

Alcohol and drug use are highly prevalent and problematic among youth worldwide 1,2 and have long-term health and societal consequences. Reference Odgers, Caspi, Nagin, Piquero, Slutske and Milne3,Reference King, Meehan, Trim and Chassin4 The World Health Organization has identified alcohol use as one of its top health concerns. 5 Evidence-based early prevention strategies targeting risk factors are therefore essential. Several risk factors associated with substance use problems are found in childhood disruptive behaviours (i.e. aggression, opposition, hyperactivity). Reference Mâsse and Tremblay6–Reference Pardini, White and Stouthamer-Loeber10 The robust link between disruptive behaviours and substance use has also been supported by a few experimental studies showing that childhood interventions designed to prevent disruptive behaviour problems have beneficial effects on substance use behaviours, at least in early and middle adolescence. Reference Dishion, Nelson and Kavanagh11–Reference Tremblay, Masse, Pagani, Vitaro, Peters and McMahon16 Unfortunately, none of these studies have addressed the mechanisms or factors by which these interventions have produced beneficial effects, but research has shown that understanding the key mechanisms involved is the cornerstone for devising effective prevention. Reference Brown and Liao17
In theory, the link between disruptive behaviours and substance misuse is thought to arise from a person-environment interplay, in which biological, personality, family, peer and/or other environmental variables relate causally to involvement in problem behaviours including alcohol and drug use. Substance use is therefore conceived as one heterotypic outcome of a disruptive pattern of behaviour, which usually begins in childhood, and can be exacerbated by poor socialisation. There are several models that support this view. The behavioural dysregulation model, Reference Tarter, Kirisci, Mezzich, Cornelius, Pajer and Vanyukov18 based on psychobiological theory of human behaviour, emphasises genetic liability and intra-individual factors such as impulsivity and a general proneness to disruptive behaviours to explain a host of maladaptive outcomes, including substance misuse and antisocial behaviours. According to this model, the mechanism through which substance use could be reduced or prevented should be through a reduction in antisocial behaviours and/or in impulse-control problems. In complement, the social deviance model, Reference Jessor, Turbin, Costa, Dong, Zhang and Wang19 emphasises the role of poor socialisation and environmental factors such as parental, school and peer influence. According to this second perspective, the mechanisms though which substance use and other problem behaviours could be reduced or prevented should be through socialisation skills by, for example, improving parental supervision, school engagement and reducing the affiliation with deviant peers.
The Montreal Longitudinal and Experimental Study (MILES) of low socioeconomic status boys Reference Mâsse and Tremblay6,Reference Lacourse, Nagin, Vitaro, Cote, Arseneault and Tremblay20 was initiated in 1984 and included a randomised prevention programme delivered over a 2-year period when boys were aged 7–9 years. The programme targeted disruptive behaviours and included two main components: social skills training for the boys at school and training for parents during family visits. This prevention programme has been shown to have short- and long-term effects on disruptive, antisocial and delinquent behaviours, Reference Tremblay, Pagani-Kurtz, Masse, Vitaro and Pihl21–Reference Vitaro, Brendgen, Pagani, Tremblay and McDuff23 identified as the study's primary outcomes, as well as academic performance and drop out from school. Reference Tremblay, Pagani-Kurtz, Masse, Vitaro and Pihl21,Reference Vitaro, Brendgen and Tremblay24 However, no study has evaluated the long-term effects of this prevention programme on substance use behaviours across adolescence, as well as the contribution of key intra-individual and environmental risk factors that may potentially explain these effects. Thus, the aims of the present study were to conduct a secondary analyses and examine the long-term intervention effects on adolescent substance use and whether these effects are explained by a reduction of risk factors targeted by the intervention, in accordance with either the behavioural dysregulation or the social deviance models.
Method
Participants
The 172 boys who participated in this study were a subsample of the MLES. In the spring of 1984, 1037 boys attending the last year of kindergarten (mean age: 6.1 years) were recruited from schools in low socioeconomic neighbourhoods of Montreal, Quebec. For further information on recruitment and selection criteria, please see Vitaro et al Reference Vitaro, Brendgen and Tremblay24 and Tremblay et al. Reference Tremblay, Pihl, Vitaro and Dobkin25 Gender (boys), ethnicity (White) and socioeconomic status were homogeneous as a result of the selection procedure. This study was approved by the University of Montreal Institutional Review Board, with participation in the study requiring both parental consent and child assent.
Selection of subsample
From the original sample, those who received scores above the seventieth percentile on the teacher-rated disruptiveness scale (n = 250) of the Pre-school Behavior Questionnaire (PBQ) Reference Behar and Stringfield26 in kindergarten were classified as disruptive and designated as at-risk for conduct disorder (Fig. 1). These 250 boys were then randomly assigned according to a 1:1:2 randomisation scheme to one of three groups (intervention group, n = 69; no-treatment control group, n = 60; and intensive observation group, n = 121 Reference Lavigueur, Saucier and Tremblay27 ) by drawing the names from a box until the necessary numbers were obtained. Of these, 23, 18 and 37 parents from each of these groups, respectively, refused to take any further part in the study. Thus, of the 172 participants included for analysis in the current study, 46 boys and their parents took part in the intervention, 42 were assigned as controls and 84 were assigned to an intensive observation group. Boys included in analyses did not differ significantly from those who refused to participate on any of the variables implemented in this study. The intensive observation group differed from controls in that every 2 years
Study profile.
PBQ, Pre-school Behavior Questionnaire.
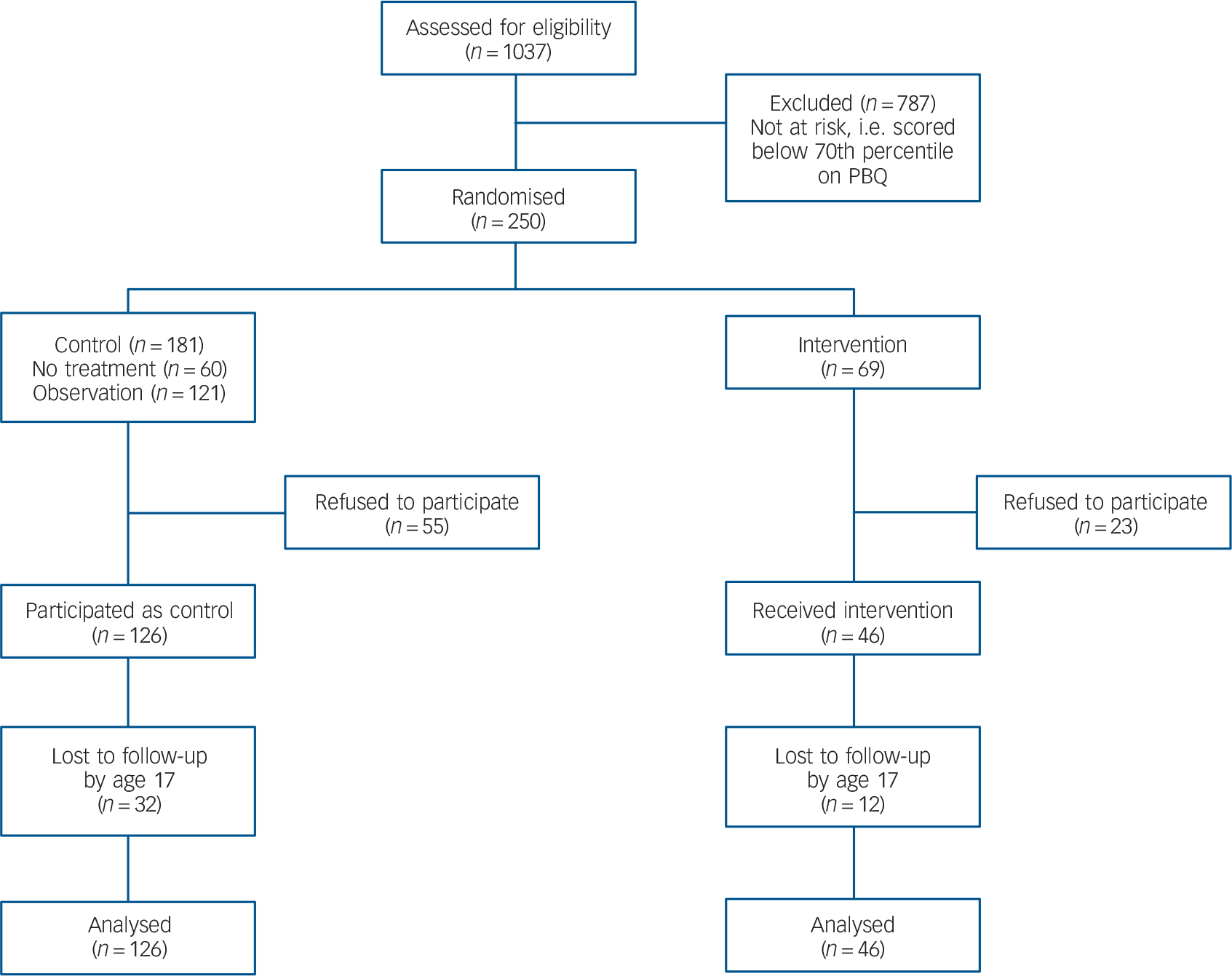
the families in this group were visited in their homes by researchers (four visits over four evenings per family), came to the university for a day-long laboratory-based testing session, and the boys were observed at school for half a day. Because previous studies have shown that there were no significant differences between the control and intensive observation groups on any of the pre- and post-test variables, Reference Vitaro, Brendgen and Tremblay24 these two groups were combined for analysis in the current study. Sample size was calculated to detect small to moderate effects on disruptive behaviours. The enrolment of participants was done independently from their randomisation. After the end of the preventive intervention programme, boys were followed annually from 10 to 17 years. Research workers involved in follow-up were masked to intervention conditions.
Intervention
The intervention was implemented over 2 school years, from September 1985 to June 1987, when boys were 7–9 years of age. The first component of the intervention, social and problem-solving skills training, aimed to promote healthy peer relations. It also aimed to promote self-control and consequently reduce impulsivity and antisocial behaviour. Boys took part in training sessions at their schools in small groups of four to seven children. These groups of children generally had a ratio of three to four prosocial children to one disruptive child, with a ratio of five to two in groups of seven. The sessions were conducted by four trained professionals (one psychologist, one social worker and two psychoeducators), lasted about 45 min each, and included verbal instructions, positive reinforcement, behaviour modelling and rehearsal. The professionals who delivered the training sessions for boys also offered to meet twice with each teacher to monitor the child's progress in the classroom and help the teacher set up reinforcement contingencies to support practice of the learnt skills in the classroom. However, this was implemented in only half of the classrooms with a target child because half of the teachers refused to participate in this part of the programme.
The second component, training for parents, was based on the Oregon Social Learning Center Model. Reference Patterson, Reid, Jones and Conger28 Those sessions were conducted at the parents' homes by a different professional from the one who worked with the children. It included teaching parents to recognise problematic and appropriate behaviours in their boys, to set clear objectives for them and reinforce appropriate behaviours. Parents were also encouraged to supervise their children's schoolwork and behaviour outside the home.
Implementation assessment
To evaluate programme implementation, the therapist responsible for each child-family-teacher unit indicated at the end of each training session the percentage of content that had been delivered in the session. More than 85% of the participating boys attended at least two-thirds of the social skills training sessions. In total 75% of the parents covered a minimum of two-thirds of the content and objectives of the planned training programme, with a mean of 17.4 sessions given to parents over the 2-year programme, including parents (14 of them) who discontinued their participation in the programme (the maximum number of sessions was 46). Boys from families who discontinued their participation in parental training were still included in analyses. Meetings with teachers were few (i.e. about 50% of teachers participated in at least one meeting). Consequently, less than half of the teachers implemented a behaviour management plan in their classroom. Social skills training sessions were videotaped and parent sessions were audiotaped; these tapes were used for weekly feedback and to maintain integrity and standardisation of the programme across therapists.
Measures
Outcomes
Two dimensions of substance use across adolescence were assessed annually from ages 14 to 17 years using the Self-Reported Antisociality Questionnaire (SRAQ): Reference LeBlanc and Frechette29 (a) alcohol use frequency, combining measures of the frequency of alcohol use and drunkenness (each rated on four-point scales, never to very often; Cronbach's alpha (2 items each year) α = 0.70, 0.81, 0.84, 0.79 respectively); (b) number of drugs tried, computed by summing nine dichotomous items assessing whether any of the following drugs were used in the past 12 months: cannabis, hallucinogens, cocaine, amphetamines, barbiturates, tranquilisers, heroin, inhalants and other drugs. Although not all were normally distributed (skewness ranged from 0.27 to 1.87, and kurtosis ranged from 0.13 to 2.87), outcome variables possessed acceptable levels of skewness and kurtosis for the use of maximum likelihood estimation (i.e. below 2 and 7 respectively Reference Curran, West and Finch30 ).
Pre-adolescent factors (potential explanatory mechanisms)
Post-intervention antisocial behaviour was assessed yearly at 11, 12 and 13 years with the SRAQ Reference Patterson, Reid, Jones and Conger28 . Participants indicated how frequently they had engaged in delinquent behaviours (one, never to four, often) over the past 12 months. Items included behaviours related to vandalism (five items, such as ‘intentionally destroyed someone's property’), interpersonal violence (five items, such as ‘beat someone up for no reason’) and theft (seven items, for example ‘stole 100 dollars or more’). Responses were summed to create a yearly total antisocial behaviour score (α = 0.90, 0.92, and 0.90 respectively), and these scores were averaged across 11–13 years (mean intraclass correlations (ICC) = 0.69).
Teacher- and mother-rated impulsivity was assessed at ages 11, 12 and 13 years using items from the Social Behavior Questionnaire. Reference Tremblay, Loeber, Gagnon, Charlebois, Larivee and LeBlanc31 At age 11, teachers and mothers were asked on a three-point scale (never, sometimes, often) whether the child was: (a) restless, runs about, jumps up and down; and (b) squirmy or fidgety. At ages 12 and 13, five more items were added to include other aspects of impulsivity: (a) jumps from one activity to another; (b) is irritable and loses his temper easily; (c) attracts attention by shouting; (d) has trouble sitting still; (e) acts without thinking. Reliability was good for the two items at 11 years (α = 0.85 and α = 0.82 for teacher and mother ratings respectively) and the seven items at 12 and 13 years (α = 0.89 for teacher and α = 0.82 for mother ratings at both time points). These six scale scores were summed combining both informants to create a total impulsivity score at ages 11–13 years (α = 0.76). Both teacher (ICC = 0.63) and mother ratings (ICC = 0.82) demonstrated acceptable stability across the three time points, and measures across raters were significantly correlated at each time point (correlations ranged from 0.30 at 11 years to 0.41 at 13 years).
Parental perceived supervision was assessed annually, when boys were aged 11–13 years, using two items: ‘Do your parents know where you are when you go out?’ and ‘Do your parents know who you hang around with?’ (responses ranged from one, never to four, always). These items were summed across all time points, with higher scores indicating greater perceived supervision (for the six items α = 0.75, ICC = 0.65 across the three time points).
School engagement was measured annually between 11 and 13 years with two self-report items: ‘How important is it for you to get good grades?’ and ‘How much effort do you put in your schoolwork?’ rated on a four-point scale (not important at all to very important, α = 0.62 for six items across 11–13 years; stability (ICC) across time was 0.64).
Affiliation with deviant peers was rated annually by the boys when they were aged 11–13 years by asking: (a) whether they were part of a group or a gang that carried out reprehensible acts; and (b) how many of their friends were arrested by or got into trouble with the police (both in the past 12 months). This last question was rated on a four-point scale (zero, none to three, nearly all). These two items were summed across 11–13 years (α = 0.75; stability (ICC) was 0.71 across the three time points).
Covariates
The boys' pre-intervention disruptive behaviour, which assesses aggression (three items), oppositional behaviour (five items), and hyperactivity (two items) in kindergarten (at age 6, α = 0.93) was included as a covariate in all analyses. A verbal IQ Reference Veroff, McClelland and Marquis32 estimate at 13 years as well as a measure of family adversity at 6 years were also included as covariates in all analyses. The measure of family adversity includes information on family status (intact or not), both parents' educational level, occupational prestige, and their age at the birth of their first child. For each item, a score of one was given to those below the thirtieth percentile of the complete sample, and a score of zero was given to those above the thirtieth percentile (an intact family status was given a score of zero), with higher scores indicating greater adversity.
Analysis
Analyses were carried out with latent growth curve and path analyses using Mplus version 5.21 on Windows. Reference Muthén and Muthén33 Maximum likelihood with robust standard errors (MLR) estimation was used in all analyses. Full information maximum likelihood (FIML) was used to account for missing data. The maximum amount of missing data at any time point was 26% (at 17 years), with equivalent numbers of attrition across intervention condition by the end of follow-up (Table 1). Attrition was not predicted by any covariates (pre-intervention disruptive behaviour, verbal IQ and family adversity; all P>0.29), alcohol use (P = 0.84) or numbers of drugs (P = 0.82) at 14 years.
Tests of goodness of model fit included the comparative fit index (CFI), the Tucker-Lewis index (TLI), the root mean square error of approximation (RMSEA) and the standardised root mean square residual (SRMR). Traditionally, CFI and TLI >0.90 and RMSEA and SRMR ≤0.08 are considered as indicative of acceptable fit, whereas CFI and TLI ≥0.95 and RMSEA and SRMR ≤0.05 are considered as indicative of good fit.
Three stages of analyses were conducted. First, latent-growth curve models (LGCM) examined change, separately, in substance use frequency and number of drugs tried. The LGCMs were modelled with the intercept centred at the first time point (14 years), giving an indication of early-onset alcohol use and drug experimentation. Second, these growth models were combined together with covariates and intervention status to test whether the intervention was associated with the average level of initiation and change in these outcomes across adolescence (conditional multivariate growth model). Cohen's d was used to assess effect size for significant intervention effects. Values of 0.80 or higher, 0.50 and 0.20 or lower represent a large, medium and small effect respectively. Finally, this was followed by mediation analyses, in which indirect effects through potential mediators (pre-adolescent factors) were tested. Significance of indirect effects was tested using the product of coefficients method. Reference MacKinnon, Lockwood and Williams34 The product of coefficients of paths implicated in an indirect effect (for example intervention to impulsivity (path a) and impulsivity to alcohol use slope (path b)) are labelled ‘ab’ in the text. Asymmetric confidence intervals were calculated using the Prodclin.sps programme, Reference MacKinnon, Fritz, Williams and Lockwood35 with an alpha of 0.05.
Results
Table 1 shows that baseline measures (at age 6) and verbal IQ were comparable across intervention conditions, but P-values were less than 0.25 for two of these measures, indicating non-perfect equivalence across groups. Table 1 also shows the means of outcome measures by intervention conditions. Simple means comparisons showed that there were significant differences
Baseline measures, verbal IQ, attrition and outcomes by intervention condition

| Control group | Intervention group | Control group, n |
Intervention group, n |
t-test/χ2 | P | |
|---|---|---|---|---|---|---|
| Disruptiveness at 6, mean (s.d.) | 14.24 (4.71) | 15.28 (4.43) | 126 | 46 | 1.31 | 0.096 |
| Family adversity at 6, mean (s.d.) | 0.40 (0.23) | 0.42 (0.25) | 126 | 46 | 0.47 | 0.329 |
| Verbal IQ at 13, mean (s.d.) | 8.46 (2.29) | 9.05 (2.24) | 126 | 46 | 1.38 | 0.085 |
| Attrition by 17, n (%) | 32 (25) | 12 (26) | 126 | 46 | 0.14 | 0.422 |
| Outcomes | ||||||
| Alcohol use frequency, mean (s.d.) | ||||||
| At 14 | 3.60 (1.57) | 3.15 (1.55) | 105 | 38 | 1.81 | 0.036 |
| At 15 | 3.97 (1.84) | 3.47 (1.74) | 103 | 36 | 1.70 | 0.046 |
| At 16 | 4.49 (1.90) | 3.94 (1.97) | 98 | 36 | 1.63 | 0.053 |
| At 17 | 4.73 (1.83) | 4.73 (1.92) | 94 | 36 | 0.10 | 0.460 |
| Number of drugs tried, mean (s.d.) | ||||||
| At 14 | 1.30 (0.68) | 1.44 (0.95) | 105 | 38 | 1.01 | 0.157 |
| At 15 | 1.53 (0.92) | 1.44 (1.11) | 103 | 36 | 0.40 | 0.345 |
| At 16 | 1.96 (1.53) | 1.41 (0.91) | 98 | 36 | 2.96 | 0.002 |
| At 17 | 2.09 (1.69) | 1.80 (1.39) | 94 | 36 | 1.97 | 0.025 |
between the two groups for alcohol use frequency across all time points, except at 17 years, and for numbers of drugs used at 16 and 17 years.
Zero-order correlations between all variables showed the intervention was associated with all pre-adolescent factors (mediators; see online Table DS1). In turn, these variables were significantly associated with most substance use outcomes, qualifying them as putative mediators. Thus, all hypothesised mediating and control variables were retained in subsequent structural equation modelling analyses.
Unconditional growth models
A linear growth function provided a good fit for the alcohol use frequency data (χ2 = 4.84, d.f. = 5, CFI = 1.00, TLI = 1.00, RMSEA = 0.00, SRMR = 0.05) and for the number of drugs data (χ2 = 3.53; d.f. = 5; CFI = 1.00; TLI = 1.00; RMSEA = 0.00; SRMR = 0.04). Growth curve factor means (alcohol use frequency: intercept 3.538, slope 0.445; drugs used: intercept 1.335, slope 0.239) were all significantly different from zero at P<0.001 and showed that there was an overall tendency for alcohol use frequency and number of drugs used to increase from 14 to 17 years. The growth curve factor variances were also significant at P<0.01 (alcohol use frequency: intercept 1.913, slope 0.112; drugs used: intercept 0.389, slope 0.147), indicating that there was significant individual variability in the mean level of alcohol use and drugs used at 14 years and their pattern of change over time. Correlations between the latent factors showed that alcohol use at age 14 years (intercept) correlated significantly, and negatively, with an increase in alcohol use between 14 and 17 years (slope, r = −0.35, P<0.01), indicating that lower or less frequent alcohol use at 14 years was associated with larger increases in substance use frequency later in adolescence. Correlations between the latent factors showed that drugs tried at age 14 years (intercept) did not correlate significantly with a linear increase (slope, r = 0.19, P = 0.58) of drugs tried across adolescence.
Conditional multivariate growth models
Main effects of the intervention
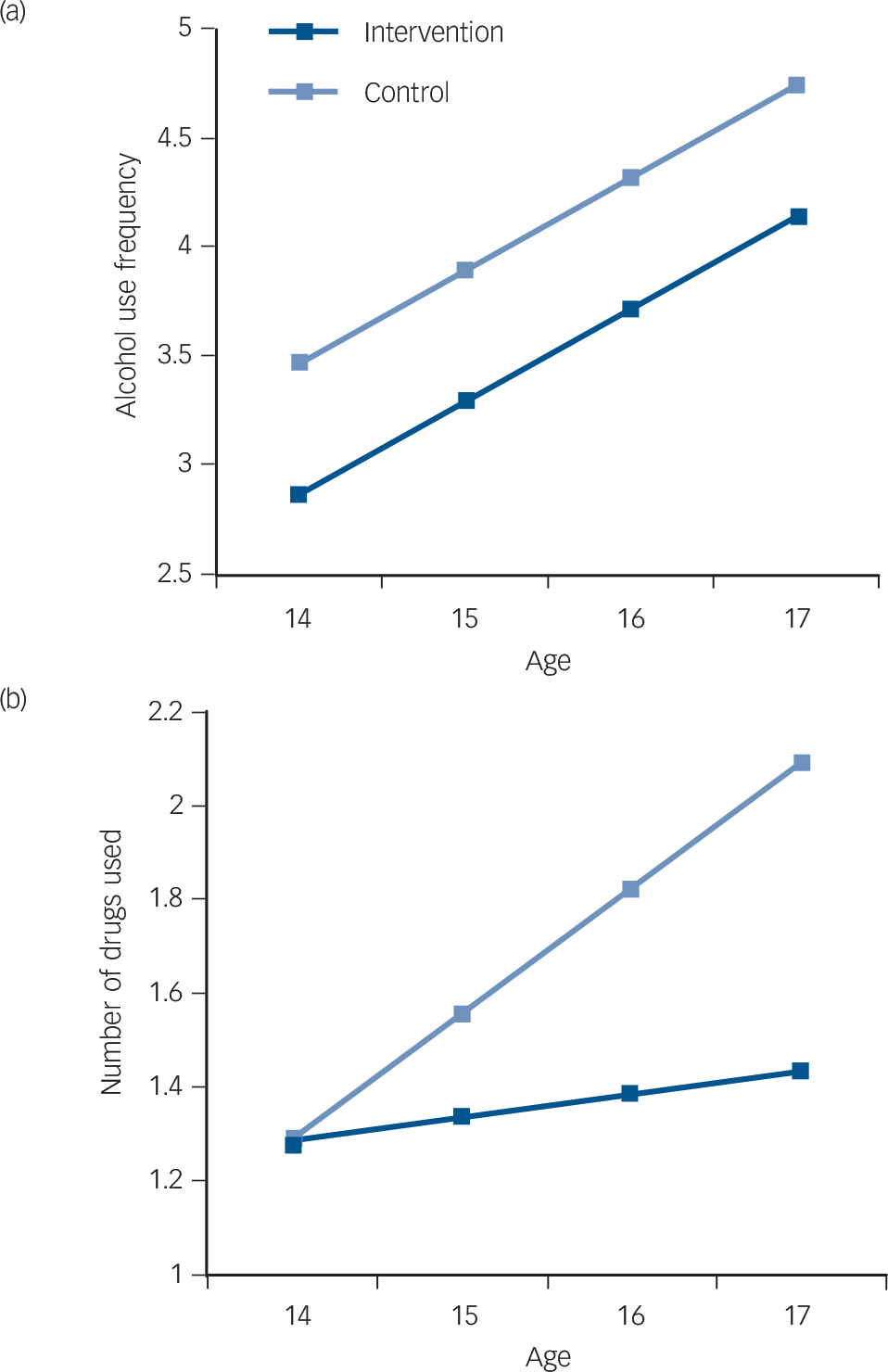
To examine the effects of participation in the intervention on alcohol use frequency and number of drugs tried across adolescence, intervention status, together with covariates (family adversity, pre-intervention disruptiveness and verbal IQ), were included in a model with both unconditional growth models described above. This model fitted the data well: χ2(34) = 37.72, CFI = 0.99, TLI = 0.99, RMSEA = 0.02, SRMR = 0.04. Results, included in Table 2 (model 1), showed that the intervention was associated with lower alcohol use frequency at 14 years (intercept: d = 0.48), but was not significantly associated with growth in alcohol use frequency from 14 to 17 years (slope). This is equivalent to a main intervention effect but no intervention time interaction, with the intervention group's alcohol use frequency remaining constantly lower than that of the control group's across adolescence (Fig. 2(a)). Additionally, only verbal IQ predicted alcohol use frequency at 14 years (intercept: B = 0.014, s.e. = 0.007, β = 0.21, P = 0.043), suggesting that high verbal IQ was associated with early alcohol use, consistent with the hypothesis that cognitive abilities may assist reward-oriented behaviours, including substance use. Reference Hyman, Malenka and Nestler36 None of the covariates predicted growth in alcohol use across 14–17 years. Conversely, the intervention was not associated with lower number of drugs used at 14 years (intercept), but was significantly associated with a reduced increase in number of drugs used from 14 to 17 years (slope d = 0.70, Fig. 2(b)). None of the covariates significantly predicted number of drugs used at 14 years (intercept) or growth in this outcome from 14 to 17 years (slope).
Explaining intervention effects through the reduction of pre-adolescent risk factors
The final model examined whether the intervention effects on substance use outcomes were the result of reducing potential risk factors targeted by the intervention. Thus, post-intervention antisocial behaviour, impulsivity, parental supervision, school engagement and affiliation with deviant peers were added to the previous model. This model fit the data well: χ2(55) = 58.32, CFI = 1.00, TLI = 0.99, RMSEA = 0.02, SRMR = 0.04. Table 2 (model 2), Table 3 and Fig. 3 show all significant paths for this model, including significant indirect effects. As expected, the intervention was associated with a reduction of self-reported antisocial behaviour (d = 0.43), lower teacher-rated impulsivity (d = 0.41), improved parental supervision (d = 0.38), higher school engagement (d = 0.58) and an affiliation with less deviant peers (d = 0.53). With the inclusion of these factors, the main effect of the intervention on alcohol use frequency at 14 years and growth in number of drugs used from 14 to 17 years were no longer significant, and were reduced by 47% and 50% respectively. Examination of indirect effects (Table 3) showed that lower levels of post-intervention antisocial behaviour (ab = −0.028, 95% CI
Main effects on substance use behavioursFootnote a

| Alcohol use frequency | Number of drugs tried | |||||||
|---|---|---|---|---|---|---|---|---|
| Intercept at 14 years | Slope, 14-17 years | Intercept at 14 years | Slope, 14-17 years | |||||
| B (s.e) | β | B (s.e) | B | B (s.e) | β | B (s.e) | B | |
| Model 1 | ||||||||
| Intervention | –0.077 (0.031) | –0.21Footnote * | 0.012 (0.012) | 0.11 | 0.001 (0.034) | 0.00 | –0.038 (0.015) | –0.31Footnote ** |
| Model 2 | ||||||||
| Intervention | –0.041 (0.029) | –0.11 | 0.007 (0.013) | 0.07 | 0.028 (0.031) | 0.09 | –0.019 (0.015) | –0.16 |
| Antisocial behaviour | 0.700 (0.182) | 0.40Footnote *** | –0.145 (0.078) | –0.28 | 0.078 (0.166) | 0.06 | –0.036 (0.107) | –0.04 |
| Impulsivity | –0.002 (0.002) | –0.10 | 0.001 (0.001) | 0.15 | –0.003 (0.002) | –0.20 | 0.004 (0.001) | 0.59Footnote ** |
| Parental supervision | 0.002 (0.012) | 0.01 | 0.000 (0.005) | –0.02 | –0.022 (0.011) | –0.23Footnote * | 0.006 (0.006) | 0.16 |
| School engagement | 0.004 (0.011) | 0.04 | 0.001 (0.004) | 0.02 | 0.010 (0.009) | 0.12 | –0.002 (0.005) | –0.04 |
| Peer deviancy | 0.111 (0.054) | 0.22Footnote * | –0.006 (0.023) | –0.04 | 0.186 (0.054) | 0.44Footnote *** | 0.038 (0.035) | 0.22 |
a. Models included family adversity, mother's age at first birth, paternal occupational prestige, pre-intervention disruptiveness and verbal IQ as covariates. The intervention was significantly associated with post-intervention antisocial behaviour (B = −0.040, s.e. = 0.015, β = −0.19, P = 0.009), impulsivity (B = −3.218, s.e. = 1.595, β = −0.18, P = 0.044), parental supervision (B = 0.542, s.e. = 0.231, β = 0.17, P = 0.019), school engagement (B = 0.911, s.e. = 0.236, β = 0.26, P = 0.002) and peer deviancy (B = −0.167, s.e. = 0.043, β = −0.243, P<0.001). In these models, covariates and all variables assessed within the same developmental period (such as pre-adolescence and adolescence) were allowed to covary. Residuals for number of drugs used were associated with residuals for alcohol use frequency across adolescence: growth in number of drugs used (slope) did not correlate significantly with alcohol use frequency at 14 years (r = 0.47, P = 0.080), but did with growth in alcohol use frequency from 14 to 17 years (r = 0.53, P = 0.030); number of drugs used at 14 correlated with alcohol use frequency at 14 years (r = 0.67, P<0.001) but not with growth in alcohol use frequency from 14 to 17 years (r = −0.15, P = 0.403).
* P<0.05
** P<0.01
*** P<0.001.
(a) Alcohol use frequency and (b) numbers of drugs used by group.
–0.05694 to −0.00614) and affiliation with less deviant peers (ab = −0.018, 95% CI −0.04162 to −0.00077) explained the effect of the intervention in reducing alcohol use frequency at 14 years. Furthermore, impulsivity explained the effect of the intervention on growth of number of drugs used from 14 to 17 years (ab = −0.013, 95% CI −0.02896 to −0.00033).
Significant indirect effects on substance use behaviours

| Unstandardised coefficient (95% CI) | ||||
|---|---|---|---|---|
| Alcohol use frequency | Number of drugs tried | |||
| Intercept at 14 years | Slope, 14-17 years | Intercept at 14 years | Slope, 14-17 years | |
| Intercept→antisocial behaviour | –0.028 (–0.05694 to −0.00614) | - | - | - |
| Intercept→impulsivity | - | - | - | –0.013 (–0.02896 to −0.00033) |
| Intercept→parental supervision | - | - | –0.012 (–0.02996 to −0.00012) | - |
| Intercept→peer deviance | –0.018 (–0.04162 to −0.00077) | - | –0.031 (–0.05812 to −0.01038) | - |
Arrows indicate ‘indirect effect through’.
Significant direct and indirect effects of the intervention on substance use outcomes.
Alcohol, alcohol use frequency; Drugs, number of drugs used. Only standardised coefficients are shown. Although not shown in the figure, the model included family adversity, pre-intervention disruptiveness and verbal IQ as covariates. Covariates and all variables assessed within the same developmental period (such as pre-adolescence and adolescence) were allowed to covary. Double-line arrows indicate significant mediated effects: the effect of programme participation on alcohol use at 14 years (intercept) was mediated by adolescent's antisocial behaviours (ab = −0.028, 95% CI −0.05694 to −0.00614) and affiliation with deviant peers (ab = −0.018, 95% CI −0.04162 to −0.00077); the effect of programme participation on growth in number of drugs used from 14 to 17 years was mediated by impulsivity (ab = −0.013, 95% CI −0.02896 to −0.00033). Additional significant indirect, but not mediated, effects were found (indicated with broken double line arrows): programme participation on number of drugs used at 14 years (intercept) through affiliation with deviant peers (ab = −0.031, 95% CI −0.05812 to −0.01038) and poor parental supervision (ab = −0.012, 95% CI −0.02996 to −0.00012). *P<0.05, **P<0.01, ***P<0.001.

Discussion
This study shows that an intensive 2-year intervention aimed at key risk factors in disruptive kindergarten boys from low socioeconomic environments can effectively reduce substance use behaviours in adolescence, not only in early adolescence, but up to the end of high school, 8 years post-intervention. The effects shown are noteworthy, first because they are stronger and longer lasting than for most substance use interventions reported in the literature to date. Reference Tobler and Stratton37–Reference Conrod, Castellanos-Ryan and Strang39 For example, two meta-analyses Reference Tobler and Stratton37,Reference Faggiano, Vigna-Taglianti, Versino, Zambon, Borraccino and Lemma38 evaluating school-based universal prevention programmes concluded that the evidence in support of their effectiveness on substance use behaviours was limited. When significant effects were found, these were small and did not last much beyond the treatment period. Reference Tobler and Stratton37,Reference Faggiano, Vigna-Taglianti, Versino, Zambon, Borraccino and Lemma38 In contrast, the effects of selective and indicated prevention programmes, such as the one reported here, have been shown to be larger and longer lasting, Reference Dishion, Nelson and Kavanagh11–Reference Zonnevylle-Bender, Matthys, van de Wiel and Lochman15,Reference Conrod, Castellanos-Ryan and Strang39 but no study, until now, had examined these effects for more than 4 years post-intervention.
These findings are also noteworthy because the effects were obtained through targeting known risk factors and not substance use directly (no information on substance use was given to the boys) before the onset of substance use in children and in their same age peers. Accordingly, findings confirmed that the protective effects occurred through the reduction of key risk factors targeted by the intervention: (a) the effect of the childhood intervention on early-onset alcohol use was explained by a reduction of both antisocial behaviour and affiliation with deviant peers in pre-adolescence; and (b) the effect of the intervention on drug experimentation from 14 to 17 years was explained by a reduction of pre-adolescent impulsivity. We note that the intervention group's alcohol use frequency between 14 and 17 years remained constantly lower than that of the control group's across adolescence, although the intervention was not associated with a decrease in growth of alcohol use frequency.
The fact that pre-adolescent explanatory variables were associated with alcohol use frequency at age 14 years, and drug experimentation across time, but not associated with growth in alcohol use frequency could suggest that other unmeasured risk factors may explain growth in alcohol use frequency. Indeed, other important pathways to adolescent substance use have also been identified, particularly those relating to affect regulation (for example negative affect/hopelessness) and pharmacological vulnerability (for example sensation-seeking, see Castellanos-Ryan & Conrod Reference Castellanos-Ryan, Conrod, Verster, Brady, Galanter and Conrod40 for a review). However, the most parsimonious account for increasing alcohol use frequency across this period could simply be that of normative social processes (for example with age the opportunities to get involved with alcohol increase 1 ), rather than a particular risk pathway.
Although this study cannot address other potential pathways to substance use, findings provide support for both the behavioural dysregulation and the social deviance models, by showing the complementary roles individual and social risk factors play in early-onset alcohol use and substance use experimentation during adolescence. Our findings demonstrate that not only by reducing antisocial behaviours and/or impulsivity in pre-adolescence, but also by improving other social factors such as affiliation with less deviant peers, the progression from disruptiveness in childhood to substance use behaviours in adolescence can be significantly reduced.
Limitations
The main limitation of this study is that most of the data presented were gathered through self-report (except for teacher- and mother-rated impulsivity and intervention status), which is susceptible to bias and may limit the experimental validity of the data. That said, several studies have shown that self-reports are reliable when assessing substance use or other behavioural problems in adolescence, Reference Clark and Winters8,Reference Crowley, Mikulich, Ehlers, Whitmore and MacDonald41 and hence are useful for treatment and research. This, together with guaranteed confidentiality to participants, should increase confidence in these data. Finally, although it is noteworthy that such long-term effects were found in this high-risk sample of boys, further studies are needed to examine whether these effects can be generalised to girls and other populations.
Implications
Despite some limitations, this is the first study to show that an intervention targeting disruptive behaviours, impulsivity, parental supervision and affiliation with deviant peers can have lasting effects on substance use experimentation across adolescence. Moreover, the present study contributes to our knowledge of developmental pathways to substance use, by clarifying the explanatory pathways to substance use behaviour in adolescence. Most importantly, findings provide support for the growing body of literature showing the promise of selective prevention programmes in the prevention of substance use problems, and shows the benefit of targeting known early risk factors for substance use.
Funding
This research was made possible by fellowships to N.C.-R. from the Ministère de l'Éducation, du Loisir et du Sport du Québec (no. 149169) and the Fonds de la Recherche en Santé de Québec (no. 22530), grants from the Canadian Institutes of Health Research (no. MOP-97910), the Social Science and Humanities Research Council of Canada, the National Health Research and Development Program, the Fonds Québécois de Recherche sur la Société et la Culture, and the Fonds Québécois de Recherche en Santé.
Acknowledgements
The authors wish to thank the boys, their families and teachers for their long-term commitment to this project.








eLetters
No eLetters have been published for this article.