


People with severe mental illness (SMI) are at an increased risk of a range of physical health conditionsReference Launders, Hayes, Price and Osborn1 and have higher premature mortality from cardiovascular disease (CVD) and other natural causes.Reference Hayes, Marston, Walters, King and Osborn2 The causes of these health inequalities are complex and include the adverse effects of psychotropic medications, poor diet or sedentary lifestyles, a higher prevalence of smoking, stigma and barriers to self-management and accessing optimal healthcare.Reference Dregan, McNeill, Gaughran, Jones, Bazley and Cross3–Reference Nash, Kingstone, Farooq, Tunmore and Chew-Graham5 Financial incentivisation for physical health checks in primary care was introduced for people with SMI in the UK in 2004, through the Quality and Outcomes Framework (QOF).6 Although definitions of SMI vary, the QOF mental health indicators incentivise general practitioner (GP) practices to hold a register of patients with SMI – defined as schizophrenia, bipolar disorder and other psychotic illness – to ensure that a care plan is in place and provide annual screening for physical health for this population. QOF incentivisation remains in place in England and Northern Ireland; Scotland withdrew from the incentivisation scheme in 2016, and Wales withdrew in 2019. Furthermore, there have been notable changes in the exact incentives applied under the mental health indicators.Reference Launders, Jackson, Hayes, John, Stewart and Iveson7
To ensure incentivisation was fairly applied, a system of exception reporting was employed until April 2019, allowing GP practices to remove patients from the denominator used to calculate incentives either because they are deemed unsuitable (e.g. because of contraindication or ineligibility) or because of informed dissent (declining invitation) or non-response.8 Although an exception-reported patient is removed from the denominator for calculating incentivisation, the patient remains on the practice list and on disease registers. The GP practice therefore continues to have a duty of care to an exception-reported patient, and the patient is included on patient lists for funding purposes other than that particular QOF indicator. In 2019, exception reporting was replaced with Personalised Care Adjustment (PCA).9 PCAs are a direct replacement of exception reporting, allowing better documentation of the reasons for removing a patient from incentivisation.
A review of pay for performance schemes lists exception reporting as a key component, ensuring practices are not penalised for factors outside of their control, such as a higher than average proportion of patients being unsuitable for a given indicator.Reference Conway and Satin10 However, although exception reporting may be necessary, it is also crucial that people removed from an incentivisation scheme receive high-quality care. In the case of patients with SMI, removal from the QOF incentivisation may signify a patient is experiencing barriers to care, issues navigating the complex and siloed healthcare system, and the complexity of managing both mental and physical health problems. There have been no studies to investigate patient characteristics associated with exception reporting from mental health measures in the UK. Given the potential impact of not providing physical health checks for people with SMI, it is imperative we understand which patients with SMI are exception reported and why. This study aims to characterise the pattern of exception reporting from QOF mental health indicators in people with SMI, and investigate patient characteristics associated with exception reporting.
Method
Study design
This study was a descriptive analysis of exception reporting from mental health measures in the UK, based on a cohort of patients with SMI identified in the Clinical Practice Research Datalink (CPRD) GOLD and Aurum databases. CPRD GOLD and Aurum contain electronic health records from over 2000 GP practices in the UK, extracted from the EMIS and Vision clinical systems, and patients have been shown to have a similar age, gender and ethnicity profile as the UK population.Reference Herrett, Gallagher, Bhaskaran, Forbes, Mathur and van Staa11,Reference Wolf, Dedman, Campbell, Booth, Lunn and Chapman12 We investigated annual trends in exception reporting at a population level, and patient characteristics associated with exception reporting in a cross-sectional analysis at an individual level. Our protocol was preregistered with the Open Science Framework (https://osf.io/czetb/).
Population
The population of interest was based on an existing cohort of patients aged over 18 years, with a diagnosis of SMI (schizophrenia, bipolar disorder or other non-organic psychosis) recorded in GP practice records for at least a year between 2000 and 2018.Reference Launders, Jackson, Hayes, John, Stewart and Iveson7 For this current study, we limited the cohort to those active for at least a year between April 2004, when QOF incentivisation was introduced, and March 2018. Entry to the cohort was the latest date of the following: first recording of SMI in GP records, registration at GP practice and 1 April 2004. Exit was the earliest date of the following: death, leaving the GP practice, age 100 years and 31 March 2018. For patients resident in Scotland, the latest date of exit was set to 31 March 2016, as they were no longer eligible for QOF incentivisation after this point. Patients were required to be registered with the GP practice for 1 year, and for annual prevalence of exception reporting, for the final 3 months of each financial year, in line with QOF reporting rules.
Covariates
We investigated the following factors potentially associated with being exception reported from the QOF mental health incentivisation and defined a priori: patient age at cohort entry, gender, ethnicity, country of GP practice, prescription of antipsychotics or mood stabilisers (lithium, sodium valproate or lamotrigine), specific SMI diagnosis (most recently recorded of schizophrenia, bipolar disorder or ‘other psychoses’) and ever appearing on another QOF register (atrial fibrillation, coronary heart disease, hypertension, peripheral artery disease, stroke or diabetes registers) that incentivises CVD risk factor screening. For ethnicity, individual terms used to define an individual’s ethnicity were grouped into the broader ethnicity categories used in the UK 2011 and 2021 Census.13,14 For mood stabilisers, we did not include carbamazepine because of the low prevalence of prescribing in the UK during the study period,Reference Ng, Man, Gao, Chan, Lee and Hayes15 potential misclassification of epilepsy use and the low number of patients with bipolar disorder for which this would be the sole antipsychotic/mood stabiliser ever prescribed. Code lists for covariates and outcomes are available on the HDR UK Phenotype Library (Supplementary Tables 1 and 2).
Outcomes
The primary outcome was exception reporting from the QOF mental health indicators. We defined this using the Read codes listed under QOF in 2017/2018, and through searches for similar terms. Our search identified four potential codes suggesting removal from either the total mental health indicator, or from physical health checks, and a further 28 that suggested removal from some part of the physical health checks. We stratified this into codes denoting exception reporting resulting from informed dissent (i.e. declining or non-response) and those denoting that a patient was unsuitable for the indicator (Supplementary Table 1).
Statistical analysis
We calculated the annual prevalence of exception reporting by financial year and stratified by covariates.
We investigated patient characteristics associated with ever being exception reported in a cross-sectional design, using logistic regression. We mutually adjusted for all covariates and used robust sandwich standard errors to account for clustering by GP practice.Reference Mansournia, Nazemipour, Naimi, Collins and Campbell16 This method of calculating standard errors allowed us to adjust confidence intervals to account for potential lack of independence between individual patients within a GP practice. We additionally adjusted for the time since SMI diagnosis, time since GP practice registration, year of end of record and total time from cohort entry to exit.
All analysis was performed in R version 4.4.0 for Windows (R Foundation for Statistical Computing, Vienna, Austria; see https://www.r-project.org/) and RStudio version 2024.04.1 Build 478 for Windows (Posit, Boston, MA, USA; see http://www.rstudio.com/), and reported in line with the RECORD checklist.Reference Benchimol, Smeeth, Guttmann, Harron, Moher and Petersen17
Missing data
Missing ethnicity was included as a separate category, as missing ethnicity is likely a marker of reduced or absent healthcare. For all diagnostic and screening variables, absence of a code was deemed to indicate an absence of diagnosis or screening. Location data for one GP practice was missing. As the country that this practice was operating in was unknown, patients from this practice (n = 122) were excluded from the analysis.
Sensitivity analysis
We investigated exception reporting by deprivation as a sensitivity analysis because of large amount of missing data for this variable. We limited the analysis to patients resident in England with available deprivation data (English Index of Multiple Deprivation quintiles) and re-ran the logistic regression models with Index of Multiple Deprivation quintiles included.
Ethics and consent
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. Approval for this study was obtained from the Independent Scientific Advisory Committee of CPRD (protocol number 18_288). All CPRD data are anonymised and therefore consent is not required.
Results
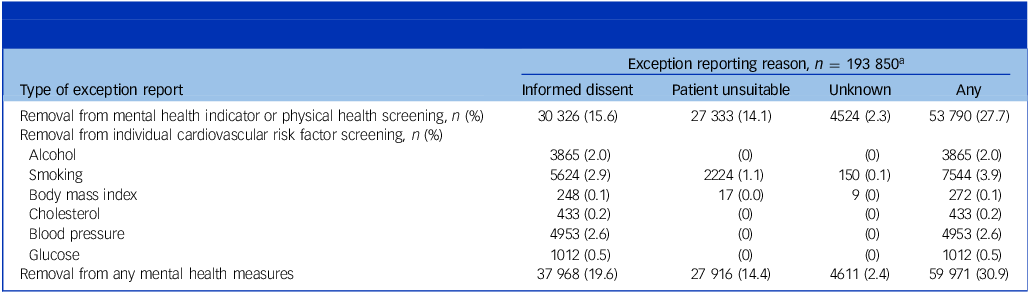
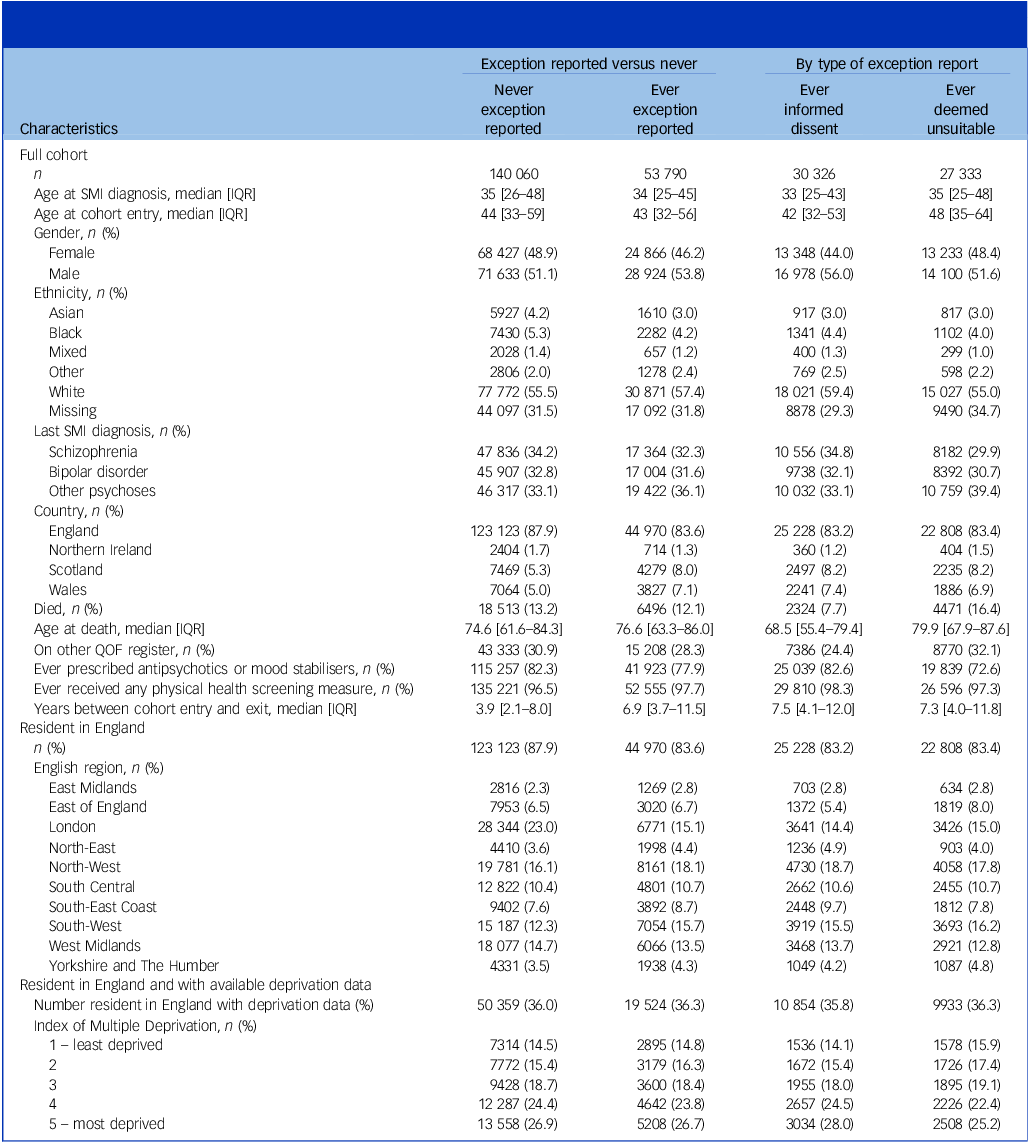
We identified 193 850 patients with SMI who were registered for at least a year between 2004 and 2018, of which 27.7% received a code suggesting they were exception reported from the QOF mental health indicators or physical health checks at least once between cohort entry and exit (Table 1). A further 3.2% were not exception reported from all measures, but received a code for withdrawal from individual CVD risk factor screening. Over half of the cohort were male (51.9%), 32% did not have details on ethnicity recorded and 2% were an ethnicity other than Asian, Black, White or Mixed (termed ‘other ethnicity’; Table 2).
Patients with severe mental illness receiving exception reporting codes for Quality and Outcomes Framework mental health indicators, April 2004 to March 2018

a. Patients may have more than one type of exception report.
Characteristics of people with severe mental illness, by Quality and Outcomes Framework mental health indicators exception reporting status, 2004–2018

SMI, severe mental illness; IQR, interquartile range; QOF, Quality and Outcomes Framework.
Of the 53 790 patients who were exception reported from all QOF mental health indicators at least once, 50.8% had a code indicating they were deemed unsuitable and 56.4% had at least one code indicating informed dissent (Table 1), and 11.1% of patients received codes for both. Of those exception reported at least once, 3568 (6.6%) of patients were exception reported for every year that they were active, and 14 692 (27.3%) for 50% or more of the years they were eligible.
Population-level trends in exception reporting from QOF mental health indicators over time
The prevalence of exception reporting from mental health indicators was lowest in 2005–2006 (2.6%) and 2004–2005 (2.7%) financial years, and highest in 2013–2014 (13.3%) followed by 2006–2007 (13.1%). For all other years, exception reporting was between 7.6 and 11.1% (Fig. 1). Over the study period, the proportion of patients who had a code for informed dissent increased, whereas the proportion of patients recorded as unsuitable decreased (Fig. 1). When stratified by patient characteristics, the pattern of exception reporting from mental health indicators was consistent over time. Annual exception reporting was more common in those who were male, of ‘other’ or missing ethnicity, not receiving antipsychotics or mood stabilisers, under the age of 40 years and with a diagnosis of ‘other psychoses’ (Supplementary Fig. 1).
Proportion of patients with severe mental illness exception reported from the UK Quality and Outcomes Framework mental health indicators, stratified by reason for exception, 2004–2018.

Individual-level factors associated with patients being exception reported from mental health indicators
Patients who were exception reported from mental health indicators were active in the cohort for longer (median years between cohort entry and exit: 6.9; interquartile range (IQR): 3.7–11.5) than those who were never exception reported (3.9 years, IQR: 2.1–8.0), although the median age at cohort entry was similar between these two groups (exception reported: median 43 years, IQR: 32–56; never exception reported: median 44 years, IQR: 33–59; Table 2).
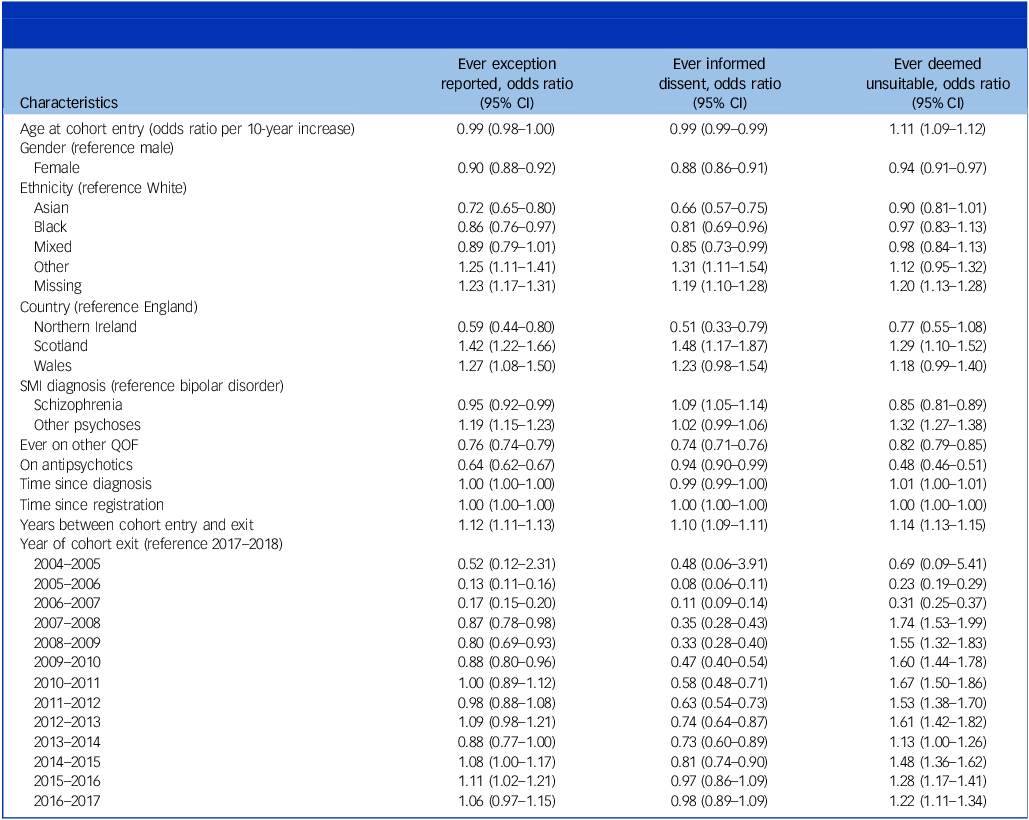
Being prescribed antipsychotics or mood stabilisers (odds ratio 0.64, 95% CI 0.62–0.67), being on another QOF register that also incentivises CVD risk factor screening (odds ratio 0.76, 95% CI 0.74–0.79), residence in Northern Ireland (odds ratio 0.59, 95% CI 0.44–0.80) compared with England, Asian (odds ratio 0.72, 95% CI 0.65–0.80) or Black ethnicity (odds ratio 0.86, 95% CI 0.76–0.97) compared with White, female gender (odds ratio 0.90, 95% CI 0.88–0.92) and a diagnosis of schizophrenia (odds ratio 0.95, 95% CI 0.92–0.99) compared with bipolar disorder were associated with reduced odds of being exception reported from mental health indicators (Table 3, Supplementary Table 3).
Mutually adjusted odds ratios and 95% confidence intervals from multivariable logistic regression comparing patient characteristics of those ever versus never exception reported from Quality and Outcomes Framework mental health indicators

SMI, severe mental illness; QOF, Quality and Outcomes Framework.
Conversely, residing in Scotland (odds ratio 1.42, 95% CI 1.22–1.66) or Wales (odds ratio 1.27, 95% CI 1.08–1.50) compared with England, having missing (odds ratio 1.23, 95% CI 1.17–1.31) or ‘other’ ethnicity (odds ratio 1.25, 95% CI: 1.11–1.41) compared with White ethnicity, or having a diagnosis of ‘other psychoses’ (odds ratio 1.19, 95% CI 1.15–1.23) compared with bipolar disorder were associated with an increased risk of being exception reported from mental health indicators (Table 3).
When the analysis was performed separately for patients who were exception reported because of informed dissent and being unsuitable, many of the associations remained (Table 3). However, despite finding no association between older age and exception reporting overall (odds ratio per 10-year increase in age: 0.99; 95% CI 0.98–1.00), increased age was associated with a slightly lower risk of being exception reported because of informed dissent (odds ratio per 10-year increase in age: 0.99; 95% CI 0.99–0.99), but an increased risk of being exception reported because of being unsuitable (odds ratio per 10-year increase in age: 1.11; 95% CI 1.09–1.12). Furthermore, Asian and Black ethnicity was only associated with lower risk of exception reporting because of informed dissent (Asian: odds ratio 0.66, 95% CI 0.57–0.75; Black: odds ratio 0.81, 95% CI 0.69–0.96; relative to White ethnicity) and not because of being deemed unsuitable (Asian: odds ratio 0.90, 95% CI 0.81–1.01; Black: odds ratio 0.97, 95% CI 0.83–1.13). Finally, a diagnosis of schizophrenia (relative to bipolar disorder) was associated with an increased risk of being exception reported because of informed dissent (odds ratio 1.09, 95% CI 1.05–1.14), but lower risk of being exception reported because of being unsuitable (odds ratio 0.85, 95% CI 0.81–0.89).
In a sensitivity analysis of patients in England with available deprivation data (n = 69 883/123 123; 56.8%), deprivation was not associated with risk of exception reporting (Supplementary Table 4). However, the lower risk of any exception reporting observed in those of Black ethnicity was no longer significant (odds ratio 0.88, 95% CI 0.76–1.01). Additionally, patients with diagnosis of schizophrenia (odds ratio 1.05, 95% CI 0.98–1.13) no longer had an increased risk of exception reporting because of informed dissent, compared with those with bipolar disorder.
Discussion
Our study is the first to investigate trends in exception reporting from the QOF mental health indicators in the UK, and patient characteristics associated with exception reporting.
This large analysis of electronic health records suggests that almost a third of patients with SMI in the UK are excepted from the QOF mental health indicators at least once. In any given year, around 10% of patients with SMI are not included in the mental health indicators. This is concerning, given the persisting physical health inequalities in people with SMI. For interventions aimed at improving the health of people with SMI to be successful, they need to consider how to best engage individuals who either do not receive screening or treatment. Missed opportunities to diagnose or intervene on cardiovascular risk factors continue to put people with SMI at increased risk of CVD.
We found that the proportion of patients exception reported because of informed dissent increased over the study period, that patients with a diagnosis of ‘other psychoses’ were more likely to be exception reported in general, and that men, patients of Asian or Black ethnicity, patients of younger age and those with schizophrenia were more likely to be exception reported because of informed dissent. Further investigation is warranted to understand the reasons for these findings. Although more details on why patients were exception reported were not available, QOF guidelines include broad criteria for exception reporting. These include non-response and informed dissent, as well as patients for whom it is not appropriate because of conditions such as terminal illness or extreme frailty, or where a patient has another condition that means these checks would be inappropriate.
No other studies have described characteristics of patients with SMI who are exception reported, although Kontopantelis et al found that in the general population of the UK, men were more likely to be exception reported from any QOF indicator than women, and older age was associated with exception reporting because of being deemed unsuitable.Reference Kontopantelis, Springate, Ashcroft, Valderas, van der Veer and Reeves18 However, in contrast to our findings, they also found older age was associated with exceptions because of informed dissent.Reference Kontopantelis, Springate, Ashcroft, Valderas, van der Veer and Reeves18 The reasons for higher exception reporting because of informed dissent in younger people with SMI in our study therefore requires further investigation. It may be that young people with SMI are more likely to not perceive the need for physical health checks than, for example, young people on the diabetes register. Alternatively, younger patients with SMI may experience more barriers to attending appointments or may have relatively new mental health diagnoses, meaning physical health screening is done under the care of secondary care mental health services.
Implications
It has been argued that exception reporting is a marker of patients making informed decisions and of high-quality practice.Reference Hopayian19 Although this may be true for some patients, perhaps because of screening activities in secondary care mental health services, the lack of screening in primary care means that GPs do not have information on CVD risk factors for these patients. This is further compounded by a lack of coordination of physical health screening between primary care, early intervention and secondary care mental health services.Reference Joury, Beveridge, Littlejohns, Burns, Copsey and Philips20,Reference Rodgers, Dalton, Harden, Street, Parker and Eastwood21 Furthermore, although informed dissent exception reporting may represent an active informed decision not to engage, it may also be used for patients who do not respond to invitations for screening. For vulnerable, complex or disengaged patients, exception reporting likely results in a reduction in services, putting them at risk of undetected physical health problems. Increasing the coverage and accessibility of broad physical health checks is crucial, if we are to improve the management of physical health in people with SMI.
Current National Health Service and National Institute for Health and Care Excellence guidance suggest that physical health checks in primary care occur as part of a comprehensive annual review of physical health, and are offered to all patients who are severely affected by their mental health.22 However, the focus of the QOF incentivisation scheme on a narrow set of CVD risk factors and on specific mental health diagnoses does not support this approach, and means that patients outside of these specific mental health diagnoses, such as those prescribed antipsychotics in the absence of an SMI diagnosis,Reference Marston, Nazareth, Petersen, Walters and Osborn23 do not receive these services, and that the broader physical health of people with SMI is not considered in physical health checks.
Broad physical health and medication reviews with support for follow-up interventions would allow for approaches such as tailored antipsychotic prescribing based on weight gain or obesity, alongside support to manage weight.Reference Nash, Kingstone, Farooq, Tunmore and Chew-Graham5 Tools and programmes to support this coordinated approach exist, but our research highlights the importance of considering those not responding to invitations or declining screening services, if these are going to be successful in managing physical health.
The Lester positive cardiometabolic resource provides a flow chart for considering the interventions and targets following physical health screening.Reference Perry, Holt, Chew-Graham, Tiffin, French and Pratt24 Further, a recent study by Joury et al produced co-designed recommendations for best practice for physical health checks and follow-up interventions in both primary and secondary care,Reference Joury, Beveridge, Littlejohns, Burns, Copsey and Philips20 and PRIMROSE-A provides a model for supported, individualised care. PRIMROSE-A is a National Institute for Health and Care Research-funded implementation programme for CVD support in SMI that aims to improve both engagement with, and outcomes of, physical health checks. The programme provides mental health review, social support and outreach to those patients who do not engage with physical health checks, and clinical review and support for behaviour change following physical health checks.Reference Shaw, Mifsud, Osborn, Nahata, Hall and Prenelle25
GPs should be aware that exception reporting is common in people with SMI, particularly in those with a diagnosis of ‘other psychosis’, and that this group of patients are less likely to have complete CVD risk factor screening.Reference Launders, Jackson, Hayes, John, Stewart and Iveson7 Although there are many different presentations included in the ‘other psychoses’ group (including schizoaffective disorder, other non-organic psychoses and symptoms of psychosis), it is likely that some patients in this group are experiencing first-episode psychosis or more transient episodes of psychosis, and therefore may be harder to engage. For some, the lack of a definitive psychiatric diagnosis may be attributable to non-engagement with services.
Younger patients, men, patients of Black or Asian ethnicity and patients with a diagnosis of schizophrenia may be more likely to decline or not respond to invitations for physical health checks. The reasons for this are likely to be complex, driven by factors associated with a patient’s underlying characteristics, their mental illness, access and barriers to care, and previous experiences within the healthcare system, and further work is warranted to identify reasons for declining these services. GPs should be aware that although informed dissent may be more common in older patients in the general population, for people with SMI, this is more prevalent in younger patients.
Strengths and limitations
We believe that our study provides the first description of exception reporting in people with SMI in the UK, using the pseudonymised records of almost 200 000 patients. We have identified key patient characteristics associated with being exception reported, such as age, gender, ethnicity and specific SMI diagnosis, and critical research gaps that urgently need filling to improve the health of people with SMI. We preregistered our protocol for this study, ensuring that we only investigated hypotheses and covariates set out a priori.
Our study is descriptive in nature, and we did not seek to ascribe causality to the groups of patients at risk of being exception reported from QOF mental health indicators. We assessed risk of ever being exception reported, and therefore unmeasured confounding and temporal change could account for some of our findings. Furthermore, we were not able to separate non-response from informed dissent, nor determine the reasons for a patient being unsuitable for physical health checks. The limited codes for exception reporting likely mean there is some misclassification bias between those deemed unsuitable and those exception reported because of informed dissent. Although this is a limitation, our study sought to describe the patterns of exception reporting, providing a basis for future studies to investigate predictors and outcomes of receiving exception reporting or PCAs. The introduction of PCAs in 2019 included more complete documentation on the reasons that patients are removed from incentivised indicators, which will aid future research using electronic health records. Further research – both quantitative and qualitative – is required to determine the drivers of the increased informed dissent from physical health screening in patients with SMI observed in this study.
Although we know that exception reporting results in low prevalence of screening for cardiovascular risk factors,Reference Launders, Jackson, Hayes, John, Stewart and Iveson7 we did not consider the impact of being exception reported on physical health outcomes. In the general population, patients who are exception reported from any QOF indicators are at a higher risk of death in the following year,Reference Kontopantelis, Springate, Ashcroft, Valderas, van der Veer and Reeves18 and the potential for life-limiting illness and complex disease to inform exception reporting makes impacts on mortality hard to determine.
In our sensitivity analysis, we did not find any association between deprivation and exception reporting. However, we only had deprivation data for England, and it was often missing (43%). This finding is in contrast to three studies of exception reporting from all QOF measures in the general population.Reference Kontopantelis, Springate, Ashcroft, Valderas, van der Veer and Reeves18,Reference Lowrie, McConnachie, Williamson, Kontopantelis, Forrest and Lannigan26,Reference Doran, Kontopantelis, Fullwood, Lester, Valderas and Campbell27 Further research is required to determine whether this finding is correct and potentially unique to people with SMI, or a result of the high level of missing deprivation data in our study.
Finally, this study investigated trends in exception reporting up to 2018, and therefore may not reflect current practices. However, our work shows the long-term trend of exception reporting remained unchanged for much of the study period, and provides a basis for further research. We did not consider the COVID-19 pandemic period because between April 2020 and March 2022, most QOF indicators were payment protected. This means that payment was made irrespective of achieving an indicator, and therefore the data from this period are therefore thought to be a less accurate representation of the activities that took place.28 Research has shown that for hypertension management in the general population, although blood pressure measurements were reduced during the pandemic, by 2023 they were returning to pre-pandemic levels.Reference Wiedemann, Speed, Cunningham, Higgins, Curtis and Andrews29 Future research is now warranted to investigate the recovery of QOF incentivisation for the mental health measures and exception reporting rates, following the COVID-19 pandemic.
In conclusion, exception reporting from the mental health QOF indicators is common in people with SMI. This is concerning, given the persisting inequities in physical health and life expectancy in this population. Although exception reporting, or PCAs, are necessary for the functioning of the QOF incentivisation, it is essential that they are applied fairly and appropriately. These measures include the provision of physical health checks, an important component of preventative medicine in a population known to have worse physical health than the general population. Men and those with ‘other psychoses’ diagnoses may be more likely to be exception reported, and men, younger patients and those with a diagnosis of schizophrenia are more likely to be exception reported because of informed dissent. Further research is required to determine the reasons for exception reporting from both patient and provider perspectives, to inform interventions to ensure that those disengaging from physical health checks are truly informed, and to improve the uptake of physical health screening and interventions in people with SMI.
Supplementary material
The supplementary material can be found at https://doi.org/10.1192/bjp.2025.49
Data availability
Data were obtained from a third party and are not publicly available. All data were obtained from Clinical Practice Research Datalink (CPRD). Data is available from CPRD, but is subject to protocol approval and ethical review: https://www.cprd.com/research-applications. Code lists are deposited in the HDR UK Phenotype library (https://phenotypes.healthdatagateway.org/) and analytical code is available on reasonable request.
Acknowledgements
The authors thank the wider collaborators involved in DATAMIND for their input, and in particular, lived experience advisors both as part of the DATAMIND Super Research Advisory Group and the UCL Division of Psychiatry Data PPI Group.
Author contributions
D.P.J.O., J.F.H. and N.L. formulated the research question. C.A.J., J.F.H., A.J., R.S., M.H.I., E.B., B.G., S.W.M. and D.P.J.O commented on the study protocol and the design the study. N.L. carried out the analysis and wrote the first draft of the manuscript. C.A.J., J.F.H., A.J., R.S., M.H.I., E.B., B.G., S.W.M. and D.P.J.O. commented on the results of the analysis and on the manuscript.
Funding
This work was funded by the HDR UK DATAMIND hub, which is funded by the UK Research and Innovation (UKRI) grant MR/W014386/1. N.L., J.F.H., M.H.I., E.B., R.S., A.J. and D.P.J.O. acknowledge funding from DATAMIND.
N.L. is additionally supported by a Health Data Research UK personal fellowship. This work is affiliated with Health Data Research UK (Big Data for Complex Disease – HDR-23012), which is funded by the Medical Research Council (UKRI), the National Institute for Health and Care Research (NIHR), the British Heart Foundation, Cancer Research UK, the Economic and Social Research Council (UKRI), the Engineering and Physical Sciences Research Council (UKRI), Health and Care Research Wales, Chief Scientist Office of the Scottish Government Health and Social Care Directorates and Health and Social Care Research and Development Division (Public Health Agency, Northern Ireland).
N.L. and J.F.H. are additionally supported by the UKRI grant MR/V023373/1. N.L., J.F.H., E.B. and D.P.J.O. are supported by the University College London Hospitals NIHR Biomedical Research Centre. N.L., J.F.H. and D.P.J.O. are also supported by the NIHR North Thames Applied Research Collaboration. This funder had no role in study design, data collection, data analysis, data interpretation or writing of the report. The views expressed in this article are those of the authors and not necessarily those of the National Health Service (NHS), the NIHR or the Department of Health and Social Care.
R.S. is additionally part-funded by the NIHR Maudsley Biomedical Research Centre at the South London and Maudsley NHS Foundation Trust and King’s College London; the NIHR Applied Research Collaboration South London at King’s College Hospital NHS Foundation Trust; the UK Prevention Research Partnership (Violence, Health and Society; grant number MR-VO49879/1), an initiative funded by UKRI Councils, the Department of Health and Social Care (England) and the UK devolved administrations; and leading health research charities.
M.H.I. is additionally supported by the Wellcome Trust (grant numbers 220857/Z/20/Z, 226770/Z/22/Z, 104036/Z/14/Z and 216767/Z/19/Z) and by a Research Data Scotland Accelerator Award (number RAS-24-2).
E.B. acknowledges additional support from the Medical Research Council (grant numbers G1100583 and MR/W020238/1), NIHR (grant number NIHR200756), Mental Health Research UK – John Grace QC Scholarship 2018, the Economic Social Research Council’s co-funded doctoral award, the British Medical Association’s Margaret Temple Fellowship, the Medical Research Council’s New Investigator and Centenary Awards (numbers G0901310 and G1100583) and the NIHR Biomedical Research Centre at University College London Hospitals NHS Foundation Trust and University College London.
Declaration of interest
J.F.H. has received consultancy fees from juli Health and the Wellcome Trust. He is a co-founder and shareholder of juli Health. juli Health has a patent pending. J.F.H. is a member of the British Journal of Psychiatry Editorial Board, but did not take part in the review or decision-making process of this paper. R.S. declares research support received in the past 3 years from GSK and Takeda. The other authors declare no conflicts of interest.




 Open access
Open access
eLetters
No eLetters have been published for this article.