


Introduction
Family caregivers of older adults living with Alzheimer’s disease and related dementias (ADRD) are uniquely at risk for sustained psychological distress (i.e., depressive and anxiety symptoms) given the progressive nature of the disease and increasing caregiving demands over time (Fonareva and Oken Reference Fonareva and Oken2014; Cho et al. Reference Cho, Sands and Stevens2024). Grief experienced while the person living with ADRD is still alive may contribute to increased psychological distress and adversely affect the long-term mental health of family caregivers (Rando Reference Rando1986; Lindauer and Harvath Reference Lindauer and Harvath2014; Dehpour and Koffman Reference Dehpour and Koffman2023; Manevich Reference Manevich2025). This form of grief is commonly referred to as anticipatory grief, although related terms such as pre-death grief and dementia-related grief are also used in the literature. Unlike bereavement following death, anticipatory grief reflects caregivers’ emotional responses to cumulative and ongoing losses related to progressive cognitive decline and changes in the caregiver–care recipient relationship, with potential implications for caregiver well-being and the quality of care provided to the person living with ADRD (Rando Reference Rando1986).
Anticipatory grief is highly prevalent among caregivers of people living with ADRD, with rates ranging from 10% to 32% (Crawley et al. Reference Crawley, Sampson and Moore2023). The elevated prevalence likely reflects the progressive and prolonged nature of dementia, which exposes caregivers to gradual losses in communication and relationship quality, stress related to managing behavioral and psychological symptoms of dementia (BPSD), and increasing caregiving burden. Prior research has identified different caregiver and contextual factors associated with higher levels of anticipatory grief, including caregivers’ sex and their relationship to the person living with ADRD, caregiving intensity (i.e., time spent providing care and number of caregiving-related tasks), dementia severity, and available social support (Chan et al. Reference Chan, Livingston and Jones2013; Crawley et al. Reference Crawley, Sampson and Moore2023; Wangliu and Che Reference Wangliu and Che2025). However, prior studies have typically examined these factors in isolation and have used heterogeneous definitions and measures of anticipatory grief, thereby limiting understanding of how caregiving-related stressors, relationship changes, and psychosocial resources are jointly associated with anticipatory grief and caregiver mental health outcomes.
Prior reviews have addressed specific aspects of anticipatory grief in ADRD caregiving, such as the social environment, measurement of pre-death grief, or the prevalence and correlates of grief before and after death (Nielsen et al. Reference Nielsen, Neergaard and Jensen2016; Crawley et al. Reference Crawley, Sampson and Moore2023; Dehpour and Koffman Reference Dehpour and Koffman2023; Ng et al. Reference Ng, Jiao and Suen2025). Additionally, prior reviews of psychosocial interventions for caregiver grief have not primarily focused on family caregivers of people living with ADRD and have largely focused on caregivers of individuals residing in long-term care settings (Wilson et al. Reference Wilson, Toye, Aoun, Slatyer, Moyle and Beattie2017). Although these reviews have advanced understanding of anticipatory grief, the literature in this area has grown rapidly in recent years. In addition, prior reviews have largely examined individual domains in isolation. The present review synthesizes evidence across caregiving-related stressors, relationship changes, and psychosocial resources within caregiving stress frameworks to better understand mechanisms associated with anticipatory grief and caregiver mental health outcomes.
Theoretical framework
The Stress Process Model provides a useful framework for understanding how caregiving-specific risk and resilience factors influence caregivers’ psychological outcomes, including anticipatory grief (Pearlin et al. Reference Pearlin, Mullan and Semple1990). The model posits that relationships among caregivers’ background and context, caregiving primary and secondary stressors, and mediating factors contribute to psychological and physical health outcomes. Background and context include caregiver sociodemographic characteristics, such as age and gender. Primary stressors refer to demands directly related to caregiving, such as ADRD severity, BPSD management, and functional limitations, whereas secondary stressors are those indirectly related to the caregiving role, such as financial strain and competing family or work demands. Finally, mediating factors, such as coping strategies and social support, represent resources that can mitigate the adverse effects of caregiving-related stressors on caregivers’ health.
Building on the Stress Process Model, the Grief-Stress Model of caregiving conceptualizes anticipatory grief as a central outcome of caregiving stress, driven primarily by ambiguous loss and role overload (Noyes et al. Reference Noyes, Hill and Hicken2010). Ambiguous loss refers to changes in the caregiver–care recipient relationship (e.g., changes in communication or companionship over time), while role overload reflects caregiver losses associated with the demands of caregiving (e.g., loss of personal freedom, personal identity, and social connections). This model emphasizes that caregiver grief is influenced by the perceived significance of these losses and available coping resources.
Guided by the Stress Process Model and the Grief-Stress Model of Caregiving, the purpose of this scoping review was to synthesize evidence on risk and resilience factors associated with anticipatory grief, its relationship with caregiver mental health, and psychosocial interventions targeting anticipatory grief among family caregivers of people living with ADRD. Given the breadth of the topic, the conceptual heterogeneity of anticipatory grief, and the wide range of study designs and outcomes in recent literature, a scoping review was appropriate to comprehensively map what is known about anticipatory grief in dementia caregiving. This review extends prior research by organizing existing evidence within caregiving stress frameworks to identify potentially modifiable risk and resilience factors associated with anticipatory grief and caregiver mental health outcomes (Figure 1). The following research questions guided this scoping review:
1. What caregiving-related stressors, relationship changes, and psychosocial resources are associated with anticipatory grief among family caregivers of people living with ADRD?
2. How is anticipatory grief associated with caregiver mental health outcomes among family caregivers of people living with ADRD?
3. What psychosocial interventions have been evaluated to address anticipatory grief and caregiver mental health outcomes among family caregivers of people living with ADRD?
Figure 1.Sociodemographic, caregiving, and psychosocial factors associated with anticipatory grief.


Methods
This scoping review was conducted following the Arksey and O’Malley (Reference Arksey and O’Malley2005) methodological framework, which includes 5 key stages: specifying the research question; identifying relevant literature; selecting studies; mapping the data; and summarizing, synthesizing, and reporting the results. Reporting of the review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (Tricco et al. Reference Tricco2018).
Search strategy
An academic reference librarian (JG) conducted a comprehensive search across 6 electronic databases: PubMed, CINAHL, Embase, Scopus, Web of Science, and PsycINFO. To extend and update prior reviews that included earlier literature, the search was limited to publications from January 2014 to May 2025 and was completed on May 23, 2025. This timeframe was selected to capture recent studies published following earlier reviews and reflect more recent conceptual and empirical developments in anticipatory grief research in dementia caregiving. The search terms included, but were not limited to, “caregivers,” “dementia,” “Alzheimer’s disease,” “pre-death grief,” and “anticipatory grief.” Detailed search terms for each database are available in Supplementary Material 1.
Eligibility criteria
To be included in the review, studies needed to (i) examine anticipatory grief among family caregivers of people living with ADRD and (ii) report empirical findings related to caregiving-related stressors, relationship changes, psychosocial resources, caregiver mental health outcomes, or psychosocial interventions targeting anticipatory grief. Peer-reviewed original research articles written in English, with full-text access, were included. Studies focused exclusively on bereaved caregivers or post-bereavement outcomes were excluded.
Selection of sources of evidence
For the screening and selection process, search results were exported into Covidence, a web-based collaboration software designed to support literature reviews (Covidence 2025). Duplicate articles were removed by Covidence and manually by 2 independent reviewers (NARC and LAD). Both reviewers independently screened potential abstracts and full-text articles using the predefined inclusion criteria. A third reviewer (FP) resolved conflicts, as needed.
Data extraction
Data from eligible studies were extracted in Covidence using a data extraction matrix that was developed a priori. Two reviewers (NARC and LAD) independently extracted study data, and then collaboratively refined and finalized the entries using an iterative process. Extracted data included study characteristics (e.g., authors, country, study design and aims, and anticipatory grief assessment), sample characteristics (e.g., sample size, age, sex, caregiver relationship to the care recipient, and race/ethnicity), and main findings (e.g., risk and protective factors associated with anticipatory grief). Additional details are presented in Table 1.
Sampled study characteristics (n = 30)

ACT = acceptance and commitment therapy, AD = Alzheimer’s disease, AG = anticipatory grief, BPSD = behavioral and psychological symptoms of dementia, CG = caregivers, LBD = Lewy Body Dementia, YOD = Young-onset dementia. The study by Pérez-González et al. (Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023) was built upon the data collected in their earlier research from 2021 (Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021). The study conducted by Moore et al. (Reference Moore, Crawley and Fisher2023) and Moore et al. (Reference Moore, Crawley and Vickerstaff2020) used the same sample of caregivers. The study conducted by Liew et al. (Reference Liew, Tai and Yap2019) corresponds to the follow-up for the participants recruited in their previous study (Liew et al. Reference Liew, Tai and Yap2018).
Synthesis and reporting
A descriptive synthesis was conducted to summarize key findings across included studies. Studies were first characterized by design and sample characteristics. Findings were then organized and synthesized across the following key domains: (i) sociodemographic characteristics and caregiving context, (ii) caregiving-related stressors, (iii) relationship changes, (iv) psychosocial resources, (v) mental health outcomes, and (vi) intervention approaches. Quantitative results were synthesized narratively to summarize the direction and nature of associations across studies, while qualitative data were analyzed to identify recurrent themes and explanatory insights. Figure 1 presents the organizing framework for the results.
Results
Study selection and characteristics
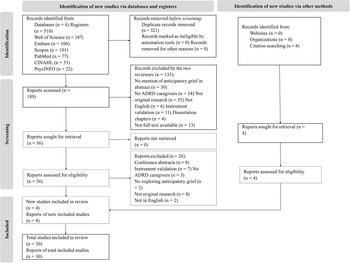
The search resulted in 510 articles. After removing 321 duplicates, 189 articles were screened for eligibility. Of these, 133 were excluded after title and abstract screening. Thirty studies met the inclusion criteria and were included in the final review (Figure 2).
PRISMA flow diagram of study selection process.

Of the included studies, 18 were quantitative, 4 were qualitative, 2 were mixed methods, and 6 were intervention studies. Almost half of the studies were cross-sectional (n = 14). Most of the studies were conducted in the United States (n = 11) and Singapore (n = 5). The most common anticipatory grief measures were the Marwit–Meuser Caregiver Grief Inventory Short Form (MM-CGI-SF) (n = 10) and the Marwit–Meuser Caregiver Grief Inventory (MM-CGI) (n = 7), including sub-scales measuring personal sacrifice and burden (PS&B), heartfelt sadness and longing (HS&L), and worry and felt isolation (W&FI).
Across all studies, 4,580 family caregivers of people living with ADRD were included. Sample sizes ranged from 103 to 530 in quantitative studies, 8 to 33 in qualitative studies, 106 to 150 in mixed methods studies, and 9 to 273 in intervention studies. The average age among caregivers ranged from 53 to 71 years. Caregivers were predominantly female (52.5–88.7%) and most commonly adult children (n = 2,106) or spouses (n = 1,669). Samples primarily included caregivers identifying as White or Asian. Additional study characteristics are presented in Table 1.
Sociodemographic characteristics and caregiving context
Caregiver sociodemographic characteristics were frequently examined as variables associated with anticipatory grief. Two studies found no significant association between caregiver age and anticipatory grief (Park and Galvin Reference Park and Galvin2021; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021). Findings regarding sex were mixed. Three studies reported that the caregiver’s sex was not associated with anticipatory grief (Meichsner et al. Reference Meichsner, Theurer and Wilz2018; Park and Galvin Reference Park and Galvin2021; Türk et al. Reference Türk, Aydemir and Özel-Kizil2025), while 3 studies reported that female caregivers had higher levels of anticipatory grief (Moore et al. Reference Moore, Crawley and Vickerstaff2020; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024). Educational attainment showed similar mixed patterns. Two studies reported that lower caregiver educational attainment was associated with higher levels of anticipatory grief (Liew et al. Reference Liew, Tai and Yap2018; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024), while other studies found no statistically significant differences by educational attainment (Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021; Türk et al. Reference Türk, Aydemir and Özel-Kizil2025).
Relationship to the person living with ADRD demonstrated more consistent associations. Six studies found that spousal caregivers reported higher levels of anticipatory grief (Meichsner and Wilz Reference Meichsner and Wilz2016; Liew et al. Reference Liew, Tai and Yap2018; Meichsner et al. Reference Meichsner, Theurer and Wilz2018; Moore et al. Reference Moore, Crawley and Vickerstaff2020; Park and Galvin Reference Park and Galvin2021; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021). However, one study reported that adult children had higher scores on the MM-CGI W&FI subscale compared to spousal caregivers (Türk et al. Reference Türk, Aydemir and Özel-Kizil2025). Caregivers who co-resided with the person living with ADRD reported more negative caregiving experiences, which were associated with higher levels of anticipatory grief (Chaudhry et al. Reference Chaudhry, Poco and Balasubramanian2024). Finally, greater caregiver involvement, including identifying as the primary caregiver, longer caregiving duration (i.e., number of years as a caregiver), and more daily hours spent providing care were associated with higher levels of anticipatory grief (Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021).
Characteristics of the person living with ADRD were also associated with caregivers’ anticipatory grief. Three studies reported that the younger age of the person living with ADRD was associated with higher levels of anticipatory grief (Liew et al. Reference Liew, Tai and Yap2018; Moore et al. Reference Moore, Crawley and Vickerstaff2020; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021). Six studies reported that dementia severity was associated with anticipatory grief (Cheung et al. Reference Cheung, Khm and Cheung2018; Liew et al. Reference Liew, Tai and Yap2018; Park and Galvin Reference Park and Galvin2021; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024; Türk et al. Reference Türk, Aydemir and Özel-Kizil2025). Further, caregivers of people with a later stage ADRD reported higher levels of anticipatory grief (Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2021; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024; Türk et al. Reference Türk, Aydemir and Özel-Kizil2025). Specifically, spousal caregivers of people in late-stage ADRD reported significantly higher PS&B and W&FI scores of the MM-CGI-SF than those caring for people in early stages and adult child caregivers of a person in either early or later ADRD stages (Cheung et al. Reference Cheung, Khm and Cheung2018). However, among caregivers of people with Lewy Body Dementia, dementia stage was not associated with anticipatory grief (Park and Galvin Reference Park and Galvin2021).
Caregiving-related stressors and burden, relationship changes, and psychosocial resources associated with anticipatory grief
Caregiving-related stressors and burden
One study found that BPSD, established caregiving-related stressors, increased anticipatory grief directly and indirectly through negative caregiving experiences. Specifically, BPSD increased negative caregiving experiences, which in turn were associated with higher levels of anticipatory grief (Chaudhry et al. Reference Chaudhry, Poco and Balasubramanian2024). However, another study reported that BPSD were not significantly associated with anticipatory grief (Park and Galvin Reference Park and Galvin2021). Nine studies reported that higher levels of anticipatory grief were associated with higher perceived caregiving burden (Cheung et al. Reference Cheung, Khm and Cheung2018; Liew et al. Reference Liew, Tai and Yap2018, Reference Liew, Tai and Wee2020; Park and Galvin Reference Park and Galvin2021; Gilsenan et al. Reference Gilsenan, Gorman and Shevlin2023; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024; Wangliu and Chen Reference Wangliu and Chen2024; Türk et al. Reference Türk, Aydemir and Özel-Kizil2025). Among the 3 MM-CGI-SF subscales, the PS&B subscale had the strongest association with caregiving burden. After excluding the PS&B subscale, caregiving burden remained associated with HS&L and W&FI subscales (Gilsenan et al. Reference Gilsenan, Gorman and Shevlin2023). Finally, Liew et al. (Reference Liew, Tai and Yap2018) found that caregiving burden and anticipatory grief were both associated with ADRD stage, BPSD, and caregiving role (i.e., being the primary caregiver).
Relationship changes
Three studies reported that ADRD family caregivers experienced anticipatory grief related to the loss of the person they had known and the realization of future losses (Champlin Reference Champlin2020; Duplantier and Williamson Reference Duplantier and Williamson2023; Moore et al. Reference Moore, Crawley and Fisher2023). Caregivers described progressive losses in their relationship with the person living with dementia, including decreased reciprocity and emotional connection. Three studies described role changes in the relationship with the person living with ADRD (e.g., becoming the primary decision-maker, assuming responsibility for organizing their social life, or feeling like a separated spouse despite being married), which contributed to feelings of relationship loss (Duplantier and Williamson Reference Duplantier and Williamson2023; Moore et al. Reference Moore, Crawley and Fisher2023; Kotwal et al. Reference Kotwal, Allison and Halim2024). Spouses also described loss of reciprocity in the relationship, and daughters described becoming the “new parent” (Duplantier and Williamson Reference Duplantier and Williamson2023). As caregivers acknowledged relationship changes, they described adjusting their expectations of the relationship and adapting shared social activities to preserve relationship quality (Kotwal et al. Reference Kotwal, Allison and Halim2024). Finally, anticipatory grief was negatively associated with marital satisfaction and life satisfaction (Pote and Wright Reference Pote and Wright2018). However, the quality of the caregiver–care recipient relationship was not associated with caregiver anticipatory grief (Chaudhry et al. Reference Chaudhry, Poco and Balasubramanian2024).
Psychosocial resources
Across studies, psychosocial resources were consistently examined as potential protective factors associated with lower levels of anticipatory grief; however, findings varied by domain. Higher psychological well-being, quality of life, and resilience were associated with lower levels of anticipatory grief (Cheung et al. Reference Cheung, Khm and Cheung2018; Liew et al. Reference Liew, Tai and Wee2020; Park and Galvin Reference Park and Galvin2021; Gilsenan et al. Reference Gilsenan, Gorman and Shevlin2023). Similarly, greater perceived closeness was associated with lower levels of anticipatory grief (Pote and Wright Reference Pote and Wright2018; Moore et al. Reference Moore, Crawley and Vickerstaff2020). Further, among spousal caregivers, low levels of avoidant (i.e., experiencing discomfort with intimacy and preferring independence) and anxious attachments (i.e., fearing rejection and abandonment) were associated with lower levels of anticipatory grief (Pote and Wright Reference Pote and Wright2018).
Coping strategies emerged as a predominant psychosocial factor associated with anticipatory grief. Specifically, greater anticipatory grief was associated with higher use of dysfunctional coping, such as denial, avoidance, and self-blame (Kobiske et al. Reference Kobiske, Bekhet and Garnier-Villarreal2019; Duplantier and Williamson Reference Duplantier and Williamson2023; Moore et al. Reference Moore, Crawley and Fisher2023; Kotwal et al. Reference Kotwal, Allison and Halim2024; Wangliu and Chen Reference Wangliu and Chen2024). Adaptive coping, such as acceptance, humor, carer identity, and seeking support, was found to help caregivers manage anticipatory grief (Moore et al. Reference Moore, Crawley and Fisher2023). Active coping mediated the association between caregiving burden and anticipatory grief among female ADRD caregivers (Wangliu and Chen Reference Wangliu and Chen2024), while personal resourcefulness (e.g., planning tasks) buffered the association between anticipatory grief and perceived stress (Kobiske et al. Reference Kobiske, Bekhet and Garnier-Villarreal2019). Further, age-related differences in coping were also observed. Older ADRD family caregivers described relying on faith and spirituality to manage anticipatory grief, emphasizing connection to a higher power and community, while younger caregivers reported prioritizing social connection outside the home (Duplantier and Williamson Reference Duplantier and Williamson2023). Finally, preparedness for future losses was associated with lower levels of anticipatory grief (Supiano et al. Reference Supiano, Luptak and Andersen2022), whereas certain forms of planning for future loss (e.g., funeral arrangements) were associated with higher levels of anticipatory grief (Ménard et al. Reference Ménard, Adekoya and Birchall2025).
Findings regarding social support were mixed. Some studies reported that greater perceived support was associated with lower levels of anticipatory grief (Moore et al. Reference Moore, Crawley and Vickerstaff2020; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024), whereas others found no direct or moderating effects (Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023; Malhotra et al. Reference Malhotra, Chaudhry and Shah2024a). Two studies found that high social support was associated with lower levels of anticipatory grief (Moore et al. Reference Moore, Crawley and Vickerstaff2020; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024). Specifically, social support was associated with lower scores in the MM-CGI-SF PS&B and W&FI subscales (Moore et al. Reference Moore, Crawley and Vickerstaff2020). Pérez-González et al. (Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023) found that social support did not have a direct effect on anticipatory grief; however, it had an indirect effect on anticipatory grief based on the psychological health of the caregiver (e.g., symptoms of depression and anxiety, obsessive-compulsive behaviors, and hostility). Similarly, family support did not moderate the association between caregiving burden and anticipatory grief (Malhotra et al. Reference Malhotra, Chaudhry and Shah2024a).
Mental health outcomes
Six studies reported that anticipatory grief was associated with greater depressive symptoms (Liew et al. Reference Liew, Tai and Yap2019, Reference Liew, Tai and Wee2020; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023; Argueta et al. Reference Argueta, Brice and Wu-Chung2024; Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024; Brice et al. Reference Brice, Paoletti-Hatcher and Wu-Chung2025). Depressive symptoms were associated with higher scores in the MM-CGI-SF HS&L and W&FI subscales (Sánchez-Alcón et al. Reference Sánchez-Alcón, Garrido-Fernández and Cano-Rojas2024). Some studies found that anticipatory grief contributed to caregiver depression independently of caregiving burden. Further, it was found that anticipatory grief amplified the effect of caregiving burden on depression and predicted depression up to 2.5 years later after controlling for baseline depression (Liew et al. Reference Liew, Tai and Yap2019; Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023). These findings suggest that anticipatory grief may uniquely influence long-term depression. Further, among ADRD family caregivers with high or average anticipatory grief, loneliness was associated with higher levels of depression (Brice et al. Reference Brice, Paoletti-Hatcher and Wu-Chung2025). Beyond depression, one study found that the direct effect of anticipatory grief on broader caregiver psychological health was stronger than its indirect effect through caregiving burden (Pérez-González et al. Reference Pérez-González, Vilajoana-Celaya and Guàrdia-Olmos2023).
Interventions for managing anticipatory grief
Six studies evaluated interventions to address anticipatory grief among ADRD family caregivers. Four were randomized controlled trials (Meichsner and Wilz Reference Meichsner and Wilz2016; Meichsner et al. Reference Meichsner, Theurer and Wilz2018; Risch et al. Reference Risch, Franziska and Wilz2024; Han et al. Reference Han, Oster and Yuen2025) and 2 were pre-/post-intervention studies (Paulson et al. Reference Paulson, McClure and Wharton2024; Stevens-Neck et al. Reference Stevens-Neck, Walton and Alterkawi2024). A manualized individual therapy intervention grounded in acceptance-based approaches demonstrated reductions in anticipatory grief, particularly among ADRD family caregivers actively providing in-home care (Meichsner and Wilz Reference Meichsner and Wilz2016). An online, therapist-guided writing intervention improved coping with anticipated loss and increased use of psychosocial resources (e.g., problem-solving abilities, social support, and coping) in the short term; however, these benefits were not sustained at 5-month follow-up (Meichsner et al. Reference Meichsner, Theurer and Wilz2018). Acceptance and commitment therapy (ACT), delivered via telephone or videoconferencing, showed mixed findings. Telephone-based ACT improved acceptance of loss at 6-month follow-up (Risch et al. Reference Risch, Franziska and Wilz2024), whereas a Zoom-delivered ACT intervention demonstrated within-group improvements in anticipatory grief that were maintained after 3 months, but no significant between-group differences were observed (Han et al. Reference Han, Oster and Yuen2025).
Group-based and psychoeducational interventions were found to have modest benefits. A pilot grief-focused program emphasizing identity adaptation and peer support did not show significant between-group differences in anticipatory grief, however, qualitative findings suggested improved emotional processing and normalization of grief experiences (Stevens-Neck et al. Reference Stevens-Neck, Walton and Alterkawi2024). Similarly, the Savvy Caregiver Program, which emphasizes dementia knowledge, preparedness, and self-care, was associated with reductions in anticipatory grief from baseline. Specifically, greater preparedness was associated with greater reductions in anticipatory grief (Paulson et al. Reference Paulson, McClure and Wharton2024). Overall, interventions that emphasized acceptance, preparedness, and meaning-making demonstrated the most consistent improvements in anticipatory grief, although sustained effects and between-group differences were variable.
Discussion
This scoping review synthesized evidence from 30 studies examining anticipatory grief among family caregivers of people living with ADRD and identified several consistent patterns. Caregiving-related stressors, specifically BPSD management, were associated with higher levels of anticipatory grief. Relationship changes, including loss of reciprocity and shifting roles, were key contributors to anticipatory grief. Psychosocial resources, such as coping strategies, social support, and resilience, were generally associated with lower levels of anticipatory grief; however, findings were mixed across studies. Further, anticipatory grief was consistently associated with depressive symptoms and broader psychological health, including associations with longer-term mental health outcomes independent of caregiving burden. Finally, intervention studies that assessed anticipatory grief among family caregivers of people living with ADRD were limited, but findings suggest that interventions focused on acceptance and preparedness may help mitigate anticipatory grief.
Our findings suggest that anticipatory grief can be understood as a dynamic and relationship-dependent process. This conceptualization of anticipatory grief reflects the emotional adjustments that caregivers make in response to ongoing stressors and evolving caregiving demands. Prior research demonstrates that caregivers’ day-to-day mental health is associated with daily stressors and the availability of psychosocial resources such as social support (Puga et al. Reference Puga, Wang and Rafford2023). Progressive losses experienced across the ADRD trajectory may contribute to changes in how caregivers perceive their role and their interactions with the person living with ADRD over time. Changes in role identity, increasing involvement in decision-making, and growing emotional distance may intensify caregivers’ negative perceptions of caregiving and adversely affect their mental health (Quinn and Toms Reference Quinn and Toms2018; Shrestha et al. Reference Shrestha, Richey and Lipovac-Dew2022; Malhotra et al. Reference Malhotra, Chaudhry and Shah2024b).
Based on the Stress Process Model and the Grief-Stress Model of Caregiving, ambiguous loss, relationship changes, and role overload may be conceptualized as primary and secondary stressors within the caregiving context. Variability in exposure to these stressors over time may contribute to heterogeneity in anticipatory grief onset and severity, as caregivers experience new losses, reframe the meaning of their relationship with the person living with ADRD, or develop ambivalent feelings about their role (Cross et al. Reference Cross, Garip and Sheffield2018). This conceptual framing highlights how ambiguous loss and caregivers’ emotional readjustment to the caregiving role creates a context in which anticipatory grief is recurrent and cumulative, with implications for long-term psychological functioning (Pearlin et al. Reference Pearlin, Mullan and Semple1990; Noyes et al. Reference Noyes, Hill and Hicken2010).
Our review suggests that anticipatory grief may emerge from the interaction of caregiving-related stressors and caregivers’ psychosocial resources. However, broader literature has largely focused on risk factors, with relatively few examinations of how risk and resilience processes interact in the context of anticipatory grief (Barrera-Caballero et al. Reference Barrera-Caballero, Romero-Moreno and Del Sequeros Pedroso-Chaparro2021; Gorostiaga et al. Reference Gorostiaga, Etxeberria and Salaberria2022; Liu et al. Reference Liu, Chi and Wu2022; Magan et al. Reference Magan, Hirschman and Starr2022; Fowler et al. Reference Fowler, Perkins and Park2024; Rebolo et al. Reference Rebolo, Maroco and de Mendonça2025). Considering these processes separately may obscure dynamic mechanisms that influence caregivers’ vulnerability to anticipatory grief and mental health challenges over time.
Consistent with this perspective, spousal caregivers who co-reside with the person living with ADRD, provide care to a younger care recipient, and manage multiple BPSD may be more vulnerable to anticipatory grief. In contrast, caregivers with similar risks but who use more positive psychosocial factors, such as acceptance and adaptive coping strategies, have a closer relationship to the care recipient and are more prepared for their role, may therefore demonstrate greater resilience and lower levels of anticipatory grief. Relationship changes can also bring positive caregiving experiences, including personal growth, strengthened bonds, a sense of duty, and competence, which may further strengthen resilience and enhance perceived rewards of caregiving (Lloyd et al. Reference Lloyd, Patterson and Muers2016; Park et al. Reference Park, Matta-Singh, Park, Rhee, Chung and Jang2024). These positive caregiving experiences may help buffer the emotional impact of perceived relationship loss and may be associated with lower levels of anticipatory grief among some caregivers.
Together, these findings position anticipatory grief as emerging from the intersection of caregiving-related stress exposure and adaptive capacity. Resilience has been conceptualized as a dynamic process of adaptation shaped by the caregiving context and closely linked to caregiver mental health (Poe et al. Reference Poe, Vance and Patrician2023). Prior work indicates that resilience factors (e.g., adaptive coping, self-efficacy, optimism, and social support) are associated with better health outcomes, lower psychological distress, and a stronger relationship between the caregiver and the person living with ADRD (Martyr et al. Reference Martyr, Rusted, Quinn, Gamble, Collins, Morris and Clare2023). Resilience factors, such as coping, have also been shown to mediate the relationship between caregiving burden and well-being (Dias et al. Reference Dias, Santos and Sousa2015; Clement-Carbonell et al. Reference Clement-Carbonell, Alcocer-Bruno and Ruiz-Robledillo2025). Within this context, resilience-related resources may shape how caregivers respond to relationship losses and caregiving stressors, potentially contributing to variability in anticipatory grief experiences.
Although social support is a well-established resilience factor, evidence regarding its associations with anticipatory grief in the present study was mixed (Dias et al. Reference Dias, Santos and Sousa2015; McKenna et al. Reference McKenna, Fakolade and Cardwell2022). The influence of social support on caregivers’ mental health may depend less on its presence and more on the type of support (e.g., emotional, informational, instrumental), adequacy, and quality (Liang et al. Reference Liang, Aranda and Jang2022; Zanjari et al. Reference Zanjari, Momtaz and Kamal2022; Acoba Reference Acoba2024). Prior research suggests that different forms of support may influence caregiver well-being differently. For example, instrumental support (i.e., help with a specific problem) was associated with lower daily odds of depressive symptoms, whereas emotional support was associated with higher daily odds of anxiety symptoms among ADRD caregivers (Puga et al. Reference Puga, Wang and Rafford2023). These findings underscore the need for more nuanced assessments of social support within anticipatory grief research.
Notably, most caregiving stress research has primarily examined caregiving burden and depression as key indicators of caregiver mental health (Koyama et al. Reference Koyama, Matsushita and Hashimoto2017; Tian et al. Reference Tian, Xiong and Wang2022; Zhu et al. Reference Zhu, Xing and Jia2024). The findings of this review underscore the importance of considering anticipatory grief as a distinct dimension of caregiver mental health. Across the studies included in this review, anticipatory grief was associated with poorer mental health, appeared to persist across the ADRD trajectory, and was consistently linked to higher depressive symptoms. This is consistent with prior literature suggesting that grief and depression are closely related but conceptually distinct, and that depressive symptoms can obscure the unique contribution of grief-related processes to caregiver mental health (Ying et al. Reference Ying, Yap and Gandhi2018; Sánchez-Alcón et al. Reference Sánchez-Alcón, Sánchez-Ramos and Garrido-Fernández2023; Buur et al. Reference Buur, Zachariae and Komischke-Konnerup2024).
Although anticipatory grief shares some conceptual overlap with caregiving burden, particularly in domains reflecting emotional strain and role demands (Chan et al. Reference Chan, Yap, Wee and Liew2020; Dehpour and Koffman Reference Dehpour and Koffman2023), several studies in this review reported that anticipatory grief remained associated with depressive symptoms even after accounting for caregiver burden. These findings suggest that anticipatory grief captures relationship and emotional aspects of the caregiving experience that may not be fully reflected by traditional measures of burden. Recognizing anticipatory grief as a distinct dimension of caregiver psychological distress may help inform more targeted approaches to supporting caregiver mental health.
While most interventions designed to improve caregiver mental health have primarily focused on depression and caregiving burden (Dessy et al. Reference Dessy, Zhao and Kyaw2022; Sun et al. Reference Sun, Ji and Leng2022; Widiyaningsih et al. Reference Widiyaningsih, Susanto and Chiu2025), relatively few have specifically addressed anticipatory grief. Some of the interventions included in this review did not identify anticipatory grief as a primary outcome, highlighting a gap in current intervention design. This gap suggests that anticipatory grief may represent an under-addressed dimension of caregiver well-being within existing intervention frameworks. To more effectively address anticipatory grief, future interventions should examine mechanisms such as acceptance, preparedness for the future, recognition, and validation of grief-related responses. Interventions that acknowledge ongoing relationship losses and normalize caregivers’ emotional responses may be particularly relevant in dementia caregiving contexts. Beyond risk-mitigating approaches, this review underscores the need for resilience-focused intervention frameworks. Incorporating psychosocial factors, such as self-efficacy, perceived gains, mastery, cultural beliefs, and family functioning, may further enhance caregivers’ adaptive capacity across the ADRD trajectory (Poe et al. Reference Poe, Vance and Patrician2023; Clement-Carbonell et al. Reference Clement-Carbonell, Alcocer-Bruno and Ruiz-Robledillo2025).
Limitations
This review is not without limitations. First, selection bias is possible as included studies were restricted to English-language publications from selected databases. Second, consistent with scoping review methodology, study quality and risk of bias were not assessed, limiting conclusions about evidence strength. Third, small sample sizes and limited racial/ethnic diversity across studies limit the ability to capture cultural and other contextual factors influencing caregivers’ anticipatory grief. Fourth, the anticipatory grief literature is characterized by conceptual and measurement heterogeneity, including multiple definitions and assessment tools, which may limit comparability across studies. Finally, this review focused on anticipatory grief during the caregiving period and did not synthesize evidence on post-bereavement outcomes (e.g., grief after death), which is an important related area for future research.
Implications and future directions
The findings of this review have several implications for research and practice. Healthcare providers may benefit from assessing changes in the caregiver–care recipient relationship early in the ADRD trajectory to understand how relationship dynamics contribute to anticipatory grief and caregiver well-being. Integrating anticipatory grief into caregiver assessments may help clinicians capture caregivers’ emotional experiences beyond traditional indicators of burden or depression. Future research would benefit from longitudinal designs to capture within-person fluctuations in anticipatory grief and identify contextual or psychosocial factors that exacerbate or buffer it over time. There is also a need for multicomponent interventions that explicitly target resilience-related processes associated with anticipatory grief. Finally, research with racial and ethnically diverse caregivers is essential for understanding how cultural contexts influence anticipatory grief and adaptation.
Conclusion
This scoping review synthesized evidence on anticipatory grief among caregivers of people living with ADRD. Relationship changes across the dementia trajectory and caregiving-related stressors, particularly BPSD management, were consistently associated with higher levels of anticipatory grief, whereas psychosocial resources such as adaptive coping and social support were linked to lower levels. Anticipatory grief was also consistently associated with depressive symptoms. These findings suggest that anticipatory grief represents an important dimension of the caregiving experience that warrants greater attention in research and clinical practice. Further research is needed to better understand how cultural factors can influence the anticipatory grief experiences among racially and ethnically diverse caregivers.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951526102478.
Funding
NARC’s training is supported by the National Institute on Aging (R01AG072569-PI: Puga). The authors alone are responsible for the content, which does not represent the official views of the National Institutes of Health.
Competing interests
None.





 Open access
Open access