


Introduction
Breastfeeding is very important in the entire growth and development process (Wang et al., Reference Wang, Zhao, Zhang, Li and Cong2021). Breastfeeding is also the optimal method to reduce morbidity and mortality in children (Agampodi et al., Reference Agampodi, Dharmasoma, Koralagedara, Dissanayaka, Warnasekara, Agampodi and Perez-Escamilla2021). The World Health Organization (WHO) recommends that breastfeeding should start within the first hour after birth, that infants should be only breastfed until they are 6 months old, and that infants should be breastfed for at least 2 years (World Health Organization, 2021). In the last decade, the prevalence of only breastfeeding for infants in the first 6 months has increased by 10%, reaching 48% worldwide (World Health Organization, 2023). The WHO has targeted breastfeeding rates to be 70% by 2030. To achieve this breastfeeding goal, the barriers women and their families face to breastfeeding must be eliminated (World Health Organization, 2023). To increase breastfeeding rates, interventions that can empower mothers and encourage effective breastfeeding are needed (Sinha et al., Reference Sinha, Chowdhury, Sankar, Martines, Taneja, Mazumder, Rollins, Bahl and Bhandari2015). Successful breastfeeding is influenced by several psychological factors, including mothers’ attention to breastfeeding, breastfeeding education for mothers, perceived support for breastfeeding, breastfeeding self-efficacy, and breastfeeding empowerment. Breastfeeding self-efficacy and breastfeeding empowerment are psychological and motivational factors that influence the continuity and success of breastfeeding (Mohammadi et al., Reference Mohammadi, Kohan and Heidari2022). Therefore, it is very important and necessary to use a valid and reliable tool to strengthen breastfeeding. Many scales have been developed and used in this direction (Tokat et al., Reference Tokat, Okumuş and Dennis2010; Ekşioğlu and Çeber, Reference Ekşioğlu and Çeber2011). It is also a very important parameter for breastfeeding success in evaluating breastfeeding problems and adequacy. There are scales developed in this direction and are used today (Dolgun et al., Reference Dolgun, İnal, Erdim and Korkut2018). These tools developed to evaluate breastfeeding do not evaluate many parameters together, such as adequate breastfeeding knowledge and skills, perceived breastfeeding adequacy, belief in breastfeeding, ability to overcome breastfeeding problems, efforts to receive family support, and breastfeeding self-efficacy (Dolgun et al., Reference Dolgun, İnal, Erdim and Korkut2018; Mohammadi et al., Reference Mohammadi, Kohan and Heidari2022). Moreover, these tools are quite limited. The challenges mothers face with breastfeeding have not been addressed in detail. Furthermore, there are a significant number of women of childbearing age in our country who need breastfeeding support. Given that these women marry young and that first-time mothers are less likely to breastfeed, having tools that address this issue would make the work of healthcare professionals easier. The low breastfeeding rates in our country also highlight the need for a tool on this topic. (TUIK, 2023; Alan, Reference Alan2025). In this study, it was aimed to establish the validity and reliability of the ‘Mothers’ Breastfeeding Empowerment Scale’.
Method
Type of study
The research was conducted methodologically. The reliability and validity of the Breastfeeding Empowerment Scale (Mohammadi et al., Reference Mohammadi, Kohan and Heidari2022) developed by Mohammadi et al. was tested.
Determination of the population and sample
The population consisted of all mothers who applied to a hospital. The sample consisted of mothers who had infants between 1 and 6 months of age, who did not have any problems that would prevent them from participating in the study, who were breastfeeding, and who volunteered to participate in the study (n = 377). The number of samples was determined by calculating the number of items in the scale (37 × 10 = 370). However, the study was completed by reaching 377 people. Additionally, Kaiser-Meyer-Olkin (KMO) = 0.942, Chi-square = 5989.701, p = 0.001 values gave very strong results. The information in the literature supports determining the sample in this way (Ercan and Kan, Reference Ercan and Kan2004; Vefikuluçay Yılmaz and Terzioğlu, Reference Vefikuluçay Yılmaz and Terzioğlu2011; Seçer, Reference Seçer2015). Power calculations were performed using the study by Mohammadi et al. (Reference Mohammadi, Kohan and Heidari2022). The sample size for the power analysis was calculated using the G*Power programme. The first error type was 0.05, the Cohen’s effect size was 0.3, and the sample size was 242. Based on these inputs, the calculated power was found to be 95%. But, taking into account data losses and other analyses, this study was completed with 377 people.
Collection of research data
Research data was collected with the following forms and scales.
Question form: This form includes demographic data of the mother and infant and questions about breastfeeding.
It was tested scale for validity and reliability
Mothers’ Breastfeeding Empowerment Scale (MBES): The scale was developed by Mohammadi et al. (Mohammadi et al., Reference Mohammadi, Kohan and Heidari2022) There are no reverse-coded questions in the scale items. The scale can be applied to mothers who have infants aged between 1 and 6 months and who are breastfeeding. The scale is evaluated in Likert-type scale. The scale is scored as: strongly disagree (1), disagree (2), undecided (3), agree (4), strongly agree (5). The scale has 37 items in total. The scale consists of 6 sub-dimensions: Adequate breastfeeding knowledge and skill (1–11 items), perceived breastfeeding adequacy (12–15 items), informed belief in breastfeeding value (16–22 items), overcoming breastfeeding problems (23–29 items), negotiation for receiving family support (30–34 items), and breastfeeding self‑efficacy (35–37 items). As the score increases, breastfeeding power increases. (Mohammadi et al., Reference Mohammadi, Kohan and Heidari2022). Cronbach’s alpha values for the scale and its sub-dimensions were found as follows: Adequate breastfeeding knowledge and skill: 0.88, perceived breastfeeding adequacy: 0.78, informed belief in breastfeeding value: 0.77, overcoming breastfeeding problems: 0.77, negotiation for receiving family support: 0.77, breastfeeding self‑efficacy: 0.77, whole scale: 0.93.
Scale used as parallel from
Breastfeeding Self-Efficacy Scale (BSES): It is a scale consisting of 33 items developed by Dennis to measure breastfeeding self-efficacy. It includes the determination of mothers’ breastfeeding skills and their beliefs and behaviours regarding breastfeeding. The validity and reliability study of the Turkish form of the scale was conducted by Ekşioğlu and Çeber (Reference Ekşioğlu and Çeber2011). All items are preceded by the phrase ‘I can always’ and anchored with a 5-point Likert-type scale where 1 indicates not at all confident and 5 indicates always confident. As recommended by Bandura (1977), all items are presented positively, and scores are summed to produce a range from 33 to 165, with higher scores indicating higher levels of breastfeeding self-efficacy. Content validity of the BSES was based on the literature, interviews with breastfeeding mothers, and expert judgement using a method recommended. After a pilot test, an initial psychometric assessment was conducted with a convenience sample of 130 Canadian breastfeeding women who completed questionnaires in-hospital and at 6 weeks postpartum (Dennis and Faux, Reference Dennis and Faux1999). Cronbach’s alpha coefficient for the scale was 0.96, with 73% of all corrected item-total correlations ranging between 0.30 and 0.70. Responses were subjected to principal components analysis with a varimax rotation, yielding the theorized technique and intrapersonal subscales. Technique is defined as the physical action a mother performs and represents certain tasks necessary for successful breastfeeding. Intrapersonal thoughts are defined as a mother’s perceptions of breastfeeding and include attitudes and beliefs related to a successful breastfeeding experience. Support for predictive validity was demonstrated through significant differences in BSES scores and infant feeding patterns at 6 weeks postpartum. In the current study, the BSES was completed at 1, 4, and 8 weeks postpartum (Dennis and Faux, Reference Dennis and Faux1999; Ekşioğlu and Çeber, Reference Ekşioğlu and Çeber2011).
Analysing data
The data obtained within the scope of the study were transferred to the computer environment, and Statistical Package for Social Sciences (SPSS) 25.0 and LISREL 8.80 package programmes were used for statistical analysis. In descriptive statistics, number, percentage, mean, and standard deviation values were used. Content validity was evaluated with the content validity index (CVI), which was agreed upon by experts. For construct validity, EFA, CFA, and CFA fit indices were examined. Before factor analysis, the sample size was decided using KMO and Bartlett’s Sphericity test. For the reliability study of the scale, Cronbach’s alpha coefficient and Pearson correlation coefficients were examined.
Application of research
First, permission was obtained from the researchers who developed MBES. Later, the scale was translated into Turkish. Then, a pilot study was conducted to check the face validity of the translated scale, and it was evaluated whether the items of the scale were understood. Additionally, 10 experts were consulted to evaluate the scale. These experts evaluated whether the scale was suitable for Turkish society and whether it was necessary for breastfeeding success. Experts stated that the scale was appropriate and that it would be useful to conduct this study. Then, data was collected to analyse the scale between 01 August 2023 and 05 October 2023. After data was collected, the construct validity of the scale was evaluated with factor analysis and reliability analyses were performed.
Ethics of research
Ethics committee approval was obtained from the Ethics Committee of a University. Written and verbal consent was obtained from the mothers. The research was conducted in accordance with the Principles of the Declaration of Helsinki.
Results
Participants
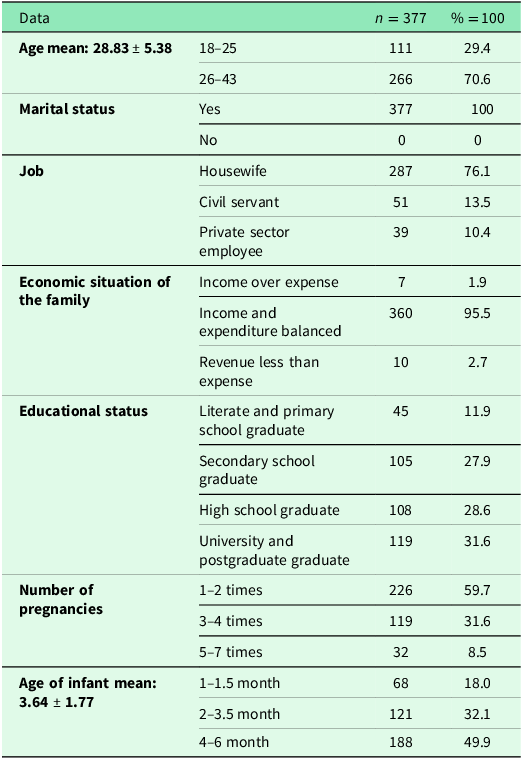
While 49.9% of the infants were between 4–6 months old, the average age of the infants was determined as 3.64 ± 1.77. While 70.6% of the mothers participating in the study were between the ages of 26–43, the average age of the mothers was 28.83 ± 5.38. It was found that of the mothers, 100% were married, 76.1% were housewives, 95.5% had a moderate economic status, 31.6% were university graduates or had postgraduate education, and 59.7% had 1 or 2 pregnancies (Table 1).
Characteristics of mothers and infants and questions regarding breastfeeding

Validity
Language adaptation
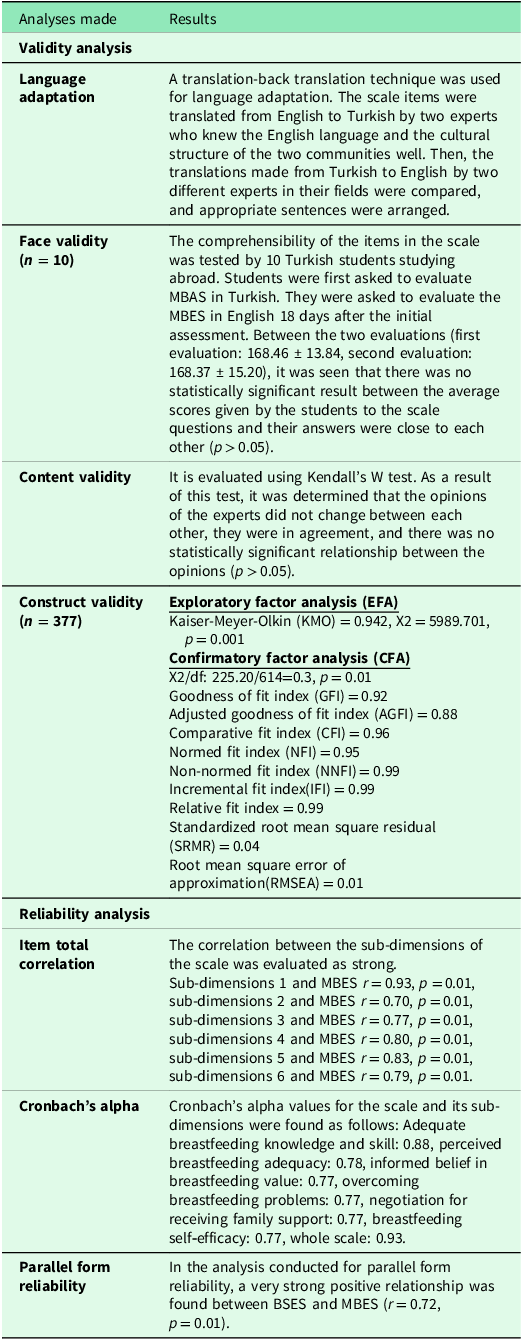
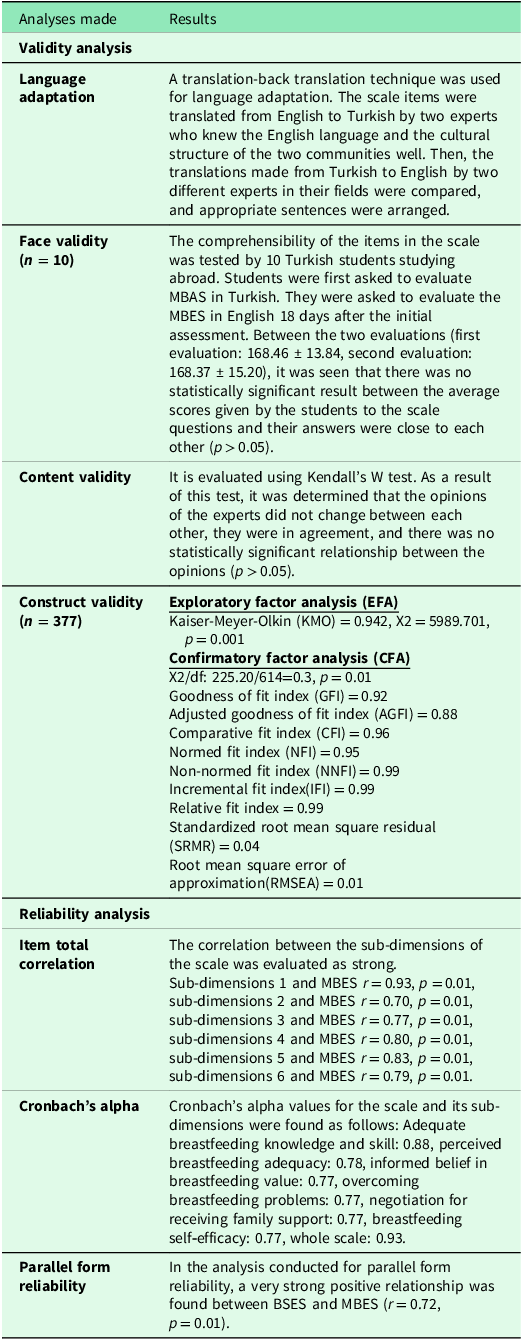
The suitability of the translation was determined as appropriate by expert opinion. Additionally, the statements sent to the owner of the scale were approved by the owner of the scale (Table 2).
Validity and reliability analyses of MBES
Face validity
The comprehensibility of the items in the scale was tested by 10 Turkish students studying abroad. Students were first asked to evaluate MBAS in Turkish. They were asked to evaluate the MBES in English 18 days after the initial assessment. Between the two evaluations (first evaluation: 168.46 ± 13.84, second evaluation: 168.37 ± 15.20), it was seen that there was no statistically significant result between the average scores given by the students to the scale questions and their answers were close to each other (p > 0.05) (Table 2).
Content validity
As a result of this test, it was determined that the experts’ opinions did not change from each other, they agreed, and there was no statistically significant relationship between the opinions (p > 0.05). Experts rated the scale items (1 point) between much change needed and (4 points) as very appropriate. It was determined that the average score given to the scale items by the experts was between 3.81 ± 0.60 and 4.00 ± 0.00 points. CVI of 0.95 was determined, demonstrating very good content validity (Table 2).
Construct validity
Exploratory factor analysis (EFA): Kaiser-Meyer-Olkin (KMO) = 0.942, Chi-square = 5989.701, p = 0.001 values gave very strong results. It was decided that other analyses could be started based on these values (Table 2).
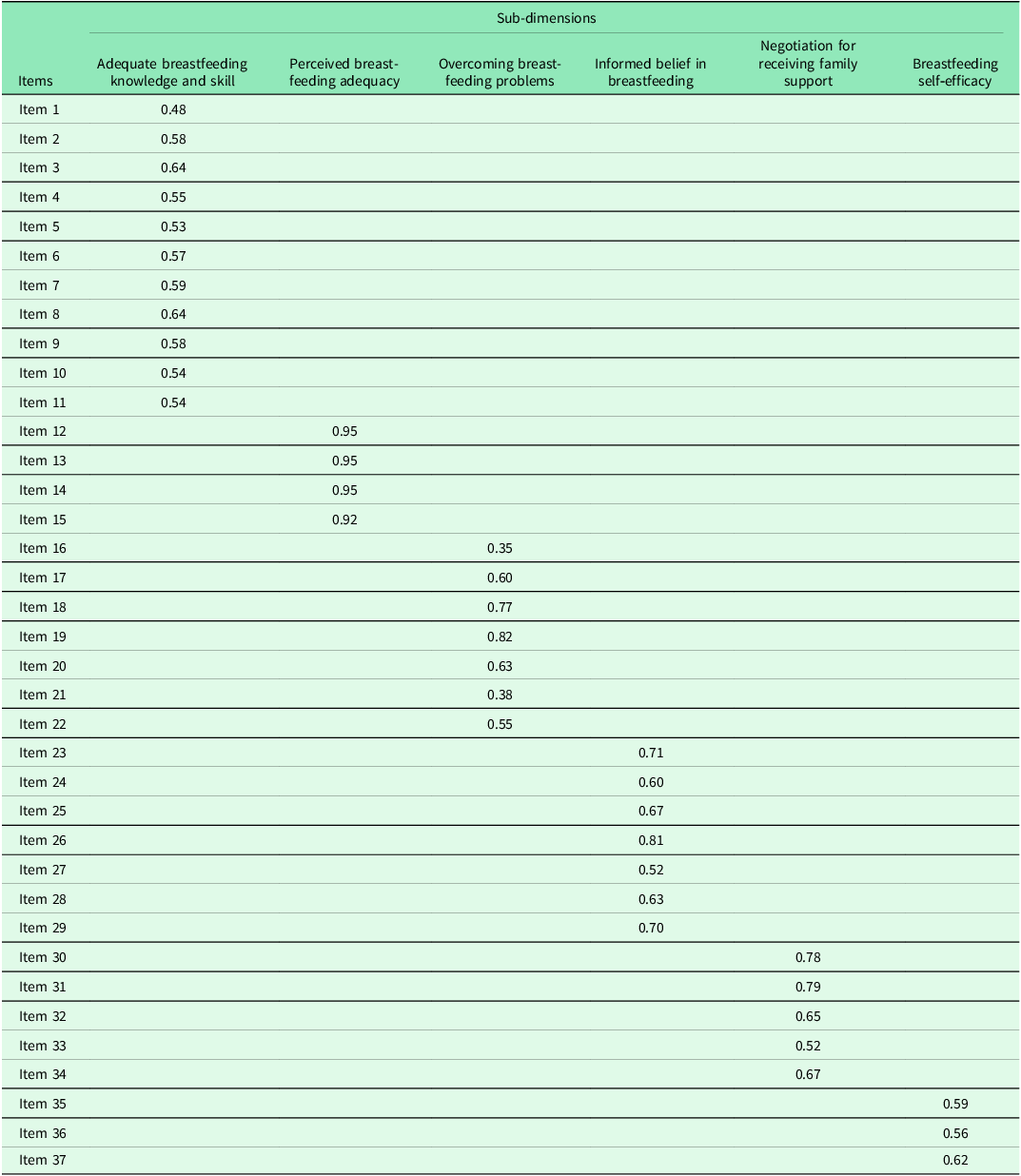
Confirmatory factor analysis (CFA): The fit index values made on the LISREL programme are as follows: X2/df:225.20/614 = 0.3, p = 0.001. Goodness of fit index (GFI) = 0.92, adjusted goodness of fit index (AGFI) = 0.88, comparative fit index (CFI) = 0.96, normed fit index (NFI) = 0.95, fit index (NNFI) = 0.99, incremental fit index (IFI) = 0.99, relative fit = 0.99, standardized root mean square residual (SRMR) = 0.04, root mean square error of approximation (RMSEA) = 0.01 (Table 2). In the factor analysis, we conducted for construct validity, the item loadings of the MBES were found to be at acceptable values between 0.35 and 0.82. In addition, all items and subscales in the scale were preserved. No items were removed (Table 3) (Figure1).
Item loadings of MBES
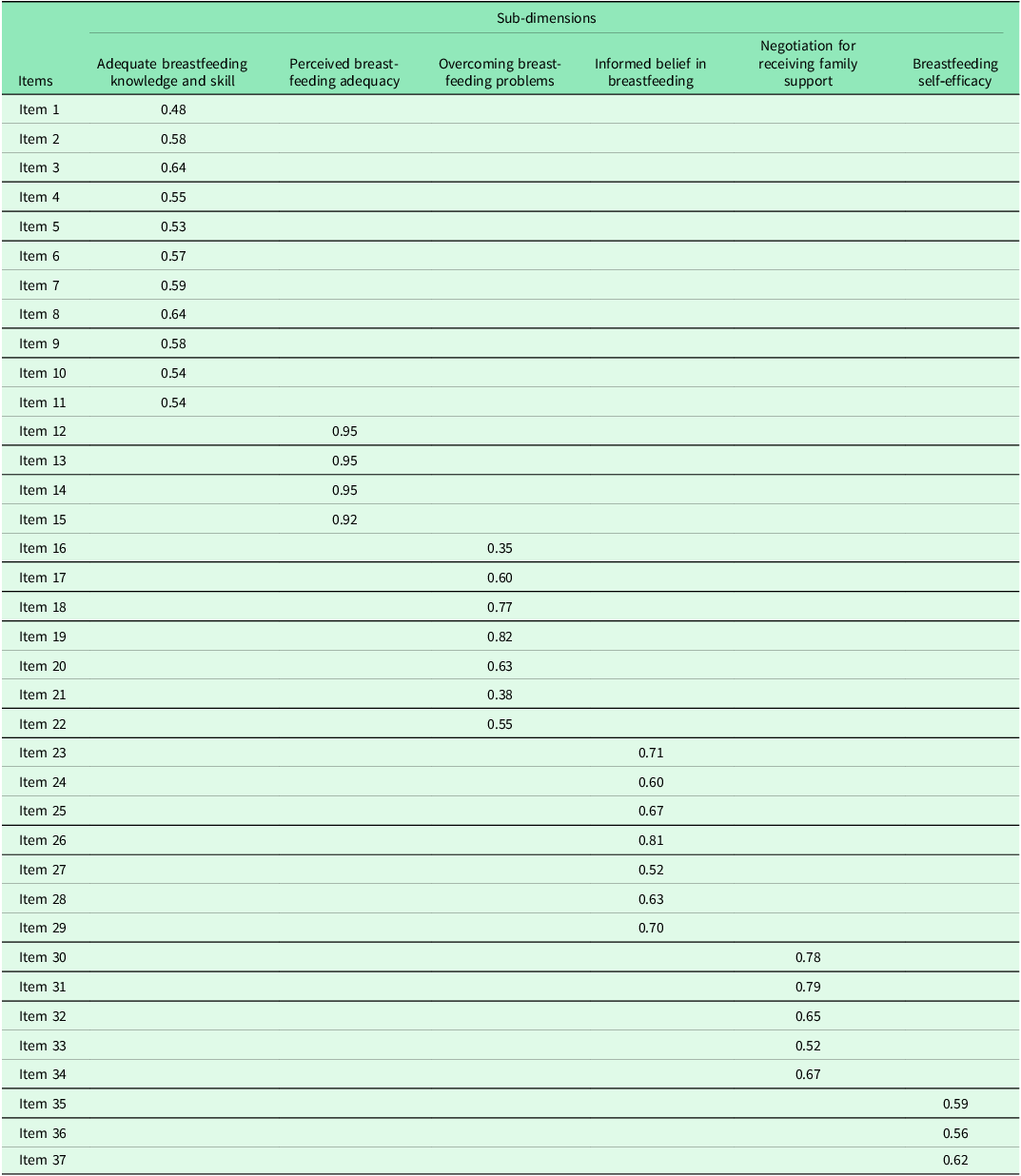
Factor analysis of the scale.

Reliability
Item total correlation
The correlation between the sub-dimensions of the scale was evaluated as strong. Sub-dimensions 1 and MBES r = 0.93, p = 0.01, sub-dimensions 2 and MBES r = 0.70, p = 0.01, sub-dimensions 3 and MBES r = 0.77, p = 0.01, sub-dimensions 4 and MBES r = 0.80, p = 0.01, sub-dimensions 5 and MBES r = 0.83, p = 0.01, and sub-dimensions 6 and MBES r = 0.79, p = 0.01 (Table 2).
Cronbach’s alpha
Cronbach’s alpha values for the scale and its sub-dimensions were found as follows:
Adequate breastfeeding knowledge and skill: 0.88, perceived breastfeeding adequacy: 0.78, informed belief in breastfeeding value: 0.77, overcoming breastfeeding problems: 0.77, negotiation for receiving family support: 0.77, breastfeeding self‑efficacy: 0.77, and total scale: 0.93 (Table 2).
Parallel forms
In the analysis conducted for parallel form reliability, a strong positive relationship was found between BSES and MBES (r = 72, p = 0.01) (Table 2). The relationship between the sub-dimensions of MBES and BSES was quite strong. The correlation values between the sub-dimensions of MBES and BSES were as follows: Sub-dimensions 1 (Adequate breastfeeding knowledge and skill) BSES r = 0.69, p = 0.01, sub-dimensions 2 (Perceived breastfeeding adequacy) and BSES r = 0.52, p = 0.01, sub-dimensions 3 (Informed belief in breastfeeding value) and BSES r = 0.54, p = 0.01, sub-dimensions 4 (Overcoming breastfeeding problems) and BSES r = 0.56, p = 0.01, sub-dimensions 5 (Negotiation for receiving family support) and BSES r = 0.58, p = 0.01, and sub-dimensions 6 (Breastfeeding self‑efficacy) and BSES r = 0.59, p = 0.01 (Table 4).
Correlation between MBES and BSES

*Correlation is significant at the 0.01 level (2-tailed).
Discussion
In this study we conducted to test the validity and reliability of MBES, we determined that the scale is a compatible tool suitable for Turkish society. With construct validity, it was determined that all items of the scale worked and factor loadings were within valid limits. In addition, the fact that our scale has a completely positive relationship with the parallel form scale has proven to us that our scale is a reliable tool. Cronbach’s alpha coefficient, which is another reliability analysis, was analysed as reliable values in the scale sub-dimensions and the overall total of the scale. According to all these analyses, we can say that our scale is a valid and reliable tool. Similar results were obtained in the study conducted by Mohammadi et al., who developed the scale (Mohammadi et al., Reference Mohammadi, Kohan and Heidari2022).
In our country, there are many tool such as breastfeeding self-efficacy scale (Dennis and Faux, Reference Dennis and Faux1999; Ekşioğlu and Çeber, Reference Ekşioğlu and Çeber2011), LATCH breastfeeding assessment tool (Jensen et al., Reference Jensen, Wallace and Kelsay1994; Yenal and Okumuş, Reference Yenal and Okumuş2003), Bristol Breastfeeding Evaluation Scale (Ingram et al., Reference Ingram, Johnson, Copeland, Churchill and Taylor2015; Dolgun et al., Reference Dolgun, İnal, Erdim and Korkut2018). However, all these scales evaluate knowledge, attitudes, and behaviours regarding breastfeeding separately or some parameters together. However, there is no tool that evaluates breastfeeding behaviour, self-efficacy, knowledge, and attitude together. However, MBES offers the opportunity to evaluate adequate breastfeeding knowledge and skills, perceived breastfeeding adequacy, informed belief in breastfeeding value, overcoming breastfeeding problems, negotiation for receiving family support, and breastfeeding self-efficacy altogether. For this reason, instead of evaluating using several tools, using a single scale can help us save labour and time. Therefore, it would be beneficial to popularize and promote the use of this scale.
In addition to reliability and validity analyses, scores from the scale were also analysed. The participants’ mother’s MBES score was found to be quite high. Accordingly, we can say that mothers are strong in breastfeeding. In fact, one of the factors that led to this result may be that the majority of mothers had a university or undergraduate education. This study supported Bu şüphelerimizi başka bir analizle desteklemiş bulunmaktayız. When we compared the total average scores of mothers from MBES in terms of their educational status, we found that mothers with university degrees and postgraduate education received higher scores than mothers with secondary school degrees, resulting in a statistically significant result. The role of education level, which is one of the demographic characteristics, is very important in continuing breastfeeding (Dennis Reference Dennis2002; McLeod et al., Reference McLeod, Pullon and Cookson2002). It has been determined that mothers with higher education levels are more successful in continuing breastfeeding (Dennis Reference Dennis2002; Blyth et al., Reference Blyth, Creedy, Dennis, Moyle, Pratt and De Vries2002). Additionally, studies have shown that mothers with lower education levels terminate breastfeeding much earlier (Ong et al., Reference Ong, Yap, Li and Choo2001; Wagner et al., Reference Wagner, Wagner, Ebeling, Chatman, Cohen and Hulsey2006). In their study, Küçükoğlu and Çelebioğlu (Reference Küçükoğlu and Çelebioğlu2014) determined that university graduates had higher breastfeeding success. In this case, it would be correct to say that education level is a factor that affects mothers’ breastfeeding success. Then we can say that it is also necessary to increase the education level of women in order to strengthen breastfeeding. Another finding of ours is that the average MBES total score of mothers working in the private sector is statistically significantly higher than that of civil servant mothers. This result may be due to the fact that mothers working in the private sector have their own workplaces, or it may be due to the fact that the majority of mothers working in the private sector quit their jobs and focused entirely on infant care.
Conclusion
The 37-item MBES is valid and reliable. Midwives, nurses, and lactation consultants can use MBES to measure breastfeeding and improve needs-based.
Author contributions
Conceptualization, ZC, LK, MYC; methodology, MYC; software, MYC; validation, MYC and formal analysis, ZC,LK,MYC; investigation, MYC; resources, MYC; data curation, MYC; writing – original draft preparation, LK, MYC; writing – review and editing, MYC; visualization, MYC; supervision, MYC; project administration, MYC; funding acquisition, MYC, ZC.
Funding statement
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Competing interests
The authors report no actual or potential conflicts of interest.
The patient consent
Patient consent was obtained from the participants in this study.



 Open access
Open access