


Introduction
In the developing fetus, the ductus arteriosus is a vascular structure that connects the pulmonary artery to the descending aorta, shunting blood flow away from the lungs. After birth, the ductus arteriosus is typically closed (functionally) within 72 hours of life in response to increased alveolar oxygen tension as well as hormonal and biochemical changes. Reference Eilers, Kyle, Allen and Qureshi1–Reference Hamrick, Sallmon and Rose5 However, when the patent ductus arteriosus fails to close, oxygenated blood from the descending aorta can course into the pulmonary artery resulting in pulmonary over-circulation and subsequent pulmonary oedema, left heart overload and ductal “steal” from the systemic circulation. This can be associated with increased morbidity, including prolonged mechanical ventilation, bronchopulmonary dysplasia, necrotising enterocolitis, and intraventricular haemorrhage, and mortality. Reference Benitz2,Reference Hamrick, Sallmon and Rose5–Reference Conrad and Newberry8
It is well documented that the rate of spontaneous closure of the ductus arteriosus is decreased with younger gestational age or lower body weight. Reference Deshpande, Baczynski, McNamara and Jain6–Reference Semberova, Sirc and Miletin9 Extremely low birth weight infants (birth weight ≤1000 g) are especially prone to persistent patent ductus arteriosus, with studies indicating that spontaneous closure occurs in only 34% of extremely low birth weight infants by day 10 of life. Reference Koch, Hensley, Roy, Brown, Ramaciotti and Rosenfeld10 By contrast, among infants with birth weight >1000 g, spontaneous closure occurs in approximately 94% of infants. Reference Nemerofsky, Parravicini, Bateman, Kleinman, Polin and Lorenz11 Furthermore, extremely low birth weight infants experience a longer time to spontaneous closure, with a median time to closure of 56 days, compared to 7 days among infants with birth weights >1000 g. Reference Hamrick, Sallmon and Rose5 It is speculated that the failure of closure is secondary to a multitude of differences in extremely low birth weight patients including mechanical differences in the patent ductus arteriosus, hypoxia, and increased nitric oxide and prostaglandin signalling. Reference Hamrick, Sallmon and Rose5,Reference Liu, Manganiello, Waleh and Clyman12
Prior observational studies have demonstrated that interventional closure before the first month of life in premature or extremely low birth weight infants is associated with decreased hospital length of stay and reduced rates of bronchopulmonary dysplasia, pulmonary hypertension, intraventricular haemorrhage, necrotising enterocolitis, and mortality. Reference Deshpande, Baczynski, McNamara and Jain6–Reference Nemerofsky, Parravicini, Bateman, Kleinman, Polin and Lorenz11 Although there is growing experience with catheter-based interventional closure, surgical ligation of patent ductus arteriosus at the onset of enrolment was the definitive treatment of extremely low birth weight infants. Moreover, optimal timing for any intervention in extremely low birth weight infants is undefined, with common practice to attempt medical closure in the first month of life prior to attempting surgical closure. Reference Deshpande, Baczynski, McNamara and Jain6,Reference Noori, McCoy and Friedlich7
The purpose of this study was to assess whether surgical ligation of patent ductus arteriosus within the first month of life is associated with decreased mortality, length of mechanical ventilation, neonatal ICU length of stay, rates of tracheostomy during hospital stay, and pulmonary vasodilator or supplemental oxygen use at discharge in extremely low birth weight infants who were diagnosed with a haemodynamically significant patent ductus arteriosus.
Methods
Study population
This was a single-centre retrospective cohort study review of infants who required surgical closure of patent ductus arteriosus between January 2017 and August 2022 at a level IV neonatal ICU based in a tertiary referral centre. The institutional review board at our institution reviewed and approved the study protocol. The study included all neonates undergoing surgical closure of a haemodynamically significant patent ductus arteriosus and weight at birth ≤1000 g. Patients transferred to other hospitals prior to discharge, discharged from the neonatal ICU prior to surgical ligation, and those with complex CHD were excluded. Patients meeting inclusion criteria were then divided into two cohorts: early ligation and late ligation. The early ligation cohort underwent patent ductus arteriosus surgical ligation at or before 30 days of life, and the late ligation cohort underwent surgery after 30 days of life.
Definitions
Haemodynamically significant patent ductus arteriosus
The diagnosis of a haemodynamically significant patent ductus arteriosus was confirmed with clinical assessment and echocardiography by a paediatric cardiologist and neonatal ICU team prior to surgical ligation.
Medical treatment
Pharmacologic therapy with ibuprofen, acetaminophen, or indomethacin was attempted in all cases unless contraindicated. Fourteen patients (33%) were referred to our institution from 8 outside hospitals, so the medical treatment regimens and the number of trials varied. In the absence of standardised protocols for the administration of medical patent ductus arteriosus closure attempts, “Medical treatment” was defined by the medical team’s intention to achieve medical closure when initiating pharmacological therapy.
Surgical ligation
The indications for surgical ligation included failure or contraindications of medical treatment with clinical and/or echocardiographic evidence of a haemodynamically significant patent ductus arteriosus. All patent ductus arteriosus ligations were performed at our institution under general anaesthesia by an experienced paediatric cardiothoracic surgeon via left posterior thoracotomy. While transcatheter closure of patent ductus arteriosus in extremely low birth weight infants has been increasingly adopted after 2019, at the time of this study, surgical ligation was the institutional preference.
Variables and outcomes
Patients’ baseline characteristics including GA, birth weight, weight for GA, sex, age at surgery, and weight at surgery were reviewed. Data concerning preoperative comorbidities, specifically necrotising enterocolitis and intraventricular haemorrhage grade 3 or greater, were also collected.
Clinical outcomes of interest were postoperative mortality during hospital stay and measures of morbidity, including total days of mechanical ventilation, days of mechanical ventilation post-surgical ligation, tracheostomy during hospital stay, length of hospital stay, weight at discharge, and pulmonary vasodilator or supplemental oxygen use at discharge. Length of hospital stay was defined as time since birth to discharge, either to home or to a rehabilitation centre, which was the case for five patients (12%).
Statistical analysis
Continuous data are expressed as mean and standard deviation, while categorical data are expressed as frequency and proportion. Comparisons between categorical variables were performed using chi-square tests or Fisher’s exact tests (if applicable). For continuous variables, data distribution was tested for normality using Shapiro–Wilks’ test. T-tests were performed to compare normally distributed variables, and non-parametric Wilcoxon rank sum tests were performed to compare non-normally distributed variables. Logistic regression modelling was utilised for dichotomous outcome variables by the continuous variable “age at procedure.” Statistical analysis was performed on JMP® Pro Version 16.0.0. A p-value of<0.05 was used to define statistical significance.
Results
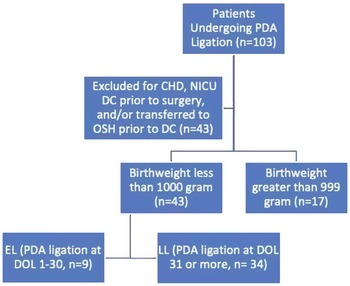
A total of 60 neonates were identified with haemodynamically significant patent ductus arteriosus who received surgical ligation prior to neonatal ICU discharge. Of these, 43 (71.7%) neonates were identified with birth weight less than or equal to 1000 g. Nine (20.9%) of these 43 patients were in the early ligation cohort, and 34 (79.1%) patients were in the late ligation cohort (Fig. 1).
Flow diagram of the study population. PDA, patent ductus arteriosus; DC, discharged; OSH, outside hospital; EL, early ligation; LL, late ligation; DOL, day of life.

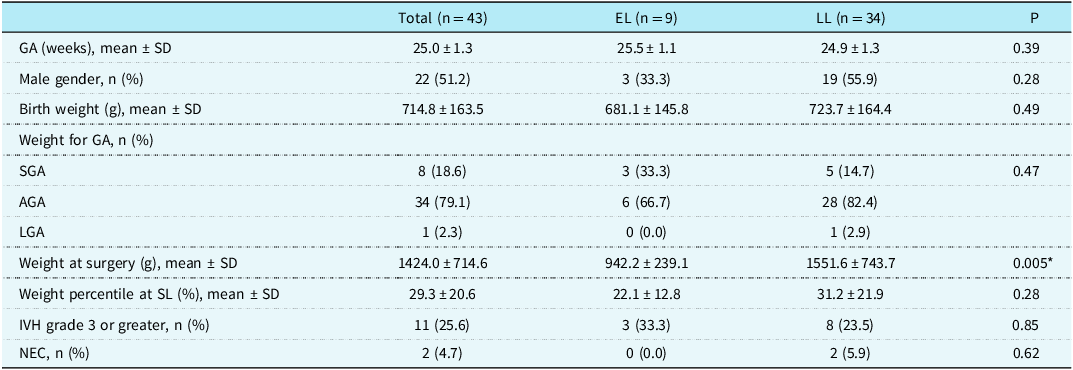
The baseline characteristics and preoperative clinical conditions of all the patients are summarised in Table 1, including a comparison of the early ligation and late ligation groups. Among all surgical ligation patients, 22 (51.2%) were male. Mean gestational age at birth was 25.0 ± 1.3 weeks and mean birth weight was 714.8 ± 163.5 g. Mean weight at the time of surgical patent ductus arteriosus closure was 1424.0 ± 714.6 g. When comparing the characteristics of the two groups, they were found to be clinically similar. As expected, given the difference in age at the time of surgery, weight at surgery was significantly lower in the early ligation group compared to the late ligation group (942.2 ± 239.1 g vs. 1551.6 ± 743.7, p < 0.05). However, weight percentile at surgery did not differ significantly between the two groups, nor did the other baseline characteristics and pre-surgical conditions measured.
Baseline characteristics and pre-ligation clinical conditions of all extremely low birth weight infants undergoing patent ductus arteriosus ligation and a comparison of clinical characteristics between the early ligation (EL) and late ligation (LL) groups

GA, gestational age; g, grams; AGA, appropriate for gestational age; SGA, small for gestational age; LGA, large for gestational age; SL, surgical ligation; IVH, intraventricular haemorrhage; NEC, necrotising enterocolitis.
* p < 0.05, statistically significant.
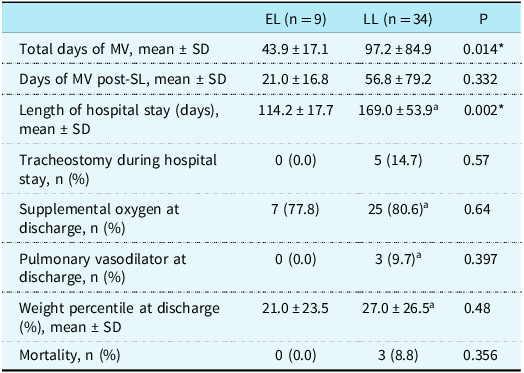
The postoperative clinical outcomes of the study patients, including measures of morbidity and mortality, are summarised in Table 2. Compared to the late ligation group, the early ligation group experienced significantly fewer total days of mechanical ventilation during their hospital stay (43.9 ± 17.1 days vs. 97.2 ± 84.9 days, p < 0.05), as well as a shorter length of hospital stay (114.2 ± 17.7 days vs. 169.0 ± 53.9 days, p < 0.05). Three neonates died during their postoperative hospital stay, with all fatalities occurring within the late ligation group and not thought to be secondary to patent ductus arteriosus ligation, but there was no statistically significant difference in mortality rate between the early ligation and late ligation groups. Causes of mortality were sepsis and pneumonia, acute cardiopulmonary arrest in a tracheostomy-dependent patient, and respiratory failure in a tracheostomy-dependent patient.
Comparison of post-ligation clinical features, morbidity, and mortality between early ligation and late ligation groups

MV, mechanical ventilation; SL, surgical ligation.
* p < 0.05, statistically significant.
a Excluded n = 3 patients who died prior to discharge.
There were no statistically significant differences in postoperative mechanical ventilation time, rates of pulmonary vasodilator or supplemental oxygen use at discharge, rates of tracheostomy during hospital stay, or weight percentile at discharge between the early ligation and late ligation groups. Individual clinical characteristics will be described in the supplemental table.
Discussion
Haemodynamically significant patent ductus arteriosus is a prevalent issue in extremely low birth weight infants and is associated with increased hospital morbidity and mortality. Reference Benitz2,Reference Hamrick, Sallmon and Rose5–Reference Koch, Hensley, Roy, Brown, Ramaciotti and Rosenfeld10,Reference Liu, Manganiello, Waleh and Clyman12 Previous studies have shown that a patent ductus arteriosus in extremely low birth weight infants are less likely to close on their own or they close at much later times than larger birth weight or older gestational age infants. Reference Noori, McCoy and Friedlich7,Reference Koch, Hensley, Roy, Brown, Ramaciotti and Rosenfeld10–Reference Liu, Manganiello, Waleh and Clyman12
The results of this study indicate that when compared with surgical ligation performed after the first month of life, earlier ligation of haemodynamically significant patent ductus arteriosus in extremely low birth weight infants may improve hospital morbidity, including significantly fewer days of mechanical ventilation, as well as shorter hospital stays. However, we found no statistically significant evidence that early patent ductus arteriosus closure was associated with decreased duration of postoperative mechanical ventilation, use of supplemental oxygen or pulmonary vasodilators at discharge, tracheostomy, or mortality.
As indicated above, we found that infants in the early ligation group had fewer total days of mechanical ventilation (43.9 ± 17.1 days vs. 97.2 ± 84.9 days, p < 0.05), but postoperative days of mechanical ventilation did not differ significantly. Due to the large systemic to pulmonary shunt resulting from a patent ductus, surgical ligation of the patent ductus arteriosus likely improved the subsequent pulmonary oedema produced by the pulmonary over-circulation. Reference Eilers, Kyle, Allen and Qureshi1,Reference Tashiro, Perez and Sola13–Reference Hsiao, Wung, Tsao and Chang22 Therefore, infants who underwent earlier surgical ligation could be weaned off support earlier, which may explain the difference in total days of mechanical ventilation between the early ligation and late ligation groups. Prior studies by Jaillard, Ibrahim, and Hsiao also documented improved ventilatory outcomes among premature infants receiving earlier surgical closure of patent ductus arteriosus, including lower fraction of inspired oxygen needed post-operatively, as well as reduced total time on assisted ventilation. Reference Ibrahim, Azab and Kamal18,Reference Jaillard, Larrue, Rakza, Magnenant, Warembourg and Storme21,Reference Hsiao, Wung, Tsao and Chang22 Our study provides further evidence to the benefits of early closure on the ventilation period, but the effects on other indicators of respiratory status remain undetermined. Reference Willis and Weems23
Similarly, our results also indicate that early ligation, as compared to late ligation, is associated with decreased hospital length of stay (114.2 ± 17.7 days vs. 169.0 ± 53.9 days, p < 0.05). In addition to the improvements in respiratory outcomes, as stated above, surgical closure of patent ductus arteriosus in this cohort has also been shown to improve nutritional status, and it is possible that earlier surgical ligation can subsequently contribute to earlier hospital discharge in extremely low birth weight infants as well. Reference Ibrahim, Azab and Kamal18,Reference Jaillard, Larrue, Rakza, Magnenant, Warembourg and Storme21,Reference Hsiao, Wung, Tsao and Chang22,Reference Vida, Lago and Salvatori24
There are few reports currently regarding the optimal timing of surgical ligation in the extremely low birth weight cohort, specifically. One randomised controlled trial by Cassady et al. examined early ligation of the patent ductus arteriosus in 84 extremely low birth weight infants with one group undergoing prophylactic ligation on the day of birth and the other group receiving standard treatment. Reference Cassady, Crouse and Kirklin14 They found that early surgical closure was associated with a lower incidence of necrotising enterocolitis. However, despite the reduced exposure to patent ductus arteriosus in the surgical group, performing prophylactic surgery on day 1 of life is an aggressive procedure that is unlikely to be adopted broadly. Furthermore, this study was unblinded, underpowered and conducted over 30 years ago, and so standard therapies have changed, requiring the results of this study to be interpreted critically. Reference Mosalli and Alfaleh25
Lee et al. assessed whether early closure of haemodynamically significant patent ductus arteriosus (within 7 days) by either medical or surgical means was associated with morbidity in extremely low birth weight, and they found that early closure was related to significantly decreased incidence of bronchopulmonary dysplasia and intraventricular haemorrhage, shorter hospital stays and ventilatory support, as well as improved nutritional outcomes. Reference Lee, Sim and Jung26 A study by Kabra et al. found that surgical ligation of patent ductus arteriosus in extremely low birth weight infants may result in long-term neurosensory impairment, but a more recent study by Fonseca et al. reported that early closure of patent ductus arteriosus (within the first 21 days of life) in preterm infants may actually improve neurological outcomes, as well as lower rates of bronchopulmonary dysplasia, intraventricular haemorrhage, and acute renal failure. Reference Fonseca, Georgiev, Gorenflo and Loukanov17,Reference Kabra, Schmidt and Roberts27 Additionally, Clyman et al. demonstrated that patients less than 28 weeks gestational age that are exposed to a moderate to large patent ductus arteriosus shunt for at least 7–13 days had an increased risk of developing bronchopulmonary dysplasia and death. Reference Clyman, Hills, Liebowitz and Johng28 Exposure beyond this window (14 days or greater) did not significantly increase the incidence. Reference Clyman, Hills, Liebowitz and Johng28
Lastly, interventional and medical management of haemodynamically significant patent ductus arteriosus has changed over the last three decades with surgical ligation rates resultantly decreasing. Reference Bixler, Powers, Clark, Walker and Tolia29–Reference Reese, Scott and Patrick31 Medical treatment alone offers moderate success rates as a non-invasive method of closure, but treatment fails in 20–40% of cases. Reference Fraisse, Bautista-Rodriguez, Burmester, Lane and Singh32 Furthermore, the agents used can have adverse effects in neonates or may be contraindicated in cases of infants with renal impairment, necrotising enterocolitis, or intestinal perforations. Reference Fraisse, Bautista-Rodriguez, Burmester, Lane and Singh32 While surgical ligation patients in the current era are a complex cohort secondary to advances in medical care, serious short-term adverse events are seen in a minority of patients with decreased mortality compared to medical treatment alone. Reference Foster, Mallett and Govande33,Reference Weisz, More, McNamara and Shah34 Intraoperative hurdles included avoiding injury to the vascular structures and the recurrent laryngeal nerve. Surgical ligation for this cohort has been further reduced by the advancement of percutaneous patent ductus arteriosus closure in recent years, which has demonstrated relative safety and effectiveness in patients under 2 kilograms when performed by a trained interventionalist. Reference Sathanandam, Gutfinger and O’Brien35–Reference Zahn, Peck and Phillips37 In a retrospective review performed by Sathanandam et al. comparing outcomes of extremely low birth weight infants undergoing transcatheter patent ductus arteriosus closure or surgical ligation, those who received transcatheter closure demonstrated more improved pulmonary outcomes post-procedure compared to surgical closure. Reference Sathanandam, Balduf and Chilakala36 Similarly, a retrospective review by Regan et al. comparing surgical and transcather closure in preterm infants found that neonates undergoing transcatheter closure experienced shorter duration of mechanical ventilation during their post-procedure stay in the neonatal ICU. Reference Regan, Benbrik and Sharma38 Further, compared to surgical ligation, transcatheter closure has been found to result in lower incidence of complications, including post-ligation syndrome. Reference Parkerson, Philip, Talati and Sathanandam39 While transcather closure was not performed at our institution at the time of this study, these observational studies suggest that transcatheter closure may offer improved outcomes compared to surgical closure techniques. However, these findings may be centre-dependent, and large randomised clinical trials comparing transcather and surgical closure are necessary to determine the true differences in short- and long-term outcomes in the extremely low birth weight cohort.
In our study, the surgical closure of patent ductus arteriosus in extremely low birth weight infants within the first 30 days of life was correlated with improved ventilatory outcomes and shorter hospital lengths of stay, similar to previous studies examining more broadly defined cohorts of infants. Nevertheless, the evidence regarding optimal timing of surgical patent ductus arteriosus closure in extremely low birth weight infants remains limited and heterogeneous and is likely to be defined only with prospective randomised studies.
Limitations
There are several limitations in our study. This is a retrospective observational design with a relatively small sample size, and given the observational nature of the study, there may be further confounding variables complicating the analyses of our data. Our single-centre study may not reflect a diverse population. Our centre did not offer transcatheter closure for the cohort in question during the enrolment period and thus only evaluated patients undergoing surgical ligation. The lack of a standardised protocol for the duration of the study period may increase selection bias. The inclusion of patients referred from outside hospitals introduced possible differences in initial treatment strategies, and other clinical conditions originating from prematurity may confound the associations measured in our study.
Conclusions
A haemodynamically significant patent ductus arteriosus should be ligated when pharmacologic treatment has failed or is contraindicated. However, the optimal timing for surgical ligation of patent ductus arteriosus in extremely low birth weight infants has not yet been defined. Extending the time to surgical ligation beyond the first month of life in extremely low birth weight infants is associated with less favourable ventilatory outcomes and prolonged hospital stays. Earlier surgical patent ductus arteriosus ligation may improve patients’ clinical outcome and should therefore be considered. Prospective randomised trials are needed to address the optimal timing of patent ductus arteriosus surgical ligation in extremely low birth weight infants in the future.
Acknowledgements
The authors would like to acknowledge Kathy Redmond, RN, Bingi Kanagwa, BS and David Alexander with data collection.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1047951123004432.
Financial support
No funding was provided for this project.
Competing interests
The authors, whose names are listed above, certify that they have no affiliations or involvement in any organisations with financial or non-financial interests outside of what is listed below that may pertain to this subject or manuscript.



 Open access
Open access