
Ultrasound is the most commonly used medical imaging method in pregnancy. In the United Kingdom, all pregnant patients are routinely offered ultrasound examinations at around 12 weeks and 20 weeks of gestation. However, the use of ultrasound prior to 12 weeks has become central to the management of patients with suspected early pregnancy problems. In particular, earlier ultrasound examinations are indicated after assisted conception and for those in whom an ectopic pregnancy or miscarriage is suspected.
The aims of an early pregnancy ultrasound scan (USS) are to confirm the presence of a normally sited pregnancy, establish viability, determine number of embryos, determine gestational age and to reassure about the absence of complications.
Setting
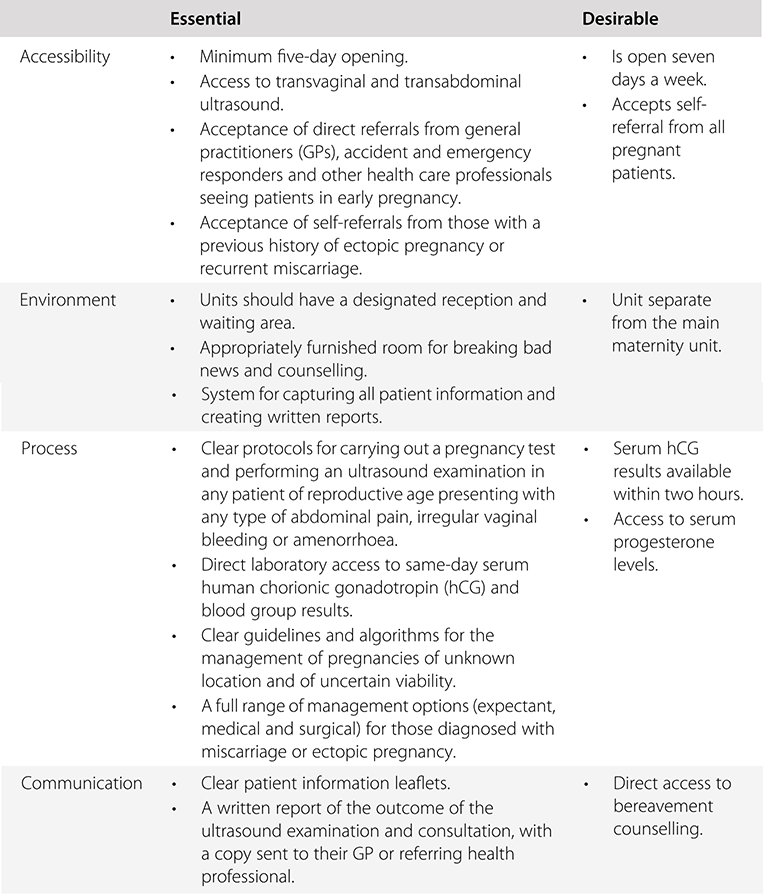
In the United Kingdom, the majority of early pregnancy ultrasound examinations are carried out in Early Pregnancy Units. These are specialist units for the provision of care for those with suspected early pregnancy complications. It is a recommendation of the Royal College of Obstetricians and Gynaecologists that all maternity units should have such a unit. Table 1.1 summarises some of the standards that should be expected in an Early Pregnancy Unit.

Safety
In recent years, there has been much interest in the safety of early ultrasound examinations. The evidence so far suggests that ultrasound used for clinical reasons with standard presets during embryonic development (conception to 10 weeks’ gestation) is safe and the benefits outweigh any theoretical risks. It is, however, essential that whoever is carrying out the ultrasound examination is aware of the safety indices and scanning modes. A fundamental approach to the safe use of diagnostic ultrasound is to use the lowest output power and the shortest scan time consistent with acquiring the required diagnostic information. This is referred to as the ALARA (‘as low as reasonably achievable’) principle.
Safety Indices
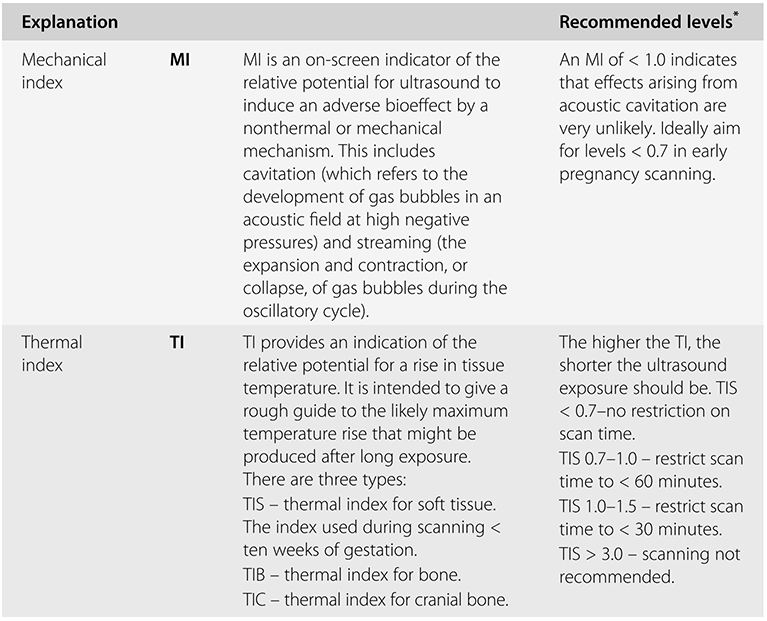
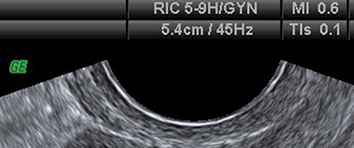
Ultrasound examination of the developing embryo or fetus exposes it to both mechanical and thermal stress. The potential effects of these forms of stress are represented by the mechanical index (MI) and thermal index (TI) respectively. These two indices are summarised in Table 1.2. They are displayed on the ultrasound screen during the examination, as shown in Figure 1.1.
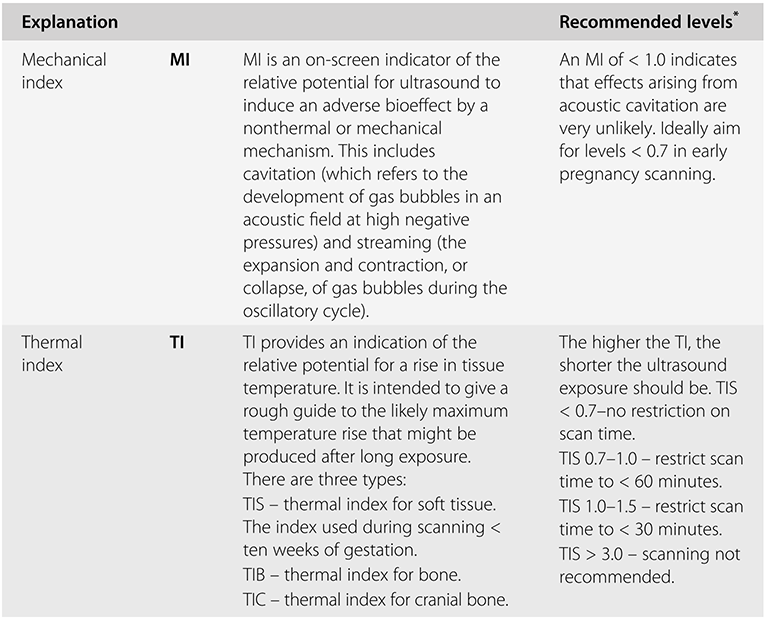
* Recommended by the British Medical Ultrasound Society.
Image showing on-screen display of mechanical index (MI) and thermal index (TI).
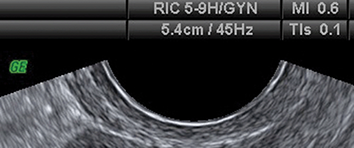
Figure 1.1 Long description
The ultrasound scan view depicts a cross-section of pelvic structures. At the top, the on-screen display provides technical settings including R I C 5-9 H G Y N, mechanical index 0.6, depth 5.4 centimetres, frequency 45 hertz, and thermal index s 0.1.
Scanning Modes
Evidence suggests that the most commonly used B-Mode ultrasound is safe in early pregnancy when using standard obstetric presets on modern machines. Colour Doppler and pulsed wave Doppler involve greater average intensity and power outputs as shown by higher TIS (TI soft tissue) levels compared to B-Mode imaging. There is therefore a greater risk to the developing fetus of overheating. If Doppler ultrasound is used in early pregnancy, the operator should aim to keep the TIS < 1.0 and limit the scan exposure time. Currently it is not recommended that Doppler be routinely used in early pregnancy ultrasound assessments. The M-Mode is a low-energy alternative to pulsed wave Doppler, which can be used to insonate the embryonic heart if required in early pregnancy.
There is no current evidence that three-dimensional (3D) ultrasound leads to higher ultrasound exposure than two-dimensional (2D) examinations. In fact, scanning and exposure times may actually be reduced, as the data set can be analysed offline. The routine use of 3D examinations, however, is also not routinely recommended.
Scanning Route
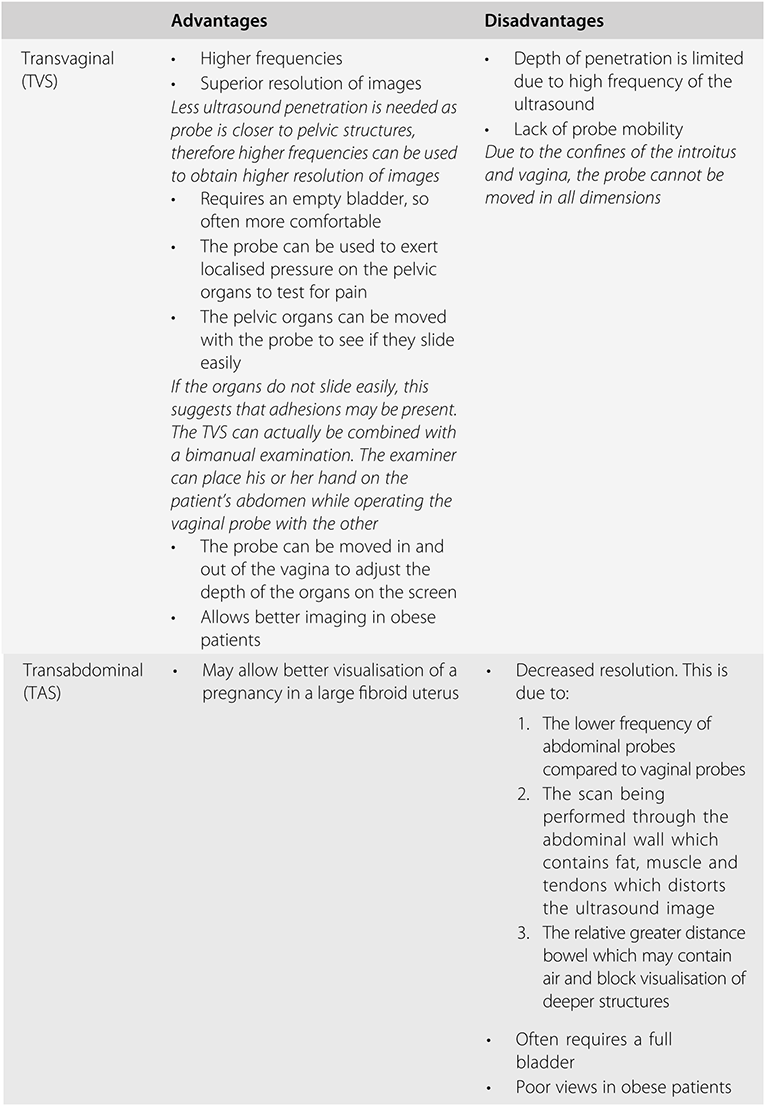
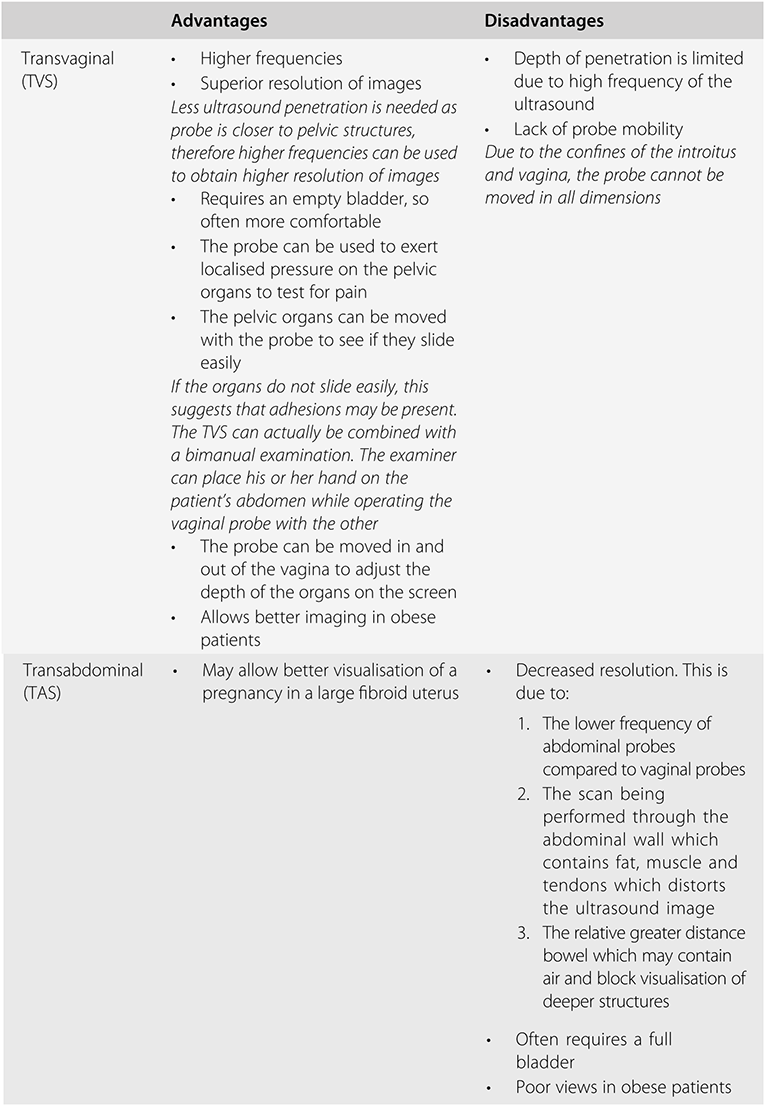
There are a number of advantages of the transvaginal route over the transabdominal route in early pregnancy, as indicated in Table 1.3. There is plenty of evidence in the literature suggesting that in the early first trimester a transvaginal scan (TVS) can reliably identify normal and abnormal pregnancies and various developmental markers at an earlier stage than a transabdominal scan (TAS). A TVS has been shown to be acceptable to patients attending Early Pregnancy Units and in fact some do actually prefer it to a TAS. The reasons for this include the discomfort and time needed to fill the bladder to adequately examine the pelvis abdominally. Transvaginal scans are also superior in obese patients and those with a retroverted uterus.
Occasionally it may be necessary to perform a transrectal ultrasound scan. This may be used as an alternative to a TVS if either a TVS is not possible and insufficient information is obtained by a TAS.
Ultrasound Technique
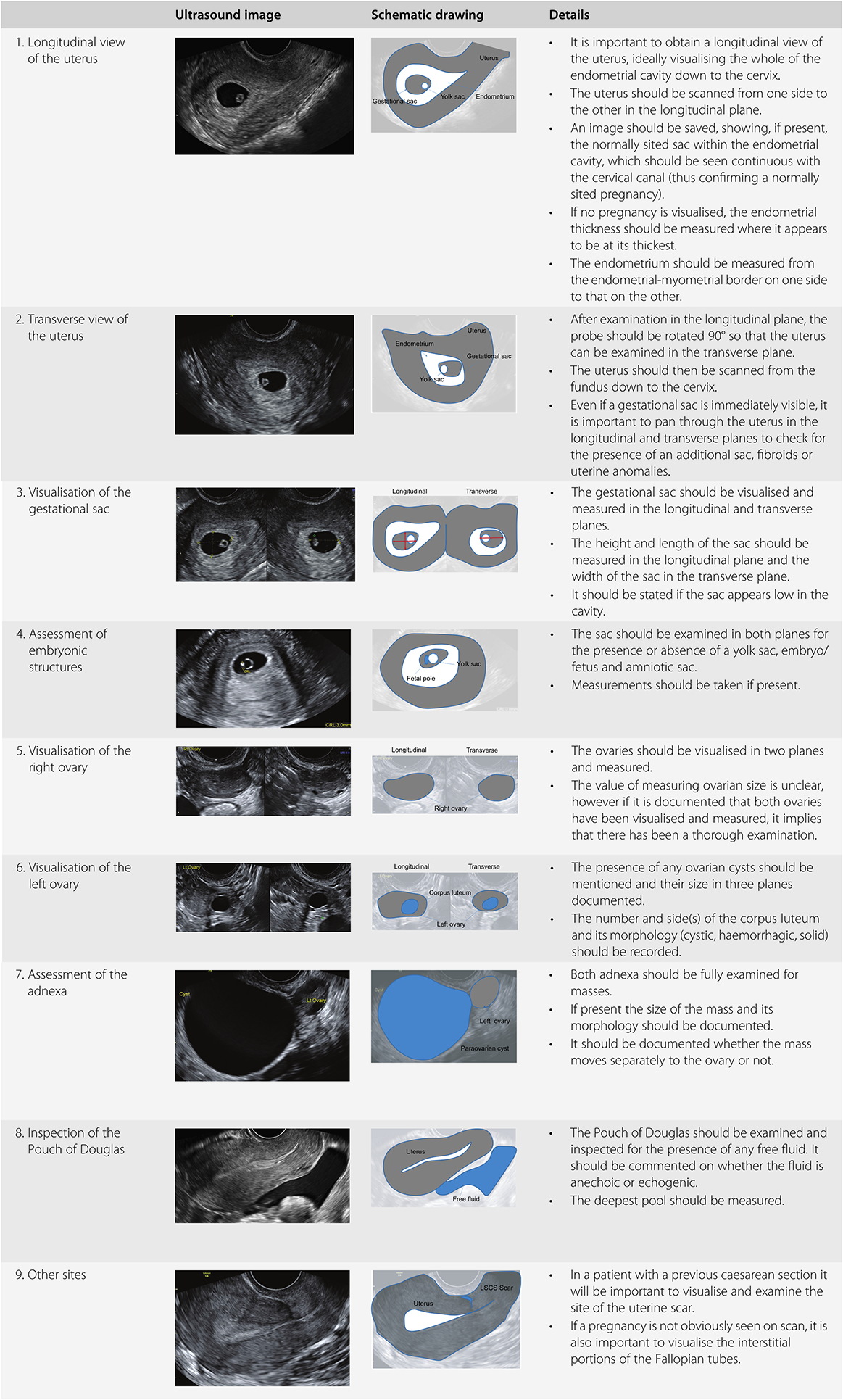
Whether performing a TVS or TAS, it is essential that the examination is performed in a systematic fashion and the image is optimised to enable the examiner to get the most information from the procedure.
Image Orientation
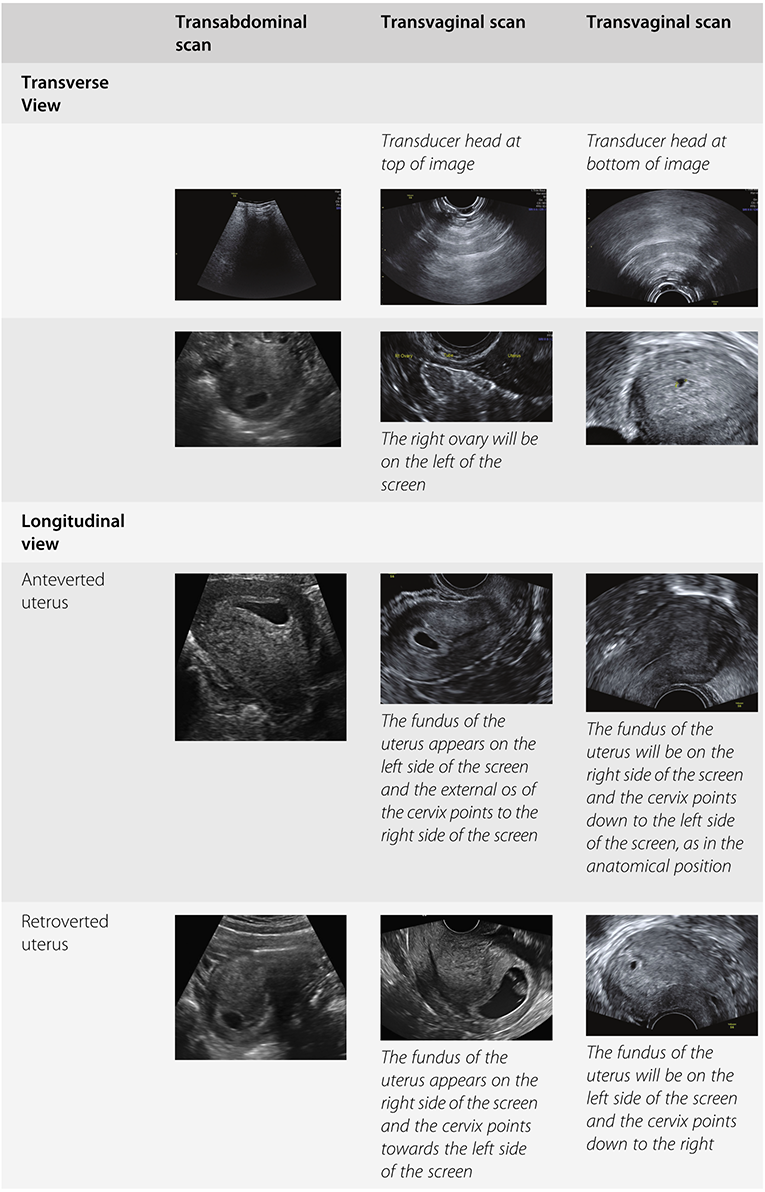
There is a general agreement that when in transverse section, the patient’s right side should be seen on the left side of the ultrasound screen. With a TAS, in the longitudinal view the cranial structures should be seen on the left side of the screen and the caudal structures on the right side. Superficial structures should be seen on the top half of the screen and deeper structures on the bottom half, as indicated in Table 1.4.
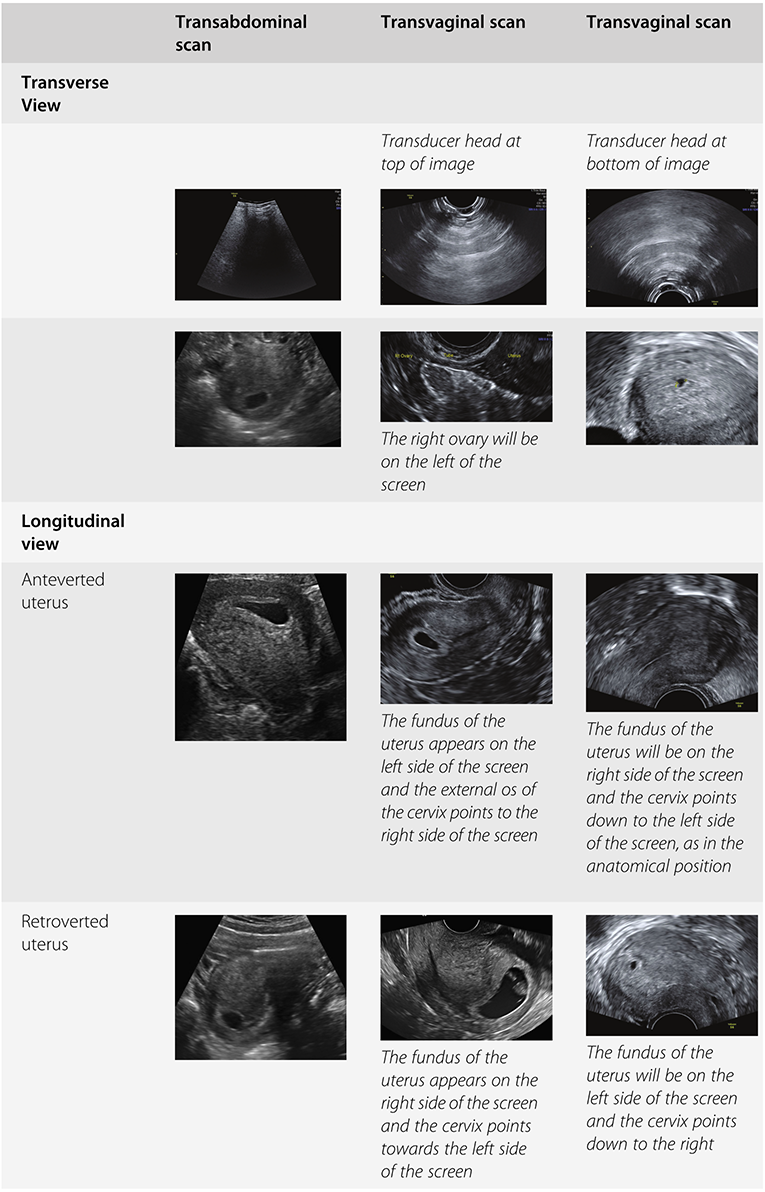
With TVS, there is no agreement on image orientation. Some scan with the transducer head in the upper part of the screen and some with it at the bottom.
Similarly, when examining in the longitudinal plane, some will have the bladder on the left and some will have it on the right, as indicated in Table 1.4. The most important thing is that the examiner is aware of his or her own orientation when performing the ultrasound examination.
Image Optimisation
Whilst most modern ultrasound machines are now programmed with suggested presets for the examination type intended in order to obtain the best images, there are still some things that usually need to be changed during every examination.
Depth
Usually the examination is started using high depth or a low magnification. Increasing the depth allows deeper structures to be viewed. Reducing the depth allows more superficial structures to be viewed.
Magnification
For superficial structures it is usually easiest to magnify the image by reducing the depth of the image. For deeper structures or to get an even bigger image, the zoom function can be used. This zoom function just takes a portion of the screen and magnifies it. It can be used whilst scanning or whilst the image is frozen.
Focus
The focus can be adjusted to manipulate the pulse of the ultrasound to be at its narrowest at a particular depth. This means that the image quality is maximised at this level. It allows the best lateral resolution (the ability to see two things as two things) to be achieved.
Gain
The overall brightness of the image can be adjusted by altering the gain. This is usually one of the most important changes to make to optimise the image, as if the image is too light or too dark, it is difficult to see subtle changes in texture.
The ultrasound waves change and get smaller as they pass through tissues (attenuation). In order to make structures look the same even if they are located in different depths, the time gain compensation (TGC) can be adjusted. Usually there is lower gain superficially and higher gain deeper in the image where the image quality is weaker.
Frequency
The highest ultrasound frequency possible should be chosen. However, the higher the frequency, the lower the depth of penetration. Therefore, if the object of interest is situated far away from the transducer, the frequency may need to be reduced to get the best image. A disadvantage of the lower frequency, however, is a reduction in the image resolution.
Transvaginal Scan
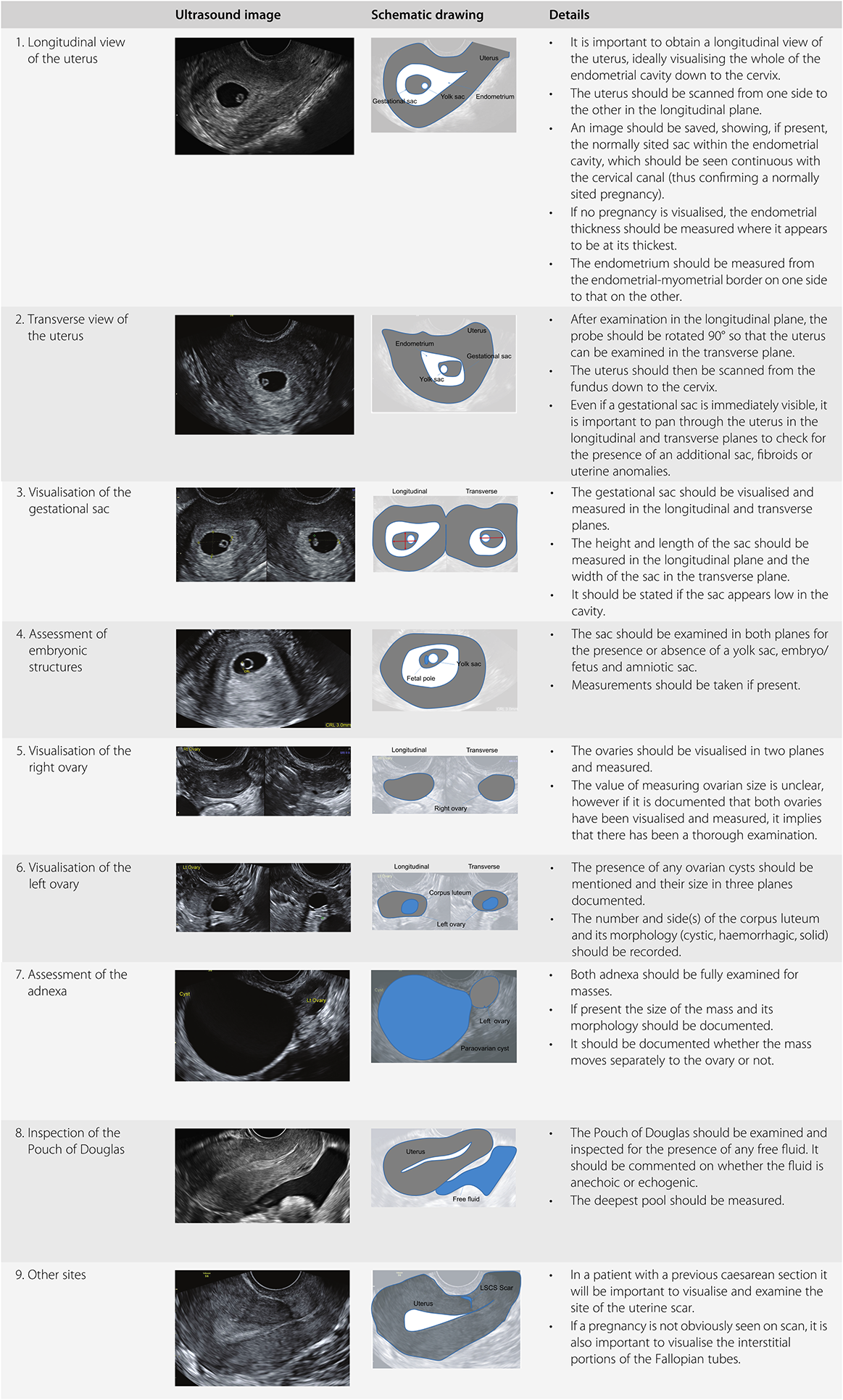
A TVS should be performed when the patient has an empty bladder. The procedure should be explained to the patient and consent taken. The probe should be thoroughly cleaned and disinfected before the procedure. An automated decontamination system is best practice; however, where this is not possible, manufacturer-approved wipes or cleaning systems should be used. The probe should be covered with a protective sheath. There should be a layer of ultrasound gel between the transducer head and the probe cover, with all air expelled. Extra lubricating gel should then be put on the covered probe. The operator should introduce the probe slowly into the vagina whilst watching the screen. It is sometimes helpful to ask the woman to take a deep breath at this point. The scan should then be performed in a systematic manner. A suggested method of doing this is shown in Table 1.5. After the examination is completed, the probe should be removed from the vagina, the probe cover removed and the probe cleaned.
If a transrectal scan is performed, the same examination technique should be used as for a TVS.
Transabdominal Scan
A TAS should be performed when the patient has a full bladder. A full bladder displaces the bowel and allows the ultrasound beam to travel through the urine until it reaches the uterus and ovaries. Again, it should be performed in the same systematic way suggested for TVS (see Table 1.5).
Documentation and Storage of Images
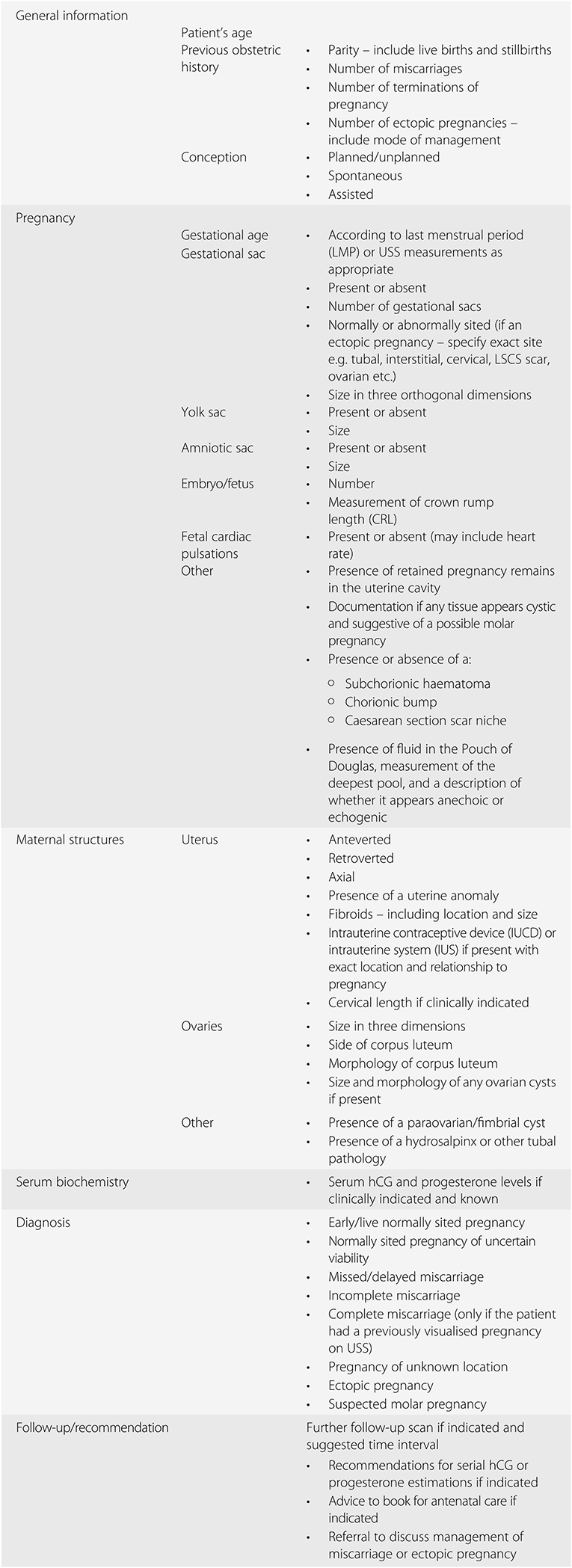
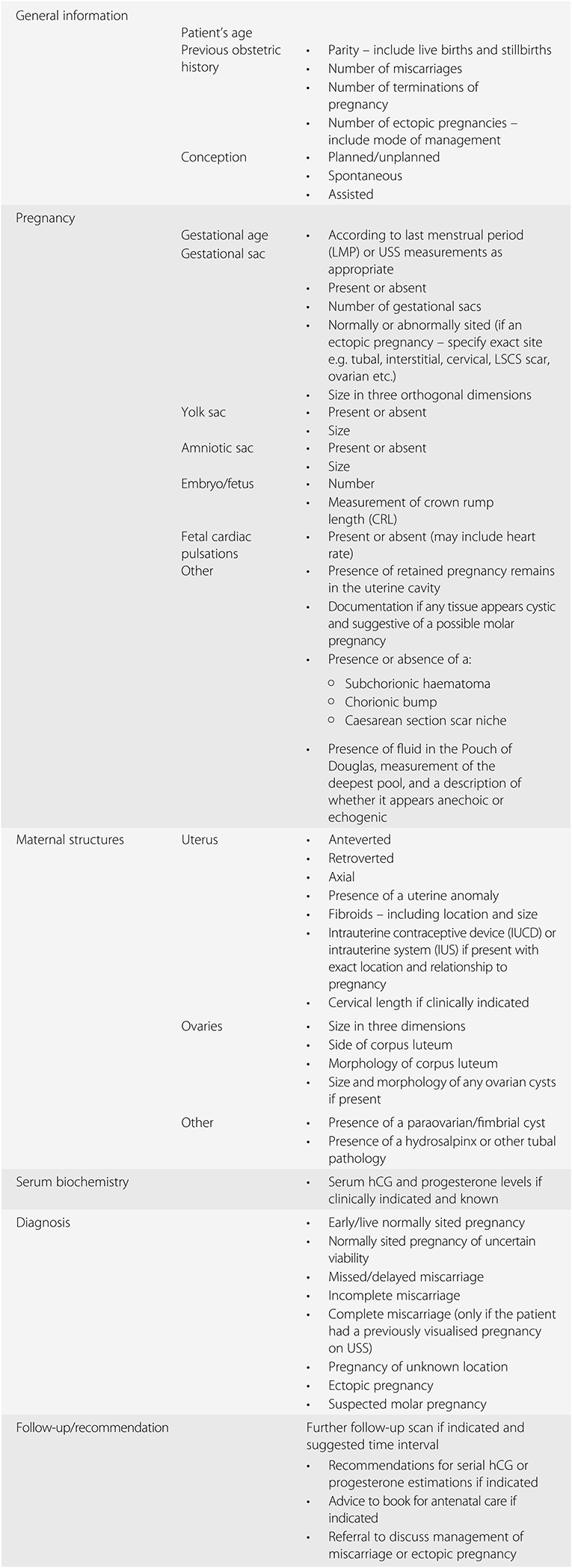
It is important to carefully document all findings in a systematic fashion when providing a report of the ultrasound examination. Suggested information to include in a report is given in Table 1.6. It is also important to store copies of the USS images taken. When writing the report and storing images, it is important to document all findings and to label all images taken and stored.
Specialist computer programs are available that allow the storage of USS images and offer the ability to generate a structured report as soon as the examination is complete. As all reports and images are saved under a patient’s particular identification number, all previous scan images and reports can be reviewed easily. This is extremely useful when a patient is returning for a follow-up scan after a previous inconclusive scan. Normal values for USS measurements such as gestational sac size and crown rump length (CRL) are contained within the programs, allowing them to assist with pregnancy dating. Another advantage of such a program is that they can enable a clinic to run efficiently by becoming paperless. However, the most important thing is that they allow a patient to leave the clinic with a written report in her hand.
Auditable Standards
It is good practice for all those performing ultrasound examinations in early pregnancy to attend regular departmental meetings to review guidelines and protocols and discuss difficult cases. Regular audits should also be performed on the rates of pregnancy of unknown locations and number of ectopic pregnancies diagnosed on ultrasound prior to treatment.
Learning Points
The aims of an early pregnancy ultrasound scan are to confirm pregnancy location, establish viability, determine number of embryos and determine gestational age.
Ideally all those with suspected complications should be seen in a dedicated Early Pregnancy Assessment Unit.
Ultrasound used with standard presets for clinical reasons during embryonic development (conception to 10 weeks’ gestation) is safe and the benefits outweigh any theoretical risks.
A transvaginal scan has a number of advantages over a transabdominal scan in early pregnancy.
It is essential to provide a structured written report of the ultrasound scan examination findings.