



Impact statement
Mental health stigma is characterized by prejudice, negative stereotypes and discriminatory behavior toward people with mental illness, and it remains highly prevalent and widespread across different cultures and communities. This study aimed to examine factors associated with stigmatizing attitudes of mental health professionals in Kazakhstan toward people with mental illness. Kazakhstan is the largest upper-middle-income country in the Central Asian region, which has long been ranked among the highest for suicide rates globally. Despite the widespread prevalence of mental health stigma throughout Central Asia, there is a lack of studies on this important topic, and no prior studies have examined mental health stigma among healthcare specialists. Our study has the potential to make a significant impact by shedding light on the Kazakhstani mental health professionals’ outlook toward mental illness, and informing policymakers, educators and healthcare leaders on where to focus training and awareness efforts in order to improve quality and accessibility of care, and treatment outcomes. A cross-sectional online survey was conducted among psychiatrists, narcologists, mental health nurses and psychiatry residents from all regions of Kazakhstan. The study findings highlight the persistence of stigma among mental health professionals in Kazakhstan, with overall stigma levels higher than those reported in previous studies. Key findings indicate that older professionals, those working in the drug addiction field and individuals perceiving the profession as less respectable and impactful, possess higher stigma. Gender differences were also observed, with male professionals reporting lower stigma. Those with personal experiences of mental illness and engagement in psychotherapy demonstrated lower stigma levels. Study findings emphasize the critical need for directed efforts to combat stigma, particularly for professionals working with addictions. Addressing occupational stigma, promoting psychotherapy training and strengthening the professional perception of mental health workers are essential steps toward improving attitudes toward patients with mental illness and patient care.
Introduction
Mental health stigma is a complex and pervasive issue that negatively impacts individuals, communities and healthcare systems. It has a deep-rooted past and is widespread in numerous societies (Rössler, Reference Rössler2016).
The stigma surrounding mental health conditions plays a significant role in marginalizing and discriminating against those affected, hindering their access to critical resources and limiting their ability to engage fully in society. It also disrupts nearly all areas of mental healthcare, from health promotion and early support to the availability and consistency of treatment (Sirey et al., Reference Sirey, Bruce, Alexopoulos, Perlick, Raue, Friedman and Meyers2001; Thornicroft, Reference Thornicroft2006, Reference Thornicroft2008; Mehta et al., Reference Mehta, Clement, Marcus, Stona, Bezborodovs, Evans-Lacko, Palacios, Docherty, Barley, Rose, Koschorke, Shidhaye, Henderson and Thornicroft2015). Stigma toward mental illness can damage self-esteem, diminish quality of life, reduce social support and lower treatment adherence, thereby worsening overall mental health (Livingston and Boyd, Reference Livingston and Boyd2010; Fox et al., Reference Fox, Smith and Vogt2018). Furthermore, stigma intensifies suicidal thoughts and behaviors, especially in those already at risk, and correlates with higher suicide and mortality rates (Thornicroft, Reference Thornicroft2006; Taylor et al., Reference Taylor, Gooding, Wood and Tarrier2011; Rimkeviciene et al., Reference Rimkeviciene, Hawgood, O’Gorman and De Leo2015; Schomerus et al., Reference Schomerus, Evans-Lacko, Rüsch, Mojtabai, Angermeyer and Thornicroft2015).
There is a growing interest in research on stigma and social exclusion related to mental health among different populations (Evans-Lacko et al., Reference Evans-Lacko, Courtin, Fiorillo, Knapp, Luciano, Park, Brunn, Byford, Chevreul, Forsman, Gulacsi, Haro, Kennelly, Knappe, Lai, Lasalvia, Miret, O’Sullivan, Obradors-Tarragó, Rüsch, Sartorius, Svab, van Weeghel, Van Audenhove, Wahlbeck, Zlati, McDaid and Thornicroft2014). Stigmatizing attitudes vary by cultural and social context. Stigma toward people with mental illness remains prevalent in the Nordic region, despite strong welfare systems and equal access to healthcare (Högberg et al., Reference Högberg, Magnusson, Lützén and Ewalds-Kvist2012; Hellström et al., Reference Hellström, Gren Voldby and Eplov2022). People with schizophrenia and psychotic disorders experienced the highest levels of stigma, more than those with depression or autism (Jensen et al., Reference Jensen, Martens, Nikolajsen, Skytt Gregersen, Heckmann Marx, Goldberg Frederiksen and Hansen2016; Svensson and Hansson, Reference Svensson and Hansson2016). While in the United States, stigma around depressive disorders resembles the situation in Nordic countries and has significantly decreased, stigma reduction efforts have had limited success in changing behaviors, especially for schizophrenia and alcohol dependence (Pescosolido et al., Reference Pescosolido, Halpern-Manners, Luo and Perry2021). In Asian nations and low- and middle-income countries, stigma toward mental illness is highly prevalent. In contrast with the European region, cultural beliefs and myths play a significant role; for example, mental illness is linked to karma, supernatural forces or moral weakness. In addition, older age, male gender and lower socioeconomic status were linked to higher levels of stigma (Vaishnav et al., Reference Vaishnav, Javed, Gupta, Kumar, Vaishnav, Kumar, Salih, Levounis, Ng, Alkhoori, Luguercho, Soghoyan, Moore, Lakra, Aigner, Wancata, Ismayilova, Islam, Da Silva, Chaimowitz, Xiaoping, Okasha, Meyer-Lindenberg, Schulze, Roger, Chiu, Wa, Tanra, Park, Panteleeva, Taveras, Mazaliauskiene, Sulaiman, Sanchez, Sedain, Sheikh, Lien, Rasool, Buenaventura, Gambheera, Ranasinghe, Sartorius, Charnsil, Larnaout, Nakku and Ashurov2023). There is limited research on the topic in post-Soviet Union countries and the Central Asian region (Aliev et al., Reference Aliev, Roberts, Magzumova, Panteleeva, Yeshimbetova, Krupchanka, Sartorius, Thornicroft and Winkler2021; Quirke et al., Reference Quirke, Klymchuk, Suvalo, Bakolis and Thornicroft2021).
Research on stigma among mental health professionals presents mixed findings. Some studies suggest that mental healthcare providers hold more positive attitudes than the general population (Lauber et al., Reference Lauber, Anthony, Ajdacic-Gross and Rössler2004; Hori et al., Reference Hori, Richards, Kawamoto and Kunugi2011; Hellström et al., Reference Hellström, Gren Voldby and Eplov2022; Vaishnav et al., Reference Vaishnav, Javed, Gupta, Kumar, Vaishnav, Kumar, Salih, Levounis, Ng, Alkhoori, Luguercho, Soghoyan, Moore, Lakra, Aigner, Wancata, Ismayilova, Islam, Da Silva, Chaimowitz, Xiaoping, Okasha, Meyer-Lindenberg, Schulze, Roger, Chiu, Wa, Tanra, Park, Panteleeva, Taveras, Mazaliauskiene, Sulaiman, Sanchez, Sedain, Sheikh, Lien, Rasool, Buenaventura, Gambheera, Ranasinghe, Sartorius, Charnsil, Larnaout, Nakku and Ashurov2023). Conversely, other studies indicate that their biases are comparable to those found in the general public (Schulze, Reference Schulze2007; Jensen et al., Reference Jensen, Martens, Nikolajsen, Skytt Gregersen, Heckmann Marx, Goldberg Frederiksen and Hansen2016). Additionally, some research suggests that mental health professionals may, in certain cases, exhibit even higher levels of stigma. For instance, psychiatrists have been reported to endorse more negative stereotypes about individuals with mental illness than both the general population and other mental health professionals (Lauber et al., Reference Lauber, Nordt, Falcato and Rössler2000; Nordt et al., Reference Nordt, Rössler and Lauber2006; Henderson et al., Reference Henderson, Noblett, Parke, Clement, Caffrey, Gale-Grant, Schulze, Druss and Thornicroft2014). Notably, there is evidence that psychiatrists themselves may reinforce stigmatizing beliefs – for example, associating individuals with schizophrenia with traits such as “unpredictability” and “dangerousness” (Lauber et al., Reference Lauber, Anthony, Ajdacic-Gross and Rössler2004). This highlights a paradox: mental health professionals serve as both advocates for change and, at times, contributors to stigma (Schulze, Reference Schulze2007).
Research on the stigmatizing attitudes of mental health professionals remains scarce, with even fewer studies exploring the underlying factors influencing these perceptions. Burnout and lower job satisfaction have been pointed out as contributing factors to stigma among mental health professionals (Gibb et al., Reference Gibb, Beautrais and Surgenor2010; Solmi et al., Reference Solmi, Granziol, Danieli, Frasson, Meneghetti, Ferranti, Zordan, Salvetti, Conca, Salcuni and Zaninotto2020; Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020; Vaishnav et al., Reference Vaishnav, Javed, Gupta, Kumar, Vaishnav, Kumar, Salih, Levounis, Ng, Alkhoori, Luguercho, Soghoyan, Moore, Lakra, Aigner, Wancata, Ismayilova, Islam, Da Silva, Chaimowitz, Xiaoping, Okasha, Meyer-Lindenberg, Schulze, Roger, Chiu, Wa, Tanra, Park, Panteleeva, Taveras, Mazaliauskiene, Sulaiman, Sanchez, Sedain, Sheikh, Lien, Rasool, Buenaventura, Gambheera, Ranasinghe, Sartorius, Charnsil, Larnaout, Nakku and Ashurov2023). Findings on age and stigma among psychiatrists are conflicting. Some studies link younger age to greater negative stereotyping, especially toward patients with schizophrenia (Loch et al., Reference Loch, Hengartner, Guarniero, Lawson, Wang, Gattaz and Rössler2013b), while others associate older age, higher education and longer patient contact with more favorable attitudes (Vibha et al., Reference Vibha, Saddichha and Kumar2008). However, longer careers in psychiatry have also been linked to higher stigma levels (Nordt et al., Reference Nordt, Rössler and Lauber2006; da Silva et al., Reference da Silva, Loch, Leal, da Silva, Rosa, Bomfim, Malloy-Diniz, Schwarzbold, Diaz and Palha2021), with older psychiatrists more likely to hold stigmatizing attitudes (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a).
Attitudes toward mental illness vary across healthcare professionals and levels of training. Among trainees, medical students often hold opposing views, underscoring gaps in education (Vaishnav et al., Reference Vaishnav, Javed, Gupta, Kumar, Vaishnav, Kumar, Salih, Levounis, Ng, Alkhoori, Luguercho, Soghoyan, Moore, Lakra, Aigner, Wancata, Ismayilova, Islam, Da Silva, Chaimowitz, Xiaoping, Okasha, Meyer-Lindenberg, Schulze, Roger, Chiu, Wa, Tanra, Park, Panteleeva, Taveras, Mazaliauskiene, Sulaiman, Sanchez, Sedain, Sheikh, Lien, Rasool, Buenaventura, Gambheera, Ranasinghe, Sartorius, Charnsil, Larnaout, Nakku and Ashurov2023). However, those considering a career in psychiatry, along with psychiatrists themselves, tend to display more favorable attitudes (Reavley et al., Reference Reavley, Mackinnon, Morgan and Jorm2013; Janoušková et al., Reference Janoušková, Formánek, Bražinová, Mílek, Alexová, Winkler and Motlová2021; Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022). Although research on nurses’ attitudes remains limited, some findings suggest that community and public health nurses demonstrate more accepting views, whereas inpatient nurses are more socially restrictive toward individuals with mental illness (Ishige and Hayashi, Reference Ishige and Hayashi2005; Linden and Kavanagh, Reference Linden and Kavanagh2012).
Mental health professionals’ attitudes toward mental illness can be influenced by personal experiences and exposure. Those who are hesitant to seek mental healthcare for themselves tend to exhibit stronger stigmatizing views (Corrigan et al., Reference Corrigan, Mittal, Reaves, Haynes, Han, Morris and Sullivan2014). Conversely, psychiatrists with a history of psychiatric diagnosis or treatment generally demonstrate more accepting attitudes (Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020; Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022, Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). Regular interactions with individuals with mental illness in community settings have also been associated with reduced stigma among psychiatrists (Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020; da Silva et al., Reference da Silva, Loch, Leal, da Silva, Rosa, Bomfim, Malloy-Diniz, Schwarzbold, Diaz and Palha2021). However, in some cases, frequent exposure to mental illness has been linked to heightened stigmatizing views within the mental health professional community (Nordt et al., Reference Nordt, Rössler and Lauber2006; da Silva et al., Reference da Silva, Loch, Leal, da Silva, Rosa, Bomfim, Malloy-Diniz, Schwarzbold, Diaz and Palha2021).
Beyond personal experience, a professional environment also plays a role in shaping attitudes. Psychiatrists who provided psychotherapy and worked in settings with less stigmatizing colleagues were significantly more likely to hold positive views toward individuals with mental illness (Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022, Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). However, levels of stigma may also be influenced by broader socio-cultural factors. Studies suggest that psychiatrists in post-communist countries exhibit higher levels of stigma compared to their counterparts elsewhere (Harangozo et al., Reference Harangozo, Reneses, Brohan, Sebes, Csukly, López-Ibor, Sartorius, Rose and Thornicroft2014), particularly high stigma scores were reported among psychiatrists in Latvia, Ukraine and Belarus (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a).
There is a lack of comprehensive data on how stigma among mental health professionals differs across cultural contexts, particularly in non-Western countries, emphasizing the need for more globally representative research.
Stigma is reported to be widespread throughout Central Asia, and it is characterized by prevalent societal misunderstandings about mental health (Aliev et al., Reference Aliev, Roberts, Magzumova, Panteleeva, Yeshimbetova, Krupchanka, Sartorius, Thornicroft and Winkler2021). Kazakhstan is the largest upper-middle-income country in the Central Asian region, which has been ranked among the highest for suicide rates globally, particularly affecting adolescents (WHO, 2025). The country implemented its first national suicide prevention strategy in 2014, drawing attention to a deep-rooted reluctance among families to assist individuals dealing with mental health issues, including suicidal tendencies, due to prevailing fears of social judgment and stigma. Destigmatization became a central focus of the prevention effort in the country, supported by technical assistance from UNICEF (WHO, 2022) however, no prior studies have examined mental health stigma among healthcare specialists.
The research aims of this study were to (1) investigate how prevalent stigma toward mental illness is among mental health specialists (psychiatrists, narcologists, psychotherapists, psychiatry residents and mental health nurses) in Kazakhstan, and (2) what factors contribute to the stigmatizing attitudes. Understanding the stigma toward mental illness among healthcare professionals is essential, as it directly influences the quality of care patients receive. Study findings can provide insights into the barriers to effective mental healthcare and inform interventions aimed at improving attitudes toward patients with mental illness among medical workers.
Methods
Study design and sample
This study used a cross-sectional design, collecting data through a self-administered online questionnaire shared via secure links. The gathered data were analyzed quantitatively to spot key patterns in attitudes of mental health professionals toward mental illness. The reporting of this observational study follows the STROBE guidelines.
The questionnaire was distributed among psychiatrists, narcologists, psychotherapists, psychiatry residents and mental health nurses working in various healthcare institutions across different regions of Kazakhstan. The recruitment message, including a link to the online survey, was distributed among mental health specialists using purposive, snowball and convenience sampling methods. Social media platforms such as WhatsApp, Instagram and Telegram were utilized to distribute the link. Specifically, the survey link was shared in group chats on WhatsApp for mental health professionals from key hospitals and clinics. The survey was sent to direct contacts of mental health specialists, who were encouraged to share the link with colleagues to maximize the response rate.
With a total population of 4,561 mental health professionals in Kazakhstan (803 psychiatrists, 3,312 nurses, 262 psychologists and 184 child psychiatrists) (WHO, 2022), the sample size for the study was calculated as 302 participants, using the formula: n = [DEFF*Np(1-p)]/[(d2/Z21-α/2*(N-1) + p*(1-p)]. The total population size, used to apply the finite population correction factor (FPC), was 4,561. The expected prevalence of the outcome in the population was estimated at 30%, with a margin of error of ±5%. The confidence level was set at 95%, corresponding to an absolute precision of 5%. A design effect (DEFF) of 1 was assumed.
Inclusion criteria include currently practicing mental health professionals with direct patient care experience.
Procedure
The survey was developed based on the literature review of previous studies (Kassam et al., Reference Kassam, Papish, Modgill and Patten2012; Modgill et al., Reference Modgill, Patten, Knaak, Kassam and Szeto2014; Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022, Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). The questionnaire was built into the Qualtrics survey platform and was developed in English, Kazakh and Russian. The link was shared with mental health specialists through purposive and snowball sampling. The online survey was conducted between December 2024 and February 2025.
The questionnaire comprised five modules with 33 questions in total. The modules were (1) sociodemographic characteristics, (2) professional characteristics and beliefs, (3) stigmatizing attitudes toward people with mental illness, (4) lived experience of mental illness and (5) job satisfaction and burnout.
Measures
Sociodemographic characteristics
This section included four questions inquiring about participants’ age, gender, ethnicity and region of residence.
Professional characteristics and beliefs
Questions included years of experience in mental health, year of graduation, qualification status (trainee or specialist), a field of psychiatry (child, adult, narcology, psychotherapy, mental health nursing), type of healthcare setting (inpatient, outpatient, private practice), perceived respectability of mental health work and perceived stigma toward people with mental illness among colleagues.
Stigmatizing attitudes toward mental illness
To evaluate the main outcome of the study, the 15-item Opening Minds Stigma Scale for Healthcare Providers (OMS-HC) was employed. Initially, this scale was developed as a 20-item scale; however, the 15-item version of the OMS-HC is considered superior because a previous validation study using factor analysis identified five items that could be dropped without compromising the scale’s effectiveness (Modgill et al., Reference Modgill, Patten, Knaak, Kassam and Szeto2014). Each item was scored on a 5-point Likert scale, where 1 represents “strongly disagree” and 5 means “strongly agree.” Questions 2, 6, 7, 8 and 14 were reverse-scored as per the OMS-HC guidelines. The overall score indicates participants’ general stigma levels, while its three subscales measure different aspects, including Attitudes, Disclosure and Help-Seeking and Social Distance subscales. Stigma was quantified by adding the responses to all 15 items on the scale, yielding a total score that could range between 15 and 75. Higher scores signify greater stigma. Prior research has indicated that the scale demonstrated a satisfactory level of internal consistency, with Cronbach’s alpha = 0.79, with subscales scoring 0.67–0.68 (Modgill et al., Reference Modgill, Patten, Knaak, Kassam and Szeto2014). The subscales’ lower alpha may result from fewer items, which can reduce reliability below the recommended 0.70 threshold (Streiner, Reference Streiner2003).
The validated Russian version of the scale was requested via e-mail from Dr. Dorottya Őri, a principal investigator of a similar study across 32 European countries (Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022, Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). The psychometric properties of the OMS-HC were examined across all participating countries using a series of confirmatory factor analyses (Őri et al., Reference Őri, Szocsics, Molnár, Bankovska Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabacos, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Rus Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Hargi, Ahmadova, Vircik, Yilmaz Kafali, Grinko and Győrffy Z Rózsa2023b), which indicated that the total score, rather than subscale scores, is recommended for assessing overall stigmatizing attitudes. The OMS-HC was translated into the Kazakh language employing the forward- and back-translation method by our bilingual research team members (Appendix 1, Supplementary Materials). We thoroughly adopted the scale with permission from developers, and tested for its reliability, face and content validity in local languages. Internal consistency of the OMS-HC scale within our study sample was evaluated using Cronbach’s alpha coefficient, which was 0.66 for the Russian version and 0.65 for the Kazakh version. The OMS-HC scale and questionnaire were pretested with a small group of mental health professionals, resulting in minor wording adjustments for clarity.
Lived experience of mental illness
This section was comprised of questions on the presence of friends or family members with mental illness, help-seeking behavior for one’s own mental health conditions, participation in psychotherapy for any reason and personal exposure to medical treatment for mental illness.
Job satisfaction and burnout
Job satisfaction was assessed using a single-item measure on a continuous scale ranging from 0 to 10, in response to the question: “On a scale from 0 to 10, how would you rate the level of your job satisfaction?” A score of 0 indicated “Very Dissatisfied,” while a score of 10 indicated “Very Satisfied.” To measure burnout, the non-proprietary single-item burnout subscale was used, which allows respondents to interpret burnout in their own terms, asking: “Overall, based on your definition of burnout, how would you rate your level of burnout?” Answers follow a five-point ordinal scale, ranging from 1 (“I enjoy my work and experience no burnout symptoms”) to 5 (“I feel completely burned out and may need to make changes or seek help”). Intermediate options describe increasing levels of stress and exhaustion, from occasional fatigue (2) to persistent symptoms and workplace frustration (4) (Schmoldt et al., Reference Schmoldt, Freeborn and Klevit1994). For analysis, responses were categorized into two groups: scores ≤2 indicate no burnout, while scores ≥3 suggest one or more symptoms of burnout. Several studies assessed its validity by comparing it to the full Maslach Burnout Inventory- Human Services Survey (MBI-HSS), concluding that it effectively identified burnout, especially in relation to emotional exhaustion (MBI-EE), while offering a more efficient and license-free alternative for data collection (Rohland et al., Reference Rohland, Kruse and Rohrer2004; Hansen and Girgis, Reference Hansen and Girgis2010; Dolan et al., Reference Dolan, Mohr, Lempa, Joos, Fihn, Nelson and Helfrich2015).
Statistical analysis
Data cleaning and analyses were performed using Stata software, version 18.0. Responses with missing data on the OMS-HC scale, as well as those containing only sociodemographic information, were excluded from the analysis; however, for other variables (sociodemographic characteristics, professional characteristics and beliefs, lived experience of mental illness, job satisfaction and burnout), cases with partial missing data were retained to avoid unnecessary reduction in sample size. Univariate analysis was conducted to examine the variables and describe participant characteristics, presenting categorical variables as frequencies and percentages, while continuous variables were summarized as mean values with standard deviation.
Bivariate analysis was then performed to explore associations between the main outcome variable, the attitudes toward mental illness assessed using the OMS-HC 15-item scale, and independent variables, including sociodemographic factors, professional data, personal experience of mental illness, job satisfaction and burnout and attitudes toward mental health recovery, using a significance threshold of p < 0.05. Simple linear regression analyses were applied to assess relationships between the OMS-HC score and independent variables. Due to low response counts in certain subcategories of independent variables and recommended guidelines, some of them were merged into broader categories.
Subsequently, multiple linear regression analysis was conducted, and after adjusting for covariates, only independent variables maintaining significance at p < 0.05 remained in the final model. To address multicollinearity, the variance inflation factor (VIF) was used, and variables were assessed for interactions and confounding to ensure the robustness of the model.
Results
Descriptive analysis
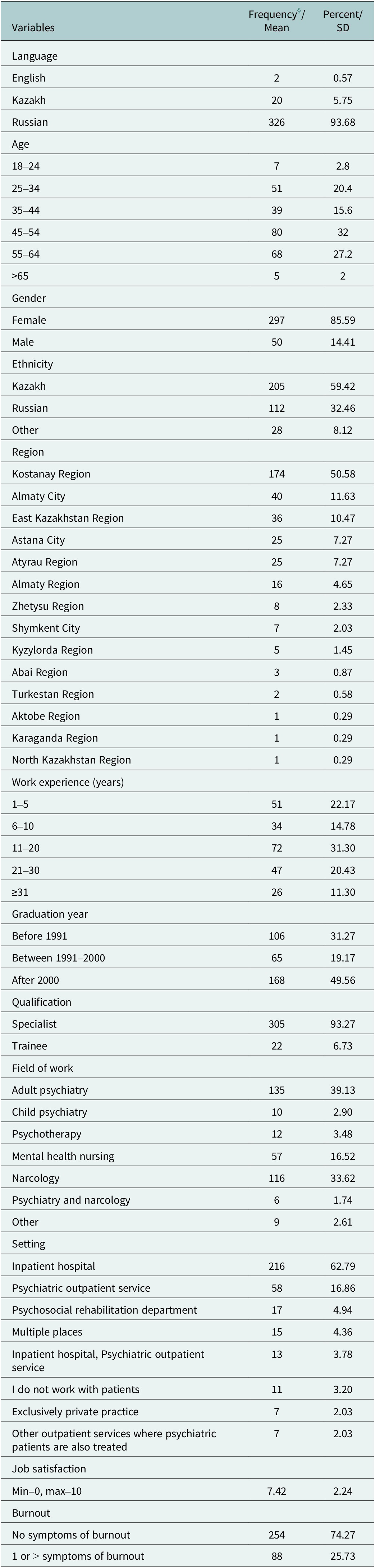
Table 1 summarizes the sociodemographic and professional profiles of the study participants, encompassing age, gender, ethnicity, region of residence, years of work experience, graduation year, qualifications, field of work, job setting, job satisfaction and burnout levels.
Sociodemographic and professional characteristics of participants (n = 348)

§ Total frequencies may vary because of the missing values.
Overall, 388 responses were recorded, and after data cleaning, 348 of them were included in the analysis. The majority of responses were in the Russian language (n = 326), followed by responses in Kazakh (n = 20) and English (n = 2). Participants’ ages ranged from 18 to over 65 years, with a minimum age of 22 and a maximum of 74 years old. The majority of participants were aged 45–54 years (22.99%), followed by those aged 55–64 years (19.54%). Regarding gender distribution, the sample consisted of 85.59% female (n = 297) and 14.41% male (n = 50). Participants were mainly Kazakh (59.42%), followed by Russian (32.46%) and other ethnicities (8.12%). Participants were from various regions across Kazakhstan, with the highest proportion from Kostanay Region (50.58%), followed by Almaty City (11.63%) and East Kazakhstan Region (10.47%). Other regions were represented in smaller proportions.
Most participants had 11–20 years of work experience (31.30%), followed by those with 1–5 years (22.17%) and 21–30 years (20.43%). Regarding graduation year, nearly half of the participants (49.56%) graduated after the year 2000, while 31.27% graduated before 1991. Predominantly, participants held the qualification of Specialist (93.27%), with a small proportion being trainees (6.73%). The highest percentage of participants worked in adult psychiatry (39.13%), followed by narcology (33.62%) and mental health nursing (16.52%). Fewer participants worked in child psychiatry (2.90%), psychotherapy (3.48%) or both in psychiatry and narcology (1.74%).
Work settings varied, with 62.79% of participants working in inpatient hospitals, followed by 16.86% in psychiatric outpatient services. Smaller proportions worked in psychosocial rehabilitation departments (4.94%), multiple settings (4.36%) or exclusively private practice (2.03%). The mean job satisfaction score was 7.42 (SD = 2.24) on a 10-point scale, indicating overall moderate to high job satisfaction among participants. Regarding burnout symptoms, 74.27% of participants reported no symptoms of burnout, while 25.73% experienced at least one symptom of burnout.
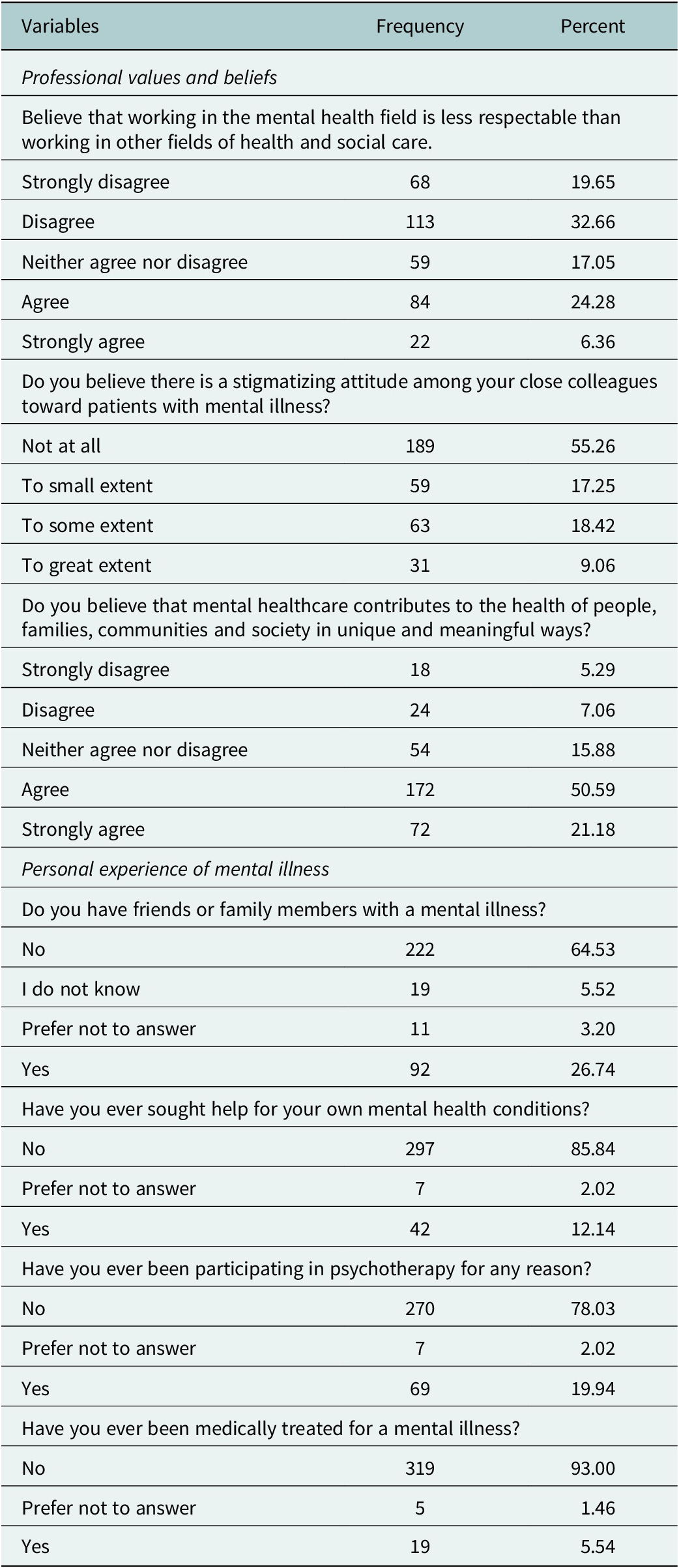
Table 2 presents findings on participants’ professional values and beliefs about mental healthcare, and personal experiences with mental illness. Participants expressed diverse opinions regarding the respectability of working in the mental health field compared to other health and social care professions. While 19.65% strongly disagreed and 32.66% disagreed with the notion that mental health work is less respectable, a considerable proportion remained neutral (17.05%). However, 24.28% agreed and 6.36% strongly agreed with this perception.
Professional values and beliefs, and personal experience of mental illness

Regarding stigmatizing attitudes among close colleagues toward patients with mental illness, more than half of the participants (55.26%) reported perceiving no stigmatization at all, while 17.25% acknowledged a small extent of stigmatization. Notably, 18.42% believed stigma existed to some extent and 9.06% perceived stigma to a great extent among their colleagues.
When asked whether mental healthcare contributes uniquely and meaningfully to society, a majority of participants held positive views, with 50.59% agreeing and 21.18% strongly agreeing. However, 5.29% strongly disagreed and 7.06% disagreed, while 15.88% remained neutral on this statement.
A significant proportion of participants (64.53%) reported not having friends or family members with mental illness, while 26.74% confirmed having such connections. A small proportion of respondents were uncertain (5.52%) or preferred not to answer (3.20%). Regarding seeking help for personal mental health conditions, 85.84% stated they had never sought professional help, while 12.14% reported having done so and 2.02% preferred not to disclose this information.
Participation in psychotherapy for any reason was reported by 19.94% of respondents, whereas 78.03% had never participated in psychotherapy and 2.02% preferred not to answer.
When asked about medical treatment for a mental illness, 93.00% reported never receiving such treatment, while 5.54% had been medically treated and 1.46% preferred not to disclose this information.
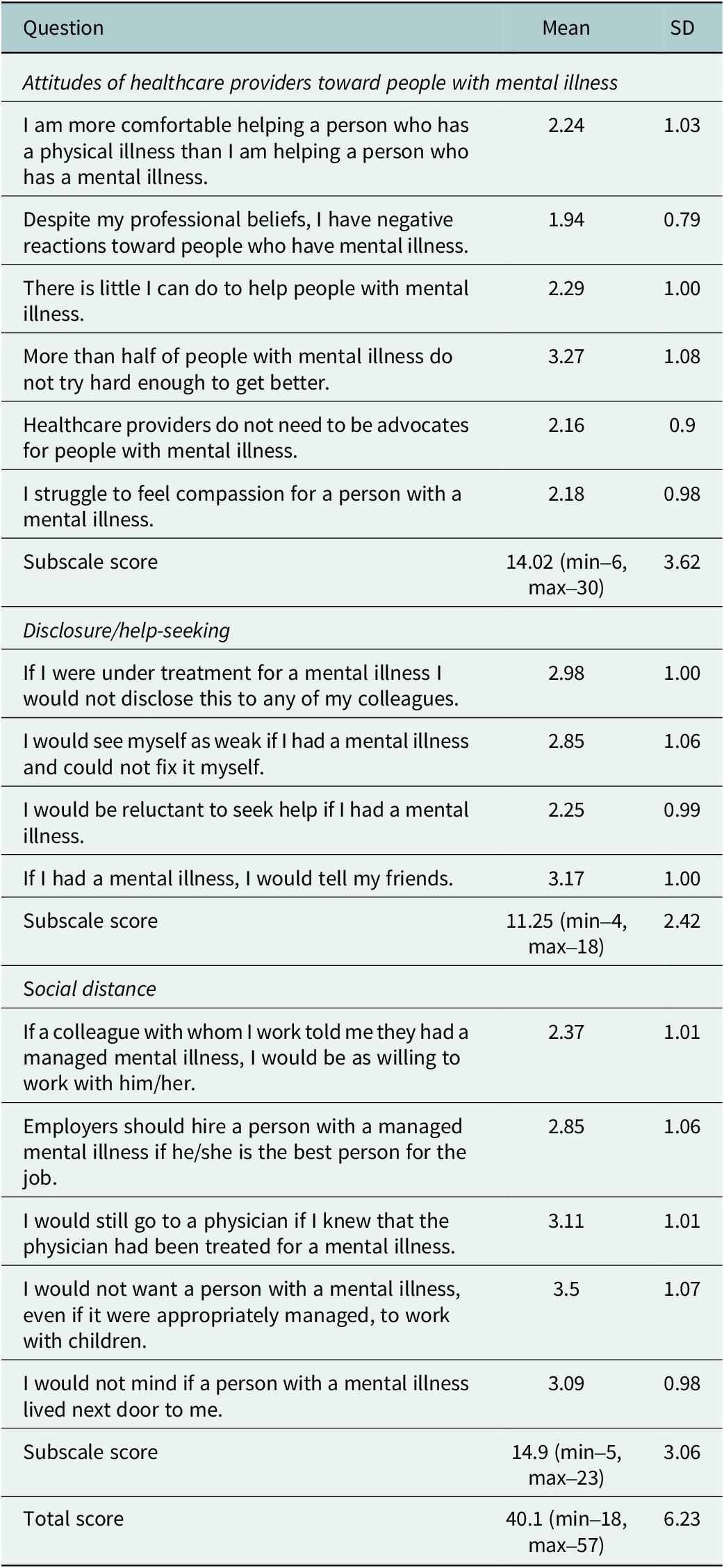
Table 3 presents the descriptive statistics for the 15-item OMS-HC. The data were normally distributed, with a total mean of 40.1 (SD = 6.23; range: 18–57).
Opening minds stigma scale for healthcare providers

For the Attitudes of Healthcare Providers Toward People with Mental Illness subscale, the mean item scores ranged from 1.94 to 3.27, with a subtotal mean of 14.02 (SD = 3.62; range: 6–30). The highest-rated item, “More than half of people with mental illness don’t try hard enough to get better,” had 3.27 (SD = 1.08), while the lowest-rated item, “Despite my professional beliefs, I have negative reactions toward people who have mental illness,” had 1.94 (SD = 0.79).
In the Disclosure and Help-Seeking subscale, a subtotal mean was 11.25 (SD = 2.42; range: 4–18). The majority of respondents were reluctant to disclose their own mental health concerns, resulting in a right-skewed distribution of responses. This trend was particularly evident in items such as “If I had a mental illness, I would tell my friends” (mean = 3.17), “If I were under treatment for a mental illness, I would not disclose this to any of my colleagues” (mean = 2.98) and “I would see myself as weak if I had a mental illness and could not fix it myself” (mean = 2.85).
The Social Distance subscale had a subtotal mean of 14.9 (SD = 3.06; range: 5–23), with item scores generally tending toward higher values. Notably, respondents expressed the greatest concern regarding individuals with mental illness working with children (mean = 3.50), followed by willingness to visit a physician who had been treated for a mental illness (mean = 3.11) and acceptance of having a neighbor with a mental illness (mean = 3.09). These findings indicate that while some respondents were open to social integration, reservations remained, particularly in professional and caregiving contexts.
Bivariate analysis
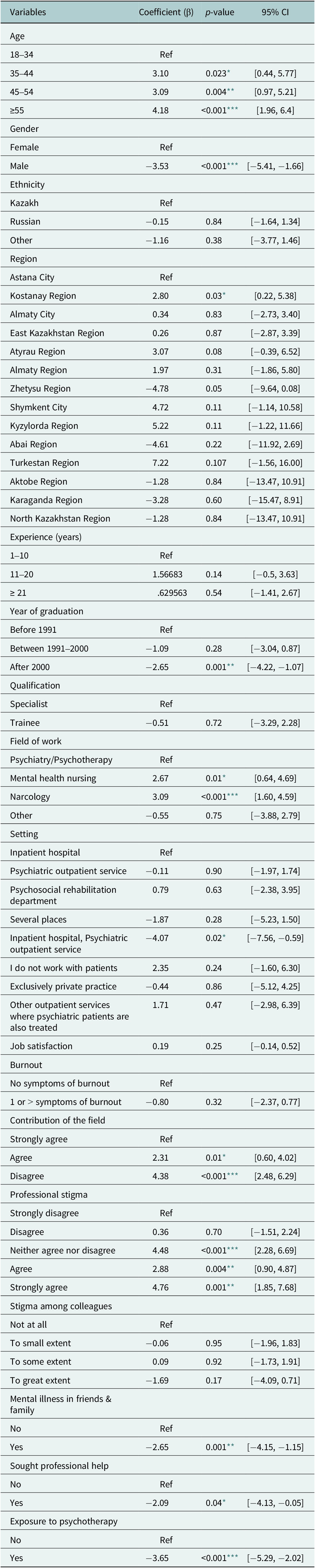
A simple linear regression analysis was conducted to examine the associations between various independent factors and stigma levels, as measured by the OMS-HC scale (Table 4).
Simple linear regression analysis of the associations of independent variables with stigma level among mental health professionals

* Significance level p < 0.05.
** Significance level p < 0.01.
*** Significance level p < 0.001.
Age was found to be positively associated with stigma levels, with older age groups demonstrating significantly higher stigma scores compared to the reference group (18–34 years). Participants aged 35–44 years (β = 3.10, p = 0.023), 45–54 years (β = 3.09, p = 0.004) and ≥ 55 years (β = 4.18, p < 0.001) had significantly higher stigma levels.
Male participants exhibited significantly lower stigma scores than females (β = −3.53, p < 0.001). Additional analyses of OMS-HC subscales revealed statistically significant gender differences on Attitudes and Social Distance subscales, with males reporting lower stigma scores (β = −1.35, p = 0.015 and β = −1.67, p < 0.001, respectively; not shown in the table), while there was no significant difference on the Disclosure/Help-seeking subscale.
Regional differences in stigma levels were observed, with mental health professionals from Kostanay Region reporting significantly higher stigma compared to those in Astana City (β = 2.80, p = 0.03). In contrast, professionals from Zhetysu Region demonstrated significantly lower stigma (β = −4.78, p = 0.05), with the largest reduction observed among all regions, although marginally significant. No significant differences were found for other regions when compared to Astana City.
Mental health professionals working in mental health nursing (β = 2.67, p = 0.01) and narcology (β = 3.09, p < 0.001) had significantly higher stigma levels compared to those in psychiatry/psychotherapy. Graduation year was also associated with stigma, as those who graduated after 2000 had significantly lower stigma scores (β = −2.65, p = 0.001) in comparison with specialists who graduated before 1991. However, ethnicity, work experience and job satisfaction did not show significant associations with stigma levels.
Participants who had friends or family members with mental illness exhibited significantly lower stigma levels (β = −2.65, p = 0.001) than those who did not. Similarly, individuals who had sought professional help for their own mental health (β = −2.09, p = 0.045) or had participated in psychotherapy (β = −3.65, p < 0.001) reported significantly lower stigma scores.
Regarding professional beliefs, there was a meaningful difference across participants who strongly agreed with the idea that mental healthcare contributes meaningfully to society and those who just agreed (β = 2.31, p = 0.008) or disagreed (β = 4.38, p < 0.001).
Furthermore, individuals who expressed neutrality (β = 4.48, p < 0.001), agreement (β = 2.88, p = 0.004) or strong agreement (β = 4.76, p = 0.001) with the perception that working in mental health is less respectable exhibited significantly higher stigma levels.
Multivariate analysis
The final multivariate linear regression model is expressed as:
Stigma level (OMS-HC) = β0 + β1Gender + β2Age + β3Field of work + β4Proffesional stigma + β5Mental illness in friends&family + β6Exposure to psychotherapy + β7Contribution of the field.
The model explained 33.5% of the variance in stigma levels among mental health professionals (R 2 = 0.335, adjusted R 2 = 0.2875, F (15, 210) = 7.05, p < 0.001). No significant interactions were observed among the study variables.
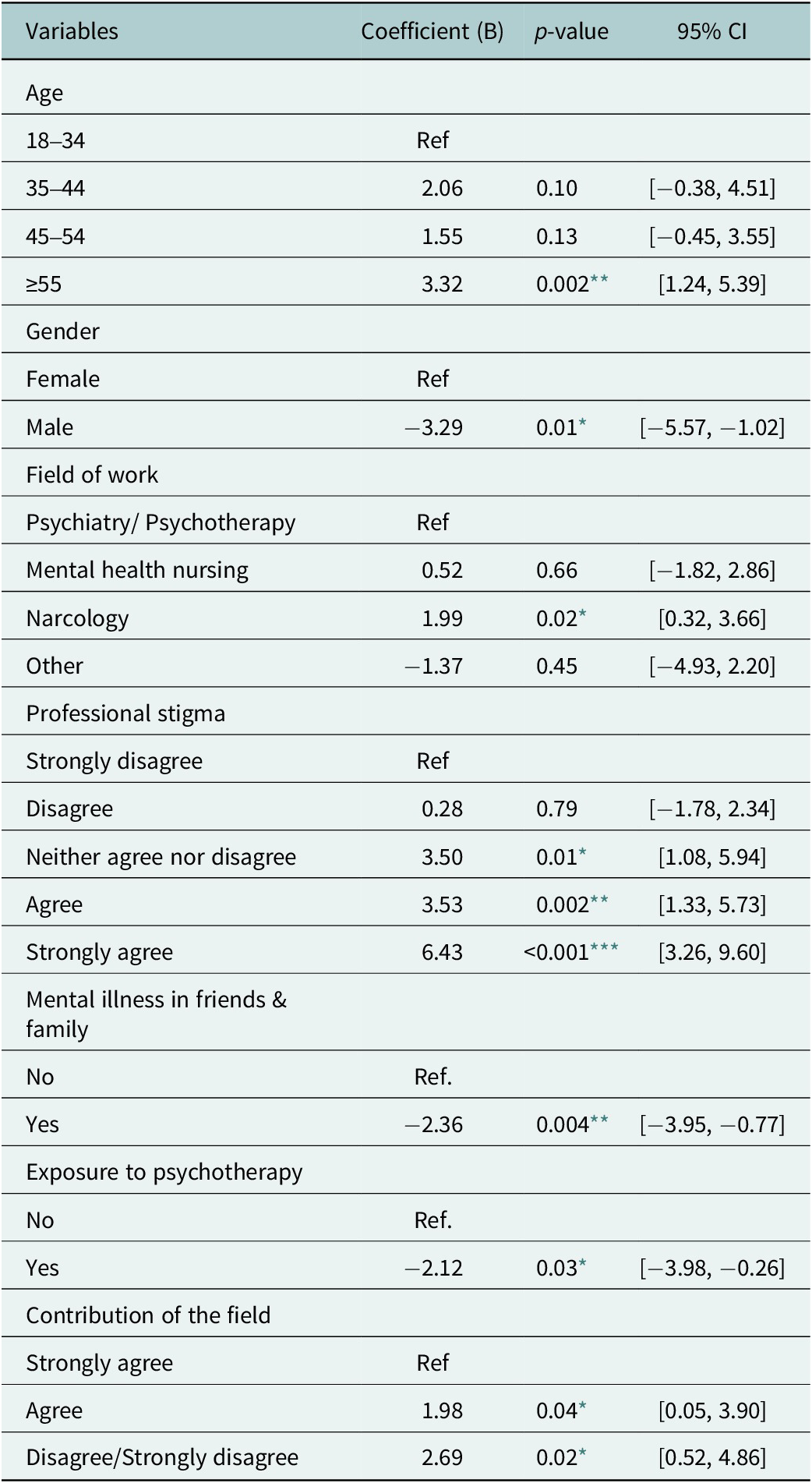
Age remained a significant predictor, with professionals aged ≥55 exhibiting significantly higher stigma levels compared to the youngest age group (β = 3.32, p = 0.002) (Table 5). Gender differences persisted, with male professionals demonstrating significantly lower stigma scores than their female counterparts (β = −3.29, p = 0.005). Field of work also played a role, as professionals in narcology had significantly higher stigma scores compared to those in psychiatry/psychotherapy (β = 1.99, p = 0.02).
Multiple linear regression analysis of the associations of independent variables with stigma level among mental health professionals

* Significance level p < 0.05.
** Significance level p < 0.01.
*** Significance level p < 0.001.
Perceived lack of respectability of career in mental health strongly predicted higher stigma, with neutrality (β = 3.50, p = 0.005), agreement (β = 3.53, p = 0.002) and strong agreement (β = 6.43, p < 0.001) linked to increased stigma levels. Personal experience with mental illness was associated with lower stigma, with those having affected friends or family (β = −2.36, p = 0.004) and psychotherapy exposure (β = −2.12, p = 0.03) showing reduced stigma. Conversely, weaker belief in their field’s positive contribution was associated with higher stigma.
Discussion
This study explores the often-overlooked issue of stigma within the mental health profession. Given the limited research on this topic, particularly among mental healthcare providers in Central Asia, this study aimed to examine the attitudes of adult and child psychiatrists, narcologists, mental health nurses and psychiatry residents toward individuals with mental health conditions. The overall stigma score among participants indicated a moderate level of stigma, though it was higher than in similar international studies. Older professionals, females and those in narcology had more stigma, as did those who viewed mental health work as less respectable. Lower stigma was linked to having friends or family with mental illness, prior psychotherapy exposure and a strong belief in the positive impact of mental health work.
Our study results are consistent with most of the previous research that has shown mental health professionals are not immune to stigmatizing beliefs (Schulze, Reference Schulze2007; Henderson et al., Reference Henderson, Noblett, Parke, Clement, Caffrey, Gale-Grant, Schulze, Druss and Thornicroft2014). The overall OMS-HC scores indicate that stigma levels among mental health workers in Kazakhstan are relatively high, with the sample’s average total score being 40.1, 53.5% of the maximum. These findings are comparable to stigma scores reported in other countries. For instance, the mean stigma score among mental healthcare professionals in Bahrain was 36.8 (Al Saif et al., Reference Al Saif, Al Shakhoori, Nooh and Jahrami2019); similar scores were observed in Belarus (35.01), Ukraine (35.02) and Latvia (35.98) (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). In comparison, a multicenter study conducted across 32 European countries reported an average total score of 30.47 (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a), indicating that stigma levels in Kazakhstan are significantly higher.
The subscale scores of the OMS-HC were also significantly high. The score for Attitudes of healthcare providers toward individuals with mental illness was 14.02 (46.7% of maximum possible), the Disclosure/Help-seeking score was 11.25 (56% of maximum possible) and the Social Distance score was 14.9 (59.6% of maximum possible). Differing from this, the average total subscale scores for European countries were 11.11, 9.78 and 9.58, respectively (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a).
Notably, Kazakhstani mental health professionals scored particularly high on the following attitude statement: “More than half of people with mental illness don’t try hard enough to get better” (mean = 3.27), reflecting a persistent stigma in this area. Our findings also emphasize that mental health specialists in Kazakhstan are particularly hesitant to disclose their personal mental health status to friends and colleagues, often perceiving themselves as weak if they cannot manage their challenges independently. The mean score for this subscale (11.25, 56% of the maximum possible) is consistent with previous research and comparable to findings from Belarus (11.31), Belgium (11.05), Latvia (11.00) and Ukraine (11.08) (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). Furthermore, Kazakhstani professionals demonstrated a stronger inclination toward maintaining social distance from individuals with mental illness. The mean score for the Social Distance subscale (14.9, 59.6% of the maximum possible) was much higher than the average scores reported in Belarus (11.20), Latvia (11.71) and Ukraine (11.63) (Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). The underlying socio-cultural and systemic differences may affect stigmatizing attitudes of professionals across countries (Harangozo et al., Reference Harangozo, Reneses, Brohan, Sebes, Csukly, López-Ibor, Sartorius, Rose and Thornicroft2014; Stefanovics et al., Reference Stefanovics, He, Ofori-Atta, Cavalcanti, Rocha Neto, Makanjuola, Ighodaro, Leddy and Rosenheck2016).
Furthermore, the findings of our study revealed several significant associations, providing insights into the factors that can contribute to stigma in mental health settings. Age emerged as a significant predictor of stigma levels, with older professionals (≥55 years) demonstrating substantially higher stigma scores than their younger colleagues. This trend may reflect generational differences in attitudes toward mental health, as younger professionals are likely to have been exposed to more recent educational programs and awareness campaigns aimed at reducing stigma. Similar findings have been reported in European studies and Bahrain, where older specialists exhibited higher stigma scores (Al Saif et al., Reference Al Saif, Al Shakhoori, Nooh and Jahrami2019; Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). On the contrary, our results contradict findings of the previous study from Turkey, which suggested that greater age and professional experience are associated with less stigmatizing attitudes among psychiatrists (Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020). This contrast highlights the complexity of stigma formation and suggests that factors beyond age, such as cultural influences and training approaches, may play a critical role in shaping professionals’ perspectives on mental illness.
Gender differences in stigma levels were also observed, with male professionals reporting significantly lower stigma compared to their female counterparts. This finding contrasts with most of the existing literature, which suggests that male health providers hold significantly more stigmatizing views toward people with mental illness, explained by theories of masculinity and stoicism, emphasizing emotional toughness and discouraging help-seeking (Almeida et al., Reference Almeida, Samouco, Grilo, Pimenta and Moreira2022; Kaitz et al., Reference Kaitz, Steinhilber and Harris2022). Furthermore, previous studies showed that female health providers tend to report lower stigma scores, showing more empathy and willingness to socialize with the mentally ill people (Pascucci et al., Reference Pascucci, La Montagna, Di Sabatino, Stella, Nicastro, Grandinetti, Testa, Parente, Janiri, Pozzi, Piemontese, Ventriglio and Bellomo2017; Chiles et al, Reference Chiles, Stefanovics and Rosenheck2018). However, the evidence on gender differences in stigma is mixed (Kruse and Dodell-Feder, Reference Kruse and Dodell-Feder2025), and many studies found no statistically significant differences between male and female participants (Destrebecq et al., Reference Destrebecq, Ferrara, Frattini, Pittella, Rossano, Striano, Terzoni and Gambini2018; Al Saif et al., Reference Al Saif, Al Shakhoori, Nooh and Jahrami2019; Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020; Őri et al., Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). While studies from Western countries consistently show lower stigma in females, our findings align with a previous study from Tunisia, which showed that female providers exhibited higher scores on specific components of stigma, such as skepticism regarding treatment (Fekih-Romdhane et al., Reference Fekih-Romdhane, Hamdi, Jahrami and Cheour2023). Findings of the current study may be explained by the specific cultural and healthcare context of Kazakhstan, where mental illness is highly stigmatized and the mental healthcare system remains focused on institutional care with a lack of community support services. While the majority of providers in the mental health field are represented by females, male professionals often occupy higher-ranking positions, granting them greater exposure to research-based, bio-psycho-social perspectives, which can contribute to lower stigma. In contrast, female professionals are more frequently involved in frontline patient care, where they experience greater exposure to severe and challenging cases, potentially reinforcing stigmatizing attitudes. Previous studies also reported that inpatient staff who primarily treat individuals with psychosis had the most negative attitudes (Hansson et al., Reference Hansson, Jormfeldt, Svedberg and Svensson2013). Moreover, higher scores on the social distance subscale in our study may reflect heightened perceptions of risk due to greater contact with individuals who have chronic or recurrent problems, which may lead to a more realistic assessment of long-term outcomes and negative attitudes (Jorm et al., Reference Jorm, Korten, Jacomb, Christensen and Henderson1999), especially in situations involving close social proximity, such as living as a neighbor or contact with children.
The professional field had a clear impact on stigma levels, with specialists in narcology showing significantly higher stigma compared to those in psychiatry and psychotherapy. In many European countries, psychiatry and addiction treatment are fully integrated disciplines. However, in post-Soviet nations such as Kazakhstan, despite the formal combination of these specialties during residency training, they continue to function as separate fields in practice, making direct comparisons difficult. Research has consistently shown that individuals with substance use disorders face some of the highest levels of stigma (Schomerus et al., Reference Schomerus, Lucht, Holzinger, Matschinger, Carta and Angermeyer2011) even within healthcare settings (van Boekel et al., Reference van Boekel, Brouwers, van Weeghel and Garretsen2013; Valdesalici et al., Reference Valdesalici, Saccon, Boatto, Manzan, Manera, Pani, Pavani, Zecchinato, Sava, Greco, Paganin and Solmi2024). The attribution theory suggests that the way people interpret the cause of a stigmatized identity influences their reactions toward the stigmatized individual (Weiner, Reference Weiner1995). Substance use disorders are often perceived as a controllable condition, compared to other uncontrollable conditions such as genetic disorders or severe mental illness, and therefore the response may be associated with higher stigma levels, including blame, anger or social exclusion, even from the side of mental health professionals. To reduce the stigma and barriers to effective treatment, educational interventions are needed to improve the understanding of drug dependence as not only a social, but rather as a health problem which should be treated and evaluated like any other complex chronic disease influenced by a combination of genetic, developmental and environmental factors (McLellan et al., Reference McLellan, Lewis, O’Brien and Kleber2000).
Perceptions of a profession in mental health played a crucial role in determining stigma levels. Professionals who considered the field less respectable demonstrated significantly higher stigma scores. Additionally, professionals who doubted the positive contribution of their field demonstrated significantly higher stigma scores compared to those who strongly affirmed its value. Research has demonstrated that psychiatrists face greater stigmatizing attitudes and discriminatory behaviors compared to other medical specialists (Gaebel et al., Reference Gaebel, Zäske, Zielasek, Cleveland, Samjeske, Stuart, Arboleda-Florez, Akiyama, Baumann, Gureje, Jorge, Kastrup, Suzuki, Tasman, Fidalgo, Jarema, Johnson, Kola, Krupchanka, Larach, Matthews, Mellsop, Ndetei, Okasha, Padalko, Spurgeoun, Tyszkowska and Sartorius2015). Addressing occupational stigma among psychiatrists is essential, as their perceptions can directly influence the quality of care they provide and affect individuals’ willingness to seek mental health support (Shi et al., Reference Shi, Li and Fan2023). Furthermore, occupational stigma is closely linked to higher burnout rates and lower patient satisfaction (Verhaeghe and Bracke, Reference Verhaeghe and Bracke2012). Despite these connections, the relationship between occupational stigma and psychiatrists’ attitudes toward patients remains largely unexplored, highlighting an important area for future research.
In our study, burnout did not emerge as a predictive factor for stigmatizing attitudes. However, a substantial body of research consistently demonstrates a strong association between stigma and burnout among mental health professionals (Gibb et al., Reference Gibb, Beautrais and Surgenor2010; Henderson et al., Reference Henderson, Noblett, Parke, Clement, Caffrey, Gale-Grant, Schulze, Druss and Thornicroft2014; Solmi et al., Reference Solmi, Granziol, Danieli, Frasson, Meneghetti, Ferranti, Zordan, Salvetti, Conca, Salcuni and Zaninotto2020; Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020), with some authors suggesting that stigmatizing attitudes may constitute a component of the burnout process itself (Holmqvist and Jeanneau, Reference Holmqvist and Jeanneau2006). Across specific burnout dimensions, emotional exhaustion appears to play a central role, showing a strong association with negative attitudes and the highest predictive value for stigma (Gibb et al., Reference Gibb, Beautrais and Surgenor2010; Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020). In parallel, low personal accomplishment is consistently linked to higher levels of stigma (Gibb et al., Reference Gibb, Beautrais and Surgenor2010; Solmi et al., Reference Solmi, Granziol, Danieli, Frasson, Meneghetti, Ferranti, Zordan, Salvetti, Conca, Salcuni and Zaninotto2020). Conversely, higher personal accomplishment is associated with more accepting attitudes toward patients (Holmqvist and Jeanneau, Reference Holmqvist and Jeanneau2006). Overall, these findings highlight the complexity of the relationship between burnout and stigma and underscore the need for further targeted research to clarify the underlying mechanisms.
Personal exposure to mental illness was linked to lower stigma levels among mental health professionals in our study. Those with close friends or family members affected by mental illness displayed significantly lower stigma scores. A study in Brazil similarly found that infrequent contact with a family member diagnosed with schizophrenia was associated with less stigma (Loch et al., Reference Loch, Guarniero, Lawson, Hengartner, Rössler, Gattaz and Wang2013a). These findings align with broader research indicating that personal experience, whether through one’s own mental health challenges or close relationships with those affected, plays a crucial role in reducing mental health-related stigma (Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022, Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). This supports the idea that fostering both personal and professional engagement with individuals experiencing mental illness can lead to more compassion and decreased stigma (Alexander and Link, Reference Alexander and Link2003; Henderson et al., Reference Henderson, Robinson, Evans-Lacko, Corker, Rebollo-Mesa, Rose and Thornicroft2016).
Specialists who also engage in psychotherapy demonstrated lower levels of stigma. These findings correlate with European studies, which indicate that openness to professional discussions, such as participation in case discussion groups, supervision or Balint groups, is strongly associated with more positive attitudes toward individuals with mental illness (Őri et al., Reference Őri, Szocsics, Molnár, Ralovich, Huszár, Bene, Rózsa, Győrffy and Purebl2022, Reference Őri, Szocsics, Molnár, Motlova, Kazakova, Mörkl, Wallies, Abdulhakim, Boivin, Bruna, Cabaços, Carbone, Dashi, Grech, Greguras, Ivanovic, Guevara, Kakar, Kotsis, Ingeholm Klinkby, Maslak, Matheiken, Mirkovic, Nechepurenko, Panayi, Pereira, Pomarol-Clotet, Raaj, Prelog, Soler-Vidal, Strumila, Schuster, Kisand, Reim, Ahmadova, Vircik, Kafali, Grinko, Győrffy and Rózsa2023a). Likewise, research from Turkey emphasizes the significance of psychotherapy training in reducing stigma (Yavuz et al., Reference Yavuz, Nalbant, Ulusoy, Esen, Burhan and Kara2020), suggesting that deeper involvement in therapeutic approaches promotes greater empathy and understanding.
Implications for practice
These findings carry significant implications for mental health education, policy and professional development. It is crucial to address both the occupational stigma directed at mental health professionals and the perceived stigma experienced by individuals working in the field. Strengthening the professional identity of mental health workers and enhancing the prestige of the field by emphasizing its societal contributions could play a primary role in reducing stigma. Efforts to promote recognition and respect for mental health professionals may not only improve their well-being but also contribute to more compassionate and effective patient care. In addition, stigma reduction initiatives should prioritize professionals with limited personal exposure to mental illness, incorporating programs that facilitate direct engagement with individuals who have lived experiences. Such interactions can foster empathy and challenge misconceptions.
Strengths and limitations
One of the key strengths of this study is that it is the first to investigate stigma levels toward people with mental disorders within the healthcare workforce in Kazakhstan, contributing novel insights to a previously unexplored context. The study was conducted with a sufficiently large sample size (n = 348), ensuring adequate statistical power. Another major strength is the use of the validated OMS-HC to assess stigma, which enhances the reliability and comparability of findings. Additionally, the study examined a broad range of potential determinants of stigma, allowing for a more comprehensive understanding of the factors influencing attitudes within the healthcare setting.
Despite these strengths, the study has several limitations. The cross-sectional design restricts the ability to establish causal relationships between determinants and levels of stigma. Furthermore, the use of self-reported questionnaires introduces the potential for social desirability bias, whereby participants may underreport stigmatizing attitudes or overreport socially acceptable responses. This could lead to an underestimation of the true prevalence of stigma among healthcare professionals. Although the translated version of the OMS-HC demonstrated good reliability, the lack of assessment of construct validity represents a limitation, and future studies are recommended to address this aspect. Additionally, the use of non-probability (snowball and convenience) sampling methods may have introduced selection bias, potentially attracting participants with greater interest in mental health topics or more favorable attitudes. As a consequence, the applicability of these outcomes to all healthcare professionals in Kazakhstan may be constrained, particularly for those working in more remote or resource-limited settings.
Future research directions
Further research is needed to explore stigma levels across different mental health conditions, as attitudes toward disorders such as schizophrenia, substance use disorders and other psychiatric diagnoses may vary significantly. Notably, this study found particularly high levels of stigma among narcologists, highlighting the need for focused investigation into stigma toward people with addictions. Substance use disorders often carry additional moral and societal judgments, which may exacerbate negative attitudes even among mental health professionals. Understanding the specific drivers of this elevated stigma within addiction treatment fields is crucial for developing effective, condition-specific anti-stigma interventions.
In addition, future studies should examine stigma across diverse populations, including the general public, general practitioners and other healthcare providers, to better inform targeted and population-specific strategies. Longitudinal research designs would allow for the assessment of how stigma evolves over time, particularly in response to educational or organizational interventions. Moreover, qualitative research could provide rich insights into the contextual and cultural factors that influence stigma, as well as uncover the reasons for variations in stigma across professional disciplines. Such multi-method approaches are essential to inform the development of comprehensive and sustainable stigma-reduction strategies within Kazakhstan’s healthcare system and beyond.
Conclusion
This study highlights the persistence of stigma among mental health professionals in Kazakhstan, with overall stigma levels higher than those reported in other previous studies. Key findings indicate that older professionals, those working in narcology and individuals who perceive the profession as less respectable and impactful, possess higher stigma. Gender differences were also observed, with male professionals reporting lower stigma. Additionally, those with personal experiences of mental illness and engagement in psychotherapy demonstrated lower stigma levels.
These findings emphasize the critical need for directed efforts to combat stigma, particularly for professionals working with addictions. Addressing occupational stigma, promoting psychotherapy training and strengthening the professional perception of mental health workers are essential steps toward improving attitudes toward patients with mental illness and patient care. Further research is needed to explore stigma variations across mental health conditions and different healthcare populations to develop future interventions.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10211.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10211.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors thank all respondents for their interest and voluntary participation in this study.
Author contribution
AA: Conceived and conducted the study, managed data collection, performed statistical analyses and wrote the original draft of the manuscript. YN: Conceived the study, provided methodological expertise and critically reviewed the manuscript. NY: Managed data collection and quality control, critically reviewed the manuscript. RA: Conceived the design and methodology of the study, supervised the project, revised and edited the manuscript. All authors have read and approved the final manuscript for submission.
Financial support
This research project received no financial support.
Competing interests
All authors declare no conflicts of interest.
Ethics statements
All procedures were conducted under the institutional guidelines and ethical standards. The Research Ethics Committee at the Nazarbayev University School of Medicine has reviewed and approved this study (Re:2024Nov#03).



 Open access
Open access