


Introduction
Obsessive-compulsive disorder (OCD) is characterized by the presence of obsessions (i.e. intrusive and distressing thoughts, images, impulses, or doubts) and/or compulsions (i.e. repetitive or ritualistic behaviours) (American Psychiatric Association, 2013). The disorder affects approximately 2% of the population (Ruscio et al., Reference Ruscio, Stein, Chiu and Kessler2010). Not only does OCD have wide ranging impacts on sufferers’ lives, but it also remains an important public health concern due to numerous associated societal costs (e.g. Bobes et al., Reference Bobes, González, Bascarán, Arango, Sáiz and Bousoño2001). Indeed, OCD is recognized as a major contributor to the global burden of non-fatal illness (Ayuso-Mateos, Reference Ayuso-Mateos2006). In spite of its prevalence and impact on individuals and society, the disorder is still widely misunderstood and misdiagnosed by mental health professionals (Stahnke, Reference Stahnke2021). As such, accurate and accessible measurement of OCD symptoms is integral to improving both research and clinical practice.
Several diagnostic interviews have been developed to assess OCD symptoms and diagnosis (e.g. SCID-5, First et al., Reference First, Williams, Karg and Spitzer2015; ADIS-5; Brown and Barlow, Reference Brown and Barlow2014; Y-BOCS, Goodman et al., Reference Goodman, Price, Rasmussen, Mazure, Fleischmann, Hill, Heninger and Charney1989; MINI, Sheehan et al., Reference Sheehan, Lecrubier, Sheehan, Amorim, Janavs, Weiller, Hergueta, Baker and Dunbar1998). While these are reliable and valid diagnostic tools, they often require specialized training and can be time intensive. Given their ease of administration, utility in measuring treatment response, and large normative databases, validated self-report symptom measures are more practical tools for both research and clinical use (Grabill et al., Reference Grabill, Merlo, Duke, Harford, Keeley and Geffken2008). Their utility in both research and clinical settings has contributed to the long and rich history of their development, validation, and employment in the field of OCD research and practice.
While ubiquitous today, Hodgson and Rachman (Reference Hodgson and Rachman1977) were perhaps the first to develop and validate a comprehensive OCD symptom measure with the creation of the Maudsley Obsessional Compulsive Inventory (MOCI). At the time of the development of the MOCI, the systematic identification of different domains of OCD symptomatology was lacking. As such, Hodgson and Rachman (Reference Hodgson and Rachman1977) aimed to identify distinct symptom clusters to explore differences in aetiology, prognosis, affective outcomes, and cognitive mechanisms. Their factor analysis resulted in a final questionnaire made up of 30 true/false statements which clustered onto four factors – cleaning, checking, doubting/conscientiousness and obsessional slowness. Despite its innovation and psychometric strength, several important shortcomings were identified with broader use. As a result, the Vancouver Obsessional-Compulsiveness Inventory (VOCI) was developed to address issues such as unclear wording, conceptual concerns with the slowness subscale, limited symptom scope, and lack of sensitivity to temporal change (Thordarson et al., Reference Thordarson, Radomsky, Rachman, Shafran, Sawchuk and Hakstian2004).
The VOCI expanded on the range of symptoms covered by the MOCI, informed by more recent and empirically supported concepts identified in the OCD literature, while excluding outdated content (e.g. strict parenting, obsessional slowness). This resulted in a measure composed of six subscales of OCD symptom domains – contamination, checking, obsessions, hoarding, just right, and indecisiveness. It also simplified response demands using a 5-point Likert-type scale, compared with measures like the original OCI (Foa et al., Reference Foa, Kozak, Salkovskis, Coles and Amir1998), in which items had to be rated on two separate dimensions. This design improved utility, particularly as individuals with OCD may be slow when completing questionnaires (Rachman and Hodgson, Reference Rachman and Hodgson1980).
The VOCI has been widely used in both clinical and non-clinical samples and has consistently shown excellent psychometric properties, including internal consistency (α=.94–.98), test–retest reliability (r=.91), and strong convergent and divergent validity (Radomsky et al., Reference Radomsky, Ouimet, Ashbaugh, Lavoie, Parrish and O’Connor2006; Thordarson et al., Reference Thordarson, Radomsky, Rachman, Shafran, Sawchuk and Hakstian2004). Since its publication, it has been translated and validated in multiple languages (e.g. Ghassemzadeh et al., Reference Ghassemzadeh, Shams, Meysami and Karamghadiri2016; Radomsky et al., Reference Radomsky, Ouimet, Ashbaugh, Lavoie, Parrish and O’Connor2006) and remains a practical and effective tool. That said, more than two decades have passed since the publication of the VOCI and our understanding and conceptualization of OCD symptomatology has continued to evolve. As such, an update to the VOCI to reflect our current understanding of the disorder is warranted.
Several other psychometrically sound self-report measures have been developed to assess OCD symptoms (Taylor, Reference Taylor, Swinson, Antony, Rachman and Richter1998; Overduin and Furnham, Reference Overduin and Furnham2012). For example, the Yale-Brown Obsessive-Compulsive Scale-Self Report (YBOCS-SR; Warren et al., Reference Warren, Zgourides and Monto1993), and the Dimensional Obsessive-Compulsive Scale (DOCS; Abramowitz et al., Reference Abramowitz, Deacon, Olatunji, Wheaton, Berman, Losardo, Timpano, McGrath, Riemann, Adams, Björgvinsson, Storch and Hale2010) assess the range and severity of obsessions and compulsions. The Obsessive-Compulsive Inventory-Revised (OCI-R; Huppert et al., Reference Huppert, Walther, Hajcak, Yadin, Foa, Simpson and Liebowitz2007) assesses the distress related to six symptom domains mainly related to compulsions: washing, checking, ordering, neutralizing, obsessing, and hoarding.
As the body of research on OCD has expanded, and new symptom domains have been identified, changes in our understanding of this heterogeneous condition, and updates to the diagnostic classification of OCD have occurred. One major change is the reclassification of hoarding disorder as a separate diagnosis (American Psychiatric Association, 2013; Rachman et al., Reference Rachman, Elliott, Shafran and Radomsky2009). The present study aimed to create a comprehensive and robust measure to easily assess OCD symptomatology, reflecting current findings in the literature. As such, we updated the VOCI, by retaining relevant domains (e.g. obsessions, checking) and incorporating novel domains identified in recent years (e.g. mental contamination, reassurance seeking) to develop the Vancouver Obsessional Compulsive Inventory-2 (VOCI-2). A previous attempt was made to update the VOCI with some of these newer symptom domains (i.e. Vancouver Obsessional-Compulsive Inventory-Revised; VOCI-R; Gönner et al., Reference Gönner, Ecker, Leonhart and Limbacher2010). However, important newer symptom types (i.e. mental contamination and reassurance seeking) were not considered in this version. The VOCI-2 therefore holds promise as a more accurate and also broader scale.
Symptom domains no longer relevant
Updates to diagnostic classification in the DSM-5 have deemed aspects of the VOCI no longer relevant to OCD. Historically, hoarding was included as a dimension or specific presentation of the disorder. However, hoarding disorder is its own diagnostic entity in the DSM-5 due to important differences between features of hoarding and OCD (e.g. age of onset, biological phenomena, clinical presentation, response to treatment, etc.; Abramowitz and Jacoby, Reference Abramowitz and Jacoby2015; Grisham et al., Reference Grisham, Brown, Liverant and Campbell-Sills2005; Rachman et al., Reference Rachman, Elliott, Shafran and Radomsky2009). As it is no longer considered a part of OCD, it is appropriate to exclude the hoarding subscale from the new VOCI.
Furthermore, although comprehensive, some of the VOCI subscales appear to be capturing OCD-related phenomena, rather than OCD symptoms. For instance, OCD is generally recognized as a disorder of doubt and indecisiveness (Esquirol, Reference Esquirol1838), and clearly related to various symptoms of OCD, such as checking (e.g. Frost and Shows, Reference Frost and Shows1993), although indecisiveness is not considered as a specific symptom of OCD. In the VOCI, the indecisiveness subscale has shown poor discriminant validity with other psychopathologies, suggesting that it would be better conceptualized as an OCD-related construct, perhaps an underlying feature characteristic of cognitive processes of OCD or a trait (Germeijs and Verschueren, Reference Germeijs and Verschueren2011).
Further, Thordarson et al. (Reference Thordarson, Radomsky, Rachman, Shafran, Sawchuk and Hakstian2004) described the Just Right subscale as, ‘Doing things exactly right, following strict routines, repeating, memorizing, concern with being perfect, and feeling compelled to count’ (p. 1299). Although this subscale shows good discriminant validity, it overlaps with a broad range of non-specific OCD phenomena, ranging from perfectionism (e.g. ‘I feel compelled to be absolutely perfect’) to aspects of checking (e.g. ‘I feel compelled to check letters over and over before mailing them’). Moreover, ‘just right’ experiences are increasingly understood as underlying motivators or cognitive-affective drivers that cut across multiple OCD symptom presentations, rather than being a standalone symptom dimension (Belloch et al., Reference Belloch, Fornés, Carrasco, López-Solá, Alonso and Menchón2016). For these reasons, the VOCI-2 does not include these two subscales.
Symptom domains introduced in the revised version
In addition to removing symptom subscales that might be better conceptualized as OCD-related phenomena, the VOCI-2 would benefit from the inclusion of novel OCD symptom domains identified in recent years. First, since the development of the original measure, researchers have identified mental contamination, a unique form of contamination concern in OCD (Rachman, Reference Rachman2004). As compared with the comprehensively studied contact contamination, mental contamination refers to feelings of internal dirtiness and/or washing behaviours that are provoked by thoughts, memories, images, or impulses that an individual perceives as immoral, wrong, or inappropriate, in the absence of direct contact with a contaminant. Unlike contact contamination where the source of contamination is an object, the source of mental contamination is proposed to be a person (Rachman, Reference Rachman2004). For this reason, the site of contamination is diffuse, and contamination feelings tend to persist even after washing (Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a). Several studies have demonstrated that MC is a central construct in OCD (Millar et al., Reference Millar, Coughtrey, Healy, Whittal and Shafran2023), reported by a high number of individuals with clinically elevated symptoms of OCD (Coughtrey et al., Reference Coughtrey, Shafran, Knibbs and Rachman2012a; Coughtrey et al., Reference Coughtrey, Shafran, Lee and Rachman2012b), significantly associated with contact contamination, and with a broad range of OCD-related symptoms and severity. Radomsky et al. (Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a) developed the VOCI-Mental Contamination Scale (VOCI-MC), as a supplement to the original VOCI and to measure this form of contamination symptomatology in OCD. Psychometric and experimental studies using the VOCI-MC have supported its strong reliability and validity in both clinical and analogue samples (e.g. Melli et al., Reference Melli, Carraresi, Stopani, Radomsky and Bulli2015; Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a). Its inclusion in an updated more comprehensive scale is warranted.
A historically understudied symptom profile in OCD are obsessions and compulsions related to symmetry, ordering, and arranging of objects (Taylor, Reference Taylor, Abramowitz, McKay and Storch2017). Epidemiological studies have since shown that ordering and arranging is one of the most common presentations of OCD (Bloch et al., Reference Bloch, Landeros-Weisenberger, Rosario, Pittenger and Leckman2015; Radomsky and Rachman, Reference Radomsky and Rachman2004); and that across studies, these symptoms reliably represent a singular symptom cluster in both healthy (Radomsky and Rachman, Reference Radomsky and Rachman2004) and clinical populations with OCD (Gönner et al., Reference Gönner, Ecker, Leonhart and Limbacher2010). Feelings of incompleteness and ‘not just right’ experiences are very common in OCD and have been proposed as a motivating factor for OCD-related symptoms (Taylor, Reference Taylor, Abramowitz, McKay and Storch2017), especially related to symmetry, ordering, and arranging (e.g. Coles et al., Reference Coles, Frost, Heimberg and Rheaume2003; Pietrefesa and Coles, Reference Pietrefesa and Coles2008; Starcevic et al., Reference Starcevic, Berle, Brakoulias, Sammut, Moses, Milicevic and Hannan2011; Summerfeldt, Reference Summerfeldt2004). As such, it seemed more appropriate to include a dimension including symmetry, ordering and arranging symptoms in the new measure, and although it may well overlap with the ‘just right’ construct, these symptoms do appear to be more specific to OCD than the desire to have things exactly right. The Symmetry, Ordering and Arranging Questionnaire (SOAQ; Radomsky and Rachman, Reference Radomsky and Rachman2004) was developed to serve as an optional module to supplement the VOCI (Thordarson et al., Reference Thordarson, Radomsky, Rachman, Shafran, Sawchuk and Hakstian2004). Items from this scale were included in the development of VOCI-2.
Similarly, in the past two decades, research has highlighted the important role of compulsive reassurance seeking in OCD, both as a symptom and maintaining factor. Reassurance seeking refers to the repeated solicitation of safety-related information from others, despite having already received this information (Parrish and Radomsky, Reference Parrish and Radomsky2010), and is one of the most common strategies used by individuals with OCD to alleviate their obsessional thoughts or images (Freeston and Ladouceur, Reference Freeston and Ladouceur1997). Excessive reassurance seeking has become a hallmark feature of the disorder (Halldorsson and Salkovskis, Reference Halldorsson and Salkovskis2023) but is not directly measured in any existing comprehensive OCD symptom measure. The Covert and Overt Reassurance Seeking Inventory (CORSI) was developed as a transdiagnostic tool aimed at measuring five different types of reassurance seeking behaviours (i.e. Covert Social/Relational Threat, Overt General Threat, Covert General Threat Passive, Overt Social Relational Threat, and Covert General Threat Active; Radomsky et al., Reference Radomsky, Neal, Parrish, Lavoie and Schell2021). Although total scores on the CORSI were found to be elevated in OCD, anxiety disorders, and depression, the Overt General Threat subscale – defined as seeking reassurance openly from others in response to distress from general threats – was uniquely associated with OCD, and as such, those items included in the VOCI-2.
In sum, there is a growing body of evidence demonstrating the prevalence and importance of these newer symptom domains in OCD (i.e. mental contamination, reassurance seeking, and symmetry, ordering, and arranging), with individual, psychometrically sound scales developed to measure each of these (i.e. VOCI-MC, CORSI, and the SOAQ; Radomsky and Rachman, Reference Radomsky and Rachman2004; Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a; Radomsky et al., Reference Radomsky, Neal, Parrish, Lavoie and Schell2021). There is great potential research and clinical benefit to creating a single and broad measure of OCD symptomatology that contains subscales for each of these constructs, in addition to the still-relevant symptom domains from the VOCI. The present study aimed to update the VOCI with these goals in mind, and was proposed to produce a newer, improved assessment tool (i.e. the Vancouver Obsessional Compulsive Inventory-2; VOCI-2); in so doing, we aimed to collect and provide information about its factor structure, reliability and validity. An exploratory factor analysis within a non-clinical population was conducted to determine the final number of items to be included in the VOCI-2 and its subscales.
Method
Participants
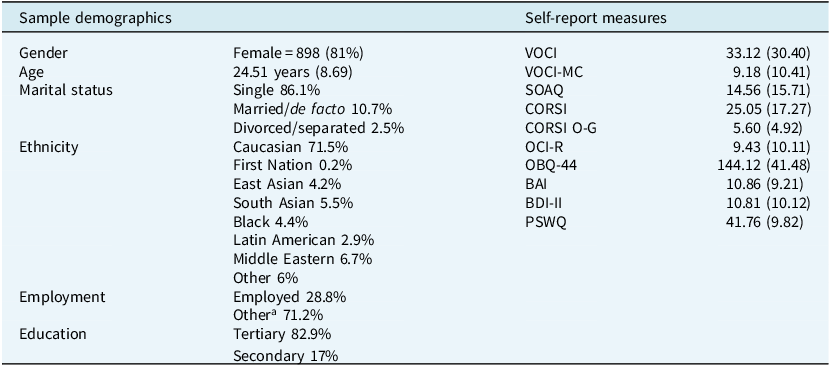
One thousand one hundred and eight undergraduate psychology participants from Concordia University (Montreal, Canada) participated in the current study for course credit. The sample consisted of 81% individuals identified as female, with a mean age of 24.51 years (SD=8.69, range 17 – 72). Demographics for these participants are provided in Table 1.
Demographics and means and standard deviations for self-report measures in the non-clinical sample (n=1108)

VOCI, Vancouver Obsessional Compulsive Inventory; VOCI-MC, Vancouver Obsessional Compulsive Inventory-Mental Contamination Scale; SOAQ, Symmetry Ordering and Arranging Questionnaire; CORSI, Covert and Overt Reassurance Seeking Inventory; O-G, Overt General Threat subscale; OCI-R, Obsessive-Compulsive Inventory-Revised; OBQ-44, Obsessive Beliefs Questionnaire-44 Item Version; BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory-Second Edition; PSWQ, Penn State Worry Questionnaire.
a Includes students and those not working, retired, and unemployed.
To establish known-groups validity, data were also collected from three clinical samples as part of a larger study (for details, see Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a); participants received financial compensation for their participation. Clinical participants were recruited through local advertisements and flyers in and around Montreal clinics, as well as via online advertisements. Clinical diagnoses were confirmed using the Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV; Brown et al., Reference Brown, Barlow and Liebowitz1994). Fifty-nine individuals had a primary diagnosis of OCD (62.7% female, mean age=39.10 years, SD=14.94). Forty-two individuals had a secondary diagnosis of a non-OCD anxiety disorder (52.4% female, mean age=41.33 years, SD=15.13), and 18 individuals had a secondary diagnosis of depression (50% female, mean age=44.06 years, SD=16.18 years). Of the 57 participants with OCD recruited for the clinical validation sample, 37 had complete data and were included in the known-groups analyses.
Materials and measures
Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV; Brown et al., 1994)
This semi-structured interview assesses a variety of symptoms associated with anxiety and other disorders (e.g. OCD, mood, somatoform, substance abuse), according to DSM-IV criteria (American Psychiatric Association, 2000). The ADIS-IV has been widely used in both clinical and research contexts (Brown et al., Reference Brown, Di Nardo, Lehman and Campbell2001) and has good to excellent inter-rater reliability when assessing depression (κ=0.67) and OCD (κ=0.85). All interviewers on the ADIS-IV had an undergraduate degree in psychology and/or were completing graduate level studies in clinical psychology. Interviewers received rigorous training on the ADIS-IV and were required to match with another interviewer’s primary and secondary diagnoses (as well as severity ratings) made on three training videos and three live interviews conducted with actual participants. These interviews were administered under the supervision of the first author (A.S.R.). To assess diagnostic reliability, a subset of 15% of all interviews conducted was audio recorded and scored by an independent rater. Agreement on diagnoses for this subset was 100% (Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a).
Vancouver Obsessional Compulsive Inventory (VOCI; Thordarson et al., Reference Thordarson, Radomsky, Rachman, Shafran, Sawchuk and Hakstian2004)
The VOCI is a 55-item self-report measure of OCD symptoms across the following six OCD symptom domains: feelings of contamination that arise from direct contact with a physical contaminant, checking, repugnant obsessions, hoarding, just right, and indecisiveness. The VOCI and its subscales have demonstrated excellent internal consistency (Cronbach’s α=.85–.94), test–retest reliability (r=.90–.96), convergent validity with other OCD symptom measures, and divergent validity with measures of general distress (Thordarson et al., Reference Thordarson, Radomsky, Rachman, Shafran, Sawchuk and Hakstian2004). Internal consistency for the subscales and total score in the current sample was excellent (Cronbach’s α=.87–.97).
Vancouver Obsessional Compulsive Inventory-Mental Contamination Scale (VOCI-MC; Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a)
The VOCI-MC is a 20-item measure of feelings of contamination that arise in the absence of direct contact with a contaminant (e.g. ‘Having an unpleasant image or memory can make me feel dirty inside’). Across both clinical and non-clinical samples, the VOCI-MC has demonstrated excellent internal consistency (Cronbach’s α=.93–.97), good convergent validity with other measures of mental contamination (r=.61–.87), and adequate divergent validity with a measure of depressive symptoms (Radomsky et al., Reference Radomsky, Rachman, Shafran, Coughtrey and Barber2014a). Internal consistency in the current sample was excellent (Cronbach’s α=.93).
Covert and Overt Reassurance Seeking Inventory (CORSI; Radomsky et al., Reference Radomsky, Neal, Parrish, Lavoie and Schell2021)
The CORSI is a 26-item measure of problematic covert and overt reassurance seeking behaviours that are motivated by the perceived general and social/relational threats relevant to many psychological disorders. The CORSI has demonstrated excellent internal consistency in both clinical and non-clinical samples (Cronbach’s α=.93), including the overt general threat (O-G) subscale, used in this study (Cronbach’s α=.90). This subscale showed significant and a strong correlation with a self-report measure of OCD (r=.65), and a moderately strong correlation with anxiety and depression, (r=.46–.48). The CORSI O-G also has good divergent validity, showing significant negative correlations with a self-report measure of self-esteem (r=–.42). Internal consistency in the current sample was excellent (Cronbach’s α=.89).
Symmetry Ordering and Arranging Questionnaire (SOAQ; Radomsky and Rachman, Reference Radomsky and Rachman2004)
The SOAQ is a 20-item self-report measure of ordering and arranging behaviours which are characteristic of OCD. The SOAQ has demonstrated excellent internal consistency in a non-clinical sample (Cronbach’s α=.96; Radomsky and Rachman, Reference Radomsky and Rachman2004). The scale has good convergent validity with the VOCI total score (r=.64) and Just Right subscale (r=.72), and good divergent validity (i.e. significantly lower correlations) with other measures of psychopathology (Radomsky and Rachman, Reference Radomsky and Rachman2004). Internal consistency in the current sample was excellent (Cronbach’s α=.97).
Obsessive-Compulsive Inventory-Revised (OCI-R; Foa et al., Reference Foa, Huppert, Leiberg, Langner, Kichic, Hajcak and Salkovskis2002)
The OCI-R is an 18-item self-report measure of OCD symptoms and was used to assess convergent validity with our new measure of OCD symptoms. The OCI-R has high internal consistencies across varying samples (Cronbach’s α=.81–.93; Foa et al., Reference Foa, Huppert, Leiberg, Langner, Kichic, Hajcak and Salkovskis2002). Internal consistency in the current sample was excellent (Cronbach’s α=.92).
Obsessive Beliefs Questionnaire-44 Item Version (OBQ-44; Obsessive Compulsive Cognitions Working Group, 2005)
The OBQ-44 is a 44-item self-report measure of the beliefs associated with OCD symptomatology: responsibility and threat estimation, perfectionism and intolerance of uncertainty, and importance and control of thoughts. Internal consistency of the total score was excellent for a sample with clinical and non-clinical participants (Cronbach’s α=.95; Obsessive Compulsive Cognitions Working Group, 2005) and similar to the current sample (Cronbach’s α=.95).
Beck Anxiety Inventory (BAI; Beck and Steer, Reference Beck and Steer1990)
The BAI is a 21-item measure of the physical symptoms associated with anxiety (e.g. numbness or tingling). It has excellent internal consistency (Cronbach’s α=.92; Beck et al., Reference Beck, Epstein, Brown and Steer1988) that was comparable in the current non-clinical sample (Cronbach’s α=.92).
Beck Depression Inventory – Second Edition (BDI-II; Beck et al., Reference Beck, Steer and Brown1996)
The BDI-II is a 21-item self-report measure of the severity of depressive symptoms. It has excellent internal consistency (Cronbach’s α=.92–.93; Beck et al., Reference Beck, Steer and Brown1996) that was comparable in the current sample (Cronbach’s α=.93).
Penn State Worry Questionnaire (PSWQ; Meyer et al., Reference Meyer, Miller, Metzger and Borkovec1990)
The PSWQ is a 16-item self-report measure of excessive worry that characterizes generalized anxiety disorder. The internal consistency of the total score is excellent across clinical and non-clinical samples (Cronbach’s α=.91–.95; Meyer et al., Reference Meyer, Miller, Metzger and Borkovec1990). Internal consistency was lower in the current sample (Cronbach’s α=.81).
Procedure
Participants who signed up via Concordia University’s research participation pool were emailed a link to the current study, which was hosted online by the Checkbox software program that was maintained by Concordia University. Clinical participants were first administered the ADIS-IV before accessing this link on the laboratory computer. The link led participants to answer a series of demographic questions followed by a battery of questionnaires including the full versions of the VOCI, VOCI-MC, SOAQ, and the CORSI overt general threat subscale, as the core instruments for the factor analysis. The OCI-R, OBQ-44, BDI-II, BAI, and PSWQ were also included for convergent and divergent validity, as validated measures of OCD, anxiety, depression, and worry. The questionnaires were presented in one of two randomized orders. A subset of the non-clinical sample (n=127) was invited to complete the same battery of questionnaires a second time one month later. Finally, participants were debriefed, thanked, and compensated for their participation.
Results
Factor structure analyses, and subsequent internal consistency, retest reliability, and convergent/discriminant validity analyses are based on the non-clinical sample only. The sample size in this study provides excellent power and stability, exceeding recommended ratios for factor analysis (Mundfrom et al., Reference Mundfrom, Shaw and Ke2005). Several outliers were detected in the VOCI-2 subscales and the potential effects of these extreme responses were reduced by winsorizing them at the 98th percentile.
Factor structure of the VOCI-2
In order to attain the most robust structure for the new measure, an exploratory factor analysis (EFA) (principal axis factoring extraction, oblimin rotation) in SPSS 26 was conducted on the 78 items resulting from the integration of the scales and subscales that were employed to be part of the new measure: VOCI obsessions (12 items), VOCI checking (6 items), VOCI contamination (12 items), VOCI-MC (20 items), CORSI Overt-General threat subscale (8 items), and SOAQ (20 items). Analysis revealed a 10-factor solution with eigenvalues greater than 1. Due to the tendency of Kaiser’s rule to over-estimate the number of factors (Horn, Reference Horn1965), a scree test of the eigenvalues and a parallel analysis were conducted to determine the optimal number of factors to retain. The analyses revealed a tentative 7-factor model with eigenvalues greater than 1, explaining a substantial portion of the variance. An examination of the item loadings revealed four items of the VOCI-MC (15, 7, 11, and 5) that loaded on two factors, presenting lower values (from .33 to .39) in a 7th factor. This solution explained 56.60% of the variance.
The most parsimonious and interpretable solution was a 6-factor structure reflecting the number of symptom categories included in the analysis. A new EFA was conducted forcing the number of factors to extract to 6. This solution explained 52.53% of the variance (KMO=.970; Bartlett’s test of sphericity: 58522, p≤.001), with eigenvalues of 25.2, 6.6, 3.6, 3.3 and 2.7 for mental contamination; symmetry, ordering and arranging; obsessions; checking; reassurance seeking; and contact contamination, respectively.
To shorten the new measure, we reduced the number of items per subscale to 5, retaining those that loaded the highest in their factor. To accomplish this, items that loaded above .2 on more than one factor were first removed. Items 2, 10, 11, 15, 17, 18, 19 and 20 from the VOCI-MC, item 49 from VOCI contamination, and item 46 from VOCI obsessions were eliminated via this process. Some overlapping occurred among these three factors: VOCI contamination, VOCI obsessions, and VOCI-MC. Although item 44 from the VOCI contamination subscale (‘One of my major problems is that I am excessively concerned about cleanliness’) also loaded highly on the VOCI-MC and the SOA subscales; it reflected a prominent symptom of the contamination subtype and so we decided to retain it. Next, items that were similar regarding their wording (e.g. ‘I often feel dirty inside my body’ vs ‘I often feel dirty under my skin’) to an item already retained (despite loading highly in the factor) were also excluded. This was the case for items 6 and 12 from VOCI-MC, item 7 from VOCI checking, item 50 from VOCI contamination, and items 4 and 9 from SOAQ. Next, items that appeared too specific (e.g. ‘Touching the bottom of my shoes makes me very anxious’) or outdated, despite loading highly in its factor (e.g. ‘I avoid using public telephones …’) were also removed and substituted with the next highest-loading item according to the EFA. This was the case for items 15 and 25 from VOCI contamination, and item 30 from VOCI obsessions. Finally, items that loaded less than the items already retained were eliminated. Items 1, 4, 5, 7 and 13 from VOCI-MC (<.60); 2, 6, 16, 27 and 28 from VOCI obsessions (<.65); 3, 8 and 32 from VOCI contamination (<.58); 3, 15 and 24 from CORSI overt general threat (<.70); and 1, 2, 3, 5, 6, 7, 12, 13, 16, 17, 18, 19 and 20 from SOAQ (<.78) were removed via this process.
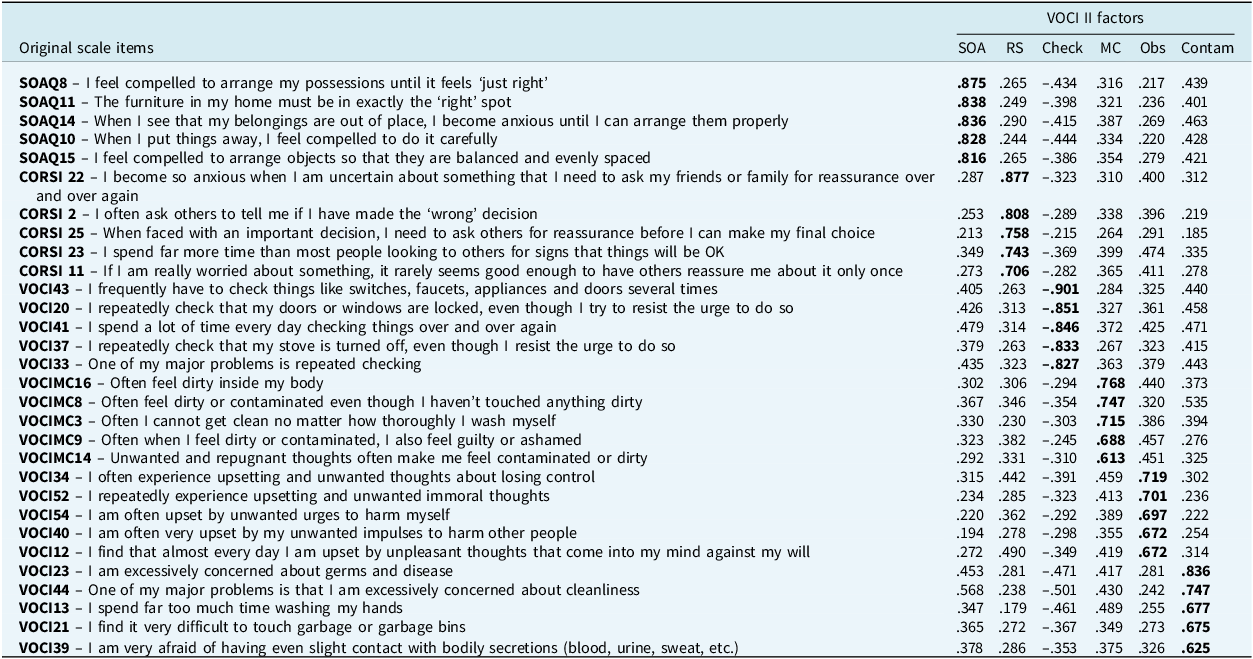
The final VOCI-2 consists of six subscales, with five items in each subscale (see Table 2): Symmetry, Ordering and Arranging; Reassurance Seeking; Checking; Mental Contamination; Obsessions explaining a substantial portion of the variance; and Contact Contamination. An additional EFA was conducted to analyze the structure of the VOCI-2 (KMO=.941; Bartlett’s test of sphericity: 20145, p≤.001). The total variance explained was 60.4%, and the variance explained by each factor was 35.5%, 10.0%, 7.0%, 6.5%, 5.1% and 3.9%, respectively.
Factor loadings of the Vancouver Obsessional Compulsive Inventory-2 (VOCI-2; n=1108)

VOCI, Vancouver Obsessional Compulsive Inventory; VOCI-MCS, Vancouver Obsessional Compulsive Inventory-Mental Contamination Scale; SOAQ, Symmetry Ordering and Arranging Questionnaire; CORSI, Covert and Overt Reassurance Seeking Inventory; SOA, symmetry, ordering and arranging; RS, reassurance seeking; Check, checking; MC, mental contamination; Obs, obsessions; Contam, contact contamination.
Internal consistency
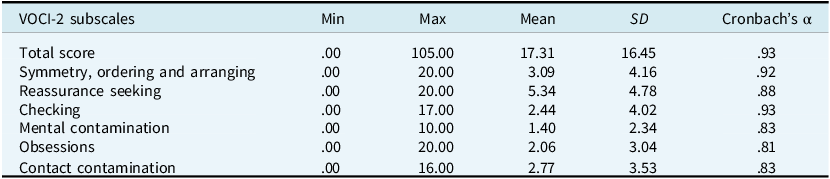
Cronbach’s α’s are presented in Table 3. Internal consistency of VOCI-2 subscales and the total scale were good (all values above .81). Correlation coefficients between subscales ranged between .28 and .49 (p≤.001), and between subscales and the total score ranged from .62 to .74 (p≤.001), indicating moderate associations among subscales and strong relationships with the overall construct.
Descriptive data and reliability of the Vancouver Obsessional Compulsive Inventory-2 (VOCI-2; n=1108)

Retest reliability
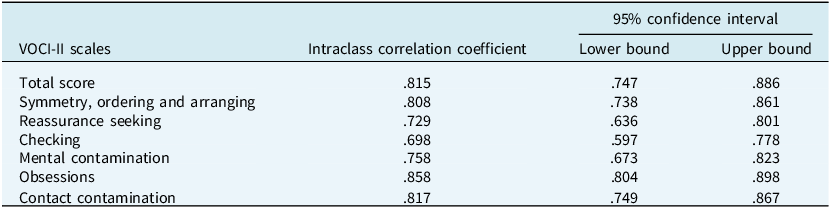
Retest reliability estimates were based on 127 participants. The mean retest interval was 29.54 days (SD=5.73). A ∼30-day retest interval was used, consistent with prior studies of OCD symptom scales [e.g. the Obsessive-Compulsive Inventory-Revised (OCI-R) demonstrated acceptable test–retest reliability over a 4-week interval]. Retest reliability estimates (intraclass correlation coefficients) for the VOCI-2 total scale and subscales are presented in Table 4. Spearman correlation coefficients for VOCI-2 total and subscale scores indicated good reliability, with values ranging from .69 to .85 (p≤.001).
Intraclass correlation coefficients (ICC) for retest reliability of the Vancouver Obsessional Compulsive Inventory-2 (VOCI-2; n=127)

Convergent and divergent validity
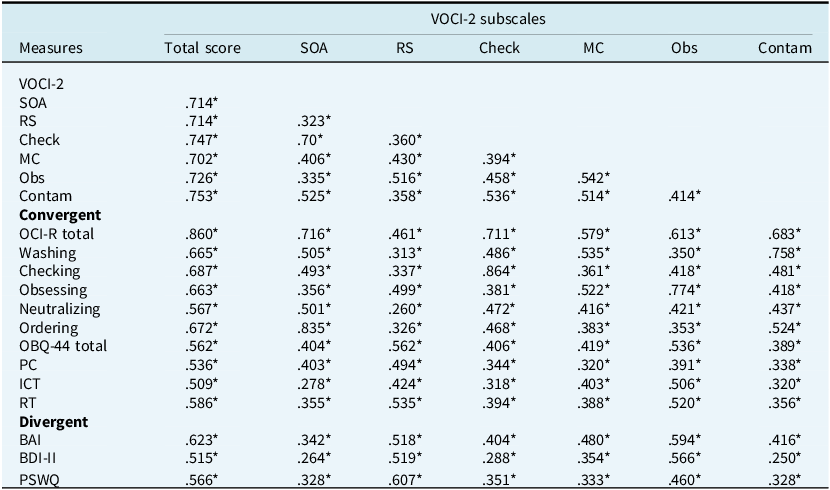
To examine the convergent validity of the new measure, we conducted Spearman correlation analyses between VOCI-2 total and subscale scores, and the OCI-R and OBQ total and subscale scores. As shown in Table 5, results revealed significant and robust correlations between the VOCI-2 total score and all convergent measures, and moderate to high correlations between VOCI-2 subscales and OCI-R and OBQ total and subscale scores. To examine the divergent validity of the VOCI-2, correlations with the BDI-II, BAI, and PSWQ were conducted. Moderate to high correlations were found between VOCI-2 and these non-OCD measures. Steiger’s Z test (Steiger, Reference Steiger1980) for comparing dependent correlations (Hoerger, Reference Hoerger2013) was used to compare the coefficients and found significant differences between the VOCI-2 and OCI-R total scores correlation and VOCI-2 and BAI correlation (r=0.860 vs r=0.623, Z=15.24, p<.001), BDI-II correlation (r=0.860 vs r=0.515, Z=18.71, p<.001), and PSWQ (r=0.860 vs r=0.566, Z=17.02, p<.001). To verify these results, analyses were also conducted in the OCD sample (n=37), with significant differences in the correlation scores as well: VOCI-2 and OCI-R total scores correlation and VOCI-2 and BAI correlation (r=0.849 vs r=0.661, Z=2.28, p=.023), BDI-II correlation (r=0.849 vs r=0.525, Z=3.14, p=.002), and PSWQ (r=0.849 vs r=0.609, Z=2.59, p=.009).
Pearson correlations between VOCI-2 subscales, and with convergent and divergent measures (n=1108)

SOA, symmetry, ordering and arranging; RS, reassurance seeking; Check, checking; MC, mental contamination; Obs, obsessions; Contam, contact contamination; OCI-R, Obsessive-Compulsive Inventory-Revised; OBQ-44, Obsessive Beliefs Questionnaire-44 Item Version (PC, Perfectionism and Intolerance of Uncertainty; ICT, Importance and Control of Thoughts; RT, Responsibility and Threat Estimation); BAI, Beck Anxiety Inventory; BDI-II, Beck Depression Inventory; PSWQ, Penn State Worry Questionnaire. *p<.001.
Known-groups validity
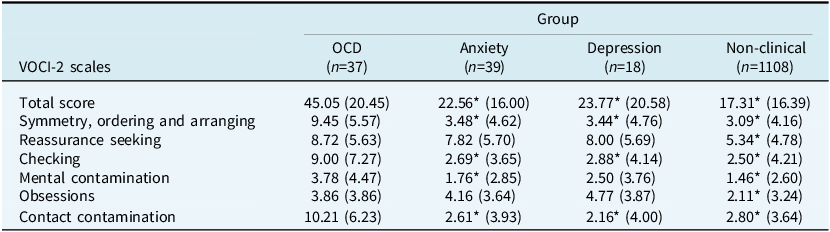
For each scale, we compared the mean score for the OCD sample with the mean for the non-clinical, non-OCD anxiety, and depression samples, using the Dunnett method of multiple comparisons, with α<.05, non-directional (see Table 6). Participants with OCD scored significantly higher than the non-clinical sample on the total and all subscale scores. Regarding the clinical samples, OCD participants scored higher than non-OCD anxiety and depression groups in checking, contact contamination, and symmetry, ordering and arranging subscales, and VOCI-2 total score, but not in obsessions, mental contamination, or reassurance seeking subscales.
Group means and standard deviations on the Vancouver Obsessional Compulsive Inventory-2 (VOCI-2; n=1202)

*Indicates means significantly different from OCD mean using the Dunnett method of multiple comparisons, α<.05.
Discussion
The aim of the present study was to revise and update the VOCI to provide a comprehensive, robust, and contemporary measure to easily assess OCD symptomatology, reflecting up-to-date research findings about symptom domains in the literature. Given its limitations, the hoarding, indecisiveness, and ‘just right’ subscales were removed from the measure, and three other subscales were added: mental contamination; symmetry, ordering and arranging; and reassurance seeking. These scales were developed to measure more novel OCD symptoms that are increasingly recognized to be relevant to the disorder.
We identified six distinctive factors corresponding to the revised symptom domains: symmetry, ordering and arranging; reassurance seeking; checking; mental contamination; obsessions; and contact contamination. Our new measure, the VOCI-2, is composed of 30 items, and as with the original VOCI, is freely available for public use. The internal consistency of the VOCI-2 subscales was excellent, and as expected, the low to moderate correlations between them suggest that they assess different aspects of OCD phenomenology. The retest reliability of the VOCI-2 subscales was adequate after 30 days, indicating that the measure is stable over time.
Convergent validity of the VOCI-2 was excellent, with total and subscale scores showing strong correlations with OCD measures (OCI-R, OBQ), especially with the distress caused by symptoms. Higher correlations were observed between VOCI-2 obsessions, checking, contact contamination, and symmetry, ordering and arranging subscales and their OCI-R counterparts. Reassurance seeking and obsessions were strongly related to OCD-relevant beliefs, particularly responsibility and threat estimation. Divergent validity was supported. Although moderate to high correlations were found with measures of anxiety, depression, and worry, the correlations between the VOCI-2 and OCI-R were significantly stronger than those between the VOCI-2 and the divergent measures. Given the common co-occurrence of these symptoms in clinical populations, the correlations between OCD and mood and anxiety measures are not completely unexpected. Specifically, past research has found that as many as 75% of individuals with OCD symptoms have also experienced subclinical or clinical dysphoric states (Black et al., Reference Black, Noyes, Goldstein and Blum1992). Reassurance seeking is a common safety behaviour for those suffering from OCD and other anxiety problems such as social, generalized and health anxiety disorders (e.g. Cougle et al., Reference Cougle, Fitch, Fincham, Riccardi, Keough and Timpano2012; Rector et al., Reference Rector, Katz, Quilty, Laposa, Collimore and Kay2019), aimed at reducing anxiety and preventing harm more generally (Rachman, Reference Rachman2002; Salkovskis and Warwick, Reference Salkovskis and Warwick1986), as well as a strategy used for coping with negative intrusive thoughts in individuals with OCD (Morillo et al., Reference Morillo, Belloch and Garcia-Soriano2007). The inclusion of only the CORSI overt general threat items may provide some specificity to OCD, as shown in earlier validation work (Radomsky et al., Reference Radomsky, Neal, Parrish, Lavoie and Schell2021).
Known-groups validity was examined across four different samples. Between-group differences in VOCI-2 scores supported the validity for the total and subscale scores when the OCD group was compared with non-clinical participants; but only the VOCI-2 total score, checking, contact contamination, symmetry, ordering and arranging subscales were significantly higher in the OCD group relative to the non-OCD clinical samples. There was no evidence for significant differences in obsessions, mental contamination and reassurance seeking subscale scores between the three clinical groups. Intrusive thoughts, precursors of obsessions according to cognitive behavioural theories of OCD, are common experiences among individuals with and without OCD (e.g. Rachman, Reference Rachman1997; Rachman, Reference Rachman1998; Radomsky et al., Reference Radomsky, Alcolado, Abramowitz, Alonso, Belloch, Bouvard, Clark, Coles, Doron, Fernández- Álvarez, Garcia-Soriano, Ghisi, Gomez, Inozu, Moulding, Shams, Sica, Simos and Wong2014b). Different studies have looked at the specificity of the cognitive contents to OCD and anxiety disorders (e.g. Coles et al., Reference Coles, Mennin and Heimberg2001; Inozu et al., Reference Inozu, Bikem Hacıömeroğlu, Keser, Akın-Sarı and Özmenler2021), and while differences in frequency, intensity, and controllability have been observed, intrusive thoughts of individuals with OCD, anxiety disorders and non-clinical individuals have been found to be similar in content. In a similar way, the results regarding reassurance seeking are not unexpected as reassurance seeking is a key factor in the persistence of anxiety in individuals with anxiety disorders (e.g. Halldorsson and Salkovskis, Reference Halldorsson and Salkovskis2023; Rector et al., Reference Rector, Katz, Quilty, Laposa, Collimore and Kay2019), and a vulnerability factor for the development of depressive symptoms (e.g. Joiner and Metalsky, Reference Joiner and Metalsky2001; Starr and Davila, Reference Starr and Davila2008). This may also have been a result of the high rates of co-morbidity between OCD, depression, and other anxiety disorders. Although not significant, individuals with OCD did score higher than the clinical groups in mental contamination. Given the small sample size, especially in the depressed group, there may have been insufficient power to detect significant differences on this subscale. Selected VOCI-2 subscales such as reassurance seeking and mental contamination could be used to detect these phenomena in other psychological problems like anxiety disorders, body dysmorphic disorder, or depression. Taken together, these findings suggest that the VOCI-2 is able to discriminate between individuals with and without OCD, particularly on the total score and several symptom-specific subscales.
A weakness of the exploratory factor analysis used in the current study is that our primary sample was composed of non-clinical individuals and thus limits the generalizability of the results. Additionally, participants were financially rewarded, and no attention check was included, which may have somewhat affected data quality. Future studies validating the VOCI-2 in a larger OCD sample are necessary to confirm the current study’s results, establish test–retest reliability in a clinical sample, and compare the measure with other well-established instruments. In connection with this, conducting a sensitivity and specificity analysis (e.g. ROC analysis) to establish clinical cut-off scores would also be helpful. In contrast, a strength of the current study is our known-groups validity analyses, which showed that the VOCI-2 was able to discriminate between individuals with and without OCD. Future research should aim to replicate these findings in larger clinical samples.
In order to provide a brief, comprehensive questionnaire, a substantial number of items was removed. As the items stemmed from previously validated and well-established measures, the original measures (i.e. CORSI, VOCI-MC, and the SOAQ) could be administered as follow-up measures when more detailed information about a participant’s or client’s specific symptomatology is required and/or when a particular subscale score is high.
We are delighted to report that the VOCI-2 is a sound questionnaire. Its items derive from well-validated and widely used scales, and its reliability as a single questionnaire has been established in this study. The heterogeneity of OCD is reflected in this questionnaire. Having a short and easy-to-use measure to assess the presence of the varied OCD symptom categories is an advantage in both clinical and research settings. Using the VOCI-2 would reduce the administration time, while providing an up-to-date measure of OCD-related dimensions. Finally, individuals with OCD tend to experience a range of symptoms concurrently, and the VOCI-2 could help to promptly detect the presence of other OCD distressing symptoms, and given its comprehensiveness and length, and retest validity over a one-month timeframe, it is likely suitable for monitoring progress in therapy. Our hope is that it will be useful to both scientists and practitioners in the field.
Practitioner points
-
- The VOCI-2 is brief, reliable, and easy to use for assessmentand treatment progress monitoring.
-
- The updated measure captures a broader range of OCD symptom domains, including mental contamination and reassurance seeking.
-
- The VOCI-2 reflects OCD’s heterogeneity, helping clinicians better identify and target relevant symptoms in treatment.
Supplementary material
To view supplementary material for this article, please visit https://doi.org/10.1017/S1352465826101325
Data availability statement
The data that support the findings of this study are available on request from the corresponding author (A.R.).
Acknowledgements
Although S. (Jack) Rachman died before this manuscript could be written, he was an integral part of the conception of this project. He contributed to discussions about which scales and subscales should be added and removed to/from the original VOCI, and as such, is listed as a co-author. We are grateful for his contributions to this study, as well as his broader contributions to the field.
Author contributions
A. Radomsky: conceptualization, methodology, resources, supervision, writing – review & editing; M. Giraldo-O’Meara: formal analysis, methodology, visualization, writing – original draft & review & editing; S. Krause: formal analysis, writing – original draft & review & editing; S. Lavoie: project administration; H. Levy: investigation, writing – review & editing; S.F. Wong: writing – original draft & review & editing; D. Thordarson: Conceptualization, writing – review & editing; S. Rachman: Conceptualization.
Financial support
This research study was not supported by any specific fund or grant.
Competing interests
The authors declare that they have no competing interests.
Ethical standards
The research has conformed to the Declaration of Helsinki. Study procedures were assessed and approved by Concordia University Research Ethics Committee (reference: HREC-UH2006-080-3).



 Open access
Open access
Comments
No Comments have been published for this article.