circuitry in PD. Such neuromodulatory effects could contribute to motor improvement directly via enhanced fronto–basal ganglia connectivity. Alternatively, increased goal-directed behaviour and motivation following tDCS may have indirectly increased daily step counts by promoting greater engagement in everyday activities.
Although numerous medications have been approved for the treatment of depression, no drugs are currently indicated for apathy, leaving a significant unmet clinical need. The American Psychiatric Association recommends a trial of antidepressants for patients with dementia who exhibit clinically significant depressed mood, with selective serotonin reuptake inhibitors (SSRIs) preferred over other classes of antidepressants (Rabins et al., Reference Rabins, Blacker, Rovner, Rummans, Schneider, Tariot, Blass, McIntyre, Charles and Anzia2007). However, a cross-sectional, retrospective study of 125 patients found that individuals treated with SSRIs had significantly higher AS scores compared with those not receiving SSRIs (Padala et al., Reference Padala, Padala, Majagi, Garner, Dennis and Sullivan2020b). As pharmacological options remain limited, noninvasive brain stimulation techniques – particularly transcranial magnetic stimulation (TMS) and tDCS – are receiving increasing attention as potential therapeutic approaches. These modalities are hypothesised to enhance neuroplasticity in brain regions implicated in apathy and depression. One study examining repetitive TMS applied to the left DLPFC demonstrated improvements in apathy and cognition among patients with AD, suggesting that this effect may reflect enhanced dopaminergic transmission resulting from rTMS targeting the DLPFC (Padala et al., Reference Padala, Boozer, Lensing, Parkes, Hunter, Dennis, Caceda and Padala2020a).
The UPDRS is a widely used tool in clinical and research settings for evaluating the progression and severity of PD. We also used UPDRS part III of the UPDRS for assessment of motor function. UPDRS part III includes various items such as speech, facial expression, tremor at rest, action or postural tremor, rigidity, finger tapping, hand movements, rapid alternating movements, leg agility, arising from chair, posture and gait. These items are scored based on the severity of symptoms observed during the examination. Despite its broad use, the UPDRS has important limitation. Administration can be time-consuming, and performance on several items may depend on contextual and task-related factors that vary across assessments, such as the available walking space, the complexity of instructions given to the participant, and the participant’s physical exertion or fatigue, which may even prevent completion of the full examination (Piro et al., Reference Piro, Piro, Kassubek and Blechschmidt-Trapp2016). In addition, although structured training and standardised instructions are intended to reduce rater-related variability, UPDRS scoring remains partly subjective; different observers may interpret the same behaviours differently based on their prior experience, expectations, or implicit assumptions (Movement Disorder Society Task Force on Rating Scales for Parkinson’s, 2003). Such rater-related variability can introduce measurement error and reduce the validity and comparability of ratings across visits or assessors (Cohen et al., Reference Cohen, Manion, Morrison, Cohen, Manion and Morrison2017).
Consistent with this concern, previous work has suggested that UPDRS change scores can contain substantial error variance, further emphasising the need for more reliable and objective outcome measures (Evers et al., Reference Evers, Krijthe, Meinders, Bloem and Heskes2019). Wearable smart devices may help address several of these limitations by enabling objective, standardised, and longitudinal measurement of activity and sleep in naturalistic settings, thereby reducing reliance on rater-dependent scoring (Channa et al., Reference Channa, Popescu and Ciobanu2020). Real-time data collection by smart devices may allow healthcare professionals to assess the progression of motor symptoms and tailor treatment plans accordingly (Vijayan et al., Reference Vijayan, Connolly, Condell, McKelvey and Gardiner2021). Continuous, real-world data capture can complement clinic-based assessments by providing sensitive markers of symptom fluctuations over time, potentially supporting treatment optimisation and individualised care (Concheiro-Moscoso et al., Reference Concheiro-Moscoso, Groba, Martínez-Martínez, Miranda-Duro Mía del, Nieto-Riveiro, Pousada and Pereira2022). In addition to motor monitoring, smart devices can quantify daily activity levels and sleep patterns, which are highly relevant to functional outcomes and quality of life in PD, and may inform tailored exercise programmes and sleep-hygiene interventions (Espay et al., Reference Espay, Bonato, Nahab, Maetzler, Dean, Klucken, Eskofier, Merola, Horak and Lang2016). Beyond passive monitoring, these technologies may also support patient self-management by providing feedback, reinforcing lifestyle recommendations, and delivering educational content that promotes engagement and autonomy (Cho and Lee, Reference Cho and Lee2021; Yeom et al., Reference Yeom, Lee, Kim, Park, Cho, Kim, Lee and Lee2025). Nevertheless, several challenges remain for the widespread adoption of smart devices in PD, including data privacy, user acceptance, and device- or algorithm-related limitations. Future research should systematically address these issues and further validate wearable-derived outcomes to ensure their reliability, clinical interpretability, and utility across diverse PD populations.
This study has several limitations. Firstly, we did not include a control group using sham tools in this experiment, making it uncertain whether the results of this study are influenced by a placebo effect. In future experiments, adding a control group is necessary to confirm this. Secondly, it is unclear whether the effects of tDCS are temporary or persist for a certain duration. It would have been beneficial to continue the action of the smart device even after the treatment and verify the data after a specific period or conduct a follow-up scale assessment on patients after a certain period. Thirdly, the small sample size makes it difficult to generalise the results. Given the small sample size, the confidence intervals around our main estimates were relatively wide, indicating limited precision. Fourthly, since there is no established tDCS protocol for PD treatment, we used a tDCS protocol designed for depression treatment. If our target region was different or the number of treatment sessions was higher, the results obtained might have been different. Furthermore, the potential for a bidirectional relationship between motor symptoms and depression in PD should be considered. Depression in PD is known to be heterogeneous; it can be a primary disease manifestation or a secondary reaction to motor-related functional limitations. In our study, both motor scores and mood scores improved concurrently in the medication ‘ON’ state. This suggests that the observed mood elevation might have been partially influenced by the improvement in motor function. However, because our tDCS protocol specifically targeted the DLPFC, a key node in emotional regulation circuits, the results likely reflect a direct modulation of mood-related pathways as well. Future studies are needed to further differentiate whether tDCS acts primarily on the neurobiological substrates of depression or indirectly via motor enhancement to better clarify its therapeutic mechanisms in heterogeneous PD populations.
Our study investigated the application of tDCS in PD as an alternative therapeutic approach. Our primary therapeutic target was the mood domain, whereas motor outcomes were treated as downstream, exploratory endpoints that might be modulated indirectly via mood-related pathways. We categorised and analysed findings related to the impact of tDCS on both mood and motor symptoms of PD. Our findings suggest that sequential bilateral DLPFC tDCS improves depressive symptom, apathy, and quality of life in patients with PD. It also enhances real-world physical activity as captured through smart band monitoring. Notably, improvements in apathy emerged as the strongest predictor of increased daily step counts, even after adjusting for demographic and clinical variables, highlighting apathy as a central therapeutic target. These results support the possibility that tDCS may modulate frontal–subcortical circuits to facilitate goal-directed behaviour and activity engagement. Furthermore, the integration of tDCS with objective, wearable-based monitoring offers a valuable complementary approach to traditional clinical assessments, providing more ecologically valid insight into treatment-related behavioural changes.
Data availability statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
This work was supported by a grant from Korea University and by the Korea National Institute of Health research project (2024-ER1002-01)
Author contribution
Conceptualisation: Ho-Kyoung Yoon, Do-Young Kwon. Formal analysis: Boram Chae. Funding acquisition: Ho-Kyoung Yoon, Do-Young Kwon. Investigation: Boram Chae. Methodology: Ho-Kyoung Yoon, Do-Young Kwon. Project administration: Ho-Kyoung Yoon, Do-Young Kwon. Resources: Do-Young Kwon. Supervision: Ho-Kyoung Yoon, Do-Young Kwon. Software: Boram Chae, Jae-ha Song. Validation: Ho-Kyoung Yoon, Do-Young Kwon. Visualisation: Boram Chae, Jae-ha Song. Writing – original draft: Boram Chae. Writing – review and editing: Boram Chae, Ho-Kyoung Yoon.
Funding statement
This research received no specific grant from any funding agency, commercial, or not for-profit sectors.
Competing interests
None.
Ethical standards
All participants received detailed information regarding the study objectives, procedures, potential risks, and their right to withdraw at any time without penalty. Written informed consent was obtained from all participants (or their legal guardians, where applicable) prior to enrolment. This study was conducted in accordance with ethical guidelines and was approved by the Institutional Review Board of Korea University Medical Center, Ansan Hospital, Gyeonggi-do, Korea. The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.


 Open access
Open access