


Introduction
On February 6, 2023, a 7.7 magnitude seismic event centered in the city of Kahramanmaraş, Türkiye, resulted in significant devastation and losses across 11 surrounding provinces, leading to the declaration of the region as a disaster zone (Özmen, Reference Özmen2023). The earthquake caused the loss of 50,500 lives. In the month following the earthquake, 11,020 aftershocks occurred. Regional inspections indicated that 215,000 buildings either collapsed or sustained serious damage as a result of the earthquake. Thousands of people have lost their homes and loved ones (AFAD, 2023).
Earthquakes not only cause physical destruction but also deeply impact on the mental health of individuals in the affected geographical area (Nakajima, Reference Nakajima2012). Individuals who have been exposed to such significant traumatic events often experience adverse effects on their mental health (Kartol et al., Reference Kartol, Üztemur and Yaşar2024; Kristensen et al., Reference Kristensen, Weisæth and Heir2012). After an earthquake, people may experience significant emotions, such as shock, disbelief, anger, helplessness, powerlessness, loss of trust, loss of control, and fear of death (Yıldız and Akkoyun, Reference Yıldız and Akkoyun2023). Among the emotional effects of earthquakes, concerns about death are particularly important. This may manifest as anxiety about death, thoughts related to death, and death depression (Mohammadzadeh et al., Reference Mohammadzadeh, Ashouri, Vahedi and Asgharipour2018). It was observed that 82% of the individuals who were exposed to an earthquake stated that they often thought about death after the earthquake and 69.7% stated that their priorities about life changed (Şeker and Akman, Reference Şeker and Akman2014). Furthermore, individuals directly affected by the earthquake experienced higher levels of death anxiety and death distress than their second-degree relatives who were affected by the earthquake. In the same study, it was found that women experienced a higher level of death distress than men (Bırni et al., Reference Bırni, Deniz, Karaağaç, Erişen, Kaya and Satıcı2023). These findings indicate that the impact of the earthquake extends beyond physical destruction and includes psychological consequences for individuals.
Significant changes in human life can lead individuals to reconsider life priorities and goals (Malicka et al., Reference Malicka, Mynarska and Świderska2021). These changes include economic, social, humanitarian, and health crises that can often reduce the desire to conceive or cause individuals to postpone the decision to have children (Brée et al., Reference Brée, Bourguignon and Eggerickx2016; Ayllón, Reference Ayllón2019; Marteleto et al., Reference Marteleto, Padilla, Dondero and Sereno2023; Somefun et al., Reference Somefun, Banougnin and Smith-Greenaway2024). A systematic review on the impacts of disasters showed that disasters generally have a negative impact on fertility rates, although the effect varies depending on the type of disaster (Lee et al., Reference Lee, Batyra, Castro and Wilde2023). Fertility intention expresses an individual’s desire to have children and is influenced by biological, socioeconomic, cultural, and religious factors (Lau et al., Reference Lau, Huo, Wang, Shi, Li, Mu, Peng, Wang, Chen, Ng and Chan2018). Fertility intention is an important factor that determines the fertility level of families. Some studies focus on women’s fertility intentions in the short term and examine their desire to have children in the next 3 years (Eurostat, 2020; Mussino et al., Reference Mussino, Gabrielli, Ortensi and Strozza2021). This is an important approach to understanding how their fertility planning is affected.
According to the Centers for Disease Control and Prevention (CDC), 34 million people in the world are affected by disasters each year, of whom 80% are women and children. It is estimated that 25% of the affected women are of childbearing age (CDC, 2021). Therefore, disasters do not have the same impact on men and women, but their effects on women of childbearing age are more severe. It has been emphasized in the literature that disasters can impact fertility (Zotti et al., Reference Zotti, Williams, Robertson, Horney and Hsia2013). With the increasing frequency and intensity of disasters, understanding the effect of disasters on fertility has become an important research topic (Grace, Reference Grace2017; Muttarak, Reference Muttarak2021). However, the cause of this effect remains unclear, as studies have mainly focused on fertility behavior. Fertility intentions measure future fertility behavior over time, and understanding these intentions is crucial in the planning of services for individuals (Malicka et al., Reference Malicka, Mynarska and Świderska2021).
Aims & hypotheses
This study aimed to investigate the relationship between death distress and fertility intentions among married women of childbearing age residing in the region affected by the earthquake of February 6, 2023. The research question was as follows: i) What is the death distress level among married women residing in the earthquake-affected region following the earthquake on February 6, 2023? ii) What is the relationship between women’s death-distress levels and descriptive characteristics? iii) What is the status of changes in women’s fertility intentions after the earthquake? iv) Is there a relationship between women’s fertility intentions and death distress levels?
Materials and methods
Type of research
This study is descriptive and correlational.
Location and characteristics of the research
The study was conducted in 11 provinces that were affected by the Kahramanmaraş-centered earthquake on February 6, 2023, and were declared disaster zones (Kahramanmaraş, Adana, Adıyaman, Diyarbakir, Gaziantep, Hatay, Kilis, Malatya, Osmaniye, Şanlıurfa, and Elazig).
Population and sample
The study population consisted of married women aged 18–49 years who resided in the provinces affected by the earthquake centered in Kahramanmaraş on February 6, 2023, and who continued to reside in these provinces after they were declared disaster zones following the earthquake. The study sample consisted of 294 women who met the inclusion criteria and agreed to participate.
G*Power version 3.1.9.2 was used to calculate the sample size (Faul et al., Reference Faul, Erdfelder, Buchner and Lang2009). Birni et al., reported the mean death anxiety scores of the participants, which were found to be 25.8 4 ± .34. Using these data, the required sample size was determined to be 265 individuals for a 95% confidence level (1−α), 80% power (1−β), an effect size of d = .176, and a two-tailed t-test. To account for potential data loss, the sample size was increased by 10%, resulting in a final sample size of 292 individuals.
Inclusion criteria for participants
Women who were residing in the provinces declared as disaster zones during the earthquake centered in Kahramanmaraş and Elbistan on February 6, 2023, and who continued to live in the same province after the earthquake, aged 18–49 years, and had been married for more than one year.
Exclusion criteria
Women with diagnosed or reported psychological problems (depression, suicidal tendencies, etc.), who reported having experienced a traumatic event in the last year before the earthquake, and who had undergone tubal ligation before the earthquake.
Data collection techniques and tools
Data were collected using the ‘Participant Information Form’ and the ‘Brief Death Distress Scale’.
Participant information form
This form was created by the researcher and included questions that inquire about the socio-demographic and obstetric characteristics, experiences about the earthquake, and fertility intentions of the participants (Luppi et al., Reference Luppi, Arpino and Rosina2020; Bırni et al., Reference Bırni, Deniz, Karaağaç, Erişen, Kaya and Satıcı2023).
One of the primary objectives of the study was to determine changes in fertility intentions. In this regard, the literature contains similar studies with comparable measurements (Luppi et al., Reference Luppi, Arpino and Rosina2020; Malicka et al., Reference Malicka, Mynarska and Świderska2021). To measure fertility intention, women were asked, ‘Before the earthquake; were you planning to have children within the next 3 years?’ Those who answered yes to this question were asked the follow-up question, ‘Did the earthquake change your intention to have children?’ and prompted to choose one of the following options: ‘(a) No, (b) Yes, I plan to have children earlier/I plan to have more children, (c) Yes, I postponed my intention to have children until later, (d) Yes, I want to have fewer or no children compared to before the earthquake’. Since only a small number of participants (n = 3) stated that they planned to have children earlier or to have more children, participants were divided into two categories and coded as ‘No change, Earlier/More’ (0) and ‘Postponing, Giving up’ (1) (Figure 1).
Variable interpretation ploot.

Figure 1. Long description
A flowchart illustrating the impact of an earthquake on individuals’ intentions to have a child within the next three years. The first decision point asks if the individual intended to have a child before the earthquake. If the answer is no, the next question is whether the earthquake has changed this intention, with possible responses being no, intending to have a child sooner or more, intending to have a child later, or deciding never to have a child. If the initial answer is yes, the same follow-up question is asked with the same possible responses. The flowchart uses rectangles for decision points and branching paths to indicate different outcomes based on the individual’s response.
Brief Death Distress Scale (DDS)
The scale was developed by Dadfar and Lerter (Reference Dadfar and Lester2020) to measure death distress. It consists of nine items. The scale has three sub-dimensions: ‘Death Anxiety’ (items 1, 2, and 3), ‘Death Depression’ (items 4, 5, and 6), and ‘Death Obsession’ (items 7, 8, and 9). Each item is rated on a five-point Likert scale (1 = never, 5 = always). There are no reverse-coded items in the evaluation of the scale. The total score is obtained by summing the Likert values of the participant’s responses. The lowest possible score on the scale is nine, and the highest is forty-five. The adaptation of the scale to Turkish was performed by Yıldırım & Güler (Reference Yıldırım and Güler2021), and the internal consistency coefficients were calculated as .77 for death anxiety, .88 for death depression, and .91 for death obsession. In the present study, the internal consistency coefficient for the total scale was .80, and the coefficients for the sub-dimensions were .80 for death anxiety, .73 for death depression, and .90 for death obsession.
Data collection
The data for the study were collected using an online survey. The survey was created using Google Forms and distributed to participants via social media platforms (WhatsApp, Facebook, etc.). Prior the study, a pilot study was conducted with 10 participants who had characteristics similar to those of the sample to assess the comprehensibility of the survey form.
Statistical analysis
Data were analyzed using SPSS (Statistical Package for the Social Sciences) version 22.0. The conformity of the variables to normal distribution was assessed based on Skewness and Kurtosis values within the range of +1 and −1 (Leech, Reference Leech, Barrett and Morgan2007). Accordingly, the scores for the scale and its sub-dimensions used in the study were normally distributed. To assess the reliability of the measurement obtained from the scale, the internal consistency coefficient (Cronbach’s alpha) was calculated. Descriptive statistics (means, standard deviations, frequencies, and percentages) and analytical statistics (one-way analysis of variance, independent t-test, and Spearman’s correlation) were used to analyze the data. p < .05 was considered statistically significant in all analyses.
Results
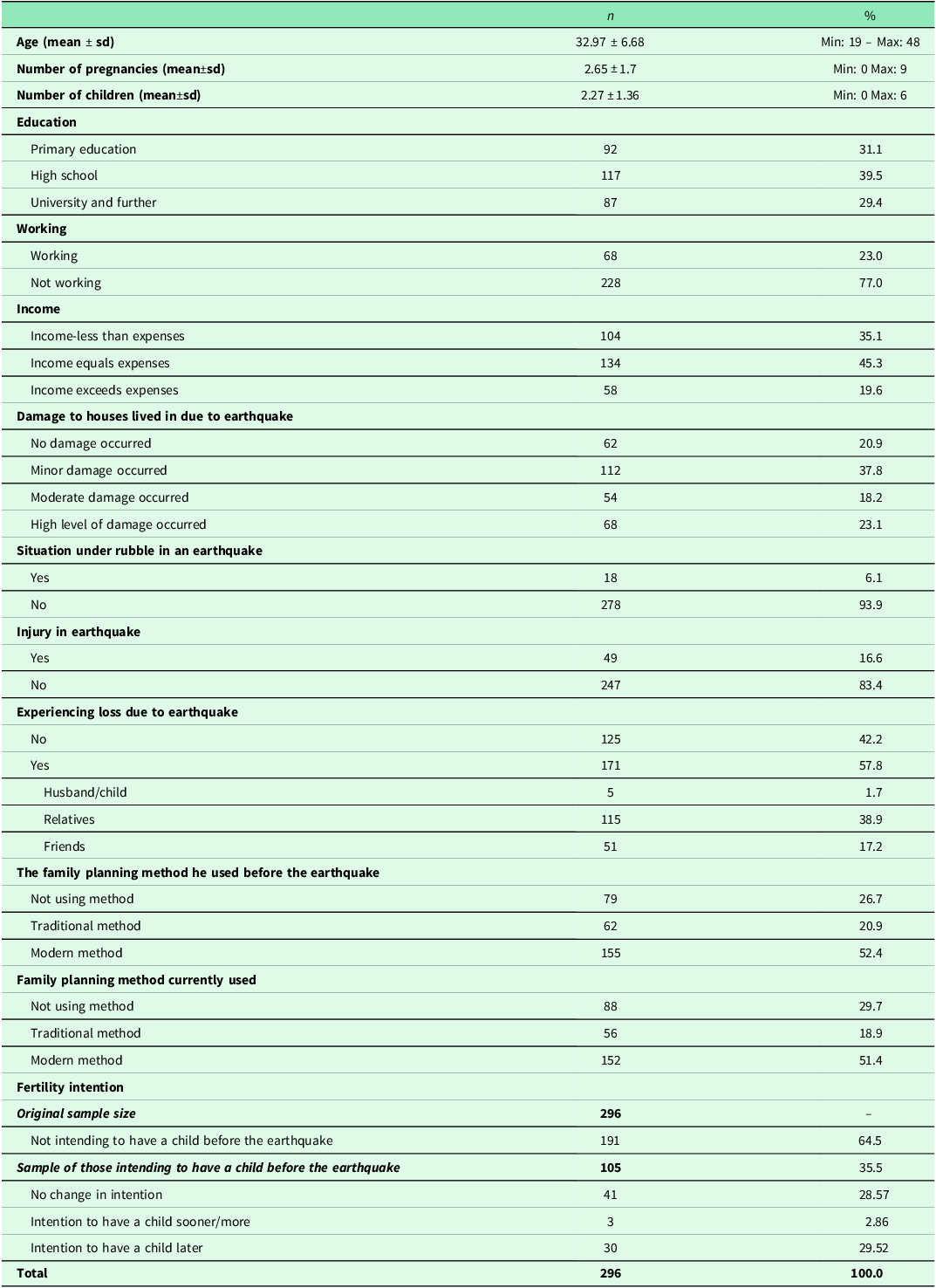
Table 1 presents descriptive data on women’s demographic characteristics, earthquake experiences, fertility characteristics, and fertility intentions.
Descriptive data on women’s demographics, earthquake experience, fertility characteristics, the explained change in childbearing intention due to the Earthquake

Table 1. Long description
The table presents data on women’s demographics, earthquake experience, and fertility characteristics. It includes information on age, number of pregnancies, number of children, education level, working status, income, damage to houses due to the earthquake, situation under rubble, injury during the earthquake, experiencing loss, family planning methods used before and after the earthquake, and fertility intentions. The table has 296 entries and covers various statistics and percentages related to these categories.
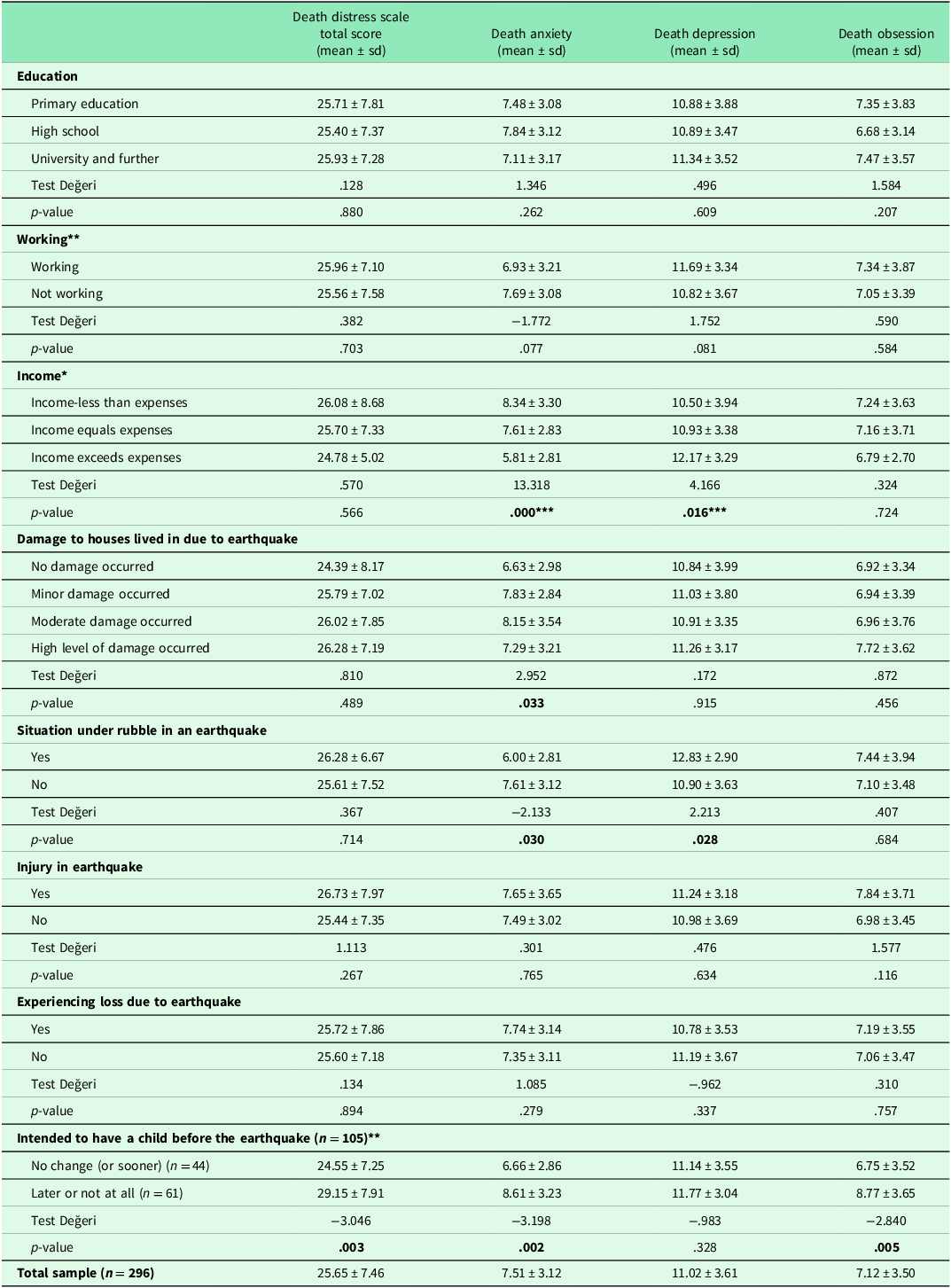
Table 2 presents variation in death distress across demographic characteristics, earthquake experience, fertility intentions, and changes in fertility intentions. Those with income higher than their expenses had lower death distress compared with those with income equal to or lower than their expenses. Those whose income exceeded their expenses had higher death depression compared with those whose income was lower than their expenses.
Death Distress Scale (DDS) scores according to women’s descriptive characteristics, earthquake experiences, fertility characteristics, and change in fertility intentions

Table 2. Long description
The table presents data on death distress scale scores, including death anxiety, death depression, and death obsession, across different characteristics and experiences of women. It includes categories such as education level, working status, income, damage to houses due to an earthquake, situation under rubble in an earthquake, injury in an earthquake, experiencing loss due to an earthquake, and intended fertility before the earthquake. The table has 19 rows and 17 columns, with each row representing a specific characteristic or experience and each column representing a different aspect of the death distress scale. Notable trends include variations in death distress scores based on income levels, damage to houses, and experiences during the earthquake.
*One-way ANOVA **İndependent T-test ***Post-hoc Tukey.
Death anxiety differed significantly according to the condition of the house damaged by the earthquake (p < .05). Those who stated that their house was moderately damaged after the earthquake had higher levels of death anxiety than those who stated that their house was undamaged. Furthermore, those who were trapped under debris during the earthquake had lower death anxiety and higher death depression than those who were not (p < .05) (Table 2).
Relationships between fertility characteristics, fertility intention, and death distress are presented below: Accordingly, there was a significant difference in death distress and death anxiety between women who experienced a change in fertility intentions and those who did not (p < .05). Compared with women who did not experience a change in fertility intentions, those who did had higher levels of death distress, death anxiety, and death obsession (Table 2).
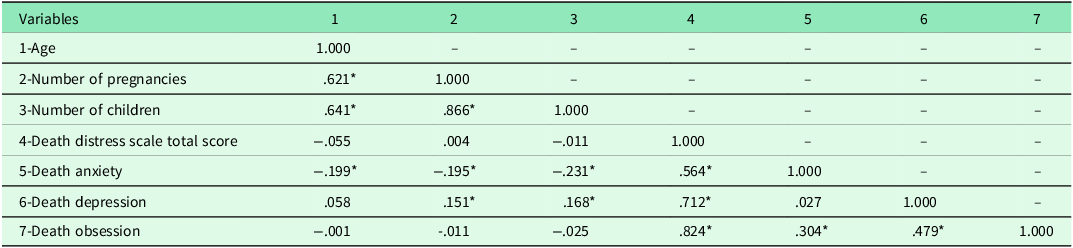
Table 3 shows the relationship between participants’ death distress and age, number of pregnancies, and number of children. Accordingly, a weak negative correlation was observed between age and death anxiety (r = −.199, p < .01). The number of pregnancies was weakly negatively correlated with death anxiety (r = −.195, p < .01) and weakly positively correlated with death depression (r = .151, p < .05). There were a weak negative correlation between the number of children and death anxiety (r = −.231, p < .01) and a weak positive correlation between the number of children and death depression (r = .168, p < .01). In addition, death obsession showed a weak positive correlation with death anxiety (r = .304, p <.01) and a moderate positive correlation with death depression (r = .479, p < .01).
Examining the relationship between women’s Death Distress Scale (DDS) scores, age, number of pregnancies, and number of children (n = 296)

Table 3. Long description
The table presents data on the relationship between women’s death distress scale scores, age, number of pregnancies, and number of children. It includes seven variables: age, number of pregnancies, number of children, death distress scale total score, death anxiety, death depression, and death obsession. The table has seven rows and seven columns, with correlation coefficients and significance values indicated. Notable trends include a weak negative correlation between age and death anxiety, and a weak positive correlation between the number of pregnancies and death depression. The number of children shows a weak negative correlation with death anxiety and a weak positive correlation with death depression. Death obsession is weakly positively correlated with death anxiety and moderately positively correlated with death depression.
Spearman’s Correlation *p < .01.
Discussion
The researchers’ aims are fourfold. Determination of death distress levels in women after the earthquake was carried out first. Accordingly, mean death distress level among the participants was found to be 25.65 ± 7.46. Birni et al. conducted a study with the survivors of the February 6, 2023 earthquake and found that the death distress levels of those directly affected by the earthquake (27.22 ± 7.01) were higher compared to those of individuals who had a loved one or second-degree relative affected by the earthquake (26.62 ± 6.90) and individuals unaffected by the earthquake (25.31 ± 9.72), and this difference was statistically significant. The death-distress levels of earthquake survivors reported by Bırni et al. are consistent with the findings of the present study.
Generally, death distress has a multidimensional structure including death anxiety, death depression, and death obsession (Dadfar and Lester, Reference Dadfar and Lester2020). Death depression is the most prominent feature of death distress and is defined as the grief experienced by an individual in relation to death (Alkış, Reference Alkış2023). This study identified bereavement-related depression as the most important factor associated with death-related distress among women. The results of another study showed that death depression is highest within 7–12 months after the loss of a loved one (Armas-Arráez et al., Reference Armas-Arráez, Padilla, Fernández-Mateos and Sánchez-Cabaco2023). The high level of death depression in the present study can be explained by the study being conducted within the first year after the earthquake. Death anxiety, conceptualized as a key component of death distress, encompasses the fears, negative emotions, and thoughts that individuals experience in relation to their own mortality and the potential loss of significant others (Abdel-Khalek, Reference Abdel-Khalek2004; Menzies and Menzies, Reference Menzies and Menzies2023; Menzies et al., Reference Menzies, McMullen, Riotto, Iliescu, Petrovic and Remfrey2024). In the present study, participants’ death anxiety levels were moderate and constituted the second most significant component, after death depression. This finding is consistent with the growing body of evidence indicating that earthquake survivors commonly experience elevated anxiety symptoms; studies following the 2023 Kahramanmaraş earthquakes found that more than 51% of adult survivors screened positive for psychological distress, with women identified as a particularly vulnerable group (Çıtak and Dadandı, Reference Çıtak and Dadandı2024). Furthermore, research conducted specifically on death anxiety among earthquake victims in Turkey has confirmed that this construct is significantly elevated in post-disaster populations (Cenat, Reference Cénat, McIntee and Blais-Rochette2020; Akturk and Yenigun, Reference Akturk and Yenigun2024; Gümüş Şekerci et al., Reference Gümüş Şekerci, Ayvazoğlu and Çekiç2024). The third component of death distress identified in this sample was death obsession, which involves recurring thoughts, intrusive images, and rumination focused on one’s own death or the death of significant others (Yıldırım and Güler, Reference Yıldırım and Güler2021). Death obsession levels were moderate among the participants. Major disasters, such as earthquakes, remind people of their vulnerability and the fleeting nature of life. This can increase thoughts about death and lead people to consider their own deaths and those of their loved ones.
In this study, a negative correlation was found between age and death anxiety, indicating a decrease in death anxiety with increasing age. This finding is consistent with longitudinal evidence demonstrating that death anxiety tends to decline with advancing age, as older individuals may develop greater psychological adaptation and acceptance of mortality over time (Guo et al., Reference Guo, Wister, Mitchell and Li2024). These differences may be attributed to older adults developing a fear of living because of physical problems and social isolation. As the fear of living becomes more dominant than the fear of death, death anxiety decreases among older adults. On the contrary, it is argued that young individuals experience more death anxiety compared to elderly individuals because they have more to do in life and have not yet achieved their goals (Gökha, Reference Göka2010). The findings obtained in the present study support this view.
In the present study, individuals with higher income levels had lower levels of death anxiety and higher levels of death depression. As indicated by Hallegatte et al. (Reference Hallegatte, Vogt-Schilb, Bangalore and Rozenberg2017), disasters can disproportionately affect low-income individuals, leaving them homeless. However, the study’s findings suggest that lower levels of death anxiety among individuals with higher incomes may be attributed to their residence in safer housing and to their greater resilience to natural disasters such as earthquakes. High income levels can provide an advantage in coping with disasters by offering more financial resources and strength, leading individuals to feel more secure and reduce their death anxiety (Huang et al., Reference Huang, Du and Qu2021).
Death anxiety among women decreases as the numbers of pregnancies and children increase. Becoming a parent can reduce death anxiety in individuals through factors such as finding the meaning and purpose of life, ensuring the continuation of life, and seeing themselves contributing to a greater purpose (Nomaguchi and Milkie, Reference Nomaguchi and Milkie2020). Women whose houses were moderately damaged experienced higher death anxiety than those whose houses were not damaged. This indicates that the fear and anxiety experienced during the earthquake tend to increase death anxiety among individuals whose homes are damaged. Additionally, greater economic and social losses may contribute to increased death anxiety. Therefore, understanding the negative effects of the earthquake on individuals’ mental health and providing support can be crucial.
In the present study, women trapped under debris had lower death anxiety but higher death depression. The women trapped under the debris may have felt a sense of survival. This, together with the awareness of the dangerous situation, can create a sense of inner strength and resilience that supports survival, leading to a reduction in anxiety about death. However, women trapped under debris may experience depression and grief. This may be linked to losses and trauma and lead to a higher incidence of death-related depression. This process of depression and grief leads to a decrease in death anxiety, but it may also lead to an increase in death depression (Yıldırım and Güler, Reference Yıldırım and Güler2021; Kalyoncu et al., Reference Kalyoncu, Aydoğdu, Polat, Karabulut, Keskin and Özkan2023).
Fertility intention is one of the most robust predictors of couples’ fertility behavior and is influenced by various factors. The literature emphasizes that fertility decisions are filled with uncertainty. These uncertainties are considered the reason for the mismatch between fertility intentions and actual fertility. Recent disasters, such as the coronavirus disease 2019 (COVID-19) pandemic and earthquakes, contribute to this uncertainty and lead to postponement of fertility intentions (Malicka et al., Reference Malicka, Mynarska and Świderska2021). The results obtained in the present study support this view. While 36.5% of women expressed the intention to have a child within the next 3 years before the earthquake, more than half of these women reported changes to their fertility intentions after the earthquake, including postponing them or completely giving up on them. Studies examining the impact of Covid-19 pandemic, which is considered a biological disaster, on fertility intentions have found that approximately one-third of women postponed their fertility intentions or expressed a desire to have fewer children (Lindberg et al., Reference Lindberg, VandeVusse, Mueller and Kirstein2020). In a study covering Italy, France, Germany, Spain, and the United Kingdom, 38%–58% of individuals reported postponing their fertility intentions due to the Covid-19 pandemic (Luppi et al., Reference Luppi, Arpino and Rosina2020). As a result of the earthquake, families often face economic difficulties and may have fewer financial resources. This may affect married women’s intentions to have children, since economic uncertainty and reduced resources can increase the financial burden of having children, thereby reducing fertility intentions.
According to the results of the present study, individuals with changes in fertility intentions had higher levels of death distress, death anxiety, and death obsession compared with those without such changes. Losses and traumatic experiences caused by earthquakes can affect the grief and loss processes of women. Changes in fertility intentions can be perceived as a need to mourn losses and complete the mourning process. This process of grief and loss may lead to an increase in death anxiety and death obsession. After an earthquake, women often experience psychological stress and trauma. Changes in fertility intentions may reflect stress and trauma experienced by individuals, leading to an increase in death anxiety and obsession.
Conclusions
The present study found a moderate level of death distress among women. Psychological symptoms, such as death anxiety, depression, and obsession, which constitute a significant component of traumatic experiences following an earthquake, are essential for assessing the emotional and psychological needs of individuals and for providing appropriate support services. Individuals experiencing distress related to death may need psychological support. These symptoms may negatively affect activities of daily living and lead to long-term psychological health problems. Death distress has emerged as a crucial component in the diagnosis of psychological trauma among trauma-exposed patients. Measurement of these symptoms is therefore essential for identifying appropriate treatment and rehabilitation programs.
The results also showed that more than half of the women who intended to give birth before the earthquake either postponed or completely abandoned their plans. Changes in fertility intentions are an important source of data for the development and implementation of family planning policies and programs. Based on these data, governments and local authorities can provide family planning services tailored to the needs of post-earthquake communities.
Changes in fertility intentions are closely related to fertility rates, but they are also highly variable due to external factors. According to the results of the present study, individuals with changes in fertility intentions had higher levels of death distress, death anxiety, and death obsession compared to those without such changes. Therefore, our study contributes a new perspective and additional information to literature.
Limitations
In interpreting the study data, certain important limitations should be considered. First, a control group not exposed to the earthquake could not be included in this study. For this reason, the sample in which the effects of the earthquake were examined could not be compared to a control group to eliminate confounding effects of other variables that may be related to mental health. Another limitation is that the data were collected online, which means that the population consisted of individuals who had internet access, owned a computer or smartphone, and knew how to use these technologies. Therefore, the results obtained can be generalized to the participants and are valid for the time period during which the research was conducted.
In the present study, the causal relationship between death distress and fertility intention could not be confirmed. Future studies should evaluate and confirm this relationship in more detail.
Data availability statement
The data underlying this article in the original language will be shared by the corresponding author upon reasonable request.
Acknowledgements
We thank all the participants.
Author contributions
In accordance with the International Committee of Medical Journal Editors (ICMJE) criteria, each author has made equal contributions to this work and fulfilled the stipulated authorship requirements.
Funding statement
This research received no specific grant from any funding agency, whether commercial or not-for-profit.
Competing interests
The authors declare none.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines on human experimentation – in our case, those of the Institutional Ethics Committee of the Necmettin Erbakan University of Health Sciences Scientific Research (App. No:2023/37-549) – and with the Helsinki Declaration of 1975, as revised in 2008. Before completing the survey, participants were informed about the study’s purpose and methodology and were shown a consent form. After indicating that they had been informed and had given their consent, they proceeded to answer the survey questions. The survey was prepared following standardized procedures in Google Forms to ensure that participants could respond only once.


 Open access
Open access