

Context
Gender in Society
The Islamic Republic of Pakistan, located in South Asia, has a population of over 241 million, making it the world’s fifth-most populous country. (1) Pakistan has a young population, with approximately two-thirds below the age of twenty-nine. (1) About half of the population of the country are women. The 2023 population and housing survey revealed that only 48% of females are literate compared to 70% of men, with only 8.3% of women have access to tertiary education. (1) The female contribution in the paid workforce is only 20%. (2)
Pakistan has gender inequalities within its patriarchal society, where men are traditionally considered the primary breadwinners and decision-makers, while women are expected to fulfil domestic roles. The Global Gender Gap Report, 2022, published by the World Economic Forum, ranked Pakistan 145 out of 146 countries, (Reference Schwab, Samans, Zahidi, Leopold, Ratcheva and Hausmann3) higher than only Afghanistan. Women lag in every sphere of life, such as education, economic opportunities, access to health care, and political representation.
Gender inequality in health is evident from a high maternal mortality ratio of 186 deaths per 100,000 live births in 2019. (4) Women’s lack of autonomy in reproductive health decisions contributes to high fertility, poor health outcomes, and higher infant and maternal morbidity and mortality. (Reference Ali, Ali, Nadeem, Memon, Soofi and Madhani5) In many regions of the country, early marriages are common, which further exacerbates women’s health challenges. (Reference Ali, Ali, Nadeem, Memon, Soofi and Madhani5)
Pakistan, as the first Muslim country with a female prime minister (Benazir Bhutto in 1988), inspired greater female involvement in public life. During her tenure, a substantial female workforce, exceeding 100,000 female health workers, was established to deliver essential health care services in semi-urban and rural areas. These women played a pivotal role in altering societal perceptions of working women, contributing to the empowerment of women in rural Pakistan. (Reference Ahmed6)
Recent years have seen progress in gender equality, especially in urban areas. There has been a gradual increase in female education access, coupled with a decline in child and early marriages. Urban regions, marked by improved literacy rates and increased workforce participation, exhibit more diverse and progressive attitudes towards gender roles. Challenges persist in rural areas and lower economic strata, where conservative values and limited educational access contribute to traditional gender norms. (Reference Lohana, Alizai and Ahmed7)
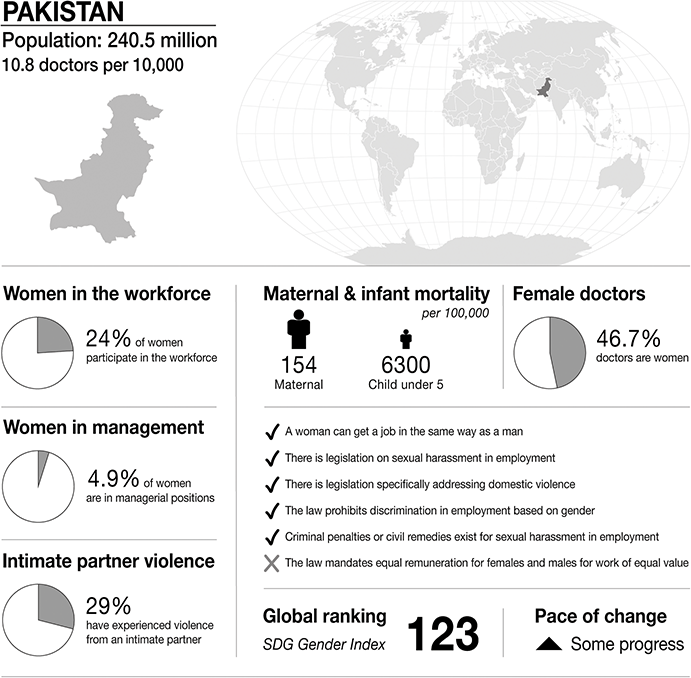
Infographic Pakistan. Infographics were provided by CartoGIS Services, The Australian National University. Population: from World Bank https://databank.worldbank.org/source/population-estimates-and-projections. Sustainable Development Progress, global ranking and statistics on women in the workplace, women in management and intimate partner violence: from United Nations SDGs Data Portal https://unstats.un.org/sdgs/dataportal. Female doctor percentage: from Global health workforce statistics www.who.int/data/gho/data/themes/topics/health-workforce. Legislation and law statements: from the World Bank gender data portal 2023 https://genderdata.worldbank.org/en/indicators. Maternal mortality statistics: from the Global Health Observatory 2020 https://mmr2020.srhr.org. Infant mortality statistics: from United Nations International Children’s Fund (UNICEF) https://data.unicef.org/topic/child-survival/under-five-mortality.

Figure 27.1 Long description
The infographic provides information about Pakistan, with a population of 240.5 million and 10.8 doctors per 10,000 people. It highlights several gender-related statistics. 24 per cent of women participate in the workforce. 4.9 per cent of women are in managerial positions. 29 per cent of women have experienced intimate partner violence. Maternal mortality is 154 per 100,000. Infant mortality under 5 is 6300 per 100,000. 46.7 per cent of doctors are women.
The infographic lists the presence or absence of law and policy on gender equality. In Pakistan:
– a woman can get a job in the same way as a man.
– there is legislation on sexual harassment in employment.
– there is legislation specifically addressing domestic violence.
– the law prohibits discrimination in employment based on gender.
– criminal penalties or civil remedies exist for sexual harassment in employment.
– there is no law that mandates equal remuneration for females and males for work of equal value.
The S D G Gender Index global ranking is 123, and there has been some progress.
Gender in Medicine
As per a study published in 2023 on barriers faced by women doctors in Pakistan, out of a total 271,560 registered doctors, 127,468 (46.9%) are female. Despite the fact that around 80% students enrolled in medical colleges are female, the number of post-graduates registered with a medical licensing and regulatory body is below 50%. A number of reasons, such as family, employment, health care system or workplace related or social/cultural factors have been linked with this shortage. (Reference Raza, Jauhar, Rahim, Memon and Matloob8) Although no published studies were identified reporting sexual harassment of doctors by doctors in Pakistan, a number of studies highlighted harassment of female health care professionals. A descriptive cross-sectional study from the metropolitan city of Karachi on 350 married female nurses and doctors revealed 59.6% (n=204) prevalence of sexual abuse in the study participants, mainly by family members. (Reference Khan, Ali, Karmaliani and Asad9) In terms of experiencing sexual harassment at a workplace, a questionnaire-based survey conducted in a general hospital in Islamabad showed 16.9% of female nurses had experienced sexual harassment (physical), while 21.2% reported verbal sexual harassment by male physicians. (Reference Shaikh10) There are, however, reports of incidents of sexual harassment from newspapers; one such incident involved a hospital in Mirpur Khas (Sindh) where a doctor (anaesthetist) was beaten up by paramedics for alleged sexual harassment of a female co-worker. (Reference Shaikh11) In a similar incident a cardiac surgeon at the Pakistan Institute of Medical Sciences (PIMS) was found guilty of sexually harassing a junior doctor by an anti-sexual harassment committee and suspended from his job. (Reference Ghani12) In terms of women in leadership positions in the health care system, data from private medical institutions show only 10% of women were found to be in leadership positions such as chairperson, pro-vice chancellor, associate dean, head of department, or principal, etc., in medical institutions. (Reference Iftikhar, Yasmeen, Khan and Arooj13)
Medical Education
The evolution of medical education cannot be seen in isolation from prevailing conditions of culture, society and state. (14) In precolonial times, the region now considered Pakistan had traditional healers providing health services. Later, the British transformed health care by laying the foundations of modern medicine. After independence in 1947, Pakistan was left to rebuild the system from scratch. A pivotal development was the establishment of the Pakistan Medical and Dental Council (PMDC) to regulate medical profession education and practice. (15) In line with this, The College of Physicians and Surgeons was established in 1962 (CPSP). The College works to maintain specialist medical practice through the organization of postgraduate medical education, training and research. (16) According to the 2021 census, 173 medical colleges are now recognized by the PMDC. Out of these, Fatimah Jinnah Medical University is the only registered university that caters to women. Young female doctors study and work alongside their male colleagues and teachers at both an undergraduate and postgraduate level.
Workplace challenges reported by a nationwide study showed that bullying, harassment and absence of support has left a marked impact on female doctors, especially trainees. (Reference Malik, Inam, Martins, Janjua, Zahid and Khan17)
An interesting article published by the BBC showcased ‘The doctor brides revolutionizing Pakistan’s health care system’. (Reference Iqbal18) The article talks about how thousands of women qualify as doctors but half of them quit after graduation.
‘Everyone wants to show doctor brides as a trophy, but then they also want them to stay at home’, says Dr Sara Saeed Khurram when asked about the ‘doctor bride’ phenomenon. Khurram stopped medical practice as well after getting married and became part of the doctor bride phenomenon herself. Her personal struggles – moving to a new city after having her first daughter and postpartum depression – encouraged her to figure out how female doctors could get back into the medical workforce.
Khurram has now launched a telemedicine social enterprise with a majority female medical staff that provides quality health care to those in need.
A way out for these female doctors was online practice, according to an article published in the British Medical Journal: ‘Pakistan attracts 700 female doctors back into practice through online service’. (Reference Yusufzai19) Furthermore, sexual harassment among surgeons remains heinously underreported according to an article posted in the British Journal of Surgery, with 91.5% cases being unnoticed and 57.5% reporting suffering from severe burnout. (Reference Malik, Inam, Martins, Janjua, Zahid and Khan17)
Law
Legislation
In recent years much legislation has been approved to support women in cases of sexual harassment and assault. There is national legislation as well as some specific to provinces. Some of them include:
1. Prevention of Anti-Women Practices (Criminal Law Amendment) Act 2011 (pertaining to forced marriages and inheritance deprivation in the name of custom)
2. The Women in Distress and Detention Fund (Amendment) Act 2011
3. Right to Ownership (Women) Act 2011
4. The Acid Control and Acid Crime Prevention Act 2011
5. The Protection Against Harassment of Women at the Workplace Act 2010
6. Domestic Violence Prevention and Protection Act Sindh (2013) and Balochistan (2014)
7. Child Marriage Restraint Act (Punjab Marriage Restraint Amendment Act 2015, Sindh 2014)
8. Criminal Law (Amendment) (Offences relating to Rape) Act 2016
9. Criminal Law (Amendment) (Offences in the name or on pretext of Honor) Act 2016
10. Punjab Protection of Women against Violence Act 2016
11. Prevention of Electronic Crimes Act (PECA) 2016
12. Khyber Pakhtunkhwa Domestic Violence Against Women Act 2021
13. Anti-Rape (Investigation & Trial) Act 2021
Despite this legislation, the implementation of these laws is an issue due to reluctance of victims to lodge a complaint, poor police practices to collect evidence and support the victim, and a slow and inefficient legal system.
Role of the Legal System in Sexual Harassment Cases
Proving sexual harassment in court is difficult. Even if witnesses are available for sexual harassment, the court cases drag on for years. If the perpetrator is a person of influence or has connection with some person of influence, they may use their influence to malign and harass the victim and their families to drop the charges. In a patriarchal society such as Pakistan, women are often blamed as the ones who led the perpetrator to commit the crime, perhaps by wearing revealing clothes, inviting behaviours, or even being at the wrong place at the wrong time. There are some organizations who provide legal support to victims of sexual harassment, for example Asma Jehangir foundation and Hina Jilani law firm.
Courts may suggest psychological support for the victim; however, in most cases victims have to pay for those services.
Role of Police and Other Law Enforcing Organizations in Sexual Harassment Cases
People do not have faith in the police. The Pakistani police, with some exceptions, have deep rooted problems of corruption. Although there are now women police officers, generally women do not feel safe and would refrain from involving the police. In most cases, evidence is not collected properly or may even be tampered with to benefit the perpetrator. Women are also scared of negative publicity by involving the police. Involving the police means that the police can visit the house of the victim or call them to a police station at any hour. If the perpetrator is powerful, there are chances that the police will side with them due to being bribed or under the orders of some influential person. In many cases, the police tell the victim to patch things up with the perpetrator as such matters bring media coverage and shame to the family.
Role of Medical Organizations in Providing Legal Representation to Doctors in Civil or Criminal Cases
There are no formal medical organizations which represent doctors legally in cases of sexual harassment or other similar cases. The Pakistan Medical and Dental Council (20) is the only statutory publicly led organization that may address such grievances and may cancel licensure of doctors involved in sexual harassment. Doctors do not have insurance to cover their expenses in case they are involved in civil or criminal cases. The government may provide a defence attorney if they are unable to afford one. However, in most cases they organize these services themselves.
Medical Regulation
Every medical and dental practitioner is registered with the Pakistan Medical and Dental Council (PM&DC). Doctors are required to renew their license every five years. Any complaints of doctors are submitted to a disciplinary committee, which then oversees the entire process. Instructions on how to fill online complaint forms are available on the PM&DC website. (20) A leading newspaper reported in 2019 that approximately 75,000 doctors in the country were working with expired licenses. (20) All such doctors were informed through newspaper adverts to renew their licenses within a period of two weeks. Furthermore, the chief secretaries (civil servants) of each province were informed to communicate with doctors regarding updating their registration.
The PM&DC is responsible for maintaining the code of conduct and professional ethics and has the authority to cancel a doctor’s license.
Besides the above provisions,
1. patients can also file a complaint to provincial health care commissions for doctors’ negligence,
2. medical services in all four provinces and federal territory are also included in the Consumers Protection Act and
3. the Law of Torts, a pre-partition law, is still valid for medical malpractices in Pakistan. (Reference Waraich21)
A victim of medical negligence or sexual harassment has a right to lodge a First Information Report, or FIR (a written document by the police), against a doctor. A newspaper report from 2021 highlights a complaint by one of the female doctors and a polio worker accusing a senior health official of sexual harassment. They reported the case to Sindh province’s health minister. (Reference Ali22)
Professionalism can be taught in both undergraduate and postgraduate levels through classroom-based lectures, PowerPoint presentations, clinical demonstrations or scenario-based workshops. An editorial published in 2022 stated that such teaching is not formally taking place in many medical schools at present. (Reference Badshah, Mahboob and Yousaf23) A qualitative study of sixty young doctors who graduated from Pakistani medical universities revealed poor management skills, knowledge and practical application of medical professionalism. (Reference Jalil, Mahmood and Fischer24) Faculty and supervisors can also undergo regular updates and be role models for junior doctors.
Case Study
Navigating Justice: A Case Study on Workplace Sexual Harassment from Pakistan
Prelude
The cardiology specialty in Pakistan is predominantly male dominated, with very few female doctors choosing this field. In 2017, a female postgraduate trainee doctor in the Cardiology Unit of Pakistan’s federal hospital filed a written complaint with the anti-harassment committee of the hospital. In the complaint she accused a senior cardiac surgeon of sexual harassment. The surgeon had recently arrived from the United Kingdom.
She reported that due to the scarcity of females in this specialty, male doctors created a challenging environment through their ‘unethical and unprofessional behaviour’. The objective appears to be discouraging female doctors from pursuing cardiology.
She expressed her frustration, stating, ‘Hardly any women opt for cardiac surgery. I’m one of the few in Pakistan to do so, and work environments like this are disheartening.’
Assault
The female postgraduate trainee recounted instances where, during her duty at the cardiac centre, the surgeon called her to his office and allegedly touched her inappropriately while demonstrating an X-ray. Subsequently, when the surgeon summoned her again, she brought an intern with her. The intern also told her that she had experienced lewd comments from him.
The surgeon expressed displeasure at the presence of the intern. The trainee, feeling uncomfortable, began avoiding the professor, especially when called to his office alone. The surgeon started making derogatory remarks about her to colleagues, stating that it was unfortunate she chose cardiology as a female and that there was a ‘price’ to pay, suggesting she should leave cardiac surgery if unwilling.
The trainee claimed the surgeon threatened her with defamation if she reported the matter, leading to mental and psychological stress, ultimately resulting in a decline in her performance.
Limbo
Against the advice of her colleagues, the trainee filed a written complaint with the hospital’s anti-harassment committee. Despite this, the surgeon continued working in the cardiac unit, causing her extreme discomfort and fear. The surgeon, denying the charges, claimed the complaint was a conspiracy by a group opposing foreign qualified doctors in Pakistan.
Colleagues and friends suggested compromising with the surgeon to protect her reputation. The hospital involved the police in the inquiry, and during questioning, the trainee was pressured to reach a settlement due to the surgeon’s alleged strong political connections within the ruling party. These circumstances escalated her mental anguish, leading to sleep and appetite disturbances.
Exposure
The media covered the case, reporting it on the local news without mentioning her name. However, this drew attention from other doctors who inquired about her identity. Despite her awareness of the risks, she was worried about the potential outcome of the inquiry if it went against her.
While some colleagues were sympathetic, a few avoided her due to fear of the surgeon’s reaction. Even though other female staff also had a negative experience with the surgeon, they chose not to be involved in the case. The surgeon asserted to everyone that a false case had been registered against him under external pressure.
Aftermath
A four-member anti-harassment committee, after thorough deliberations, ruled in favour of the trainee, leading to the termination of the surgeon. The committee’s decision was promptly implemented, resulting in the suspension of the accused surgeon’s services.
Furthermore, the anti-harassment committee uncovered that the surgeon had been dismissed from a hospital in the United Kingdom due to sexual molestation complaints by two junior female colleagues. This incident occurred five years earlier, and the regulatory body in the UK deemed him unfit to practise. According to the Pakistan Medical and Dental Council, a doctor whose registration has been revoked by a foreign regulatory body is ineligible to practise in Pakistan. Despite this, the surgeon secured a position in a federal hospital through political connections.
The female trainee expressed gratitude for the justice served, emphasizing its importance not only for her security but for the wellbeing of other female employees as well.
Discussion
Numerous issues have been highlighted in this chapter; among them are gender inequalities, fewer females in leadership posts, not many female physicians in employment after graduating, no formal sexual harassment reporting procedures and policies in a number of medical institutions and facilities in both the public and private sectors. Gender equity in urban areas of the country is improving though. Although studies including systematic reviews have been published on various forms of workplace violence in hospitals, (Reference Rehan, Shan, Shuja, Khan, Hussain and Ochani25) there is a paucity of evidence in the published literature on sexual harassment. A number of reports, studies and newspaper columns have recommended having policies to address harassment at the workplace; however, little action has taken place over the years. Likewise, helplines for women facing challenges at home or work lack a robust mechanism for successful action plans. In the backdrop of no well-organized primary care health system, patient signposting, education or a referral pathway, reporting of such incidents is discouraged or masked. The lack of a facilitating environment at work and poor support from family members, particularly in-laws, adds more to the suffering of female physicians experiencing harassment. It leads to mental health issues, poor performance at work and relationship issues with partners. A deficiency of counselling or psychological support at work or its availability within the public sector badly affects those who are unable to afford private care. As for those female doctors who are not allowed by their spouse or in-laws to work after marriage, we shared success stories of individuals who have undergone hardships and utilized their experience to help others. (Reference Yusufzai19)
With regards to legislative reforms, we listed and mentioned a number of acts and laws relating to the protection of women; however, awareness and information dissemination to health care professionals and the ordinary person are missing links. Regarding a country which is predominantly rural with an adult literacy rate of 58% (2019) (26) and a significant proportion of youth population, its vulnerable population must have access to safe working environments and training or guidance in dealing with threatening situations. Acknowledging and encouraging speaking up and reporting such incidents at home and in the workplace must be ensured. Medical regulatory bodies should offer advice in such cases and bring about reforms in both undergraduate and postgraduate curricula/continuing medical education, focusing on professionalism training and the development of competencies. Incidents reported in newspapers showed sexual harassment complaints were escalated by victims to the higher ministerial level.
In the case study, we discussed a case of suffering in silence initially due to a number of societal pressures and also because the perpetrator had an influential background and network. The female doctor then took matters to an anti-harassment committee and eventually won the case, exposing a series of unpleasant actions by the male surgeon. Her act saved a lot of future trainees from getting manipulated and harassed by that doctor. She also set an example for other females to follow.
Pakistan is a committed and resilient nation, and it has the potential to overcome hardships and succeed. We do need to focus on being more organised and take measures to deal with harassment issues more seriously. We need to identify ways to talk to and train our future generations on what constitutes good touch and bad touch. Such training can take place at home or in schools; this will encourage those at risk to raise their voice. Moreover, a well-functioning primary care system with support networks in place will help in dealing with the abovementioned issues more effectively.

 Open access
Open access