


Impact statements
This review shares findings on a historically overlooked public health crisis: access to sexual and reproductive health (SRH) care for women with severe mental illness (SMI) in low- and middle-income countries (LMICs). By synthesizing qualitative evidence from the past two decades, this study identifies barriers and facilitators that hinder or promote access to SRH care. Our findings show how women with SMI face barriers, such as sociocultural, autonomy-related, and systemic inaccessibility challenges that impact access to SRH care. This has broad implications for mental health integration in global systems and reproductive and gender equity, especially for women with SMI – a group that faces intersectional, layered barriers to care due to sexism, ableism, stigma and institutional marginalization. This research can contribute to evidence-based interventions for international organizations, humanitarian groups and local policymakers to create targeted, community-specific interventions that address the nuances of access to both reproductive and mental health services for women in LMICs. By amplifying the experiences of women with SMI, their caregivers, and healthcare providers, this study aims to further research that assesses inclusive SRH care for women with SMI and advocates for a global health agenda that is more inclusive, comprehensive and rights-based.
Introduction
Sexual and reproductive health (SRH) care encompasses access to effective contraception, evidence-based sexual education, appropriate sexually transmitted infection (STI) treatment, safe antenatal, childbirth and postnatal care, and the right to medical treatment and legal action in case of sexual violence. Accessing SRH care is fundamental to the realization of SRH and rights, yet millions of women worldwide, especially those in low- and middle-income countries (LMICs), remain chronically underserved (Starrs et al., Reference Starrs, Ezeh, Barker, Basu, Bertrand, Blum, Coll-Seck, Grover, Laski, Roa, Sathar, Say, Serour, Singh, Stenberg, Temmerman, Biddlecom, Popinchalk, Summers and Ashford2018; Kaul et al., Reference Kaul, Connell-Jones, Paphitis and Oram2024). Five dimensions of healthcare accessibility have been identified, and these can be applied to SRH care: (a) approachability: the ability to perceive a need for care; (b) acceptability: the ability to seek care within the constraints of sociocultural values and expectations; (c) availability and accommodation: the ability to reach care, both physically and in a timely manner; (d) affordability: the ability to pay for care through income or social capital; and (e) appropriateness: the ability to engage with care in a way that is adequate for an individual’s unique needs (Levesque et al., Reference Levesque, Harris and Russell2013). This five-pronged framework can help distinguish facilitators of care access and evaluate the alignment between healthcare systems and the needs of individuals, families and communities, allowing the conception of more comprehensive interventions (McIntyre et al., Reference Mcintyre, Thiede and Birch2009). Despite global commitments to bettering access to SRH care, such as Sustainable Development Goal 3.7, which aims for universal access to SRH services by 2030, social and institutional barriers, like shame, stigma and lack of provision of care, continue to prevent women in LMIC from accessing appropriate and necessary SRH care. The effects of poverty, sociocultural pressures and systemic underfunding of, and widespread stigma surrounding, SRH services restrict the accessibility of SRH care in these settings (Desrosiers et al., Reference Desrosiers, Betancourt, Kergoat, Servilli, Say and Kobeissi2020).
Among the most marginalized are women living with severe mental illness (SMI), which are mental illnesses associated with enduring disability, including severe depression, schizophrenia and bipolar disorder. The United Nations Convention on the Rights of Persons with Disabilities (CRPD) states that people with disabilities, which includes people living with SMI, should have access to the same range and quality of affordable SRH care as provided to other persons (United Nations, 2006). Yet due to the intersectional layers of gender and health status discrimination, women with SMI face compounded barriers to SRH care that reflect not only stigma around mental illness, but also sexism, ableism and institutional marginalization; this can manifest through limited access to menstrual products and contraception, SRH education and abortion services (Howard et al., Reference Howard, Wilson, Reilly, Moss, Mishra, Coupland-Smith, Riecher-Rössler, Seedat, Smith, Steinberg, Van Ditzhuijzen and Oram2025). In under-served populations, these challenges can be intensified: for instance, in LMIC settings, women with SMI are vulnerable to heightened risks of HIV and other STIs, sexual dysfunction and stigma, contraception avoidance or coercion, sexual violence and complexities in pregnancy (Sisodia et al., Reference Sisodia, Hammond, Leonardi-Bee, Hanlon and Asher2025).
Evidence synthesis is crucial because while empirical research usually focuses on women with single diagnoses or in specific countries, a broader synthesized understanding is necessary to identify predominant themes, recurring gaps and contextual variations in access to care. A previous scoping review identified a number of qualitative studies exploring the SRH needs of women with SMI in LMICs but did not include in-depth analysis (Sisodia et al., Reference Sisodia, Hammond, Leonardi-Bee, Hanlon and Asher2025). A previous systematic review examined barriers and facilitators in accessing SRH care for women with SMI, but concentrated primarily on HIV and family planning services and drew largely on studies from high-income settings (Brown et al., Reference Brown, Tassie, Carlisle, Covshoff, Ronaldson, Williams, Smith, Trevillion, Hughes and Heslin2025). While experiences in HIC may have broad relevance (Usman et al., Reference Usman and Schaafsma2025), a focus on LMIC allows us to consider the specific issues that may arise from lower availability of formal resources, more pronounced gender inequalities and diverse cultural and social contexts.
By drawing on qualitative studies that center on lived experiences in various contexts, this qualitative systematic review aimed to address these gaps by exploring the barriers and facilitators to access to SRH care for women with SMI in LMICs.
Methods
This systematic review was conducted in accordance with the Joanna Briggs Institute (JBI) meta-aggregative approach to the synthesis of qualitative evidence (Munn et al., Reference Munn, Porritt, Lockwood, Aromataris and Pearson2014; Lockwood et al., Reference Lockwood, Munn and Porritt2015; Munn et al., Reference Munn, Dias, Tufanaru, Porritt, Stern, Jordan, Aromataris and Pearson2021). This approach seeks to observe the original meanings reported by the primary researchers. Analysis involves organizing primary study findings into categories and then into synthesized findings that aim to generate meaningful insights and recommendations to inform practice. The review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (PRISMA, 2020) (see Supplementary File S1). The study protocol was registered with PROSPERO (ID:573143).
Inclusion and exclusion criteria
We included studies that met the following criteria:
-
• Concept: Studies that explored barriers and facilitators for women with SMI (including schizophrenia, bipolar disorder, severe depression and psychosis) in accessing SRH care (including, but not limited to, care related to family planning, contraception, antenatal and postnatal care, STI treatment, abortion and fertility).
-
• Population: Studies that included women aged 18 years or older diagnosed with an SMI; or included both sexes aged 18 years or older if the results could be differentiated by gender or, in the case of aggregated data, if there were at least 80% women; or included families, community members and professionals that interact with women aged 18 years or older diagnosed with an SMI. We included studies that involved participants with depression, where it was defined by authors as SMI and/or where participants were receiving treatment from specialized facilities.
-
• Context: We included studies conducted in LMICs as defined by the World Bank (World Bank, 2024).
-
• Study design: Peer-reviewed qualitative studies were included with no restriction on study type.
We excluded studies focused only on men and studies focused on women diagnosed with mild depression, post-partum depression, or anxiety disorders.
Search strategy and study selection
A preliminary search was conducted on MEDLINE using the three concepts: “severe mental illness,” “sexual and reproductive health,” and “low- and middle-income countries.” The final search strategy, developed with a research librarian, combined Medical Subject Headings (MeSH) and keywords (see Supplementary File S2). We searched the electronic bibliographic databases MEDLINE, EMBASE and PsycINFO on July 31, 2024, adapting the strategy as required. The search was limited to studies from 2004 to 2024 to ensure relevance of findings and recommendations to current health systems. Only English language articles were included for logistical reasons (Hannes et al., Reference Hannes, Petry and Heyvaert2017). The reference lists of included studies were screened for additional studies.
Study selection
Studies were imported into Covidence, duplicates removed, and titles and abstracts screened, with 30% double screened due to operational reasons. Any disagreements were resolved through discussion between reviewers. Full texts of relevant studies were then retrieved and screened against inclusion criteria by one reviewer, again due to operational reasons.
Assessment of methodological quality
We assessed the methodological quality of eligible studies using the ten criteria of the JBI critical appraisal checklist for qualitative research. Studies were not excluded based on scores because low-quality studies can also generate relevant and usable findings (Lockwood et al., Reference Lockwood, Munn and Porritt2015).
Data extraction and assessment
We extracted study characteristics (i.e., country, phenomena of interest, participant characteristics, sample size, data collection and analysis methods) from each article using a data extraction tool. Specific findings and respective supporting evidence (i.e., quotations) were extracted and classified as facilitators or barriers. The extracted findings were evaluated for credibility using the following definitions (JBI, 2025):
-
• Unequivocal (U): The findings are accompanied by a contextually rooted, detailed, rich and clearly associated illustration (e.g., participant quote or fieldwork observation).
-
• Credible (C): The findings are accompanied by an illustration lacking detail, richness or clear association with it.
-
• Not Supported (NS): The findings are not supported by the data or there are no data to support the finding.
Data synthesis
The findings were grouped into categories and unsupported findings were eliminated to improve the validity and credibility (Lockwood et al., Reference Lockwood, Munn and Porritt2015). Categorized findings were then further grouped into synthesized findings. We graded the final synthesized findings using the ConQual approach for establishing confidence in the output of qualitative synthesis. Studies were initially ranked as “high” in terms of both dependability and credibility. We then scored each study for dependability based on five pre-determined questions from the JBI critical appraisal tool, with studies downgraded in the case of low-quality ratings. The overall dependability of each synthesized finding was determined by JBI critical scores (Munn et al., Reference Munn, Porritt, Lockwood, Aromataris and Pearson2014; Munn et al., Reference Munn, Dias, Tufanaru, Porritt, Stern, Jordan, Aromataris and Pearson2021).
Results
Study inclusion
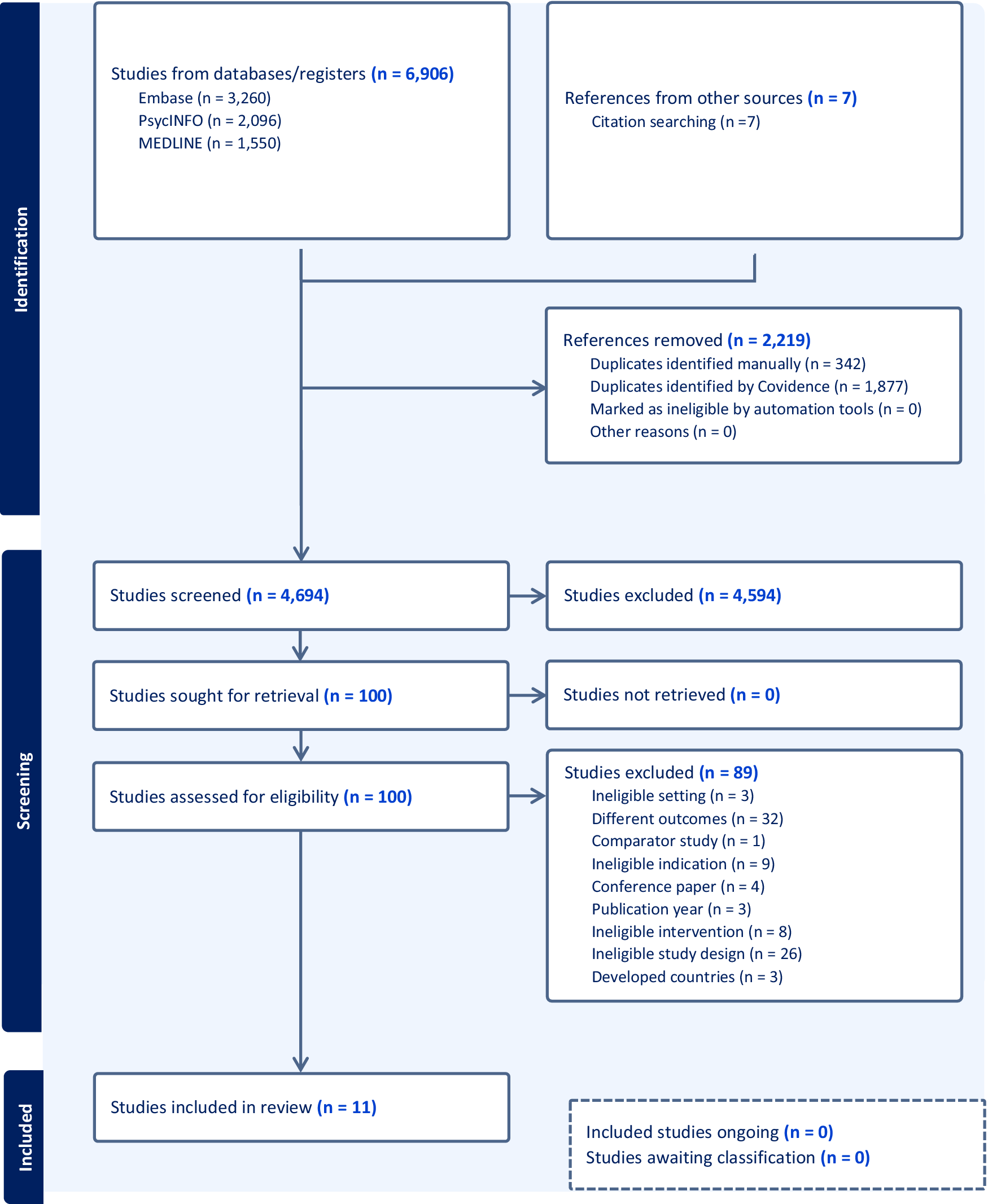
The search identified 6,913 records (Figure 1). Following the removal of 2,219 duplicates, 4,694 publications were screened for inclusion based on the title and abstract. A total of 4,594 studies were excluded at this stage, leaving 100 full texts which were screened for inclusion. Eleven papers met the inclusion criteria.
PRISMA flow diagram.

Figure 1. Long description
At the top, two boxes: left, Studies from databases/registers n equals 6,906, broken down as Embase n equals 3,260, Psyc I N F O n equals 2,096, M E D L I N E n equals 1,550; right, References from other sources n equals 7, Citation searching n equals 7. Both feed into References removed n equals 2,219, with Duplicates identified manually n equals 342, Duplicates identified by Covidence n equals 1,877, Marked as ineligible by automation tools n equals 0, Other reasons n equals 0. The remaining Studies screened n equals 4,694, with a right branch for Studies excluded n equals 4,594. Downward, Studies sought for retrieval n equals 100, with a right branch for Studies not retrieved n equals 0. Next, Studies assessed for eligibility n equals 100, with a right branch for Studies excluded n equals 89, detailed as Ineligible setting n equals 3, Different outcomes n equals 32, Comparator study n equals 1, Ineligible indication n equals 9, Conference paper n equals 4, Publication year n equals 3, Ineligible intervention n equals 8, Ineligible study design n equals 26, Developed countries n equals 3. The final box at the bottom is Studies included in review n equals 11. A dashed box below notes Included studies ongoing n equals 0, Studies awaiting classification n equals 0.
Methodological quality
The included studies’ quality ranged from 40%–100%. All the studies met JBI criteria Q3 (congruity between the research methodology and data collection methods), Q4 (congruity between the research methodology and data representation/analysis) and Q7 (influence of the researcher on the research is addressed). The fewest number of studies met Q6 (locating the researcher culturally or theoretically; see Supplementary File S3).
Characteristics summary of studies included
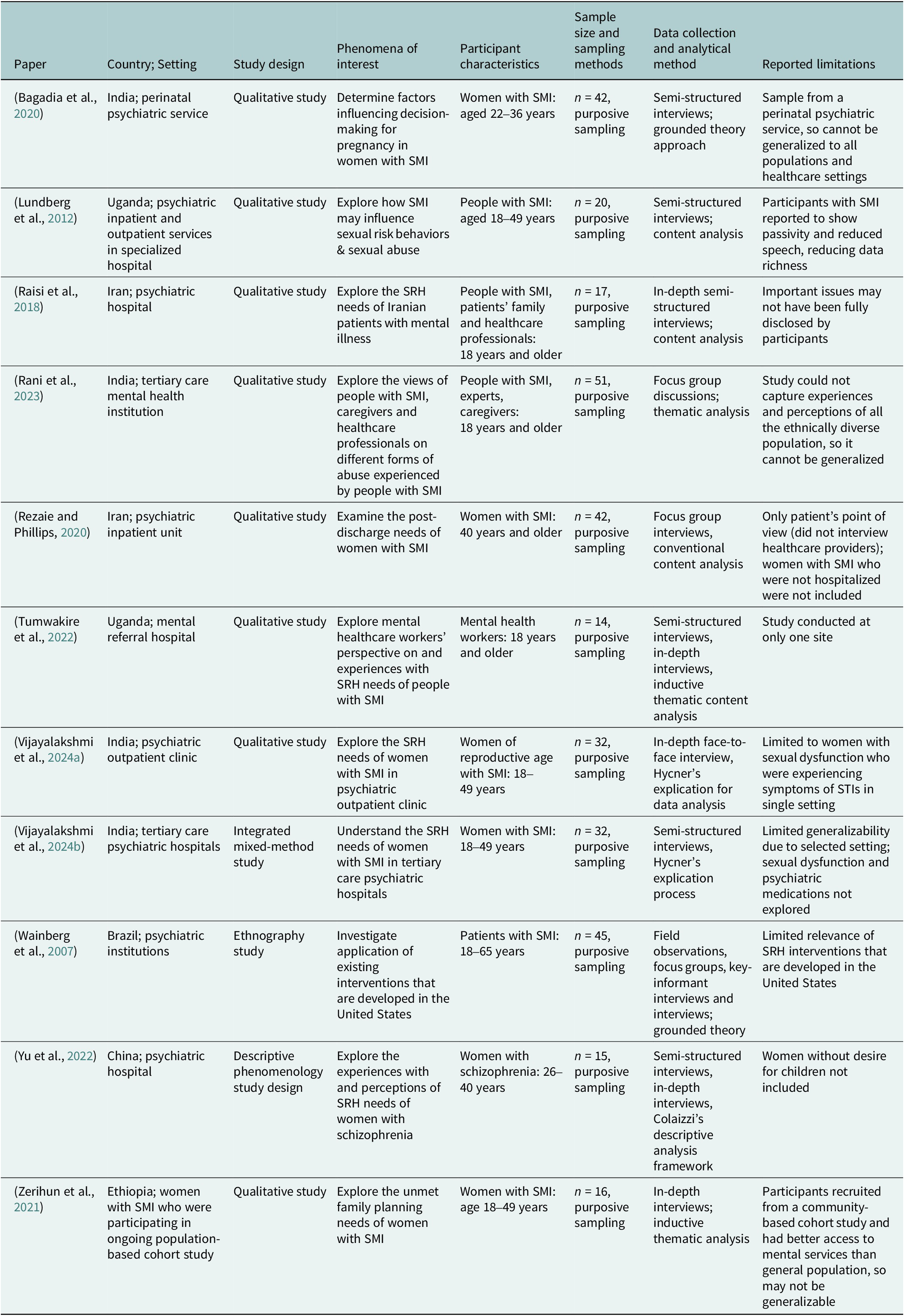
The included studies were conducted in India (n = 4), Uganda (n = 2), Iran (n = 2), Ethiopia (n = 1), Brazil (n = 1) and China (n = 1) (Table 1). Data collection methods included in-depth, semi-structured or key informant interviews, focus group discussions and participant observation. Data analysis and research methods included thematic analysis, content analysis, and grounded theory. Study participants included women with SMI, family members and healthcare providers.
Characteristics of the included studies

Table 1. Long description
Column headers from left to right are Paper, Country and Setting, Study design, Phenomena of interest, Participant characteristics, Sampling methods, Data collection and analytical method, and Reported limitations. The first row details Bagadia et al., 2020, India, perinatal psychiatric service, qualitative study, factors influencing pregnancy decision-making in women with S M I, women aged 22 to 36 years, n equals 42, purposive sampling, semi-structured interviews with grounded theory, limitation is sample from perinatal psychiatric service not generalizable. The second row is Lundberg et al., 2012, Uganda, psychiatric inpatient and outpatient services, qualitative study, S M I influence on sexual risk behaviors and abuse, people aged 18 to 49 years, n equals 20, purposive sampling, semi-structured interviews with content analysis, limitation is participant passivity and reduced speech. The third row is Raisi et al., 2018, Iran, psychiatric hospital, qualitative study, S R H needs of Iranian patients with mental illness, people with S M I, family and healthcare professionals aged 18 years and older, n equals 17, purposive sampling, in-depth semi-structured interviews with content analysis, limitation is incomplete disclosure of issues. The fourth row is Rani et al., 2023, India, tertiary care mental health institution, qualitative study, views on abuse experienced by people with S M I, people with S M I, experts, caregivers aged 18 years and older, n equals 51, purposive sampling, focus group discussions with thematic analysis, limitation is lack of generalizability to ethnically diverse populations. The fifth row is Rezaie and Phillips, 2020, Iran, psychiatric inpatient unit, qualitative study, post-discharge needs of women with S M I, women aged 40 years and older, n equals 42, purposive sampling, focus group interviews with conventional content analysis, limitation is only patient perspective included. The sixth row is Tumwakire et al., 2022, Uganda, mental referral hospital, qualitative study, mental healthcare workers’ perspectives on S R H needs, mental health workers aged 18 years and older, n equals 14, purposive sampling, semi-structured and in-depth interviews with thematic content analysis and inductive approach, limitation is single site. The seventh row is Vijayalakshmi et al., 2024a, India, psychiatric outpatient clinic, qualitative study, S R H needs of women with S M I, women of reproductive age with S M I aged 18 to 49 years, n equals 32, purposive sampling, in-depth face-to-face interview with Hycner's explication, limitation is focus on women with sexual dysfunction and S T I symptoms in single setting. The eighth row is Vijayalakshmi et al., 2024b, India, tertiary care psychiatric hospitals, integrated mixed-method study, S R H needs of women with S M I, women aged 18 to 49 years, n equals 32, purposive sampling, semi-structured interviews with Hycner's explication process, limitation is limited generalizability and unexplored sexual dysfunction and psychiatric medications. The ninth row is Wainberg et al., 2007, Brazil, psychiatric institutions, ethnography study, application of interventions developed in the United States, patients aged 18 to 65 years, n equals 45, purposive sampling, field observations, focus groups, key-informant interviews, grounded theory, limitation is limited relevance of U S interventions. The tenth row is Yu et al., 2022, China, psychiatric hospital, descriptive phenomenology study, S R H needs of women with schizophrenia, women aged 26 to 40 years, n equals 15, purposive sampling, semi-structured and in-depth interviews with Colaizzi's descriptive analysis, limitation is exclusion of women without desire for children. The eleventh row is Zerihun et al., 2021, Ethiopia, women with S M I in population-based cohort study, qualitative study, unmet family planning needs, women aged 18 to 49 years, n equals 16, purposive sampling, in-depth interviews with thematic analysis and inductive approach, limitation is participants had better access to mental services than general population.
Review findings
From the included studies, a total of 78 findings were extracted. Of these, 74 (~95%) findings were “unequivocal” and 4 (~5%) were “credible.” There were no unsupported findings. Findings were grouped into 33 categories (24 barriers and 9 facilitators), and finally into four synthesized findings (see Supplementary File S4). In Figures 2 to 5, barriers are in red boxes and facilitators are in green boxes with the synthesized finding in the middle.
Synthesized finding 1.

Figure 2. Long description
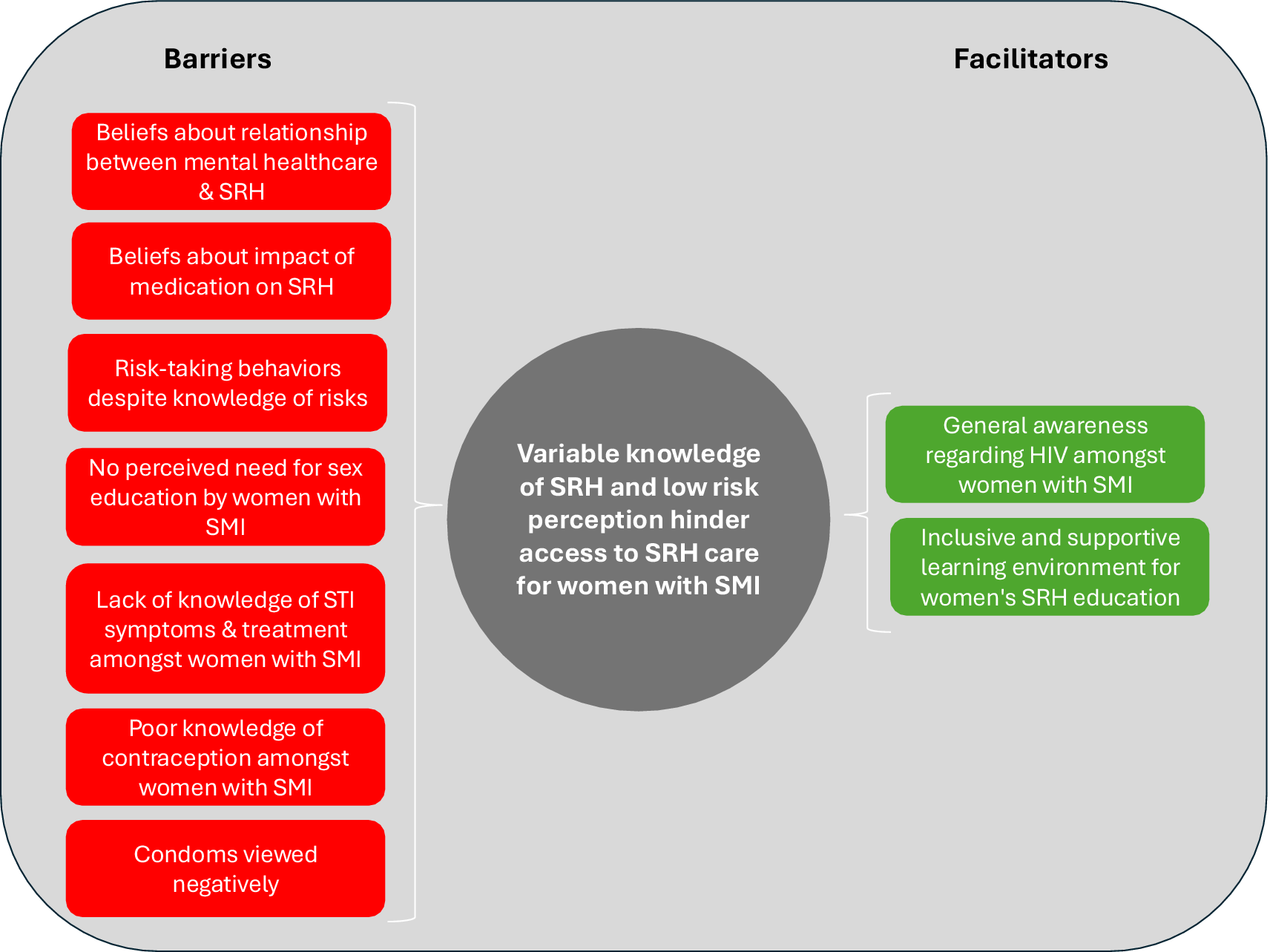
From left to right, the leftmost column labeled Barriers contains seven red rounded rectangles stacked vertically: Beliefs about relationship between mental healthcare and S R H, Beliefs about impact of medication on S R H, Risk-taking behaviors despite knowledge of risks, No perceived need for sex education by women with S M I, Lack of knowledge of S T I symptoms and treatment amongst women with S M I, Poor knowledge of contraception amongst women with S M I, and Condoms viewed negatively. The central gray circle states Variable knowledge of S R H and low risk perception hinder access to S R H care for women with S M I. The rightmost column labeled Facilitators contains two green rounded rectangles stacked vertically: General awareness regarding H I V amongst women with S M I, and Inclusive and supportive learning environment for women's S R H education.
Synthesized finding 2.

Figure 3. Long description
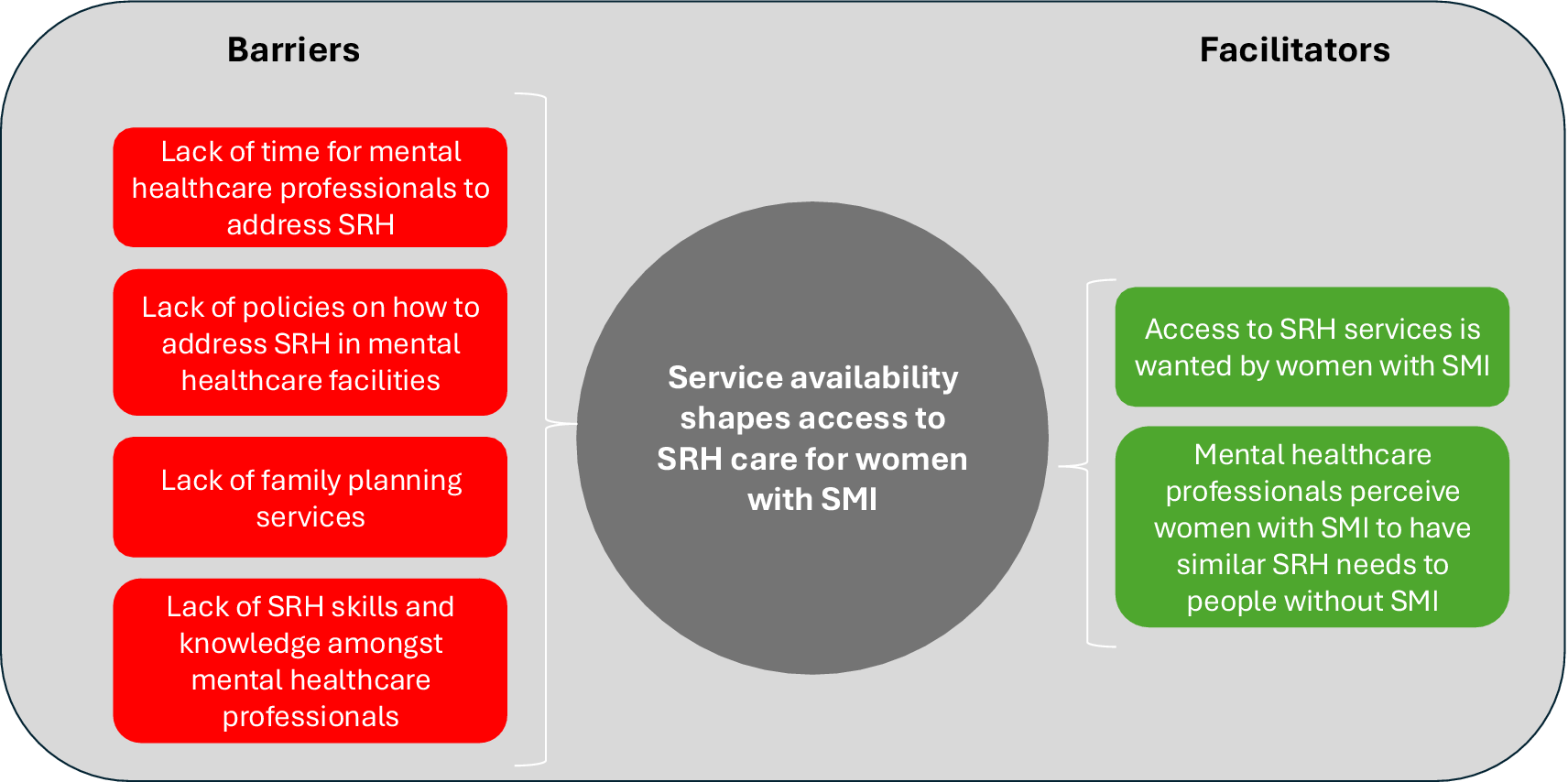
At the center is a grey circle labeled Service availability shapes access to S R H care for women with S M I. To the left, under Barriers, four red boxes list Lack of time for mental healthcare professionals to address S R H, Lack of policies on how to address S R H in mental healthcare facilities, Lack of family planning services, and Lack of S R H skills and knowledge amongst mental healthcare professionals. To the right, under Facilitators, two green boxes list Access to S R H services is wanted by women with S M I and Mental healthcare professionals perceive women with S M I to have similar S R H needs to people without S M I.
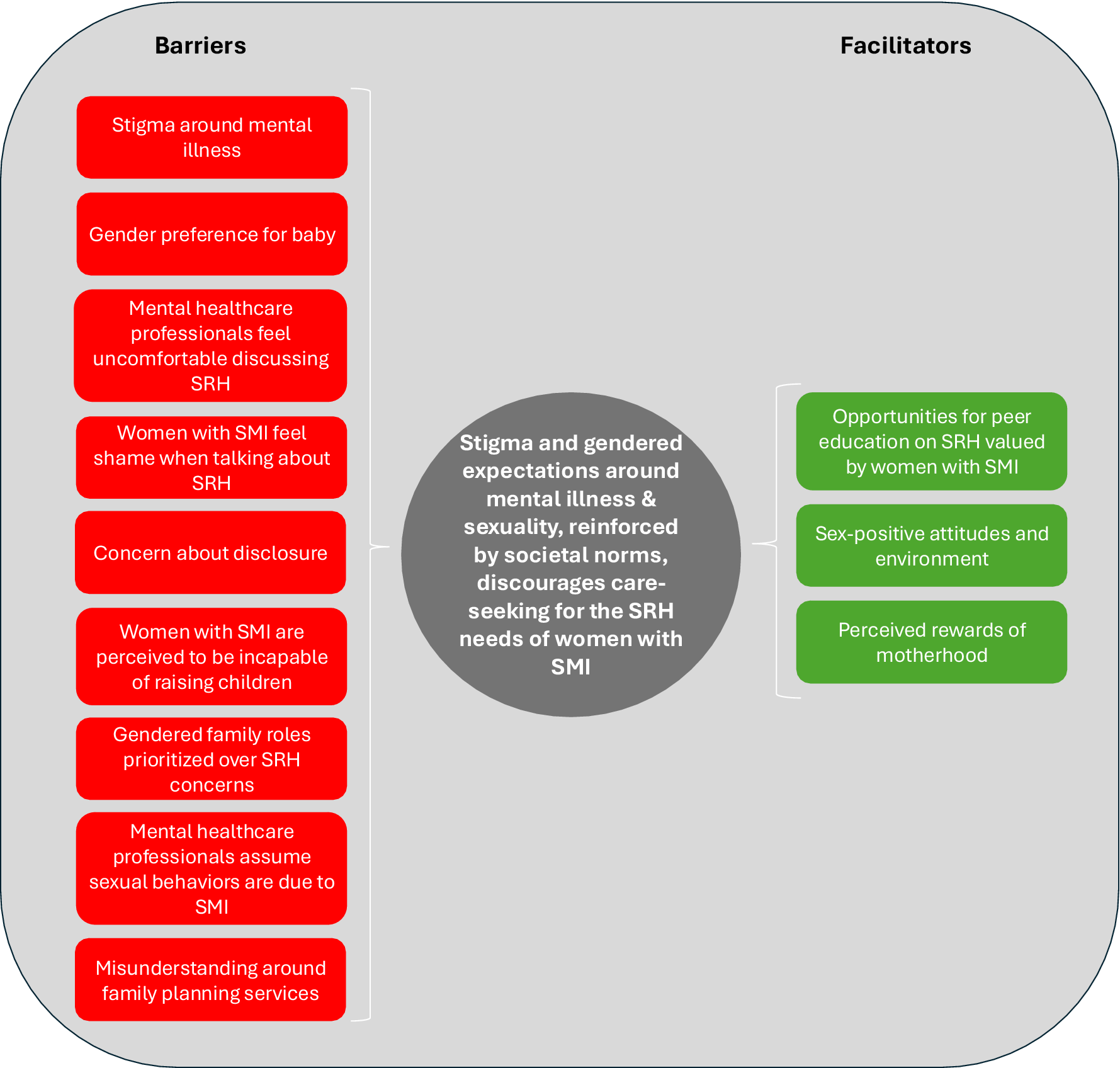
Synthesized finding 3.

Figure 4. Long description
On the left, under the heading Barriers, nine red boxes are stacked vertically: stigma around mental illness, gender preference for baby, mental healthcare professionals feel uncomfortable discussing S R H, women with S M I feel shame when talking about S R H, concern about disclosure, women with S M I are perceived to be incapable of raising children, gendered family roles prioritized over S R H concerns, mental healthcare professionals assume sexual behaviors are due to S M I, misunderstanding around family planning services. At the center, a gray circle states that stigma and gendered expectations around mental illness and sexuality, reinforced by societal norms, discourage care-seeking for the S R H needs of women with S M I. On the right, under the heading Facilitators, three green boxes are stacked vertically: opportunities for peer education on S R H valued by women with S M I, sex-positive attitudes and environment, perceived rewards of motherhood.
Synthesized finding 4.

Synthesized finding 1: Variable knowledge of SRH and low risk perception hinder access to SRH care for women with SMI (Figure 2)
Barriers
Findings show that women with SMI had variable knowledge about the effects of SMI on their SRH (Yu et al., Reference Yu, Wang, Wang, Ma, Li and Zhou2022). Some women were fearful about the effect of SMI on pregnancy, with women in both Iran and India expressing a desire to have a “healthy” baby (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020; Rezaie and Phillips, Reference Rezaie and Phillips2020). Concerns extended to psychiatric treatment for SMI as well. Some women perceived their STI symptoms to be side effects of their psychiatric medication (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b), while others feared that their medication would have negative impacts on their fetus (Yu et al., Reference Yu, Wang, Wang, Ma, Li and Zhou2022). In response, some women stopped taking psychiatric medication during pregnancy, but subsequently feared relapse of their SMI (Yu et al., Reference Yu, Wang, Wang, Ma, Li and Zhou2022). Women with SMI also attributed the experienced decrease in sexual desire to psychiatric medication (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020; Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b). Despite consulting perinatal psychiatrists, women in an Indian study reported that such views about the effects of medications on SRH remained unchanged (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020), suggesting a gap not in awareness of potential side effects (e.g., reduced sexual desire) but in receiving adequate information about which medications are most likely to cause these effects and what alternative treatment options may exist.
Lack of medical knowledge also manifested in decreased awareness of STI symptoms and treatment among women with SMI (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Chacko and Prathyusha2024a). Some believed that STI symptoms were a result of other unrelated health conditions, like partners’ smoking addictions (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b). When experiencing STI symptoms, some women did not know of the possible treatment options (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b).
Low levels of knowledge of contraceptive methods among women with SMI were also reported (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Chacko and Prathyusha2024a). In women with SMI who were aware of contraceptive methods, negative attitudes toward condoms were common, including beliefs that condoms were linked to promiscuity (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021). These attitudes were apparent in healthcare professionals too, with one stating that access to condoms for women with SMI in psychiatric facilities will encourage sexual activity. Even among women with SMI who were knowledgeable about STIs, they did not report practicing safer sex; mental healthcare professionals confirmed this, saying that despite the availability of condoms, they were not used by people with SMI (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007). Women in this study reported that Brazilian churches have claimed that condoms are not efficacious as an HIV transmission prevention method, rather encouraging worshippers to believe in religious protective mechanisms (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007).
Despite these numerous challenges, some women also expressed that they did not need sexual health education (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018).
Facilitators
Other women with SMI did report a need for sexual education concerning SMI and sexual relations to maintain normal relations with their partners (Rezaie and Phillips, Reference Rezaie and Phillips2020). Some women reported already having a baseline knowledge of HIV symptoms from governmental health campaigns (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007). There was also a call for inclusive learning environments for SRH education, especially ones that are gender-inclusive, culturally sensitive and foster community (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007).
Synthesized finding 2: Service availability shapes access to SRH care for women with SMI (Figure 3)
Barriers
Many mental healthcare providers expressed an inability to address SRH concerns due to a lack of time. Some admitted to not addressing SRH at all, unless the issue is raised specifically by the patient (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022). Others believed it was a better use of time to treat SMI symptoms than it was to address SRH, especially given short inpatient stays (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018). Another factor was insufficient training: some providers believed that they did not have adequate education or the appropriate medical specialization (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018). Women participants mirrored this sentiment, saying that they did not think their mental healthcare professionals were equipped to handle SRH concerns. Mental healthcare professionals also felt there were no policies and governance to address SRH needs and behaviors (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022). One mental healthcare professional expressed frustration with the lack of proper hospital protocol and training for addressing sexual interactions between patients in psychiatric facilities (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007). Women in the only community-based study reported a lack of family planning services (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021).
Facilitators
In some studies, women wanted increased access to SRH services (Rezaie and Phillips, Reference Rezaie and Phillips2020; Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021). Women with SMI highlighted a need for advice on pregnancy-related topics and some suggested that family planning services be integrated into mental healthcare (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021). Health professionals supported this need for family planning (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022). Many mental healthcare professionals perceived women with SMI to have similar SRH needs to people without SMI. They also believed that intimate relationship maintenance and security were big motivators for continuing with psychiatric treatment (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022).
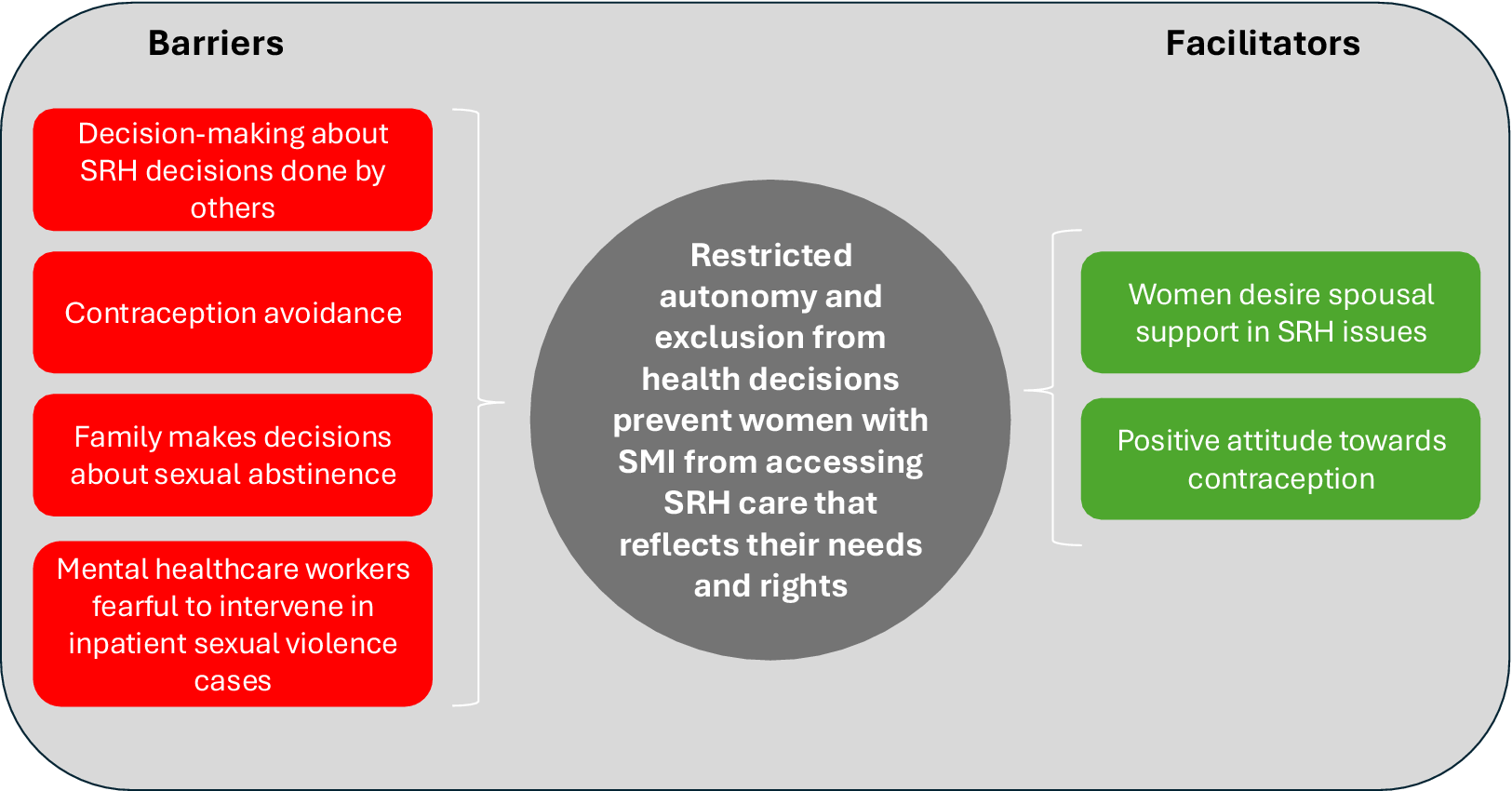
Synthesized finding 3: Restricted autonomy and exclusion from health decisions prevent women with SMI from accessing SRH care that reflects their needs and rights (Figure 4)
Barriers
Women with SMI across diverse contexts described decreased autonomy in making decisions about their SRH. Rather than exercising individual agency, many women relied on healthcare providers, partners or family members to guide or fully make decisions regarding pregnancy, contraception and sexual relationships (Lundberg et al., Reference Lundberg, Johansson, Okello, Allebeck and Thorson2012; Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020; Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022; Rani et al., Reference Rani, Raman, Antony, Thirumoorthy and Chethan2023; Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Chacko and Prathyusha2024a; Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b).
This pattern of decreased autonomy extended to experiences where decisions were made with no regard to women’s knowledge or consent. In fact, some healthcare professionals reported making family planning decisions on behalf of their patients (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022). In other cases, women reported that both healthcare professionals and family members pushed sterilization as the most appropriate form of contraception (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b).
Women with SMI expressed emotional distress when their partners made decisions about their sexual health without consulting them (Rani et al., Reference Rani, Raman, Antony, Thirumoorthy and Chethan2023). Economic dependence further exacerbated these power dynamics. When describing how her parents would not pay for her healthcare costs, a woman told researchers that she “paid” her clinician by non-consensually engaging in sexual activity with him (Lundberg et al., Reference Lundberg, Johansson, Okello, Allebeck and Thorson2012).
Women also reported limited choice in the use of contraception (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020; Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Chacko and Prathyusha2024a; Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b). Although some women reported a general refusal to use contraception, saying that they are not worried about repercussions (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020), others expressed that this decision is usually made by partners, detailing that their partner dislikes using any contraception (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b). One study found that family members sometimes stopped women from engaging in sexual intercourse entirely by limiting who they interacted with (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007).
Despite knowing about both the emotional and physical violence perpetrated against women, many mental healthcare providers did not intervene in cases of inpatient violence, due to fear of patient aggression (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022) or concern that action against the abuser may result in consequences for the victim, such as abandonment or retribution (Rani et al., Reference Rani, Raman, Antony, Thirumoorthy and Chethan2023).
Facilitators
A few studies found that women desire to share decision-making with their spouses. One participant in China expressed that she wished she could bear the risks of reproduction with the help of her husband (Yu et al., Reference Yu, Wang, Wang, Ma, Li and Zhou2022). Women in Ethiopia with SMI also expressed positive attitudes toward, and agency over, contraceptive use (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021).
Synthesized finding 4: Stigma and gendered expectations around mental illness and sexuality, reinforced by societal norms, discourage care-seeking for the SRH needs of women with SMI (Figure 5)
Barriers
Women with SMI often struggle to openly discuss their SRH needs due to cultural and familial expectations. Feelings of shame, discomfort and fear of disclosure emerged across studies as key deterrents to care-seeking (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018; Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021). One mental healthcare professional in Iran stated that patients only talk about SRH issues after a few sessions, and still caution, like a private setting, has to be used (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018). Many women in Iran also expressed not raising sexual inquiries due to cultural norms of abstinence before marriage, and Iranian mental healthcare professionals reiterated this social norm as a factor behind patients asking questions about SRH only after marriage (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018). Women also voiced fear about private SRH information being unduly disclosed to others by healthcare professionals (Raisi et al., Reference Raisi, Yahyavi, Mirsepassi, Firoozikhojastefar and Shahvari2018).Women also expressed concern that their baby will also have an SMI and therefore be labeled as “disabled” by society (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021).
These cultural constraints were compounded by internalized norms around gender and sexuality. Many women reported that prescribed gender roles were more important than sexual desire, with one declaring that her children’s education was more important than her SRH needs (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b). Studies also reported women with SMI overlooking STI symptoms due to family issues, which they perceived to be more pressing (Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Chacko and Prathyusha2024a; Vijayalakshmi et al., Reference Vijayalakshmi, Rajagopal, Govindan, Ganjekar, Prathyusha and Chacko2024b).
Mental healthcare professionals tended to make assumptions about the capability of women with SMI; these attitudes often limited the reproductive choices and medical options women were given. Healthcare professionals often believed that women with SMI have decreased caretaking abilities, and such beliefs enabled them to administer family planning services to women with SMI without consent (Tumwakire et al., Reference Tumwakire, Arnd and Gavamukulya2022). In one study, women with SMI reported disliking family planning, believing it was for preventing birth rather than planning it (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021). Mental healthcare professionals also believed that the sexual habits of women with SMI were attributable to their SMI (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007).
Lastly, the reproductive decision-making of women with SMI was heavily driven by expectations surrounding motherhood, often leading to delayed care or compromised autonomy. In one study, women with SMI reported letting familial opinions influence their decisions regarding SRH care, including contraception (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020). Women with SMI in Ethiopia also expressed their experience that other people did not think that women with SMI should have children due to a perceived caretaking inability and the possibility of children inheriting SMI (Zerihun et al., Reference Zerihun, Sorsdahl and Hanlon2021). Additionally, a familial expectation for male children in India was reported to lead to abortion of female fetuses and delayed sterilization of women (Bagadia et al., Reference Bagadia, Nanjundaswamy, Ganjekar, Thippeswamy, Desai and Chandra2020).
Facilitators
Motherhood was reported as a powerful motivator for recovery in China, as it helped women with SMI feel similar to people without SMI. Women with SMI also exhibited positive attitudes toward SRH care, especially pre- and antenatal care, which they believe is technologically advanced and therefore reliable (Yu et al., Reference Yu, Wang, Wang, Ma, Li and Zhou2022). Others reported feeling more comfortable pursuing sexual relationships within psychiatric treatment facilities (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007).
Additionally, a mental healthcare professional reported women’s sex-positive attitudes when given a proper outlet, and a woman with SMI expressed a desire to learn more about STI prevention in order to educate her community (Wainberg et al., Reference Wainberg, Alfredo González, Mckinnon, Elkington, Pinto, Gruber Mann and Mattos2007).
Confidence of findings
For dependability, all synthesized findings were informed by high-quality studies; however, because these studies contained limitations, dependability for all four synthesized findings was downgraded to “moderate.” For credibility, because most contributing findings were ranked as “unequivocal,” all synthesized findings were rated as “high.” As a result, all synthesized findings received a final “moderate” ConQual rating (see Supplementary File S5).
Discussion
This review found that limited knowledge and service availability, women’s restricted autonomy and stigma and societal norms were intersecting factors that shape access to SRH care among women with SMI in LMICs. Our findings provide varying degrees of insight across the five dimensions of access.
Approachability: When considering approachability of services, a general lack of knowledge and reduced risk perception of SRH needs sometimes led to decreased perception of need for care. Women with SMI were sometimes not aware of STI symptoms or, even if they were aware, did not prioritize treatment due to a lack of concern for potential negative impacts or familial issues.
Acceptability: In terms of acceptability, social norms were both a barrier and facilitator to access. Some barriers, such as shame and stigma around discussing SRH needs, may reflect patterns in the general population (Cook and Dickens, Reference Cook and Dickens2014) – particularly among unmarried women (Mohammadi et al., Reference Mohammadi, Kohan, Mostafavi and Gholami2016) or young people (Riabroi et al., Reference Riabroi, Gregory, Mackay and Germeni2025) – rather than phenomena unique to women with SMI. However, other barriers were more clearly tied to perceptions of SMI. For example, mental healthcare professionals and family members often perceived women with SMI to have reduced caretaking abilities. The lack of access to essential SRH care, particularly for women who are less educated, live in rural areas and are poorer, is a global phenomenon that reflects deep-rooted gender inequalities (Starrs et al., Reference Starrs, Ezeh, Barker, Basu, Bertrand, Blum, Coll-Seck, Grover, Laski, Roa, Sathar, Say, Serour, Singh, Stenberg, Temmerman, Biddlecom, Popinchalk, Summers and Ashford2018). These gaps seem to be intensified further for women with SMI, echoing the experiences of other marginalized populations of women. For example, a global systematic review found that the femininity of women with intellectual disabilities was considered “defective” and that their caretakers considered them to be undeserving of perceived “adult” needs like sexual desires, limiting access to SRH care (Pérez-Curiel et al., Reference Pérez-Curiel, Vicente, Morán and Gómez2023).
Interpersonal violence is mentioned in many of the papers in the form of gendered physical, sexual and emotional abuse that is perpetrated by partners, family or community members, healthcare workers and others in positions of power. However, despite the exacerbation of sexual violence among women with SMI (Lundberg et al., Reference Lundberg, Nakasujja, Musisi, Thorson, Cantor-Graae and Allebeck2015), the studies in this review did not mention the impact that it may have on access to care. Experience of sexual violence is a health concern itself, and may have mental health, SRH and other physical health sequelae (Hillcoat et al., Reference Hillcoat, Prakash, Martin, Zhang, Rosa, Tiemeier, Torres, Mustieles, Adams and Messerlian2023). Previous research in the general population indicates that sexual assault may lead to avoidance or disengagement with gynecological care (Razi et al., Reference Razi, Walfisch, Sheiner, Abd Elrahim, Zahalka, Abdallah and Wainstock2021) and more rapid discontinuation of contraception (Allsworth et al., Reference Allsworth, Secura, Zhao, Madden and Peipert2013). It is conceivable these experiences could have similar effects among women with SMI, but there was insufficient data in our review to form conclusions on this point. Although traditional and religious providers are commonly sought for mental health problems in LMIC (Asher et al., Reference Asher, Birhanu, Baheretibeb and Fekadu2021), the included studies did not explore preferences for alternative sources of care for SRH among women with SMI.
Availability: Availability of SRH care varied across studies. Though it was not always explicitly stated, it seemed that in some cases these services were available, but were harder to access for women with SMI. A perceived gap was that mental healthcare professionals did not proactively ask about SRH, nor signpost to available services, and this was traced back to mental healthcare workers not feeling equipped – both in terms of training and time – to address SRH needs. There was less information on how practical issues such as geographic location, transport or opening hours affected access, and little exploration of how services could be tailored to the specific needs of women with SMI.
Affordability: The lack of emphasis on affordability in our findings may be because this was simply not the focus of the included papers. Out-of-pocket expenditure is a major barrier to accessing SRH services in LMICs among the general population (Ravindran and Govender, Reference Ravindran and Govender2020); however, our study was not able to shed light on any differential impacts on women with SMI.
Appropriateness: There were several barriers relating to appropriateness of care. Mental healthcare providers attributed abnormal sexual behavior to SMI, not intervening in cases of sexual violence and in some cases seeming indifferent to the SRH needs of women. Additionally, women with SMI expressed fear that providers would disclose information to family members that would then change the way family members perceived them, making them more hesitant to access care. Engagement with care was highly shaped by lack of autonomy in decision-making. People with SMI in LMICs may be uninvolved in decision-making in general (Souraya et al., Reference Souraya, Hanlon and Asher2018), but also women in LMICs have low decision-making autonomy in relation to SRH, such as contraceptive use (Belachew et al., Reference Belachew, Negash, Bitew and Asmamaw2023). Women with SMI in LMICs, ergo, face intersectional layers of disempowerment – stemming from gendered discrimination, SMI stigma and lack of resources in health systems – that lead to decreased autonomy over SRH care decisions.
Recommendations
We propose the following policy and practice recommendations on the basis of our findings.
Synthesized finding 1: Variable knowledge of SRH and low risk perception hinder access to SRH care for women with SMI
The majority of evaluations aiming to improve SRH in women with SMI are health promotion interventions focused on changing women’s awareness, skills and behaviors in relation to SRH. To our knowledge, all evaluations have been conducted in the US or UK (Pandor et al., Reference Pandor, Kaltenthaler, Higgins, Lorimer, Smith, Wylie and Wong2015; Hughes et al., Reference Hughes, Mitchell, Gascoyne, Moe-Byrne, Edmondson, Coleman, Millett, Ali, Cournos, Hewitt, Johnson, Kaur, Mckinnon, Mercer, Nolan, Walker, Wainberg and Watson2020) and the overall quality of evidence is limited. Although similar interventions could be adapted or developed to suit LMIC settings, our findings suggest focusing on service user factors may be necessary but not sufficient to improve access to SRH care.
Synthesized finding 2: Service availability shapes access to SRH care for women with SMI
The inclusion of essential SRH services in universal health coverage is a crucial step to increasing access for all women (Starrs et al., Reference Starrs, Ezeh, Barker, Basu, Bertrand, Blum, Coll-Seck, Grover, Laski, Roa, Sathar, Say, Serour, Singh, Stenberg, Temmerman, Biddlecom, Popinchalk, Summers and Ashford2018). Further, addressing the specific provider-side factors affecting access for women with SMI may involve training mental healthcare professionals, and other health workers involved in delivering mental healthcare (for example, community health workers) in the SRH needs of women with SMI. Training could be modeled on that developed for healthcare professionals working with similarly vulnerable populations, like refugee women (Mengesha et al., Reference Mengesha, Perz, Dune and Ussher2018). Local guidelines to ensure routine assessment and referral for SRH needs are also indicated. Using mHealth innovations to deliver SRH care could conceivably address limitations of healthcare worker’s workload by spreading care demand, and increased anonymity could combat the shame both patients and mental healthcare professionals reported by allowing non-face-to-face treatment (Laar et al., Reference Laar, Harris, Shifti and Loxton2022). However, this may not serve the entire population due to gaps in literacy or digital access (Alkureishi et al., Reference Alkureishi, Choo, Rahman, Ho, Benning-Shorb, Lenti, Velázquez Sánchez, Zhu, Shah and Lee2021), and our data did not speak to the acceptability or feasibility of an mHealth approach.
Global guidance may also be important: while the WHO Guidance on Community Mental Health Services (WHO, 2021) and WHO QualityRights Initiative (WHO, 2019b) seek to support mental health services to align with the CRPD, there is limited guidance on how SRH needs can be addressed among people with SMI. The WHO’s Mental Health Gap Intervention Guide also does not signpost clinicians to routinely consider SRH concerns, other than sexual abuse, dysfunction and infection, in women with SMI (WHO, 2019a).
Synthesized finding 3: Restricted autonomy and exclusion from health decisions prevent women with SMI from accessing SRH care that reflects their needs and rights
Studies in some contexts have shown that autonomy is positively associated with healthcare decision-making and better health outcomes, especially in SRH (Osamor and Grady, Reference Osamor and Grady2016). However, in other contexts, family decision-making is expected and disregarding these norms could result in worse outcomes. For example, unilateral decision-making on contraception could conceivably rupture intimate relationships or even lead to harm or abuse. Care models that actively support and foster women’s agency should therefore be developed while paying attention to cultural and social norms. One approach is to employ recovery-oriented models of care that center on personal goals and restoration of autonomy, while being grounded in positive family relationships (Asher et al., Reference Asher, Birhane, Weiss, Medhin, Selamu, Patel, De Silva, Hanlon and Fekadu2022; Asher et al., Reference Asher, Rapiya, Repper, Reddy, Myers, Faris, Petersen, Hanlon and Brooke-Sumner2024; Brooke-Sumner et al., Reference Brooke-Sumner, Repper, Petersen, Hanlon, Myers, Faris, Rapiya and Asher2024). Because autonomy in LMICs is often dictated by communality rather than individuality (Mumtaz and Salway, Reference Mumtaz and Salway2009), community health workers who have intimate knowledge about social spheres and the marginalized populations within them (Ahmed et al., Reference Ahmed, Chase, Wagnild, Akhter, Sturridge, Clarke, Chowdhary, Mukami, Kasim and Hampshire2022) can act as key facilitators in supporting contextually appropriate expressions of autonomy. However, confidentiality concerns arising from the close social and geographical proximity of local community health workers providing SRH services (Sidamo et al., Reference Sidamo, Kerbo, Gidebo and Wado2024) might be amplified in settings where the prevailing belief is that women with SMI should not want or need access to SRH care. Such contextual sensitivities should be actively identified and addressed when developing interventions.
Synthesized finding 4: Stigma and gendered expectations around mental illness and sexuality, reinforced by societal norms, discourage care-seeking for the SRH needs of women with SMI
The normalization of both SMI and SRH care is essential in combating societal stigma. Social contact interventions have been shown to decrease mental health stigma in LMICs (Makhmud et al., Reference Makhmud, Thornicroft and Gronholm2022). Healthcare workers hearing directly from women with SMI about their experience of SRH may have an important contribution to changing attitudes and willingness to address SRH concerns. Family members had a critical role in shaping the sexual relationships and access to SRH care of women SMI. Work with families may therefore be important in changing expectations and attitudes in relation to SRH, while carefully navigating contextual gender norms. This might include partners, parents or other family members, who are typically heavily involved in care of people with SMI in many LMIC (Dijkstra et al., Reference Dijkstra, Weiss, Birhane, Medhin, De Silva, Hanlon, Fekadu and Asher2025; Rapiya et al., Reference Rapiya, Khuzwayo, Asher and Brooke-Sumner2025). Broader policy and legislative changes that promote gender equality and give women more control over their lives are also needed to shift social norms that impede women’s access to SRH care (Starrs et al., Reference Starrs, Ezeh, Barker, Basu, Bertrand, Blum, Coll-Seck, Grover, Laski, Roa, Sathar, Say, Serour, Singh, Stenberg, Temmerman, Biddlecom, Popinchalk, Summers and Ashford2018). These reforms are likely to sit outside the health sector and include education, economic policy, community and civil society, and the criminal justice system (Sarri et al., Reference Sisodia, Hammond, Leonardi-Bee, Hanlon and Asher2025).
Research recommendations
More research is needed to understand the interactions between enduring emotional, physical and sexual abuse and its impact on accessing SRH care. Research must also be done on the affordability and feasibility of accessing SRH care, including transport and location of care among women with SMI. Interrogation of the extent to which problems with access to SRH among women with SMI reflect access gaps in the general population could also be a focus. Lastly, development and evaluation of interventions to address SRH – focusing on women, families, health systems and broader social, cultural and economic structures – is needed.
Strengths and limitations
Rigorously applying the JBI meta-aggregation approach facilitates the formation of recommendations that can be readily translated into public health interventions. Further, using ConQual increases confidence in the validity of our synthesized findings. However, pooling findings by meta-aggregation may overlook important contextual differences between countries, including cultural and social norms and health service availability. Furthermore, as only six countries were represented, we should be wary of generalizing our findings to diverse LMIC contexts. Additionally, as most studies were set in specialized psychiatric settings, our findings may not be generalizable to community or primary care settings. The majority of screening was carried out by a single reviewer, which may increase the possibility of incorrect assessment and missing data.
Conclusion
This review synthesized the barriers and facilitators to SRH with women with SMI in LMICs, identifying four main addressable findings that serve as influencers to access. These findings can help policymakers in making targeted interventions to improve access to SRH in these settings. Differences in cultural and social context and healthcare systems must be considered before adopting interventions.
Open peer review
To view the open peer review materials for this article, please visit http://doi.org/10.1017/gmh.2026.10222.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/gmh.2026.10222.
Data availability statement
Data sharing is not applicable – no new data is generated.
Author contribution
A.C.: data curation, investigation, formal analysis, writing – original draft, writing – reviewing & editing, B.P.: conceptualization, data curation, investigation, formal analysis, writing – original draft, writing – reviewing & editing, S.S.: data curation, investigation, C.B.S.: writing – reviewing & editing, R.B.: writing – reviewing & editing, C.H.: writing – reviewing & editing, L.A.: conceptualization, supervision, writing – reviewing & editing. A.C. and B.P. are contributed equally.
Financial support
This project did not receive external funding. A.C. received a stipend as part of her internship work while conducting this study.
Competing interests
The authors declare none.
Inclusivity statement
In this article, the term “women” is used to refer to study participants who were individuals who self-identified as women within the socially defined gender norms of their country.



 Open access
Open access