


Nocebo refers to a negative placebo; the nocebo effect describes a phenomenon in which negative expectations about treatments, symptoms or broader illness lead to adverse outcomes. Expectations arise through knowledge, conditioning, suggestion or modelling; these influence the autonomic nervous system and other neurobiological pathways, resulting in negative physical, emotional and behavioural consequences. The fact that the nocebo effect has been seen across different domains and procedures points to its universality. Its relevance therefore extends beyond medical settings to educational, digital and other social environments.
The social transmission of symptoms refers to the spread of subjective experiences and observable functional manifestations of illness among individuals in the absence of an underlying disease process or injury. The nocebo effect has been implicated in the social transmission of a variety of symptoms: nocebo-induced pain is the most researched, but it has also been demonstrated in the induction of low mood, itching, nausea and side-effects from vaccines and other medications. It leads to measurable physical consequences – for example, altered cardiorespiratory physiology and hyperalgesia linked to neurobiological changes.
This editorial argues that anxiety has a role in the emergence of the nocebo effect (anxiety as an input); the nocebo effect is relevant to mass psychogenic illness and other forms of socially transmitted illness; symptoms of anxiety are sometimes socially transmitted; and the nocebo effect potentially explains how socially informed negative expectations lead to the development and persistence of anxiety disorders (anxiety as an output). A theoretical model is used to explain the process. An important limitation of this paper is the breadth of the nocebo construct, which invites its application to a wide range of expectation-induced processes; future research on nocebo effects would benefit from the identification of which mechanisms apply in different contexts, thereby reducing the potential to overgeneralise.
The genesis of nocebo effects relates to anxiety in two ways: first, individuals with pre-existing anxiety disorders are more susceptible,Reference Colloca, Panaccione and Murphy1 and second, state anxiety contributes in many cases to the nocebo phenomenon. Experimental nocebo treatment has been shown to induce anticipatory anxiety (a form of state anxiety) and to increase autonomic arousal, with this then mediating the persistence of nocebo-induced hyperalgesia.Reference Colagiuri and Quinn2 Although nocebo effects sometimes arise in the absence of state anxiety, negative expectancy appears to play a much larger role than state anxiety in generating the nocebo effect.Reference Rooney, Sharpe, Todd, Richmond and Colagiuri3 Anxiety’s contribution may be to worsen expectations; this is the input role of anxiety in the nocebo effect.
Anxiety also plays a role in the genesis of mass psychogenic illness.Reference Halimi, Jarrahi, Kian, Nejadghaderi, Jorjani and Keramatinia4 This occurs when people have a plausible reason to become unwell – for example, a presumed gas leak, insect bite or proximity to people who have a virus – and the expectation that they will develop symptoms creates genuine but socially constructed symptoms; these then spread among a group of people, who are usually in close physical proximity to each other. The nocebo effect is an important mechanism in the spread of mass psychogenic illness: negative expectations arise from being near people displaying symptoms that are believed to have an organic cause, which themselves inform symptom development.
The nocebo effect has also been implicated in a wide range of syndromes and other conditions thought to have a socially transmissible element, including Havana syndrome, wind turbine syndrome and gluten sensitivity. A meta-analysis of gluten re-challenge trials, for example, found no significant difference in the risk of relapse between individuals consuming gluten and those consuming a placebo among patients diagnosed with non-coeliac gluten sensitivity. The analysis found a significant difference between these two groups when using stricter criteria, but a substantial proportion (24%) still relapsed after consuming the placebo.Reference Lionetti, Pulvirenti, Vallorani, Catassi, Verma and Gatti5 In these more chronic conditions, expectations may arise from personal experience; however, these are often culturally mediated through, for example, news reports or television documentaries.
Symptoms of anxiety also appear to be socially transmissible. Research controlling for the effects of genetics shows transmission of anxiety through family environments. Anxiety is also shared in friendships and other peer groups, sometimes as a result of homophily (choosing to associate with people who are similar) and sometimes as a result of social influence. Co-rumination, for example, is linked to the development of internalising problems such as anxiety. The nocebo effect may contribute to the social transmission of anxiety in a number of ways, originating from social environments that imply harm.
Mental health awareness efforts are common, due to well-intentioned ambitions to reduce stigma and encourage support-seeking. According to the prevalence inflation hypothesis, these awareness efforts create improved recognition of mental illness but they can also contribute to the over-interpretation of subclinical worries and sadness as mental health problems; and the attached labels become a self-fulfilling prophecy. Evidence has been found of potential harm from universal school-based mental health interventions that fits the prevalence inflation hypothesis.Reference Foulkes, Winterburn, Sandra, Inzlicht, Andrews and Guzman Holst6 This could represent a nocebo effect via socially informed expectations: adolescents who become more aware of mental illness form negative expectations that are made real through awareness of negative emotions, over-interpretation, rumination and related processes.
There are several other ways in which mental health awareness and broader cultural contexts can create expectations and concerns, and a sense of threat. Generic anxiety quizzes common to websites and social media capture enough of normal human experience (‘I find it hard to relax’ or ‘I get easily annoyed with people’), for example, that they may cause concern among individuals completing them that they suffer from anxiety. Creation of safe spaces risks the implication that other spaces or the people within them are not safe, leading to anticipation of harm away from them. Prevalent therapeutic language (the ‘wounded inner child’ and similar expressions) implies vulnerability and lack of resilience, potentially leading people to anticipate fragility in themselves. Ideas of potential harms also spread through symptom modelling: being in close proximity to people displaying clear anxiety symptoms can create negative expectations of poor functioning.
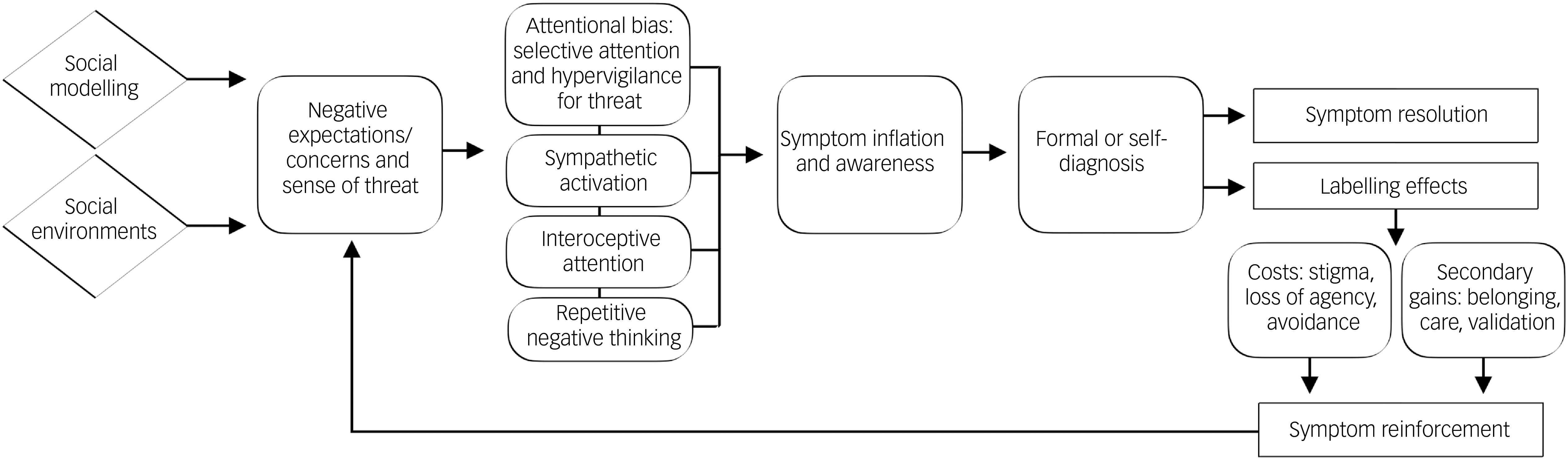
Figure 1 shows the theoretical model of nocebo mechanisms (negative expectations causing or exacerbating symptoms) in the social transmission of anxiety. In this model, socially informed negative expectations lead to threat-related attentional bias in the form of selective attention (focusing in on potential threats) and hypervigilance (horizon-scanning for threats). They also activate the sympathetic nervous system and lower parasympathetic activity. Threat increases interoceptive attention, and may make individuals falsely believe they are experiencing physical anxiety-related symptoms such as an increased heart rate. Repetitive negative thinking has been found to mediate the link between negative concerns and anxiety.
Theoretical model of nocebo mechanisms in the social transmission of anxiety.

Symptoms are activated and inflated through these processes. Anxiety is predicted by selective attention to threat, hypervigilance for threat, sympathetic nervous system activation, interoceptive processing and repetitive negative thinking. Once individuals are aware of symptoms, they diagnose themselves or seek formal diagnosis.
The resulting labels, such as generalised anxiety disorder, have a variety of negative and positive reinforcement effects. The resulting stigma can lead to more negative self-perception and worse treatment by others; labels can make some individuals believe they lack agency over their condition, further undermining well-being; and having an anxiety diagnosis makes some individuals avoid situations that cause them anxiety, resulting in symptom persistence or progression. Positive reinforcement mechanisms include secondary gains, such as a sense of belonging, care and attention from others, and symptom validation.
These labelling effects reinforce symptoms, which result in further negative expectations or concerns and a sense of threat, creating ongoing feedback loops. Digital amplification is another potential mechanism in symptom reinforcement. There may even be a role for nocebo-related anxiety cascades: as already mentioned, people with pre-existing anxiety disorders are more susceptible to the nocebo effect, which has the potential to sustain or worsen their anxiety in future.
Should the social transmission of anxiety via the nocebo effect be demonstrated empirically, it will be important to recognise that not everybody will be affected in this way. Some people who develop anxiety through socially transmitted negative expectations will no doubt quickly achieve symptom resolution through formal treatment, support and care from friends and family, self-management or the natural passage of time.
Empirical validation would also entail practice-related considerations. One such consideration is nocebo education, which holds early promise for mitigating some of the impact of the nocebo effect. Experimental evidence shows that nocebo education can reduce expectations of medication side-effects;Reference Spotts and Geers7 reduce nocebo effects from exposure to infrasound, which is believed by campaigners to contribute to wind turbine syndrome;Reference Crichton and Petrie8 and reduce false self-diagnosis of attention-deficit hyperactivity disorder.Reference Sandra, Segal, Majoo, Sistanis, Burke and Inzlicht9 It is feasible that widespread education about the nocebo effect could reduce negative expectations in regard to social modelling of anxiety and social environments that contribute to a sense of threat; and that nocebo education could help patients diagnosed with anxiety disorders to understand how such expectations may be contributing to reinforcement of their symptoms. Other clinical considerations include positive framing of outcomes and supporting patients to develop a recovery mindset.
Anxiety is often recognised as an input to the nocebo effect, but it has not yet been properly assessed as an output from it. The theoretical framework proposed here suggests that, while state anxiety can contribute to nocebo mechanisms, the nocebo effect itself can lead to clinical anxiety, making anxiety both input and output. The social transmission of anxiety via the nocebo effect has a number of clinical implications.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Declaration of interest
None.

eLetters
No eLetters have been published for this article.