


Main points
-
• Percutaneous treatments are radiological interventions gaining momentum in the treatment of hepatic cystic echinococcosis.
-
• Puncture Aspiration Injection Re-aspiration (PAIR) and Puncture Aspiration Injection Drainage (PAID) are the techniques classically used.
-
• Variants of both these methods were established in order to provide a tailored treatment for each cyst type.
-
• We used a new modified technique which allowed us, besides treating simple and multivesicular cysts, the successful percutaneous management of an infected cyst with gastric fistula in one patient
Introduction
According to the latest recommendations from the World Health Organization - Informal Working Groups on Echinococcosis (WHO-IWGE) published in 2010, hepatic cystic echinococcosis (HCE) can be managed in different ways using the watch and wait strategy, drug therapy (Albendazole/Mebendazole), surgery, or percutaneous treatments (PTs) (Brunetti et al. Reference Brunetti, Kern and Vuitton2010). PTs can be separated into two categories: the first, called the puncture aspiration injection re-aspiration (PAIR) technique, was described by Ben-Amour et al. in 1986 (Ben Amor et al. Reference Ben Amor, Kchouk, Ayachi, Ben Chehida, Golvan, Gargouri, Ben Cheikh and Gharbi1987), and consists of using scolicidal agents such as hypertonic saline to destroy the germinal layer of the cyst; the second technique aims to remove all the cyst content (entire endocyst and daughter vesicules) using large-bore catheters and cutting devices, with aspiration apparatus. It includes the catheterization technique also known as the puncture aspiration injection drainage (PAID) technique, and other modified techniques such as the modified catheterization technique (MoCaT) (Bakdik et al. Reference Bakdik, Arslan, Oncu, Tolu and Eryilmaz2018) and percutaneous evacuation (PEVAC) (Schipper et al. Reference Schipper, Laméris, Delden, Rauws and Kager2002).
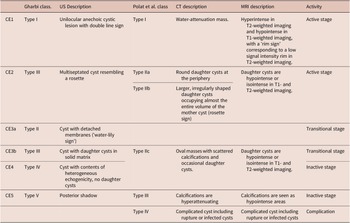
There are two cyst classifications based on ultrasound, the WHO 2003 classification of hepatic hydatid cysts (CE1 to CE5) (WHO Informal Working Group 2003) and the Gharbi classification (Type I to Type V) (Gharbi et al. Reference Gharbi, Hassine, Brauner and Dupuch1981): CE1/Gharbi Type I (unilocular anechoic cystic lesion with double line sign), CE2/Type III (multiseptated cyst resembling a rosette), CE3a /Type II (cyst with detached membranes ‘water-lily sign’), CE3b/Type III (cyst with daughter cysts in solid matrix), CE4/Type IV (cyst with contents of heterogeneous echogenicity, no daughter cysts), and CE5/Type V (posterior shadow). Another classification worth mentioning, based on CT, is the Polat classification (Type I to Type IV) (Polat et al. Reference Polat, Kantarci, Alper, Suma, Koruyucu and Okur2003). More details and correlations between these three classifications are suggested in Table 2.
In this article, we report our successful experience in HCE treatment using a new modified PAIR technique for 8 patients with 19 HCE between June 2011 and July 2021. We compared our modified PAIR technique in a table to all previously described percutaneous HCE treatment series in the literature.
HCE terminology is in accordance with that provided by the 2020 international consensus in the field of echinococcosis (Vuitton et al. Reference Vuitton, McManus, Rogan, Romig, Gottstein, Naidich, Tuxun, Wen and Menezes da Silva2020).
Materials and methods
Patients selection
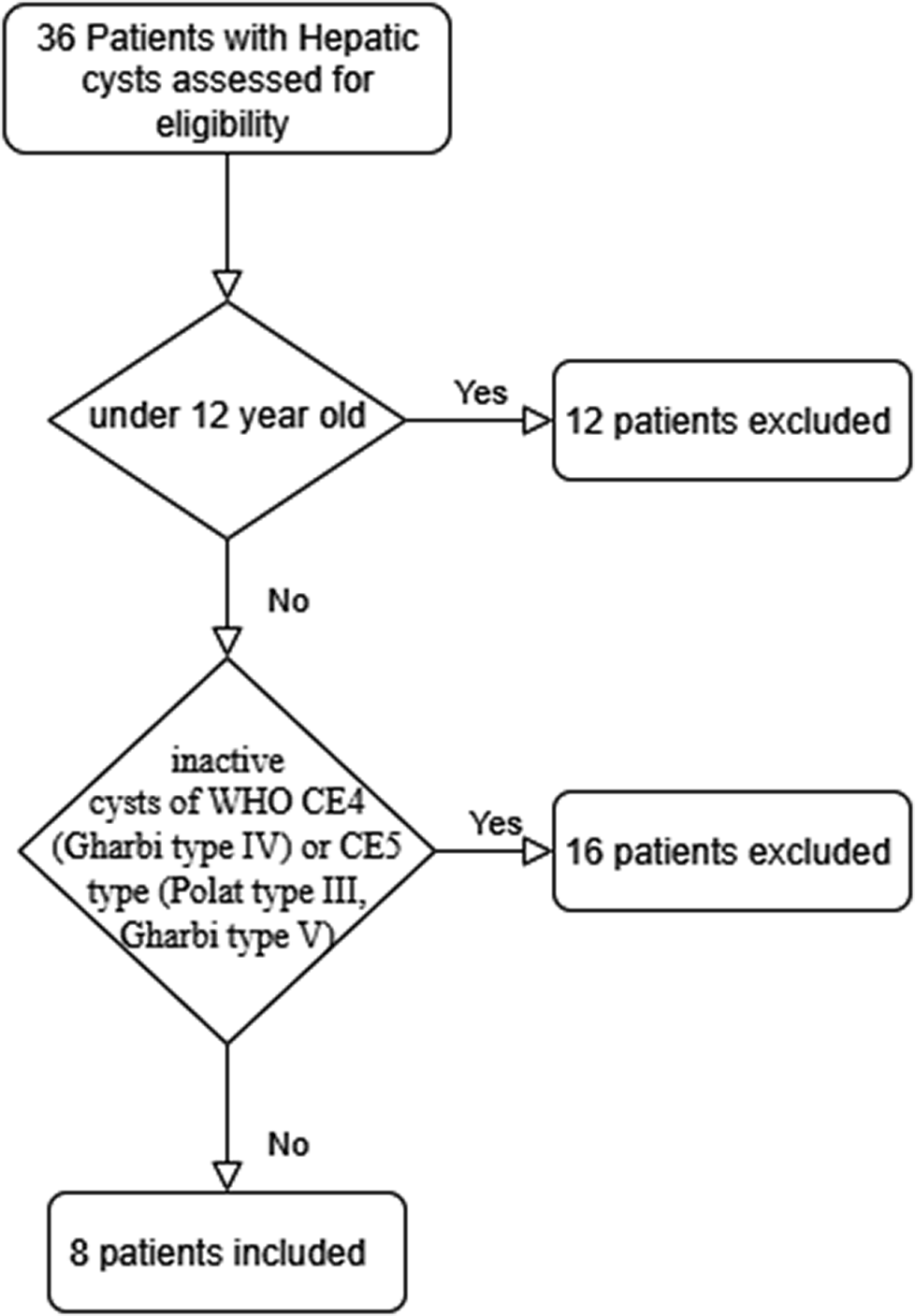
In this descriptive and retrospective study, we included a total of 8 patients (Figure 1 and Table 1) with 19 HCE who underwent a modified PAIR technique between June 2011 and July 2021. The inclusion criteria were a positive HCE diagnosis, simple cyst classified as WHO CE1 type (Polat I, Gharbi I), cysts with daughter cysts classified as WHO CE3b type (Polat IIc, Gharbi II), complicated cysts (infected cyst, fistulated cyst), multiple cysts if accessible to puncture, failure of drug therapy alone, patients who refuse surgery, relapses after surgery and surgery contraindications. The exclusion criteria were patients under 12 years of age and inactive cysts of WHO CE4 (Gharbi type IV) and CE5 type (Polat Type III, Gharbi Type V). We report neoadjuvant and adjuvant drug therapies, type and location of cysts, post-procedural complications, size of cyst, and changes in cyst morphology after treatment for each patient.
Flowchart of the study representing the criteria and number of patients.

Demographic information, biological analysis, and cyst characteristics in all patients

NA = not available. Classification standardized according to WHO-IWGE, Polat, and Gharbi systems.
Correlation between WHO, Gharbi, and Polat classifications

This table represents a descriptive correlation based on literature and was not derived from a formal validation study.
Ethical standards
This retrospective case series was approved by the Ethics Committee of Hôpital Psychiatrique de la Croix-Hôpital Universitaire Saint Joseph of Beirut, Lebanon (approval reference number: HPC 001-11-25). All patients provided written informed consent for the percutaneous procedure after being informed of its nature, potential risks, and expected benefits. Data used for this analysis were anonymized prior to evaluation.
Classification and diagnosis of hepatic cystic echinococcosis
HCE diagnosis was based on clinical findings associated with imaging (computed tomography (CT), ultrasonography (US), or magnetic resonance imaging (MRI)), and a positive indirect hemagglutination (IHA) test for Echinococcus granulosus or the detection of protoscoleces via a parasitology analysis of cyst content. The Polat classification with ‘MRI correlation’ was also used in this study (Table 2). In our series, the CE3b cyst, which presented daughter cysts in a predominantly solid matrix with partial septal calcifications, was categorized as Polat Type IIc in accordance with these imaging criteria.
Technique and follow-up
Local anaesthesia was administered during the procedure, and patients were monitored for possible anaphylaxis. The cysts are localized via CT guidance and a transhepatic puncture was performed using an 18-gauge needle (G). A third of the content is aspirated and an equal amount of 20% hypertonic saline solution (HSS) is injected. After a 5-minute interval a cystogram is obtained to show any possible communication between the cyst cavity and the biliary tract. An 8.5 French (F) drainage catheter is then placed into the cyst and half the content is aspirated. The cyst is filled again with HSS equal to the amount aspirated and left for 10 minutes. Further irrigations (3–4 times) are made in the same way. The procedure is complete after re-aspiration of all cyst content and removal of the drainage catheter. If the cyst measures more than 10 cm, 95% ethanol is injected and left for 10 minutes at the end of the procedure, then completely aspirated. After cyst puncture, aspirated fluid is evaluated for the presence of protoscoleces, and albendazole is given 4 days before PTs and at least one month after the procedure.
The criteria for effective therapy were: reduction of the cyst dimensions, complete disappearance or irregularities in the cyst wall based on US, CT, or MRI results obtained at least three months after the procedure.
Statistical analysis
Given the small number of cysts with complete imaging follow-up, statistical analyses were considered exploratory. A comparison of hepatic cyst size before and after treatment was performed using Student’s paired t-test to summarize changes, but the resulting p-value is interpreted descriptively rather than as confirmatory evidence of efficacy. We also report absolute and relative size changes, along with ranges.
Literature contextualization
To contextualize our findings, we compiled a comparative table of previously published percutaneous series in hepatic cystic echinococcosis. We performed a targeted narrative search of PubMed up to September 2025, using combinations of the terms ‘cystic echinococcosis’, ‘hepatic hydatid cyst’, ‘percutaneous treatment’, ‘PAIR’, ‘catheterization’, and ‘modified catheterization’, and included human series that reported technical details and outcomes of percutaneous interventions. This approach does not meet formal systematic review criteria, and the table is intended as an illustrative, non-exhaustive synthesis of representative series to highlight technical nuances and reported efficacy and safety profiles.
The study is reported in accordance with the CARE guidelines adapted for case series.
Results
This study involved a total of 8 patients (7 women and 1 man) with 19 hepatic hydatid cysts who underwent our modified PAIR technique between 2011 and 2021. Only two of these patients presented lung hydatid cysts and were treated by surgery and drug therapy (Albendazole) alone. Table 1 presents each patient with their demographic information, cyst characteristics (size, classification, localization), and diagnostic tests (imaging, indirect hemagglutination test for cystic echinococcosis, cytology). Briefly, the patients were aged between 24 and 78 years (mean 46.4 + 16.5 years), cyst size ranged between 15 and 3.5 cm (mean 8.6 + 3.2 cm) with 78.9% of cysts localized in the right hepatic lobe, and 90% classified as CE1 cyst (Polat Type I). We noted one CE3b (Polat IIc) cyst and one complicated cyst (infected cyst with gastric fistula, Polat IV). All patients but one were symptomatic at presentation, with seven patients complaining of right upper quadrant pain/heaviness, and fever, chills, and epigastric pain noted in the patient with a complicated cyst. In this last case, gastroscopy was performed showing erythematous and congestive antral gastritis with the presence of a raised area, on the side of the small curvature, cantered with a fistulous orifice which prompted us to perform an MRI for the better assessment of cysto-gastric fistula (Figure 2). Bacterial cystic fluid culture later detected an extended-spectrum β-lactamase (ESBL)-producing Escherichia coli. A CT was used in most cases, and MRI was performed in two cases: the case mentioned above for cysto-gastric fistula localization, and in the second case for the better diagnosis and staging of a hydatid cyst (here CE3b cyst (Polat IIc)) after a CT showing a cyst with partial septal calcifications. An indirect hemagglutination test was positive in 75% of patients (6 of 8 tested patients), and viable scolices were detected in the cystic fluid of 50% of patients (data was available for only 6 out of 8 patients). Each patient without imaging control data or cysts that responded to drug therapy alone without the necessity of PAIR procedure was excluded from the study (Table 3). The risk and outcomes analyses of our PAIR procedure are based on this selected population, which is about 6 patients with 9 HCE, and are presented in Table 3 and Figure 3.
Abdominal MRI demonstrating a cysto-gastric fistula associated with a hepatic hydatid cyst. Axial (1) and coronal (2) T2-weighted images show a hepatic abscess located between segments II and IV, with communication between the cyst cavity and the gastric lumen.

Clinical and radiological outcomes in patients with complete follow-up (n = 6 patients, 9 cysts)

* Radiographic classification according to Polat/to the WHO 2003 classification.
** Complicated cyst: infected + gastric fistula.
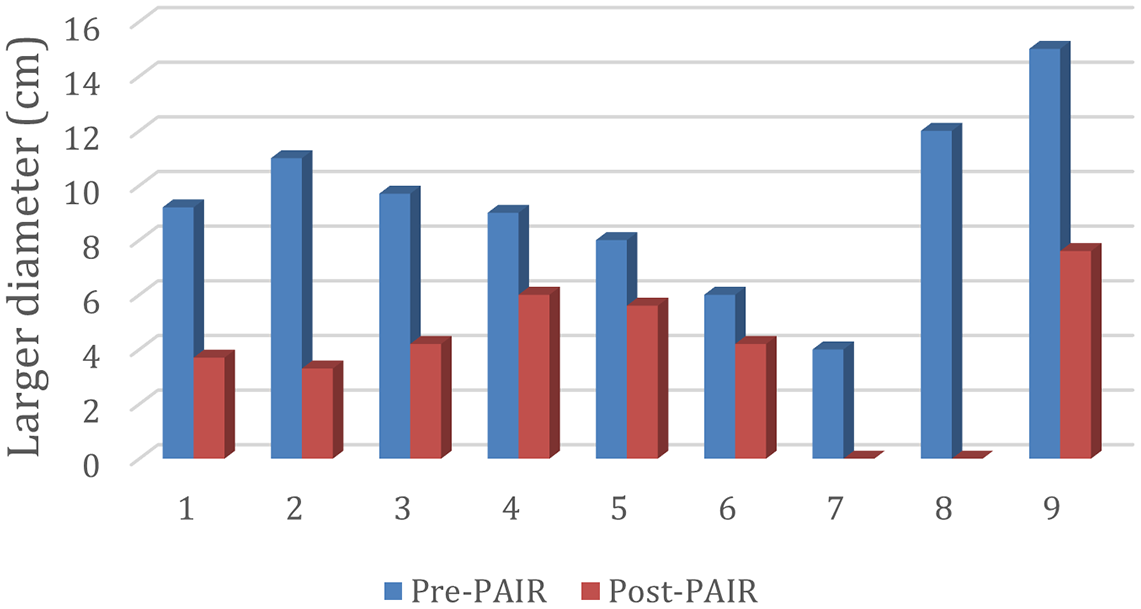
Comparison of maximum cyst diameter (cm) before and after treatment in patients with complete follow-up (n = 6 patients, 9 cysts), demonstrating overall reduction in cyst size.

Outcomes
Post-PAIR imaging control was performed after a mean of 31 months (+/− 19 months, range 6–60). No clinical or imaging evidence of cyst recurrence or reactivation was observed during the available follow-up. The mean reduction in maximal cyst diameter was 59% (p <0.001, range 30–100%), with a 50–70% reduction in 4 cysts, 30% in 3 cysts, and complete regression in 2 cysts (Figure 3). In the remaining cysts, new wall irregularities were noted, consistent with inactivation.
Complications
No major complications were noted. Minor complications were reported in two cases, as two patients developed a fever after the procedure. In the first case (3 cysts treated) the fever lasted for a few hours without requiring any treatment, and in the second case the patient had already presented with fever due to their infected fistulized cyst and required intravenous antibiotics for 10 days after the procedure.
Discussion
Despite the abundant literature on this topic, there is no ‘best treatment option’ for HCE and the randomized evidence comparing the different available interventions remains scarce (Kuehn et al. Reference Kuehn, Uchiumi and Tamarozzi2024). According to WHO-IWGE experts (Arif et al. Reference Arif, Shams-Ul-Bari, Wani, Zargar, Wani, Tabassum, Hussain, Baba and Lone2008; Menezes da Silva Reference Menezes da Silva2003), therapeutic decisions depend on the physician’s competence, the available resources, patient characteristics, and the imaging stage of HCE as stated by the WHO US classification published in 2003 (WHO Informal Working Group 2003). In our study CT and MRI were used instead of US for diagnosis. We thus couldn’t use the WHO classification in the first step, so we first adopted the Polat classification (Vuitton et al. Reference Vuitton, McManus, Rogan, Romig, Gottstein, Naidich, Tuxun, Wen and Menezes da Silva2020), then correlated each category of it to the WHO and Gharbi classification, as shown in Table 2. We compare our therapeutic approach to the WHO-IWGE expert opinions and data in the literature below (Table 4). This comparison is based on a narrative, non-systematic selection of percutaneous series and is intended to illustrate technical nuances and reported outcomes rather than to provide a formal meta-analysis.
Comparison of the modified PAIR technique used in this study with previously reported percutaneous treatment approaches for HCE

Note: This comparison is intended to provide contextual understanding of the technical differences between approaches and should not be interpreted as a formal comparative analysis.
P: Puncture, A: Aspiration, D: Drainage, DD: Daily Drainage, D-PAI: Multiple Sessions Double Percutaneous Aspiration and Ethanol Injection, F: French, G: Gauge, I: Injection, HS: Hypertonic Saline, KT: Catheter, MD: Membrane Detachment, m.d.: Missing Data, no: Number, OCV: Original Cyst Volume, R: Respiration, V.: Volume
* Mean larger diameter reduction.
** Trocar type all-purpose drainage catheter (SkaterTM, Angiotech Pharmaceuticals) + Stopcock.
Our modified technique in symptomatic patients with CE1 cyst with a diameter >5 cm
Classical PAIR consists of puncture with an 18G needle, aspiration of cyst fluid, instillation of a scolicidal solution such as hypertonic saline or ethanol for approximately 20–30 minutes, and a single re-aspiration before removal of the needle in one session (Akhan et al. Reference Akhan, Salik, Ciftci, Akinci, Islim and Akpinar2017; Men et al. Reference Men, Hekimoğlu, Yücesoy, Arda and Baran1999).
PAID modifies this approach by leaving a catheter in situ until drainage decreases to <10 mL per day, a strategy that may improve clearance but is associated with longer dwell times and catheter-related complications (Polat et al. Reference Polat, Balik and Oren2002).
PEVAC (percutaneous evacuation of cyst contents) has been developed for CE2/CE3b cysts, enabling direct suction of membranes and daughter vesicles after catheter insertion; however, significant complications such as CBF, and a high rate of cavity infection have been reported (Schipper et al. Reference Schipper, Laméris, Delden, Rauws and Kager2002).
In contrast, Mo-CAT (modified catheterization) relies on the ‘effective irrigation’ technique using a 14F or smaller catheter without additional devices, allowing continuous evacuation and irrigation but often requiring extended catheterization (Karaagac and Durmaz Reference Karaagac and Durmaz2025).
Our protocol was performed in 7 CE1 (Polat Type I) cysts with a diameter superior to 5 cm. Following the WHO recommendations, PAIR combined with albendazole should have been indicated as first-line therapy. We began our procedure (Figure 4) with the three classical steps of PAIR. Puncture with an 18G needle followed by aspiration of approximately one-third of the cyst fluid released intracystic pressure and helped to prevent leakage. We then injected 20% of hypertonic saline. After these three steps instead of maintaining the 18G needle as in classical PAIR, we inserted an 8F catheter to complete the aspiration. This substitution was intended to reduce the risk of fluid leakage and needle displacement, which are also concerns during Mo-CAT procedures. Avoiding leakage and displacement minimizes the risk of major complications such as anaphylaxis and fistula formation. Compared with established modalities, the 8F catheter allowed faster aspiration and injection and facilitated evacuation of cyst contents, including detached membranes that may obstruct aspiration through an 18G needle.
Step-by-step demonstration of the modified PAIR technique under CT guidance, showing transhepatic puncture and catheter placement (For Video see Supplementary Material).

Through the catheter we performed three cycles of instillation and re-aspiration of hypertonic saline, in contrast to the single dwell used in classical PAIR, thereby maximizing scolicidal exposure (Giorgio et al. Reference Giorgio, De Luca, Gatti, Ciraci’, Montesarchio, Santoro, Di Sarno, Coppola and Giorgio2021; Schipper et al. Reference Schipper, Laméris, Delden, Rauws and Kager2002). This approach may enhance exposure of the germinal layer to scolicidal agents and more complete evacuation of cyst contents. Finally, the catheter was removed immediately after aspiration of all cyst fluid. In classical PAIR, the needle is withdrawn immediately, whereas in PAID the catheter is retained until daily drainage decreases below 10 mL. Finally, the sclerosing agent (alcohol) was selectively injected and re-aspirated in cysts with a diameter superior to 10 cm in order to reduce the residual cavity volume.
This hybrid strategy retains the minimally invasive nature of PAIR, incorporates the improved evacuation of catheterization techniques, and avoids the prolonged dwell times frequent in Mo-CAT. In our series, no major complications such as anaphylaxis, bile leak, or infection were observed, although some authors have reported an increase in the risk of anaphylaxis with early catheter withdrawal, and recommended at least a 24-h delay (Nayman et al. Reference Nayman, Guler, Keskin, Erdem, Borazan, Kucukapan, Ozbiner, Batur, Ertekin, Feyzioglu, Koc, Kaya, Temizoz, Kartal and Ozbek2016). Our findings suggest that a short-cycle catheter-assisted protocol may provide a favourable balance between efficacy and safety. Larger comparative studies with longer follow-up are warranted to confirm whether this approach achieves inactivation and recurrence rates equivalent to or better than existing percutaneous techniques.
Asymptomatic patient with CE1 cyst with a diameter >5cm
In our population, only one patient was asymptomatic with a 9 cm CE1 cyst. We elected to treat this active large cyst using our minimal invasive procedure (modified PAIR) combined with drug therapy. A study published in 1999 demonstrated that the majority of asymptomatic cysts remain asymptomatic regardless of cyst types (Frider et al. Reference Frider, Larrieu and Odriozola1999), and outcomes reveal the 20% spontaneous inactivation of these cysts with long-term stability (Junghanss et al. Reference Junghanss, da Silva, Horton, Chiodini and Brunetti2008; Rinaldi et al. Reference Rinaldi, Brunetti, Neumayr, Maestri, Goblirsch and Tamarozzi2014). Despite this, the WHO recommends a ‘watch and wait’ approach, with long-term US monitoring only in the case of inactive and asymptomatic cysts (CE4 and CE5), while all other cyst types have to be treated using different methods depending on their size and type (Brunetti et al. Reference Brunetti, Kern and Vuitton2010).
In symptomatic patient with CE3b cyst
We treated one CE3b (Polat Type IIc) cyst without noticing any major or minor complication or recurrences. Length of hospitalization was 48 hours. The choice of a non-PAIR percutaneous treatment for this CE3b cyst is in accordance with the 2009 WHO recommendations (Brunetti et al. Reference Brunetti, Kern and Vuitton2010), and in the 2001 WHO/OIE (Organization for Animal Health) manual on Echinococcosis, surgery was stated as a first-line therapy (World Health Organization and World Organisation for Animal Health, 2001). Other sources still consider surgical treatment as a first-line therapy in this type of cyst (Bektasoglu et al. Reference Bektasoglu, Hasbahceci, Tasci, Aydogdu, Malya, Kunduz and Dolay2019; Bhutani and Kajal Reference Bhutani and Kajal2018; Tuxun et al. Reference Tuxun, Aji, Tai, Zhang, Zhao, Cao, Li, Shao, Abudurexiti, H-Z and Wen2014), despite the high risk of complications and mortality. For example, statistical studies on laparoscopic surgery for CE3b and CE2 cysts showed hospitalization for 3–4 days, with 30% complications, and 17% recurrences. In the case of open surgery the length of hospitalization was 4.7 days, with 27% complications (including one case of mortality), and 8.3% recurrences (Bektasoglu et al. Reference Bektasoglu, Hasbahceci, Tasci, Aydogdu, Malya, Kunduz and Dolay2019).
In symptomatic patient with complicated cyst with infection and gastric fistula (Figure 2)
In a second case, we treated an infected hepatic hydatid cyst with gastric fistula (complicated cyst, Polat Type IV) (Figure 2) using our modified PAIR technique. To our knowledge, few cases of liver/intra-abdominal hydatid cyst with gastric fistula have been reported in the medical literature, and no one has been treated by a PT rather than by surgery as recommended by the WHO (Mehta et al. Reference Mehta, Singh and Sood2017; Yildiz et al. Reference Yildiz, Berkem and Hengirmen2010). We thus report here the first use of a PT on a complicated liver cyst with gastric fistula. The patient presented with fever and chills after the procedure. She required 10 days’ hospitalization post-procedure to receive intravenous antibiotherapy for her ESBL E. coli cyst infection. Staying in the context of complicated cysts, a modified PAIR technique called the percutaneous evacuation of cyst content (PEVAC) seems to be effective and safe on non-drainable multivesicular echinococcal cysts (CE2) with or without a cysto-biliary fistula, and on univesicular cysts (CE1–CE3a) presenting a cysto-biliary fistula or compression of the hepatic or portal veins or bile ducts; but no one has presented a gastric fistula (Schipper et al. Reference Schipper, Laméris, Delden, Rauws and Kager2002). This last study and our case highlight the possibility of developing percutaneous treatment for complicated hepatic hydatid cysts.
Drug therapy (albendazole) Peri-procedural drug therapy
We elected to give albendazole 1 week before and 1 month after the procedure. There are no studies evaluating the need for peri-procedural drug therapy in modified PAIR, while in classical PAIR and surgery it is known to reduce and prevent recurrences (Arif et al. Reference Arif, Shams-Ul-Bari, Wani, Zargar, Wani, Tabassum, Hussain, Baba and Lone2008; Gomez I Gavara et al. Reference Gomez, Gavara, López-Andújar, Belda Ibáñez, Ramia Ángel, Moya Herraiz, Orbis Castellanos, Pareja Ibars and San Juan Rodríguez2015; Smego et al. Reference Smego, Bhatti, Khaliq and Beg2003). The post-procedural drug duration should not exceed one month’s therapy to avoid an increase in the rate of side effects, such as perturbation of liver enzymes, as described in the case of a 3-month drug therapy (Akhan et al. Reference Akhan, Yildiz, Akinci, Yildiz and Ciftci2014). Note that albendazole was used for a period of 6 months in adjunction with the PEVAC technique, as mentioned above (Schipper et al. Reference Schipper, Laméris, Delden, Rauws and Kager2002).
Drug therapy alone
Used alone, drug therapy is recommended as the first-line therapy in CE1 and CE3a cysts inferior to 5 cm. Drug therapy is indicated as a second-line therapy when surgical treatment is contraindicated, or for patients with multiple cysts in two or more organs (Brunetti et al. Reference Brunetti, Kern and Vuitton2010). In our case one patient presented 1 pulmonary hydatid cyst and 8 CE1 (Type I Polat) hepatic hydatid cysts. Albendazole was given for 3 months with an effective response for the majority of cysts, except for three hepatic hydatid cysts with diameters of 6, 8, and 9 cm. These cysts were treated successfully with our modified PAIR technique. This result underlines the fact that drug therapy alone is ineffective in cysts with a diameter superior to 5 cm (Stojkovic et al. Reference Stojkovic, Zwahlen, Teggi, Vutova, Cretu, Virdone, Nicolaidou, Cobanoglu and Junghanss2009), and that PTs have to be indicated as first-line therapy.
Classification
HCE classification is well defined by the WHO in the case of uncomplicated cysts investigated with US, but should be revised to include complicated cysts which are yet unclassified. This study highlights the need to consider a CT/MRI classification for HCE. As mentioned before, and used in this article, the Polat classification is based on the hydatid cyst stage and seems to be correlated to the US classification for most categories except CE3a and CE4 types. We performed a simple descriptive correlation between these different classifications to adapt the CT and MRI results to the US results (Table 2). More studies are required to correlate the WHO and the Polat classifications.
Despite its limitations, this study provides a detailed and reproducible technical description that may be of practical interest to clinicians managing hepatic cystic echinococcosis.
Conclusion
Although there is no strong evidence for the superiority of one treatment over others, percutaneous treatments have gained momentum since the discovery of PAIR and PAID in the treatment of HCE. Multiple variants of both these methods have been established in order to provide tailored treatment for each cyst type. In addition to treating seven simple cysts (CE1) and one multivesicular cyst (CE3b) with success, our method permitted us to go beyond percutaneous treatment indications by successfully treating one complicated cyst with gastric fistula without major complications while reducing catheterization time, in a single patient.
These results are promising, but a bigger sample and comparative prospective study are needed in the HCE domain for better assessment and stronger evidence in the treatment of this parasitic disease.
Supplementary material
The supplementary material for this article can be found at http://doi.org/10.1017/S0022149X26101503.
Financial support
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical standard
The authors assert that all procedures contributing to this work were conducted in accordance with the ethical standards of the institutional and national research committees and with the Helsinki Declaration of 1975, as revised in 2008. This retrospective study was approved by the Institutional Review Board (IRB) of Hôpital Psychiatrique de la Croix-Hôpital Universitaire Saint Joseph of Beirut, Lebanon (approval reference number: HPC 001-11-25), and anonymized data were used for analysis.
Artificial intelligence statement
Generative artificial intelligence tools were used to assist with language editing and clarity. The authors take full responsibility for the content, interpretation, and conclusions of this manuscript.








 Open access
Open access