


Introduction
Sexual (SM) and gender (GM) minoritised people (SGM; i.e. lesbian, gay, bisexual, transgender, queer, and people who identify with other minoritised sexual orientations and gender identities) experience higher rates of mental health difficulties and suicidal and non-suicidal self-injurious behaviours than cisgender and heterosexual people (Camp et al., Reference Camp, Kashirsky, Pinckard, Hambleton, Oliver, Smith, Badrick, Bhopal, Baudinet and Absoud2026; Dürrbaum and Sattler, Reference Dürrbaum and Sattler2020; Hainey et al., Reference Hainey, Connolly, Thomson, Smalley, Campbell, Wells and Katikireddi2025; Liu et al., Reference Liu, Sheehan, Walsh, Sanzari, Cheek and Hernandez2019; Marchi et al., Reference Marchi, Arcolin, Fiore, Travascio, Uberti, Amaddeo and Galeazzi2022; Wittgens et al., Reference Wittgens, Fischer, Buspavanich, Theobald, Schweizer and Trautmann2022). They also report elevated levels of emotion dysregulation (Camp et al., Reference Camp, Blundell, Smith and Rimes2025). Minority-stress frameworks posit that these disparities arise from chronic, minority-related stressors layered onto general life stressors, alongside disproportionate exposure to adverse childhood experiences (Brooks, Reference Brooks1981; Frost and Meyer, Reference Frost and Meyer2023; Hendricks and Testa, Reference Hendricks and Testa2012; Meyer, Reference Meyer2003; Pachankis and Clark, Reference Pachankis and Clark2025; Roberts et al., Reference Roberts, Austin, Corliss, Vandermorris and Koenen2010). Thus, while minority-stress frameworks provide a shared theoretical foundation, SGM groups experience distinct and intersecting stressors related to sexual orientation and gender identity, as well as within-group variation, supporting the need to examine these populations separately in mental health research (Frost and Meyer, Reference Frost and Meyer2023; Hendricks and Testa, Reference Hendricks and Testa2012).
Given these disparities and the demands of navigating cis-heteronormative contexts, SGM people may have a heightened need for effective, affirming interventions – and may require adaptations that address minority- and group-specific mechanisms (i.e. factors not likely to be experienced by cisgender and heterosexual people, like identity concealment and internalisation of stigma; Burger and Pachankis, Reference Burger and Pachankis2024; Pachankis, Reference Pachankis2018). Yet, the extent to which standard evidence-based treatments generalise to SGM populations remains unclear because studies frequently do not ascertain or report sexual orientation and gender identity (Heck et al., Reference Heck, Mirabito, LeMaire, Livingston and Flentje2017). Consistent with this, a recent scoping review of suicide prevention interventions for SGM people identified few tailored suicide-specific interventions and highlighted limitations in the strength and consistency of the evidence base, with most studies demonstrating feasibility and/or acceptability rather than robust effectiveness data. Dialectical behaviour therapy (DBT) was the only established suicide-specific intervention examined (Chang et al., Reference Chang, Livingston, Rashkovsky, Harper, Kuehn, Khalifian, Harned, Tucker and Depp2025).
Evidence from adjacent intervention literature suggests that sexual orientation and gender identity reporting is uncommon. In a systematic review of acceptance and commitment therapy (ACT) trials, 3% (2 of 75) reported gender identity beyond men and women and 7% (5 of 75) reported sexual orientation (Misra et al., Reference Misra, Bryan, Faber, Printz Pereira, Faber, Williams and Skinta2023). Notably, among the studies that assessed gender identity, one reported that 100% of participants were ‘cisgender’, while the other reported that 2% of the sample identified as nonbinary but did not assess or report transgender or cisgender status within the men and women categories. A review of randomised controlled trials (RCTs) for anxiety and depression found 0.43% (1 of 232) reported sexual orientation and 0% reported gender identity (Heck et al., Reference Heck, Mirabito, LeMaire, Livingston and Flentje2017). In substance use intervention research, 2.30–6.50% of studies reported sexual orientation data and 0–2.30% reported gender identity (Flentje et al., Reference Flentje, Bacca and Cochran2015). Consequently, it is often impossible to determine whether SGM participants were included in efficacy/effectiveness trials, in what proportion, or whether outcomes are comparable to those of cisgender, heterosexual participants.
Where sexual orientation and gender identity data are reported, estimates of SGM representation vary. In ACT trials, 21% of participants across relevant samples were from SM groups (Misra et al., Reference Misra, Bryan, Faber, Printz Pereira, Faber, Williams and Skinta2023). In routine out-patient services for anxiety and depression in the UK, SM participant representation was 7.20% in a national cohort (Rimes et al., Reference Rimes, Ion, Wingrove and Carter2019) and 7.39% in a London cohort (Kent et al., Reference Kent, Suh, Lewis, Saunders, Davies, Lewis and Buckman2025), with similar rates in US campus mental health services (Dunbar et al., Reference Dunbar, Sontag-Padilla, Ramchand, Seelam and Stein2017). High-intensity settings (e.g. in-patient, day-patient, and residential) often show greater representation – 11–20% where data exists (Beard et al., Reference Beard, Kirakosian, Silverman, Winer, Wadsworth and Björgvinsson2017; Bezahler et al., Reference Bezahler, Kuckertz, Schreck, Narine, Dattolico and Falkenstein2022; Donahue et al., Reference Donahue, DeBenedetto, Wierenga, Kaye and Brown2020; Plöderl et al., Reference Plöderl, Kunrath, Cramer, Wang, Hauer and Fartacek2017; Plöderl et al., Reference Plöderl, Mestel and Fartacek2022). These figures exceed UK (3.30%; Office for National Statistics, 2023) and US (5.50%; Flores and Conron, Reference Flores and Conron2023) population estimates of SM people and may reflect elevated need amid health inequalities. At the same time, several studies document under-utilisation relative to need, citing barriers to access and negative experiences of care (Compton and Morgan, Reference Compton and Morgan2022; Dunbar et al., Reference Dunbar, Sontag-Padilla, Ramchand, Seelam and Stein2017; Ellis et al., Reference Ellis, Bailey and McNeil2015; Foy et al., Reference Foy, Morris, Fernandes and Rimes2019; McDermott, Reference McDermott2014; McDermott et al., Reference McDermott, Hughes and Rawlings2018; Williams and Chapman, Reference Williams and Chapman2011; Williams and Chapman, Reference Williams and Chapman2015).
Notably, GM participant representation data in psychological intervention research remain scarce. One study reported on the representation of GM participants (3.27%; Donahue et al., Reference Donahue, DeBenedetto, Wierenga, Kaye and Brown2020). This study was conducted within a day hospital eating disorder programme and included transgender and nonbinary identity categories; however, it is not clear that cisgender status was assessed within binary gender groups, potentially limiting precision in estimating representation. Consistent with this, a systematic review of ACT trials found that one study reported all participants as cisgender, while another reported that 2% of participants were nonbinary but did not assess transgender status within binary categories; these data were not aggregated due to inconsistencies in reporting and the small number of studies assessing gender identity (Misra et al., Reference Misra, Bryan, Faber, Printz Pereira, Faber, Williams and Skinta2023). Together, these mixed estimates and frequent non-reporting illustrate potential invalidation by omission, constraining appraisal of representation and outcomes for SGM people.
Even when SGM participants are included in evaluations of psychological therapies, studies rarely test whether effectiveness and acceptability/feasibility (e.g. completion and attrition) are equivalent across groups. Many analyses are secondary, relying on routinely collected service outcomes without pre-specified subgroup tests, which often limits power and interpretability. Where examined, findings are mixed: some studies report lower improvement or higher end-of-treatment severity among SM compared with heterosexual participants (Donahue et al., Reference Donahue, DeBenedetto, Wierenga, Kaye and Brown2020; Plöderl et al., Reference Plöderl, Mestel and Fartacek2022). Others find overall parity, but disparities for specific subgroups (e.g. bisexual participants) relative to heterosexual, and sometimes gay/lesbian, participants (Beard et al., Reference Beard, Kirakosian, Silverman, Winer, Wadsworth and Björgvinsson2017; Rimes et al., Reference Rimes, Ion, Wingrove and Carter2019). Others report no group differences or, in some instances, better outcomes for SM groups (Bezahler et al., Reference Bezahler, Kuckertz, Schreck, Narine, Dattolico and Falkenstein2022; Kent et al., Reference Kent, Suh, Lewis, Saunders, Davies, Lewis and Buckman2025; Plöderl et al., Reference Plöderl, Kunrath, Cramer, Wang, Hauer and Fartacek2017). Therefore, these inconsistencies – compounded by frequent non-reporting – underscore the need for systematic, adequately powered subgroup analyses and standardised sexual orientation and gender identity measurement to detect or rule out inequalities.
DBT is a cognitive-behavioural intervention with demonstrated effectiveness in reducing mental health difficulties, self-harm, suicidality, and emotion dysregulation in adult and adolescent populations (DeCou et al., Reference DeCou, Comtois and Landes2019; Kothgassner et al., Reference Kothgassner, Goreis, Robinson, Huscsava, Schmahl and Plener2021; Panos et al., Reference Panos, Jackson, Hasan and Panos2014). Dialectical behaviour therapy for adolescents (DBT-A) is a developmentally adapted version of DBT designed for adolescents and their families, typically aged 12–18 years, which retains the core treatment functions and modes while incorporating increased family involvement, developmental considerations, and age-appropriate adaptations to materials and principles (Miller et al., Reference Miller, Rathus and Linehan2007; Rathus and Miller, Reference Rathus and Miller2015).
Emerging evidence indicates that DBT trials and clinics often include a high proportion of SGM clients (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Harned et al., Reference Harned, Coyle and Garcia2022) – higher than would be expected from general population estimates and elevated risk for self-harm and related difficulties in comparison with cisgender and heterosexual people in community and clinical samples (e.g. Liu et al., Reference Liu, Sheehan, Walsh, Sanzari, Cheek and Hernandez2019). For example, a review of US-based DBT RCTs estimated that 27.30% of the pooled sample identified as SM (Harned et al., Reference Harned, Coyle and Garcia2022). Representation of GM was not calculated as insufficient studies recorded gender identity in a way that allowed for the identification of transgender and gender diverse people compared with cisgender people (Harned et al., Reference Harned, Coyle and Garcia2022). Clinic data from a national adolescent DBT service in the UK reported that the percentage of their clients over five years was 65.25% SM and 16.77% GM (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). At the same time, sexual orientation and gender identity reporting within the DBT literature may be higher than adjacent literature: in the US-based DBT RCT review, 50% (9 of 18) of trials reported sexual orientation and 11% (2 of 18) reported minoritised gender identities, but outcome equity by SGM status was not evaluated (Harned et al., Reference Harned, Coyle and Garcia2022).
Despite evidence that DBT is relevant to SGM-salient targets/mechanisms (e.g. emotion dysregulation, self-harm) and indications of high SGM representation, the DBT literature often does not (a) report sexual orientation or gender identity with sufficient detail to identify minorities, (b) test whether DBT is effective for SGM groups specifically, and (c) examine whether outcomes are comparable between SGM and cisgender and heterosexual participants, including acceptability and feasibility outcomes. Prior work (e.g. Harned et al., Reference Harned, Coyle and Garcia2022) was restricted to US-based RCTs and did not evaluate outcome equity by sexual orientation and gender identity. By contrast, the present review aims to include international and broader study designs, enabling a broader account of sexual orientation and gender identity reporting, representation, and outcomes in the DBT literature.
To capture DBT applications across developmental contexts, both adult and adolescent DBT studies were included in the present review for conceptual, clinical, and methodological reasons. First, DBT targets transdiagnostic mechanisms highly relevant to SGM mental health across the lifespan, including emotion dysregulation, self-harm, and suicidality (Camp et al., Reference Camp, Blundell, Smith and Rimes2025; Liu et al., Reference Liu, Sheehan, Walsh, Sanzari, Cheek and Hernandez2019). Second, adolescence represents a critical developmental period for sexual orientation and gender identity development, during which minority stress exposure often intensifies, while adulthood reflects longer-term accumulation of these stressors (Rosario et al., Reference Rosario, Schrimshaw, Hunter and Braun2006). Including both age groups therefore allows examination of SGM representation, outcomes, and feasibility across key developmental contexts rather than restricting conclusions to a single life stage.
Therefore, this systematic review and meta-analysis aims to (1) quantify how often DBT studies record sexual orientation and gender identity – and whether reporting is sufficiently detailed to identify minoritised groups; (2) estimate the proportion of SGM participants in DBT samples to inform access and representations; and (3) synthesise effectiveness and acceptability/feasibility outcomes for SGM participants and compare them with cisgender-heterosexual participants where possible. The research questions are:
-
(1) What proportion of DBT studies record sexual orientation and gender identity, and is reporting sufficient to identify which SGM groups are represented?
-
(2) What proportion of participants in DBT studies report a minoritised sexual or gender identity (i.e. representation in samples)?
-
(3) Among SGM participants, what is the magnitude of improvement on effectiveness outcomes (e.g. symptoms/functioning) and what are their acceptability/feasibility outcomes (e.g. treatment completion and phase-specific attrition)?
-
(4) Do SGM and cisgender, heterosexual participants differ in effectiveness (pre–post change or post-treatment outcomes) and/or in acceptability/feasibility (overall completion and pre- vs during-treatment attrition)?
Method
Search strategy
A systematic search of the literature was conducted on OvidSP in December 2024 using Embase (1974 to present), Ovid MEDLINE® ALL (1946 to present), Global Health (1973 to present), APA PsycArticles, APA PsycInfo (1806 to present), and APA PsycTherapy. To maximise specificity to comprehensive DBT studies, the intervention search terms (‘dialectical behav* therapy’ OR DBT).ti,kw. were applied to title and keyword fields. Boolean operators were used to combine terms. A limit was applied to English-language publications. The protocol was pre-registered on PROSPERO (ref: CRD42025609288).
Selection criteria
Inclusion criteria
Studies were included if they evaluated the effectiveness of comprehensive DBT based largely on the original adult (Linehan, Reference Linehan1993; Linehan, Reference Linehan2025) or adolescent (Rathus and Miller, Reference Rathus and Miller2015; Miller et al., Reference Miller, Rathus and Linehan2007) models. Comprehensive DBT was defined as delivery of the four core modes: (a) individual therapy, (b) skills training group, (c) between-session telephone coaching, and (d) consultation team. In DBT-A studies, the skills training component could include those that use the multi-family skills group format or separate skills training for adolescents. This review focused exclusively on comprehensive DBT, rather than DBT-informed, skills-training only, or similar interventions. This decision was made to maximise internal validity and interpretability of findings, as DBT-informed and partial DBT interventions vary widely in structure, dose, and treatment components, limiting meaningful comparison across studies (Valentine et al., Reference Valentine, Smith and Stewart2020). Comprehensive DBT represents the most standardised and theoretically coherent implementation of the model, allowing clearer evaluation of outcomes across populations. Studies of DBT plus DBT-prolonged exposure (DBT-PE) were included because the four modes are retained.
Eligible designs included RCTs and controlled or uncontrolled effectiveness studies, or similar, with n = ≥2 and quantitative outcomes comprising at least one of (a) effectiveness indicators (e.g. symptoms, functioning) over time or comparison between groups, and/or (b) acceptability/feasibility indicators (e.g. treatment completion or non-completion).
Exclusion criteria
We excluded studies that (a) did not include, or clearly document, all four DBT modes; (b) substantially adapted the intervention structure such that it deviated from the original models (e.g. adaptations for in-patient or day services, hybrids of DBT with other programmes, removal of modes altogether, etc.); (c) lacked quantitative data; or (d) were opinion/theoretical papers, qualitative-only reports, protocols, or single-case reports. Studies were also excluded if they were not written in English.
Selection process
Search results were de-duplicated and then imported into EndNote for screening. Titles and abstracts were screened by the second author; a 30% random subset was independently double-screened by the first author (blind to one another’s ratings). Articles deemed potentially eligible were retrieved and screened against the inclusion/exclusion criteria by the second and third authors, both blind to one another’s ratings. Discrepancies in inclusion and exclusion at this stage were resolved through discussions between authors.
Data extraction
For studies meeting inclusion criteria, study methodology and sample characteristics were extracted. For studies that included sexual orientation or gender identity data, we additionally extracted details of their data collection along with effectiveness and acceptability/feasibility outcomes, measurement instruments, and assessment timepoints. We extracted effect sizes and statistical significance where available. If effect sizes were not reported but appropriate descriptive statistics were reported, we calculated effect sizes for the study.
Data were entered into a spreadsheet by the second author and an independent research assistant, and this extraction was checked for accuracy by the first author. Where published reports indicated sexual orientation and gender identity were collected but insufficient detail was provided or outcome data required disaggregation (e.g. completion by sexual orientation or gender identity subgroup), corresponding authors were contacted to request additional information relevant to this review. Corresponding authors of all publications reporting SGM participant data (k = 38) were contacted, of whom four provided additional data.
Quality assessment
Methodological quality was appraised using the Effective Public Health Practice Project (EPHPP) Quality Assessment Tool (Armijo-Olivo et al., Reference Armijo-Olivo, Stiles, Hagen, Biondo and Cummings2012; Thomas et al., Reference Thomas, Ciliska, Dobbins and Micucci2004). The EPHPP includes eight domains: study design, selection bias, control of confounders, blinding, data collection methods, withdrawals/drop-outs, intervention integrity, and analyses. Each domain is rated as strong, moderate, or weak. Following the tool’s rules, a global rating is assigned as strong (1) if no domain is rated weak, moderate (2) if exactly one domain is rated weak, and weak (3) if two or more domains are rated weak. Ratings were completed by the first author and the third author, and consensus ratings are reported.
Data synthesis
Most data were synthesised narratively, structured by the research questions and by sexual orientation and gender identity groups. Studies using overlapping datasets were kept separate for the results regarding how many studies collected and reported on sexual orientation and gender identity data. For the remaining questions, studies using overlapping datasets were collapsed so participants were not double counted. The study used to represent any overlapping dataset was chosen based on having the largest and/or latest sample, in consultation with the authors. The first and second authors independently drafted narrative summaries using the extraction spreadsheet and cross-checked each other’s sections to ensure completeness and consistency.
Where ≥2 studies reported comparable outcomes, we conducted meta-analyses in line with recommendations by the Cochrane Handbook (Higgins et al., Reference Higgins, Thomas, Chandler, Cumpston, Li, Page and Welch2024). Continuous outcomes were synthesised as standardised mean differences (Hedges’ g, small-sample corrected). Binary outcomes (acceptability/feasibility) were analysed as risk ratios (RRs) for overall completion (vs non-completion) where reported. Where studies reported multiple assessment time points, outcomes were extracted at baseline and at the end of the intervention to maximise comparability across studies.
All meta-analyses used random-effects models with restricted maximum likelihood (REML) as the primary τ 2 estimator. We reported pooled effects with 95% confidence intervals, between-study heterogeneity (τ, τ 2, I 2), and 95% prediction intervals. In one study reporting multiple SGM subgroups (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024), aggregated group-level data (i.e. means and standard deviations for SM vs heterosexual participants) were obtained from the authors to derive a single independent effect size; all other studies reported aggregated comparisons. This was done to avoid non-independence of effect sizes and to maximise inclusion in the meta-analyses.
Analyses were conducted in Stata using meta esize to compute effect sizes from study-level data and meta summarise, random reml for pooling (StataCorp, 2023).
Artificial intelligence (AI) tools were used to check formatting of the text and the reference list.
Results
Study selection
Study selection is summarised in Fig. 1. One hundred and seventy studies were identified as meeting the inclusion criteria for this review. Of the 38 studies that included data on sexual orientation or gender identity, 14 studies utilised one of four overlapping datasets (Camp et al., Reference Camp, Hunt and Smith2023a overlaps with Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Cook, Reference Cook2022; Nardone et al., Reference Nardone, Pascual-Leone, Kramer, Cristoffanini, Grandjean, Culina and McMain2024; Ip et al., Reference Ip, McMain, Chapman and Kuo2024 overlaps with Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024; King, Reference King2018; King et al., Reference King, Rizvi and Selby2019; Rizvi and Fitzpatrick, Reference Rizvi and Fitzpatrick2021; Weatherford et al., Reference Weatherford, Ruork, Yin, Lopez and Rizvi2024; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 overlaps with Yin et al., Reference Yin, Selby and Rizvi2022; and Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021 overlaps with Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023). Thus, we largely report on study characteristics and outcomes of interest for 28 studies with unique datasets (24 unique studies/datasets and 4 studies representing one of each of the four overlapping datasets). There were eight studies that did not report on sexual orientation and gender identity in their original publications, but these data were retrieved from the authors and reported in another review (Harned et al., Reference Harned, Coyle and Garcia2022), therefore these studies were included in this review.
PRISMA flow diagram. This figure depicts the identification of studies and inclusion/exclusion at various stages of screening. *Other reasons for exclusion (k = 13): non-English language; not a DBT study; wrong population/focus (parent pre-treatment expectations); qualitative design (ineligible per protocol); non-empirical publication type (book chapter or narrative/opinion); correction/erratum.

Figure 1. Long description
The flowchart depicts the identification of studies and inclusion/exclusion at various stages of screening. The process begins with the identification of records from databases and a specific study, totaling 2699 records. After removing 54 duplicate records, 2645 records are screened. Out of these, 2310 records are excluded, leaving 336 reports sought for retrieval. One report is not retrieved, resulting in 335 reports assessed for eligibility. Reports are excluded for various reasons, including not being comprehensive, not being out-patient, not being standard DBT, no data, and other reasons. Initially, 170 studies are included in the review. Further filtering includes studies with data on LGBTQ+ participants, resulting in 38 studies, and studies with unique datasets, resulting in 28 studies.
Study characteristics
Methodological characteristics and study location
Methodological characteristics are summarised in Table 1. Methodologies among the 28 unique studies were: cohort (one-group pre-test-post-test; 28.57%); RCTs (35.71%); case series (7.14%); cohort analytic (two group comparisons; 7.14%); case–control (two-group; 3.57%); controlled clinical trial (3.57%); cross-sectional survey (3.57%); interrupted time series (3.57%); a secondary cohort-analytic study of DBT outcomes using pooled data from multiple clinical trials (3.57%) and a pilot sequential multiple assignment randomized trial (SMART) trial (3.57%). Sampling methods across the included studies were convenience sampling. Recruitment typically occurred via routine clinical intake at DBT clinics and university training clinics; referrals from public hospitals, in-patient and partial hospitalisation programs, community mental health services, veteran association clinics, case management agencies, schools, and child protective services; and program databases/archived lists. Of the 28 independent studies, 82.00% were conducted in North America (US and Canada), 4.50% in the United Kingdom, 4.50% in Australia, 4.50% in Germany, and 4.50% in the Netherlands.
Included study characteristics

Table 1. Long description
The table summarizes the methodological characteristics of 28 unique studies. It has 28 rows and 10 columns. The columns are labeled as follows: Study, Country, Study Design, Sample Size, Age Range, Intervention, Comparator, Outcomes, Follow-up, and Notes. The table includes various study types such as cohort, RCTs, case series, cohort analytic, case-control, controlled clinical trial, cross-sectional survey, interrupted time series, secondary cohort-analytic study, and pilot sequential multiple assignment randomized trial (SMART). Sampling methods across the included studies were convenience sampling. Recruitment typically occurred via routine clinical intake at DBT clinics and university training clinics; referrals from public hospitals, in-patient and partial hospitalization programs, community mental health services, veteran association clinics, case management agencies, schools, and child protective services; and program databases/archived lists. Of the 28 independent studies, 82.00% were conducted in North America (US and Canada), 4.50% in the United Kingdom, 4.50% in Australia, 4.50% in Germany, and 4.50% in the Netherlands.
a Camp et al., Reference Camp, Hunt and Smith2023a and Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 use overlapping samples;
b Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023 includes data from Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021, therefore samples overlap;
c these studies use the same participant cohort as the McMain et al. (Reference McMain, Chapman, Kuo, Guimond, Streiner, Dixon-Gordon and Hoch2018) RCT, drawing on either the full sample or a subset – so the samples overlap across these studies;
d these studies use the same participant cohort as Yin et al. (Reference Yin, Selby and Rizvi2022), drawing on either the full sample or a subset – so the samples overlap across studies.
ACES (DBT-ACES), Accepting the Challenges of Employment and Self-Sufficiency; AIDS, Acquired Immune Deficiency Syndrome; CAMS, Collaborative Assessment and Management of Suicidality; CTE, Community Treatment by Experts; DBT, Dialectical Behaviour Therapy; DBT-A, Dialectical Behaviour Therapy for Adolescent; DBT-PE, Dialectical Behaviour Therapy Prolonged Exposure; DBT-S/DBT-ST, Dialectical Behaviour Therapy Skills Training; HIV, Human Immunodeficiency Virus; LGBQ, Lesbian, Gay, Bisexual, Queer/Questioning; LGBT, Lesbian, Gay, Bisexual, Transgender; M, Mean; N, sample size; NA, not applicable; NR, not reported; PE, Prolonged Exposure; RCT, Randomised Controlled Trial; SD, standard deviation; TAU, Treatment as Usual; UPMC, University of Pittsburgh Medical Center; USA, United States of America; UK, United Kingdom; VA, Department of Veterans Affairs.
Sample characteristics
Sample characteristics are summarised in Table 1. Across the 28 independent studies, the total sample included 2268 participants, with a mean age of 27.02 (SD = 8.54). Among the 12 studies that recorded sex assigned at birth (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Frazer, Reference Frazer2021; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; Goldstein et al., Reference Goldstein, Fersch-Podrat, Rivera, Axelson, Merranko, Yu and Birmaher2015; Goodman et al., Reference Goodman, Banthin, Blair, Mascitelli, Wilsnack, Chen and New2016; Harned et al., Reference Harned, Korslund and Linehan2014; Koons et al., Reference Koons, Robins, Tweed, Lynch, Gonzalez, Morse and Bastian2001; Linehan et al., Reference Linehan, Dimeff, Reynolds, Comtois, Welch, Heagerty and Kivlahan2002; Linehan et al., Reference Linehan, Comtois, Murray, Brown, Gallop, Heard and Lindenboim2006b; Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; Linehan et al., Reference Linehan, Armstrong, Suarez, Allmon and Heard1991; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012), 77.90% were assigned female (n = 504) and 22.10% male (n = 143). However, seven of these studies (Harned et al., Reference Harned, Korslund and Linehan2014; Koons et al., Reference Koons, Robins, Tweed, Lynch, Gonzalez, Morse and Bastian2001; Linehan et al., Reference Linehan, Dimeff, Reynolds, Comtois, Welch, Heagerty and Kivlahan2002; Linehan et al., Reference Linehan, Comtois, Murray, Brown, Gallop, Heard and Lindenboim2006b; Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; Linehan et al., Reference Linehan, Armstrong, Suarez, Allmon and Heard1991; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012) did not explicitly report the sex assigned at birth but instead used terms such as ’female’ to describe their sample and did not report gender explicitly. Thus, we assumed that the authors were referring to sex rather than gender, but this cannot be verified.
Using the broad classification of race as reported across studies, 26.58% belonged to minoritised racial groups (n = 550). Among the participants with more granular data in this domain (excluding ‘not reported/declined’; n = 195), 3.00% were Asian (n = 62), 6.09% were Black (n = 126), 6.67% were Hispanic (n = 138), 0.53% were indigenous (n = 11), 8.17% were mixed (n = 169), and 2.13% identified as other (n = 44).
Study methodological quality
Across the included studies, methodological quality varied (see Table 2). Seven studies were rated as strong, 10 as moderate, and 21 as weak. The most common methodological limitations related to confounder control, blinding, and withdrawals/attrition, which were frequently rated as weak. In contrast, data collection methods were largely strong across studies, and most employed moderate-to-strong study designs.
Study methodological quality ratings via the EPHPP Quality Assessment Tool (Armijo-Olivo et al., Reference Armijo-Olivo, Stiles, Hagen, Biondo and Cummings2012; Thomas et al., Reference Thomas, Ciliska, Dobbins and Micucci2004)

Consensus ratings reported in this table. EPHPP, the Effective Public Health Practice Project Quality Assessment Tool (Armijo-Olivo et al., Reference Armijo-Olivo, Stiles, Hagen, Biondo and Cummings2012; Thomas et al., Reference Thomas, Ciliska, Dobbins and Micucci2004).
Study results
Study Inclusion of SGM data
In this section, each study is treated as an individual unit of analysis, even where datasets overlap. Attention is drawn to instances of overlap, as the focus here is on whether studies recorded and reported sexual orientation and gender identity data. Of the 170 comprehensive DBT studies that met the inclusion criteria, 38 (22.35%) reported on the sexual orientation and/or gender identity of their sample (see Tables 3 and 4).
Representation of sexual minoritised and heterosexual participants in comprehensive DBT studies

Of the 463 participants identifying as a sexuality minoritised, 36 (7.78%) were not further disaggregated beyond ‘sexual minorities’ and thus are only present in the sexual minoritised aggregated column.
a Camp et al. (Reference Camp, Hunt and Smith2023a) was not used in the collapsed totals due to sample overlap with Camp et al. (Reference Camp, Durante, Cooper, Smith and Rimes2024) to avoid double-counting of participants.
b Harned et al. (Reference Harned, Schmidt, Korslund and Gallop2021) was not used in the collapsed totals due to sample overlap with Chang et al. (Reference Chang, Halvorson, Lehavot, Simpson and Harned2023) to avoid double-counting of participants.
c Pistorello et al. (Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012) did not disaggregate between lesbian, gay, bisexual or transgender and reported: ‘LGBT’ = 20 (31.75%) and this study is not included in the collapsed totals therefore. Dashes represent where data was not reported or not possible to obtain.
Representation of cisgender and transgender/gender diverse participants in DBT studies

Table 4. Long description
The table is divided into three sections: Studies that explicitly reported cisgender status, Studies that did not confirm cisgender status, and Studies that categorized gender as: man/boy, woman/girl, and ‘other’. Each section lists references, the number and percentage of participants identified as cisgender, transgender/gender diverse, cisgender female, cisgender male, non-binary, transgender women/girls and men/boys, unsure/questioning, and not reported. The table includes collapsed totals for each section. For example, in the first section, Camp et al., 2024 reported 93 (83.04%) cisgender participants and 19 (16.96%) transgender/gender diverse participants. The table provides a detailed breakdown of gender identity representation across various studies.
Where studies reported participants as ‘transgender’ and did not confirm whether these were transgender women/girls and men/boys or non-binary, they were counted in the ‘Transgender/gender diverse’ column only. Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012 did not disaggregate between lesbian, gay, bisexual or transgender and reported: ‘LGBT’ = 20 (31.75%) and this study is not included in this table.
a Camp et al., Reference Camp, Hunt and Smith2023a was not used in the collapsed totals in the relevant section due to sample overlap with Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 to avoid double-counting of participants.
b Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021 was not used in the collapsed totals in the relevant section due to sample overlap with Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023 to avoid double-counting of participants.
c Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 was not used in the collapsed totals in the relevant section due to sample overlap with Ip et al., Reference Ip, McMain, Chapman and Kuo2024 to avoid double-counting of participants.
d Cook, Reference Cook2022 and Nardone et al., Reference Nardone, Pascual-Leone, Kramer, Cristoffanini, Grandjean, Culina and McMain2024 were not used in the collapsed totals in the relevant section due to sample overlap with Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024 to avoid double-counting of participants.
e King, Reference King2018, King et al., Reference King, Rizvi and Selby2019, Rizvi and Fitzpatrick, Reference Rizvi and Fitzpatrick2021, and Weatherford et al., Reference Weatherford, Ruork, Yin, Lopez and Rizvi2024 were not used in the collapsed totals in the relevant section due to sample overlap with Yin et al., Reference Yin, Selby and Rizvi2022 to avoid double-counting of participants.
Dashes represent where data was not reported or not possible to obtain.
Sexual orientation recording
Nineteen (11.18%) studies reported sexual orientation (see Table 3; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Camp et al., Reference Camp, Hunt and Smith2023a; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Goldstein et al., Reference Goldstein, Fersch-Podrat, Rivera, Axelson, Merranko, Yu and Birmaher2015; Harned et al., Reference Harned, Korslund and Linehan2014; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; Koons et al., Reference Koons, Robins, Tweed, Lynch, Gonzalez, Morse and Bastian2001; Linehan et al., Reference Linehan, Armstrong, Suarez, Allmon and Heard1991; Linehan et al., Reference Linehan, Comtois, Murray, Brown, Gallop, Heard and Lindenboim2006b; Linehan et al., Reference Linehan, Dimeff, Reynolds, Comtois, Welch, Heagerty and Kivlahan2002; Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022; Ribeiro, Reference Ribeiro2016). When combining the overlapping datasets, 16 (9.41%) studies reported on sexual orientation (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Goldstein et al., Reference Goldstein, Fersch-Podrat, Rivera, Axelson, Merranko, Yu and Birmaher2015; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; Koons et al., Reference Koons, Robins, Tweed, Lynch, Gonzalez, Morse and Bastian2001; Linehan et al., Reference Linehan, Armstrong, Suarez, Allmon and Heard1991; Linehan et al., Reference Linehan, Comtois, Murray, Brown, Gallop, Heard and Lindenboim2006b; Linehan et al., Reference Linehan, Dimeff, Reynolds, Comtois, Welch, Heagerty and Kivlahan2002; Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022; Ribeiro, Reference Ribeiro2016). Additionally, one (0.58%) study recorded SM and GM as one group without disaggregation (i.e. ‘LGBT+’; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012).
Gender identity recording
Twenty-nine (17.06%) studies reported gender beyond man/boy and woman/girl (see Table 4; Assmann et al., Reference Assmann, Schaich, Arntz, Wagner, Herzog, Alvarez-Fischer and Fassbinder2024; Camp et al., Reference Camp, Hunt and Smith2023a; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Cook, Reference Cook2022; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; DeLong, Reference DeLong2018; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Frazer, Reference Frazer2021; Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023; Goodman et al., Reference Goodman, Banthin, Blair, Mascitelli, Wilsnack, Chen and New2016; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Hiller and Hughes, Reference Hiller and Hughes2023; Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024; Huntjens et al., Reference Huntjens, van den Bosch, Sizoo, Kerkhof, Smit and van der Gaag2024; Ip et al., Reference Ip, McMain, Chapman and Kuo2024; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; King, Reference King2018; King et al., Reference King, Rizvi and Selby2019; Landes et al., Reference Landes, Chalker and Comtois2016; Lu et al., Reference Lu, Dyce, Hughes, DeBono, Cometto and Boylan2020; Nardone et al., Reference Nardone, Pascual-Leone, Kramer, Cristoffanini, Grandjean, Culina and McMain2024; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Phalen et al., Reference Phalen, Grossmann, Bruder, Jeong, Calmes, McGrath and Bennett2022; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017; Rizvi and Fitzpatrick, Reference Rizvi and Fitzpatrick2021; Weatherford et al., Reference Weatherford, Ruork, Yin, Lopez and Rizvi2024; Yin et al., Reference Yin, Selby and Rizvi2022). When collapsing the overlapping datasets, 19 (11.88%) studies reported on gender beyond man/boy or woman/girl (Assmann et al., Reference Assmann, Schaich, Arntz, Wagner, Herzog, Alvarez-Fischer and Fassbinder2024; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; DeLong, Reference DeLong2018; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Frazer, Reference Frazer2021; Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023; Goodman et al., Reference Goodman, Banthin, Blair, Mascitelli, Wilsnack, Chen and New2016; Hiller and Hughes, Reference Hiller and Hughes2023; Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024, Huntjens et al., Reference Huntjens, van den Bosch, Sizoo, Kerkhof, Smit and van der Gaag2024; Ip et al., Reference Ip, McMain, Chapman and Kuo2024; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024, Landes et al., Reference Landes, Chalker and Comtois2016; Lu et al., Reference Lu, Dyce, Hughes, DeBono, Cometto and Boylan2020; Phalen et al., Reference Phalen, Grossmann, Bruder, Jeong, Calmes, McGrath and Bennett2022; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017, Yin et al., Reference Yin, Selby and Rizvi2022).
Out of these 29 studies, nine (31.03% of the 29; 5.29% of all studies: 9/170) studies recorded gender as ‘male, female, or other’ (Cook, Reference Cook2022; Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023; Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024; King, Reference King2018; King et al., Reference King, Rizvi and Selby2019; Nardone et al., Reference Nardone, Pascual-Leone, Kramer, Cristoffanini, Grandjean, Culina and McMain2024; Rizvi and Fitzpatrick, Reference Rizvi and Fitzpatrick2021; Weatherford et al., Reference Weatherford, Ruork, Yin, Lopez and Rizvi2024; Yin et al., Reference Yin, Selby and Rizvi2022). Once the overlapping datasets were collapsed, only three (1.88%) separate studies report on gender as ‘male, female, or other’ (Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023; Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024, Yin et al., Reference Yin, Selby and Rizvi2022).
Sixteen of the 29 studies (55.17% or 9.41% of the 170 studies) that included details on gender beyond man/boy and woman/girl included sufficient detail to identify GM participants as a distinct subgroup by recording more specific group labels for transgender and gender diverse participants (Assmann et al., Reference Assmann, Schaich, Arntz, Wagner, Herzog, Alvarez-Fischer and Fassbinder2024; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Camp et al., Reference Camp, Hunt and Smith2023a; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; DeLong, Reference DeLong2018; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Frazer, Reference Frazer2021; Goodman et al., Reference Goodman, Banthin, Blair, Mascitelli, Wilsnack, Chen and New2016; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Hiller and Hughes, Reference Hiller and Hughes2023; Huntjens et al., Reference Huntjens, van den Bosch, Sizoo, Kerkhof, Smit and van der Gaag2024; Ip et al., Reference Ip, McMain, Chapman and Kuo2024; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; Landes et al., Reference Landes, Chalker and Comtois2016; Lu et al., Reference Lu, Dyce, Hughes, DeBono, Cometto and Boylan2020; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Phalen et al., Reference Phalen, Grossmann, Bruder, Jeong, Calmes, McGrath and Bennett2022; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017). Four of these studies had overlapping datasets, thus 14 (8.23%) studies recorded gender identity in this way when overlapping datasets were collapsed (Assmann et al., Reference Assmann, Schaich, Arntz, Wagner, Herzog, Alvarez-Fischer and Fassbinder2024; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; DeLong, Reference DeLong2018; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Frazer, Reference Frazer2021; Hiller and Hughes, Reference Hiller and Hughes2023; Huntjens et al., Reference Huntjens, van den Bosch, Sizoo, Kerkhof, Smit and van der Gaag2024; Ip et al., Reference Ip, McMain, Chapman and Kuo2024; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; Lu et al., Reference Lu, Dyce, Hughes, DeBono, Cometto and Boylan2020; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Phalen et al., Reference Phalen, Grossmann, Bruder, Jeong, Calmes, McGrath and Bennett2022). Only three of these studies (1.77% of all studies; two with overlapping datasets: Camp et al., Reference Camp, Hunt and Smith2023a; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 and one without: Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; 1.25% when overlapping datasets are collapsed) explicitly reported on the participants as cisgender, whereas the remaining studies included groups labelled as or similar to man and woman, which may include transgender people within those groups.
Representation of SGM people in the studies
Sexual orientation representation
Excluding not reported/declined to answer, the pooled sample from the studies that recorded sexual orientation, once overlapping datasets were collapsed, included 64.33% identifying as heterosexual (n = 835) and 35.67% identifying as SM (n = 463; see Table 3; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Goldstein et al., Reference Goldstein, Fersch-Podrat, Rivera, Axelson, Merranko, Yu and Birmaher2015; Harned et al., Reference Harned, Korslund and Linehan2014; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024; Koons et al., Reference Koons, Robins, Tweed, Lynch, Gonzalez, Morse and Bastian2001; Linehan et al., Reference Linehan, Armstrong, Suarez, Allmon and Heard1991; Linehan et al., Reference Linehan, Comtois, Murray, Brown, Gallop, Heard and Lindenboim2006b; Linehan et al., Reference Linehan, Dimeff, Reynolds, Comtois, Welch, Heagerty and Kivlahan2002; Linehan et al., Reference Linehan, Korslund, Harned, Gallop, Lungu, Neacsiu and Murray-Gregory2015; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022; Ribeiro, Reference Ribeiro2016). Within the SM subgroups (where these were measured: N = 367), 25.61% were monosexual minorities (i.e. gay and lesbian, n = 94); 65.12% were plurisexual (i.e. bisexual and pansexual, n = 239); 6.00% were queer (n = 22); 1.91% were aro/ace spectrum (n = 7); 0.27% were questioning their sexual orientation (n = 1); and 1.09% were classified as ‘other’ (n = 4). One study (Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022) did not disaggregate SM but reported 41.03% of their sample as SM (n = 16). Additionally, one study (Pistorello et al., Reference Pistorello, Fruzzetti, MacLane, Gallop and Iverson2012) did not disaggregate SGM identities and reported only a combined category: ‘LGBT+’ (n = 20; 31.75% of their sample).
Gender identity representation
Only three studies (two studies when overlapping datasets were collapsed; Camp et al., Reference Camp, Hunt and Smith2023a; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024) explicitly identified participants as cisgender compared with GM, whereas the remaining studies included groups labelled as or similar to male and female without clarification whether these were exclusively cisgender or transgender. While it is not clear whether these groups contain GM participants, they are reported separately from the ‘transgender’ group in these studies and thus are of interest to highlight. For the two studies that did explicitly check cisgender status, 83.33% were cisgender (n = 150) and 16.67% were GM (n = 30; see Table 4; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Kassing et al., Reference Kassing, Seeley, Rizvi, Compton, Sinclair, Oshin and Pistorello2024). Within these studies, 12.71% (n = 23) were nonbinary transgender and 3.87% (n = 7) were transgender women/girls or men/boys.
For the 14 studies that recorded gender as ‘man/boy’, ‘woman/girl’, and ‘transgender/gender diverse’, or similar, once overlapping datasets were collapsed, 96.75% (n = 1369) were classified as men or women and 3.25% (n = 46) were transgender/gender diverse (Assmann et al., Reference Assmann, Schaich, Arntz, Wagner, Herzog, Alvarez-Fischer and Fassbinder2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Darrow et al., Reference Darrow, Maliken, Piatigorsky, Stuart, Todd, Yaeger and Londahl-Shaller2022; DeLong, Reference DeLong2018; Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Frazer, Reference Frazer2021; Goodman et al., Reference Goodman, Banthin, Blair, Mascitelli, Wilsnack, Chen and New2016; Hiller and Hughes, Reference Hiller and Hughes2023; Huntjens et al., Reference Huntjens, van den Bosch, Sizoo, Kerkhof, Smit and van der Gaag2024; Ip et al., Reference Ip, McMain, Chapman and Kuo2024; Landes et al., Reference Landes, Chalker and Comtois2016; Lu et al., Reference Lu, Dyce, Hughes, DeBono, Cometto and Boylan2020; Phalen et al., Reference Phalen, Grossmann, Bruder, Jeong, Calmes, McGrath and Bennett2022; Pistorello et al., Reference Pistorello, Jobes, Compton, Locey, Walloch, Gallop and Goswami2017). Where the transgender/gender diverse group was further disaggregated in these studies, 2.50% (n = 33) were nonbinary and 0.30% (n = 4) were transgender women/girls or men/boys.
In the three studies that classified gender as ‘man’, ‘woman’ and ‘other’ (or similar), once overlapping datasets were collapsed, 95.66% (n = 353) were men or women and 4.34% (n = 16) were classified as ‘other’ (Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023; Hood et al., Reference Hood, Maraun, McMain, Kuo and Chapman2024; Yin et al., Reference Yin, Selby and Rizvi2022).
Effectiveness outcomes
Effectiveness outcomes, alongside outcome measures, are summarised in Table 5. All studies measured emotion dysregulation using the Difficulties in Emotion Regulation Scale (DERS; Gratz and Roemer, Reference Gratz and Roemer2004).
Study effectiveness and acceptability/feasibility results by sexual orientation and gender identity

Table 5. Long description
A table summarizing effectiveness outcomes and outcome measures from studies on emotion dysregulation. The table has 10 rows and 10 columns. Column headers are Study, Did, N 1, N 2, N 3, N 4, N 5, N 6, N 7, N 8. Row 1: Did, 9; N 1, 28.221196; Bucket, bucket_2. Row 2: Did, 10; N 1, 28.221196; Bucket, bucket_2. Row 3: Did, 11; N 1, 28.221196; Bucket, bucket_2. Row 4: Did, 12; N 1, 28.221196; Bucket, bucket_2. Row 5: Did, 13; N 1, 28.221196; Bucket, bucket_2. Row 6: Did, 14; N 1, 28.221196; Bucket, bucket_2. Row 7: Did, 15; N 1, 28.221196; Bucket, bucket_2. Row 8: Did, 16; N 1, 28.221196; Bucket, bucket_2. Row 9: Did, 17; N 1, 28.221196; Bucket, bucket_2. Row 10: Did, 18; N 1, 28.221196; Bucket, bucket_2.
a The authors of these studies provided novel descriptive statistics on request: Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023, Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021, Hiller and Hughes Reference Hiller and Hughes2023;
b Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023: absolute mean differences are reported rather than standardized mean differences, as two of the three groups had N = 1, to allow for within-study group comparisons.
For studies that did not report effect sizes, these were computed from the available descriptive statistics, including some or all relevant outputs from Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023, Hiller and Hughes Reference Hiller and Hughes2023, and Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024. *p = < .05, **p = < .01, ***p = < .001. d, Cohen’s d (standardised mean difference; small = 0.20, medium = 0.50, large = 0.80); dₐv, Cohen’s d for repeated-measures designs (same benchmarks as d); r, Rosenthal’s r correlation coefficient (small = .10, medium = .30, large = .50); η2, eta squared (small = .01, medium = .06, large = .14); ns, non-significant (p ≥ .05). Δ, change in means/medians from Time 1 to Time 2. DBT, dialectical behaviour therapy; M, mean; SD, standard deviation; LGBQ+, lesbian, gay, bisexual, and queer; NSSI = non-suicidal self-injury; BPD, borderline personality disorder.
BPD symptoms
Across three studies (two DBT-A and one DBT), SM participants showed significant pre–post reductions with medium to large effects (Cohen’s d = 0.57–1.22; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). In the one DBT-A study that disaggregated SM subgroups, effects were large for both gay/lesbian (d = 1.22) and bisexual/pansexual (d = 0.98) participants (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). In the same study, heterosexual participants showed a medium pre–post effect (d = 0.78; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024).
Sexual orientation did not predict end-of-DBT BPD symptoms in one between-groups study (partial η2 < .01; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; DBT-A), whereas another reported higher BPD symptoms for SM participants than heterosexual participants at baseline and post-treatment (Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022; DBT-A). Another found no sexual-identity-by-time interaction (Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; DBT). The meta-analysis of pre–post change suggested a large pooled effect for SM samples (g = 0.98) with moderate between-study heterogeneity (see Fig. 2).
Borderline personality disorder symptoms forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in borderline personality disorder (BPD) symptoms for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 and Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022 are DBT for adolescent studies; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 is a DBT for adults study.

Across two DBT-A studies reporting disaggregated gender data, large pre–post reductions in BPD symptoms were observed across transgender, non-binary, and cisgender groups (d = 0.86–3.63; Δ = 0.32–1.48; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023). Gender identity did not predict post-treatment BPD symptoms after controlling for baseline severity in one study (partial η2 < .01; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Meta-analysis was not feasible due to heterogeneity in gender group definitions.
Emotion regulation
Across four studies, SM participants showed significant pre–post decreases in emotion dysregulation with large effects (d = 0.87–1.90; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022; two DBT-A and two DBT studies). In the one study that disaggregated SM subgroups, both bisexual/pansexual (d = 0.87) and gay/lesbian (d = 0.89) groups exhibited large reductions, compared with a medium reduction for the heterosexual group (d = 0.71; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; DBT-A). No study including SM data explored outcomes on the DERS subscales.
Across DBT-A studies, between-group analyses generally indicated no residual post-treatment differences by sexual orientation, with negligible-to-small effects when controlling for baseline emotion dysregulation (partial η2 < .01–.02; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). One DBT study identified a significant time × sexual orientation interaction, indicating slower rates of change among SM participants despite comparable baseline severity (ICC = .14; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024). Meta-analysis of pre–post change demonstrated a large pooled effect for SM samples (g = 1.11) with moderate heterogeneity (see Fig. 3).
Emotion regulation difficulties forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in emotion regulation for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 and Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022 are DBT for adolescent studies; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021 and Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 are DBT for adults studies.

Figure 3. Long description
The table presents a meta-analysis of studies examining pre and post changes in emotion regulation for sexual minoritised groups. It includes data from four studies: Camp et al., 2024; Harned et al., 2021; Oshin et al., 2024; Poon et al., 2022. The table has six columns: Study, Baseline N, Baseline Mean, Baseline SD, End of DBT N, End of DBT Mean, End of DBT SD, Hedges’s g with 95% CI, and Weight (%). Row 1: Camp et al., 2024; 61; 138.30; 18.06; 61; 109.35; 33.09; 1.08 [0.70, 1.46]; 49.93 percent. Row 2: Harned et al., 2021; 14; 62.36; 15.03; 9; 47.67; 21.03; 0.81 [-0.03, 1.65]; 10.10 percent. Row 3: Oshin et al., 2024; 35; 124.33; 18.17; 35; 103.17; 24.69; 0.97 [0.48, 1.46]; 29.66 percent. Row 4: Poon et al., 2022; 16; 122.35; 16.16; 16; 81.41; 23.52; 1.98 [1.15, 2.81]; 10.31 percent. The overall effect size is 1.11 [0.84, 1.38]. Heterogeneity statistics are provided: tau squared equals 0.00, I squared equals 0.00 percent, H squared equals 1.00. The Q test for homogeneity is 5.05 with a p-value of 0.17, and the z-test for the overall effect is 8.15 with a p-value of 0.00.
By gender identity, large pre–post reductions in emotion dysregulation were observed across two DBT-A studies, with effect sizes ranging from moderate to large across gender groups (d = 0.79–1.83; Δ = −0.25–0.83; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023). In DBT-A samples, gender identity did not predict post-treatment emotion dysregulation after controlling for baseline severity (partial η2 < .01; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Comparable patterns were observed across DERS subscales in the one study that reported subscale data (Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023; see Table 5). Meta-analysis was not feasible due to heterogeneity in gender identity group definitions.
Self-harm and suicidal behaviours
Across four DBT and DBT-A studies, SM participants showed pre–post reductions in self-injurious behaviours, with effects generally in the medium-to-large range (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024). Where suicidal and non-suicidal self-injury were aggregated, large reductions were observed for SM participants overall (r = .53), including bisexual/pansexual (r = .57) and gay/lesbian subgroups (r = .39), with similarly large reductions for heterosexual participants (r = .68), and no residual post-treatment differences after controlling for baseline self-injury (DBT-A; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). When examined separately, reductions in non-suicidal self-injury (NSSI) and suicide attempts were reported across sexual orientation groups, with effect sizes ranging from medium to large (d = 0.44–0.74), and no significant time × sexual orientation interactions (DBT; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024).
By gender identity, large reductions in self-injury were observed across gender groups in DBT-A studies (r = .57–.66 and d = −0.39 to −1.27), and no post-treatment differences after adjusting for baseline severity (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023). A small DBT-A case series reported variable patterns across individuals, with both the non-binary and cisgender participants showing improvements in some outcomes and minimal or no change in others, but no evidence of worsening suicidal ideation or NSSI (Frazer, Reference Frazer2021). Meta-analysis was not feasible due to small sample sizes and heterogeneity in reporting.
Depression symptoms
Across three DBT and DBT-A studies, SM participants showed medium-to-large pre–post reductions in depression (d = 0.56–1.05; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). Where examined, reductions were comparable across SM subgroups and heterosexual participants (DBT-A; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Between-group analyses were mixed: one DBT study identified a time × sexual identity interaction indicating slower rates of change among SM participants (ICC = .10; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024), whereas two DBT-A studies found no residual post-treatment differences (partial η2 < .01–.02; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). Meta-analysis demonstrated a medium pooled pre–post effect with negligible heterogeneity (g = 0.75; see Fig. 4).
Depression symptoms forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in depression symptoms for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 and Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022 are DBT for adolescent studies; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 is a DBT for adults study.

By gender identity, medium-to-large reductions in depression were observed across groups in DBT-A studies (d = 0.60–1.26), with no association between gender identity and post-treatment depression (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023).
Anxiety
Across two DBT-A studies, SM participants showed small-to-medium pre–post reductions in anxiety (d = 0.47–0.57; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022), with comparable reductions across SM subgroups and heterosexual participants (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Between-group analyses indicated no residual post-treatment differences by sexual identity, either after controlling for baseline anxiety or across time (partial η2 = .01–.02; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). Meta-analysis demonstrated a small, pooled effect with negligible heterogeneity (g = 0.42; see Fig. 5).
Anxiety forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in anxiety for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 and Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022 are DBT for adolescent studies.

By gender identity, small-to-medium reductions in anxiety were observed across groups (d = 0.40–0.78), with no association between gender identity and post-treatment anxiety after adjusting for baseline severity (DBT-A; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024).
General psychopathology
In one DBT study, SM participants showed a medium pre–post reduction in general psychopathology (d = 0.48), with no sexual identity × time interaction (Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024).
Global functioning
Across two DBT studies, SM participants showed medium-to-large pre–post improvements in global functioning (d = 0.59–1.11; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024). Between-group findings were mixed, with one DBT study reporting no sexual identity × time interaction (Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023) and the other indicating slower improvement among SM participants (ICC = .12; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024). Meta-analysis demonstrated a large, pooled improvement with high heterogeneity (g = 0.86; see Fig. 6).
Global functioning forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in global functioning for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023 and Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 are DBT for adults studies.

Coping behaviours
Across one DBT and one DBT-A study, SM participants showed medium-to-large pre–post reductions in dysfunctional coping and medium increases in skill use by the end of DBT (d = 0.60–0.89 and 0.65–0.67, respectively; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). Between-group findings were mixed: one DBT study reported slower improvement among SM participants on both outcomes (ICC = .09; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024), whereas the DBT-A study found no differential change by sexual identity after baseline adjustment (partial η2 < .01–.04; Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022). Meta-analyses demonstrated medium pooled improvements in dysfunctional coping (g = 0.65) and skill use (g = 0.71) with negligible heterogeneity (see Figs 7 and 8).
Dysfunctional coping forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in dysfunctional coping for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022 is a DBT for adolescent study; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 is a DBT for adults study.

Skill use forest plot. The forest plot depicts a meta-analysis of studies that provided data on pre–post changes in skill use for the sexual minoritised group. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero. Poon et al., Reference Poon, Galione, Grocott, Horowitz, Kudinova and Kim2022 is a DBT for adolescent study; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023 is a DBT for adults study.

By gender identity, supplementary data from one DBT study indicated pre–post reductions in dysfunctional coping and skills use across all gender groups, with the largest improvements observed among participants identifying as ‘other’, followed by male and female participants (Frost et al., Reference Frost, Strodl, Swannell, MacDonald and Madson2023).
Reasons for living
In one DBT-A study, SM participants showed medium pre–post increases in reasons for living, whereas the heterosexual group showed a small increase (d = −0.61 to −0.67 vs −0.39; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). After controlling for baseline, a medium overall group effect was observed at post-treatment (partial η2 = .07), although post hoc comparisons were not statistically significant. By gender identity, medium pre–post increases were observed for both gender minority (inclusive of transgender and non-binary individuals) and cisgender participants, with no residual post-treatment differences after baseline adjustment (d = 0.63–0.66; partial η2 < .01; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024).
Accident and emergency department attendances
Across two DBT-A studies, large pre–post reductions in accident and emergency department attendances were observed across sexual orientation and gender identity groups (r = .54–.70; d = −0.81 to −1.51; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023). After adjusting for baseline service use, no residual differences in during-treatment attendances were observed between sexual or gender identity groups in the study that examined these effects (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Meta-analysis was not conducted due to heterogeneity in gender group definitions and limited reporting by sexual orientation.
In-patient admissions/hospitalisation
Across two DBT and DBT-A studies, SM participants showed large pre–post reductions in psychiatric hospitalisation (r = .63; d = 0.84; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023), with similarly large reductions observed for bisexual/pansexual and gay/lesbian subgroups (r = .64–.70; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Reductions among heterosexual participants ranged from medium to large across studies (r = .54; d = 0.60; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023). After adjusting for baseline admission days, one study identified between-group differences during DBT, with post hoc comparisons indicating more admissions among heterosexual participants than bisexual/pansexual and gay/lesbian participants, and no other significant contrasts (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024).
By gender identity, large reductions in psychiatric hospitalisation were observed for both GM (inclusive of transgender and non-binary individuals) and cisgender participants, with no residual group differences after baseline adjustment (r = .63–.66; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Supplementary data from another DBT-A study indicated moderate-to-large reductions in in-patient bed days across transgender, boy, and girl participants (d = −0.78 to −1.16), as well as large reductions in partial hospitalisation days for girl and boy participants, with no change among transgender participants due to zero baseline admissions (Hiller and Hughes, Reference Hiller and Hughes2023).
Acceptability/feasibility outcomes
The primary acceptability/feasibility indicator was treatment completion vs non-completion, with phase-specific attrition (pre-treatment vs during treatment) reported where available (see Table 5).
Across DBT and DBT-A studies, intervention completion and attrition rates were broadly comparable between SM and heterosexual participants, with mixed patterns across individual studies (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Camp et al., Reference Camp, Hunt and Smith2023a; Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024). In the largest DBT-A dataset, completion rates were numerically lower for bisexual/pansexual and gay/lesbian participants than for heterosexual participants, with subgroup analyses suggesting higher attrition among bisexual participants; however, these differences were not statistically significant and similar patterns were observed in an overlapping dataset (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Camp et al., Reference Camp, Hunt and Smith2023a). Other DBT studies reported inconsistent findings, including higher attrition among SM participants (Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024), no association with treatment initiation (Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021), or higher non-completion among heterosexual participants (Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023). Meta-analysis of three studies indicated a negligible pooled difference in completion between SM and heterosexual participants (RR = 1.04), with moderate heterogeneity (see Fig. 9).
DBT completion forest plot. The forest plot depicts a meta-analysis of studies that provided data on DBT completion or non-completion for the sexual minoritised and heterosexual groups. Random effects REML model. N = sample size. M = mean. SD = standard deviation. Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024 is a DBT for adolescents study. Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023 and Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024 are DBT for adults studies. Between-study heterogeneity is reported using τ 2 (between-study variance), I 2 (proportion of variance due to heterogeneity), and H 2 (ratio of total to within-study variance). Cochran’s Q tests whether study effects are homogeneous, and the z-test evaluates whether the pooled effect differs significantly from zero.

Figure 9. Long description
The table presents a meta-analysis of studies on DBT completion rates among sexual minorities and heterosexuals. It includes four rows and seven columns. The columns are labeled Study, Sexual Minorities (Yes, No), Heterosexuals (Yes, No), Log risk-ratio with 95% CI, and Weight (%). The studies listed are Camp et al., 2024; Chang et al., 2023; Harned et al., 2021; and Oshin et al., 2024. The table also includes overall heterogeneity statistics and test results. Each row provides the number of participants who completed or did not complete DBT, the log risk-ratio with confidence intervals, and the weight percentage for each study. The overall heterogeneity is reported using tau-squared, I-squared, and H-squared values. Cochran’s Q test and the z-test results are also included.
By gender identity, DBT-A studies generally reported similar completion and attrition rates for GM and cisgender participants, with no statistically significant group differences (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Camp et al., Reference Camp, Hunt and Smith2023a). Subgroup analyses suggested greater variability among GM subgroups, with lower completion observed for transgender women/girls and men/boys participants compared with non-binary and cisgender peers in one study, and lower completion among transgender participants relative to girl and boy participants in another study (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023). These findings were not meta-analysed due to uncertainty regarding gender group classification.
Finally, one DBT-A study provided data on satisfaction as a proxy for acceptability (Hiller and Hughes, Reference Hiller and Hughes2023) and found similar satisfaction ratings for the transgender participants and the girl and boy participants. One DBT study also investigated whether GM participants had different intervention satisfaction ratings than female participants and found no significant difference (Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023).
Sensitivity analysis
Sensitivity analyses examining consistent DBT models indicated outcome-specific differences (see Table 6). For BPD symptoms, between-study heterogeneity decreased from 62.68% when DBT and DBT-A studies were combined (k = 3) to 0.00% when restricted to DBT-A, with a corresponding increase in effect size (g = 0.98 to g = 1.25). For emotion dysregulation, heterogeneity increased from 0.00% across all studies (k = 4) to 72.60% in DBT-A-only analyses, alongside an increase in effect size (g = 1.11 to g = 1.45); when restricted to adult DBT studies, heterogeneity remained at 0.00% and the pooled effect size decreased (g = 0.92). Sensitivity analyses for depressive symptoms showed minimal change, with heterogeneity remaining at 0.00% and nearly identical effect sizes (g = 0.75 vs g = 0.76). For DBT completion, heterogeneity increased modestly when analyses were restricted to DBT studies (60.68% to 73.57%; k = 4), with no change in effect size (RR = −0.04).
Sensitivity analysis including consistent DBT models only

Table 6. Long description
The table compares effect sizes and heterogeneity of DBT programs across different outcomes, divided into two main analyses: Original meta-analysis and Meta-analysis with consistent model only. It has 4 rows and 12 columns. The columns are labeled as Comparison groups, Effect size (g), 95% CI, Heterogeneity (Q), d.f., p, I squared, Effect size (g), 95% CI, Heterogeneity (Q), d.f., p, I squared. The row labels are BPD symptoms, Emotion dysregulation, Depression symptoms, DBT completion. Row 1: BPD symptoms, 0.98, 0.50, 1.47, 5.70, 2, 0.06, 62.68, 1.25, 0.95, 1.60, 0.34, 1, 0.56, 0.00. Row 2: Emotion dysregulation, 1.11, 0.84, 1.38, 5.05, 3, 0.17, 0.00, 1.45, 0.58, 2.31, 3.65, 1, 0.06, 72.60. Row 3: Depression symptoms, 0.75, 0.48, 1.02, 0.19, 2, 0.91, 0.00, 0.76, 0.44, 1.09, 0.61, 1, 0.69, 0.00. Row 4: DBT completion, -0.04, -0.24, 0.16, 7.88, 3, 0.05, 60.68, -0.04, -0.35, 0.27, 6.54, 2, 0.04, 73.57.
Random effects REML model. DBT, dialectical behaviour therapy for adults; DBT-A, dialectical behaviour therapy for adolescents.
Discussion
This systematic review and meta-analysis examined how often DBT studies record and report sexual orientation and gender identity, who is represented when they do, and whether DBT is effective and acceptable for SGM participants.
Proportion of DBT studies recording sexual orientation and gender identity
Of the 170 comprehensive DBT outcome studies, 11.18% reported participants’ sexual orientation. This rate is higher than that observed in adjacent intervention literatures (0.43–7%; Flentje et al., Reference Flentje, Bacca and Cochran2015; Heck et al., Reference Heck, Mirabito, LeMaire, Livingston and Flentje2017; Misra et al., Reference Misra, Bryan, Faber, Printz Pereira, Faber, Williams and Skinta2023), but lower than that reported in a review of US DBT randomised controlled trials (27%; Harned et al., Reference Harned, Coyle and Garcia2022).
In contrast, 17.06% of studies reported gender identity beyond ‘man/boy’ and ‘woman/girl’, although measurement quality was often limited. Nine studies (5.29%) used a single ‘other’ category, which is insufficient to identify GM participants; and one study collapsed SM and GM into a single SGM category. Consequently, only 11.17% of studies provided sufficient detail to identify GM participants as a distinct group. Only three further studies (1.88%) explicitly confirmed cisgender status; in the remaining studies, participants categorised as ‘man/boy’ or ‘woman/girl’ were not confirmed as cisgender or transgender, raising the likelihood of misclassification, particularly in self-report designs (Alpert et al., Reference Alpert, Hernandez, Ruddick, Manzano, Adams, Rivers and Cartujano-Barrera2025; Dichter and Ogden, Reference Dichter and Ogden2019). As a result, disaggregated gender identity outcomes should be interpreted with caution. This limitation likely contributes to the hesitancy of prior authors to examine DBT outcomes among GM participants (e.g. Harned et al., Reference Harned, Coyle and Garcia2022).
The most optimistic estimates of gender identity measurement in the current review are comparable to those reported by Harned et al. (Reference Harned, Coyle and Garcia2022; 11%) and exceed rates in adjacent literatures, including ACT (3%; Misra et al., Reference Misra, Bryan, Faber, Printz Pereira, Faber, Williams and Skinta2023), anxiety and depression (0%; Heck et al., Reference Heck, Mirabito, LeMaire, Livingston and Flentje2017), and substance use intervention trials (0–2%; Flentje et al., Reference Flentje, Bacca and Cochran2015). However, even among the 19 studies reporting GM identities, only three employed methods that clearly distinguished GM from cisgender participants, a well-documented limitation contributing to misclassification and invisibility in research data (Alpert et al., Reference Alpert, Hernandez, Ruddick, Manzano, Adams, Rivers and Cartujano-Barrera2025; Dichter and Ogden, Reference Dichter and Ogden2019; UK Government, 2025).
Together, these patterns reflect potential invalidation through omission or aggregation and underscore the need for more sensitive and disaggregated approaches to sexual orientation and gender identity measurement. At the same time, such data collection must be conducted with careful attention to privacy and safety, as SGM participants may have legitimate confidentiality concerns, particularly within restrictive sociopolitical contexts (Alpert et al., Reference Alpert, Hernandez, Ruddick, Manzano, Adams, Rivers and Cartujano-Barrera2025; American Psychological Association, 2025; Camp et al., Reference Camp, Morris, Wilde, Smith and Rimes2023b; Dichter and Ogden, Reference Dichter and Ogden2019; Jones, Reference Jones2024; PBS NewsHour, 2025; Shanker and Korniejczuk, Reference Shanker and Korniejczuk2024).
SGM representation in DBT study samples
The representation of SM participants within samples reporting this information was 35.67%. This is substantially higher than estimates from the general population (3% in the UK; Office of National Statistics, 2023; 6% in the USA; Flores and Conron, Reference Flores and Conron2023) and higher than rates reported in adjacent psychological intervention literatures (7–21%; Beard et al., Reference Beard, Kirakosian, Silverman, Winer, Wadsworth and Björgvinsson2017; Bezahler et al., Reference Bezahler, Kuckertz, Schreck, Narine, Dattolico and Falkenstein2022; Dunbar et al., Reference Dunbar, Sontag-Padilla, Ramchand, Seelam and Stein2017; Flentje et al., Reference Flentje, Bacca and Cochran2015; Heck et al., Reference Heck, Mirabito, LeMaire, Livingston and Flentje2017; Kent et al., Reference Kent, Suh, Lewis, Saunders, Davies, Lewis and Buckman2025; Misra et al., Reference Misra, Bryan, Faber, Printz Pereira, Faber, Williams and Skinta2023; Plöderl et al., Reference Plöderl, Mestel and Fartacek2022; Rimes et al., Reference Rimes, Ion, Wingrove and Carter2019). Representation was also slightly higher than that reported in US DBT randomised controlled trials (27%; Harned et al., Reference Harned, Coyle and Garcia2022). This elevated representation likely reflects the greater prevalence of difficulties commonly targeted within DBT among SM populations (Camp et al., Reference Camp, Blundell, Smith and Rimes2025; Hainey et al., Reference Hainey, Connolly, Thomson, Smalley, Campbell, Wells and Katikireddi2025; Liu et al., Reference Liu, Sheehan, Walsh, Sanzari, Cheek and Hernandez2019; Marchi et al., Reference Marchi, Arcolin, Fiore, Travascio, Uberti, Amaddeo and Galeazzi2022; Wittgens et al., Reference Wittgens, Fischer, Buspavanich, Theobald, Schweizer and Trautmann2022) and is consistent with minority stress frameworks, which link chronic stigma-related stressors (e.g. discrimination, internalised stigma, expectations of rejection) to increased risk of emotion dysregulation, self-harm, and related difficulties (Frost and Meyer, Reference Frost and Meyer2023). It may also reflect differential help-seeking or research participation patterns across sexual orientation groups (e.g. Dunbar et al., Reference Dunbar, Sontag-Padilla, Ramchand, Seelam and Stein2017).
Within the SM sample, over half (65.12%) were plurisexual (e.g. bisexual and pansexual), followed by monosexual minority groups (e.g. gay/lesbian; 25.61%), queer (6.00%), aro/ace-spectrum (1.91%) and ‘other’ (1.09%). This distribution suggests that plurisexual groups are more likely to be within DBT programmes and research. This higher representation may reflect increased risk of relevant difficulties among plurisexual populations relative to heterosexual and other SM groups (Brewster et al., Reference Brewster, Moradi, DeBlaere and Velez2013; Dyar et al., Reference Dyar, Feinstein, Schick and Davila2017), as well as broader population trends, with plurisexual identities comprising a substantial proportion of SM groups in some countries (e.g. Gallup, 2024). However, this pattern is not consistent across all national datasets (e.g. Office for National Statistics, 2023).
The representation of GM participants, where this was explicitly measured and confirmed as distinct from the cisgender group, was 16.67%. When gender was reported without confirmation of cisgender or transgender status (e.g. ‘man/boy’, ‘woman/girl’, and ‘transgender/gender diverse’), 3.32% were identified as GM, and when ‘other’ categories were used, 4.34% of participants fell into this group. These discrepancies suggest that GM participants are likely present within ‘man/boy’ and ‘woman/girl’ categories when cisgender status is not verified, reinforcing concerns regarding misclassification and under-identification (Alpert et al., Reference Alpert, Hernandez, Ruddick, Manzano, Adams, Rivers and Cartujano-Barrera2025; Dichter and Ogden, Reference Dichter and Ogden2019; UK Government, 2025).
Both estimates are substantially higher than the proportion of GM people in the general population (0.50% in the UK general population; Office of National Statistics, 2023; 1.00% in the USA general population; Herman and Flores, Reference Herman and Flores2025), likely reflecting elevated mental health needs associated with minority stress and related health disparities (Camp et al., Reference Camp, Kashirsky, Pinckard, Hambleton, Oliver, Smith, Badrick, Bhopal, Baudinet and Absoud2026; Hainey et al., Reference Hainey, Connolly, Thomson, Smalley, Campbell, Wells and Katikireddi2025; Liu et al., Reference Liu, Sheehan, Walsh, Sanzari, Cheek and Hernandez2019; Marchi et al., Reference Marchi, Arcolin, Fiore, Travascio, Uberti, Amaddeo and Galeazzi2022; Wittgens et al., Reference Wittgens, Fischer, Buspavanich, Theobald, Schweizer and Trautmann2022). Although comparable estimates are unavailable in adjacent intervention literatures, these findings highlight the need for improved and more granular gender identity measurement in DBT research.
Where gender identity was disaggregated further, 2.50–12.71% identified with nonbinary identities and 0.30–3.87% as transgender women/girls and men/boys. This pattern suggests that nonbinary people may be more likely to access DBT programmes and research. This higher representation may also reflect within- and between-group minority stress processes (e.g. misgendering, identity invalidation, and social exclusion) contributing to elevated mental health difficulties among nonbinary populations (Klinger et al., Reference Klinger, Oehlke, Riedl, Eschbaum, Zesch, Karwautz and Kothgassner2024; Rimes et al., Reference Rimes, Goodship, Ussher, Baker and West2020).
DBT outcomes for sexual orientation and gender identity groups
Effectiveness outcomes
Across outcomes, SM participants showed significant pre–post improvements during DBT. Meta-analytic estimates indicated large effects for BPD symptoms (g = 0.98) and emotion dysregulation (g = 1.11), medium effects for depression (g = 0.75) and coping (dysfunctional coping g = 0.65; skill use g = −0.71), small effects for anxiety (g = 0.42), and large effects for global functioning (g = −0.86), although heterogeneity was substantial for BPD symptoms and global functioning. Reductions in suicidal and non-suicidal self-injury ranged from small to large (r = .53; d = 0.44–0.67). Single-study findings showed medium-to-large improvements in general psychopathology (d = 0.48), reasons for living (d = 0.65), and service-use outcomes, including accident and emergency department visits (r = .60) and in-patient admissions (r = .63; d = 0.84). Overall, these effects are broadly consistent with DBT outcomes reported in the wider literature (Kothgassner et al., Reference Kothgassner, Goreis, Robinson, Huscsava, Schmahl and Plener2021; Panos et al., Reference Panos, Jackson, Hasan and Panos2014).
Within SM subgroups, single-study findings indicated small-to-large pre–post improvements across domains for plurisexual participants (e.g. BPD symptoms d = 0.98; emotion dysregulation d = 0.87; self-injury r = .57) and medium-to-large improvements for gay and lesbian participants (e.g. BPD symptoms d = 1.22; emotion dysregulation d = 0.89; self-injury r = .39; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Between-group comparisons generally showed few meaningful differences between SM and heterosexual participants once baseline severity was controlled, with negligible-to-small effects across outcomes (partial η2 < .01–.02; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Exceptions included trends toward higher reasons-for-living scores (i.e. more reasons for living) among bisexual/pansexual participants and higher in-patient admissions among heterosexual participants. Some studies reported slower rates of improvement among SM participants for select outcomes (ICC = .09–.14; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024), suggesting potential differences in trajectories despite comparable end-of-treatment outcomes.
Findings from the limited number of studies reporting outcomes by gender identity demonstrated significant pre–post improvements across most domains. Large effects were observed for BPD symptoms (d = 0.86–1.61), emotion dysregulation (d = 0.99–1.66), and reductions in accident and emergency department visits (d = −1.51; r = .56) and in-patient service use (d = −1.16; r = .66), with medium effects for depression (d = 0.76–0.79), anxiety (d = 0.78), and reasons for living (d = 0.62). These effects were broadly comparable to those observed for cisgender participants. Only one study directly compared cisgender and transgender groups and found no significant differences in end-of-treatment outcomes after controlling for baseline severity (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). However, given the small number of studies and limited measurement quality, conclusions regarding gender identity-related differences should be drawn cautiously.
Acceptability/feasibility outcomes
Across studies, DBT interventions appeared broadly feasible and acceptable for SM participants, although completion and attrition patterns varied. Meta-analytic findings indicated negligible differences in completion rates between SM and heterosexual participants (RR = 1.04), suggesting comparable feasibility. Individual study findings were mixed: some reported slightly higher attrition among SM participants (e.g. Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021), whereas others found no differences (Harned et al., Reference Harned, Schmidt, Korslund and Gallop2021) or higher non-completion among heterosexual participants (Chang et al., Reference Chang, Halvorson, Lehavot, Simpson and Harned2023). Within SM subgroups, bisexual participants tended to show the lowest completion and highest attrition relative to heterosexual, pansexual, or gay/lesbian participants, although these differences were not statistically significant (Camp et al., Reference Camp, Hunt and Smith2023a; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024). Where reported, attrition among bisexual participants was more pronounced during pre-treatment.
Gender identity-related findings were similarly variable but overall suggested comparable feasibility. Two DBT-A studies found no significant differences in completion or attrition between GM and participants that were not labelled as GM (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Hiller and Hughes, Reference Hiller and Hughes2023). However, disaggregated analyses indicated that transgender girl and boy participants may experience lower completion and higher attrition than nonbinary and cisgender participants, again concentrated in pre-treatment (Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Camp et al., Reference Camp, Hunt and Smith2023a).
Acceptability ratings, where reported, indicated broadly similar satisfaction across gender identity groups (Dunn et al., Reference Dunn, Walton, Matsunaga, Williams and Dimeff2023; Hiller and Hughes, Reference Hiller and Hughes2023), although no study examined acceptability by sexual orientation. Overall, DBT appears feasible and acceptable for SM and GM participants, while potential disparities in engagement for bisexual and transgender participants warrant further investigation.
Implications
The findings of this review are consistent with the adjacent psychological intervention literature in showing poor rates of sexual orientation and gender identity recording in DBT research, despite evidence of high representation of SGM participants when recorded. Researchers and therapists may have understandable concerns, including sociopolitical pressures, that discourage collecting this information. However, omission risks invalidating SGM participants by erasing their presence and visibility in the data, precluding efforts to monitor access and outcome equality. Therefore, research and clinical services need to improve sexual orientation and gender identity data collection.
Beyond invalidation, the absence of sexual orientation and gender identity data risks the delivery of interventions that are ineffective, misapplied, or insufficiently responsive to minority stress-related mechanisms. In the absence of subgroup monitoring, treatments may inadvertently reinforce invalidating environments or overlook processes that maintain distress for SGM people. It also remains uncertain whether non-specialised interventions are equally effective and acceptable for SGM people compared with cisgender heterosexual people – albeit specialised interventions demonstrate promising outcomes (Burger and Pachankis, Reference Burger and Pachankis2024; Pachankis, Reference Pachankis2018) – and the lack of routine data collection prevents systematic monitoring of outcomes. Encouragingly, the available data largely suggest equality of effectiveness and accessibility, although some findings point to inequalities, which require attention and further research. However, there continues to be outcome and access inequalities for some groups in the adjacent literature and some of the DBT literature reviewed here, as well as qualitative findings which suggest gaps in existing, non-specialised DBT and adjacent therapies, including limited acknowledgement of minority stress, inadequate space for SGM-related content, and experiences of therapist microaggressions (Beard et al., Reference Beard, Kirakosian, Silverman, Winer, Wadsworth and Björgvinsson2017; Camp et al., Reference Camp, Morris, Wilde, Smith and Rimes2023b; Camp et al., Reference Camp, Durante, Cooper, Smith and Rimes2024; Compton and Morgan, Reference Compton and Morgan2022; Foy et al., Reference Foy, Morris, Fernandes and Rimes2019; Oshin et al., Reference Oshin, Silamongkol, Pucker, Finkelstein, King and Rizvi2024; Rimes et al., Reference Rimes, Ion, Wingrove and Carter2019).
Additionally, none of the included studies examined outcomes directly related to minority stress processes, such as changes in internalised stigma, despite strong evidence that these processes are key predictors of mental health outcomes and important therapeutic targets in psychological interventions for SGM people (e.g. Frost and Meyer, Reference Frost and Meyer2023). Notably, many non-specialised interventions, including DBT, do not explicitly target minority stress mechanisms (e.g. internalised stigma, identity concealment, expectations of rejection), which may limit their capacity to address drivers of distress specific to SGM populations. Nonetheless, numerous authors have described how chronic exposure to minority stressors aligns with the invalidating transactions outlined within the DBT biosocial model (e.g. Camp, Reference Camp2023; Linehan, Reference Linehan1993; Skerven et al., Reference Skerven, Whicker and LeMaire2019). However, alignment at a theoretical level does not ensure that minority stress processes are explicitly assessed or targeted in practice, highlighting the need to consider how interventions such as DBT can be optimised for SGM populations.
This potential gap in the assessment and targeting of minority stress processes, alongside limited inclusion and reporting of SGM participants, is important given evidence suggesting that SGM populations may experience elevated prevalence of diagnoses and clinical presentations commonly treated within DBT, including borderline personality disorder and emotion dysregulation (e.g. Camp et al., Reference Camp, Blundell, Smith and Rimes2025; Rodriguez-Seijas et al., Reference Rodriguez-Seijas, Morgan and Zimmerman2021). The potential omission of SGM participants in DBT outcome research therefore risks obscuring differential treatment needs and outcomes for a group likely to be disproportionately exposed to the invalidating environments central to DBT’s theoretical model. Together, these findings underscore the importance of comprehensive and consistent assessment of sexual orientation and gender identity, alongside consideration of minority stress processes, in DBT research and intervention development.
Beyond measurement, culturally sensitive competence is critical to ensuring that DBT is experienced as safe, relevant, and effective for SGM participants. Qualitative findings in DBT and adjacent literatures indicate that reduced cultural competence – such as therapist microaggressions, avoidance of SGM-related content, or implicit cis-heteronormative assumptions – can undermine engagement and contribute to attrition despite otherwise effective interventions (e.g. Camp et al., Reference Camp, Morris, Wilde, Smith and Rimes2023b; Harding et al., Reference Harding, Pratt and Lea2025). Integrating content, identity, and minority stress into formulations/case conceptualisation; explicit validation of identity-related experiences; and attempts to reduce cis-heteronormative assumptions within DBT content and therapists may therefore be necessary to increase cultural competence for SGM people (Burger and Pachankis, Reference Burger and Pachankis2024; Camp, Reference Camp2023; Skerven et al., Reference Skerven, Whicker and LeMaire2019).
Collecting sexual orientation and gender identity data will require researchers and clinicians to do so sensitively, age-appropriately, and with clear assurances of privacy and confidentiality (Camp et al., Reference Camp, Morris, Wilde, Smith and Rimes2023b; NHS England & NHS Improvement, 2022; Shanker and Korniejczuk, Reference Shanker and Korniejczuk2024), particularly in contexts where disclosure could pose risk. Practical strategies to mitigate re-identification risk can include the use of minimum cell-size thresholds (e.g. suppressing or aggregating categories where n < 5), symbolic masking in tables (e.g. ‘ < 5’ or ‘#’), and avoiding cross-tabulation of multiple potentially identifying characteristics in small samples, as well as seeking informed consent from participants after providing clarity on where the data will be stored, for how long, and who will have access.
When collected, demographic information on sexual orientation and gender identity should be obtained with sufficient granularity to allow for the identification of relevant subgroups, given evidence of heterogeneity in outcomes between them (Beard et al., Reference Beard, Kirakosian, Silverman, Winer, Wadsworth and Björgvinsson2017; Rimes et al., Reference Rimes, Ion, Wingrove and Carter2019). However, the configuration of these measures, particularly for identifying gender diverse participants, requires careful consideration. Although two-step approaches have historically utilised questions on ‘sex assigned at birth’ and ‘current gender identity’, this format has been critiqued by trans+ and gender-diverse scholars and advocacy organisations for reinforcing a normative baseline of ‘birth sex’ that can inadvertently legitimise erasure and medical gatekeeping (UK Government, 2025). Instead, researchers are encouraged to develop and pilot sex- and gender-related measures in collaboration with trans+ and gender-diverse people and organisations to ensure that the wording, sequencing, and options used reflect lived experience, promote psychological safety, and yield data that are both inclusive and analytically useful (Alpert et al., Reference Alpert, Hernandez, Ruddick, Manzano, Adams, Rivers and Cartujano-Barrera2025; Dichter and Ogden, Reference Dichter and Ogden2019; UK Government, 2025), with reference to emerging methodological guidance and critical considerations in this area (e.g. Guyan, Reference Guyan2026; Todd & Callard, Reference Todd and Callard2026; Veldhuis et al., Reference Veldhuis, Cascalheira, Delucio, Budge, Matsuno, Huynh and Galupo2024). Such approaches should provide space for self-description and non-disclosure (e.g. ‘prefer not to say’), accompanied by clear explanations that the purpose of data collection is to recognise diversity rather than to police or invalidate identity differences. It is also important to note that different considerations will be needed when considering adolescent samples, given the potential level of parent/guardian involvement in both treatment engagement and providing sociodemographic information.
Comparisons with cisgender, heterosexual participants were used in this review to examine equity in outcomes, rather than to position cisgender or heterosexual identities as normative benchmarks. At the same time, reliance on between-group comparisons alone risks obscuring SGM-specific treatment needs, underscoring the importance of evaluating outcomes and mechanisms within SGM communities in their own right.
Finally, beyond collecting sociodemographic data, researchers should actively examine whether outcome inequalities exist between groups and whether interventions meaningfully reduce minority stress processes (e.g. internalised stigma, shame, concealment), in line with affirmative and culturally sensitive therapy principles for SGM people (e.g. Burger and Pachankis, Reference Burger and Pachankis2024). This is particularly important given emerging evidence of differences in attrition rates and trajectories of change in some outcomes in this review and similar literature (Beard et al., Reference Beard, Kirakosian, Silverman, Winer, Wadsworth and Björgvinsson2017; Pachankis, Reference Pachankis2018; Rimes et al., Reference Rimes, Ion, Wingrove and Carter2019).
Strengths and limitations
This review has several strengths: broad database coverage via OvidSP (multiple biomedical and psychology indexes), inclusion of grey literature, proactive author contact for missing data, and blinded double-screening/checked extraction – all of which enhance methodological rigour. Focusing exclusively on comprehensive DBT also supports conceptual coherence across studies.
Limitations should also be noted. First, the search strategy restricted DBT terms to titles/keywords, which likely improved specificity but may have missed eligible records with less explicit indexing; searches were also limited to English-language publications. Second, few authors supplied additional sexual orientation/gender identity or outcome detail, and many primary studies did not collect sexual orientation and gender identity with sufficient detail, yielding available-case syntheses and constraining subgroup/meta-analytic power. Additionally, not all studies that provided data on sexual orientation or gender identity provided a breakdown of which subgroups were represented. Third, the number of studies for each outcome was consistently small and between-study heterogeneity was high for some domains. Fourth, overlapping samples required conservative selection rules and checks. Fifth, this review did not include DBT-informed interventions, which may be worth considering in future reviews given the frequent use of this format in clinical practice. Additionally, the inclusion of parents or caregivers in treatment may limit adolescents’ willingness or ability to disclose sexual orientation or gender identity, particularly in contexts where family acceptance is uncertain. Consequently, demographic data in DBT-A studies may under-estimate the prevalence of SM and GM identities, reflecting safety considerations rather than absence of identity. Sixth, acceptability and feasibility outcomes were largely limited to treatment completion, attrition, and satisfaction; no included studies examined therapeutic relationship variables (e.g. alliance, validation, or perceived affirmativeness), which may be particularly salient for SGM participants and should be prioritised in future research.
The inclusion of both adolescent and adult samples necessarily introduced developmental heterogeneity, given differences in family involvement, service structures, and pathways into DBT. However, sensitivity analyses stratified by DBT versus DBT-A indicated that pooled effect sizes were largely unchanged, with improvements primarily reflected in reduced heterogeneity rather than shifts in magnitude, suggesting that core conclusions regarding effectiveness and feasibility for SGM participants may not differ across age groups. Finally, variability in definitions of completion/non-completion and in sexual orientation/gender identity measurement likely introduced measurement heterogeneity and limit the precision and generalisability of pooled estimates.
Conclusions
This review highlights that sexual and gender minority inclusion in DBT research remains limited, constraining understanding of equitable access and outcomes. Systematic, inclusive, and collaboratively developed collection of sexual orientation and gender identity data is essential to advance equity, improve transparency, and ensure that non-specialised evidence-based therapies such as DBT fully meet the needs of diverse populations. Where sufficient data were collected, there were promising acceptability/feasibility and effectiveness outcomes for SGM participants compared with cisgender/heterosexual participants, with a few exceptions. However, efforts to optimise interventions for SGM groups remain needed.
Key practice points
-
(1) Routinely collect inclusive identity data: DBT and CBT services and research should systematically collect sexual orientation and gender identity information using co-designed, affirming measures that allow for self-description and non-disclosure, as well as accurate identification of transgender/gender diverse participants.
-
(2) Monitor and report on equity in access and outcomes: services and researchers should disaggregate outcome data by sexual orientation and gender identity to identify and address disparities in access, acceptability, feasibility, and effectiveness. This should be disseminated to increase understanding within research and practice.
-
(3) Strengthen SGM culturally sensitive competence: clinicians should integrate awareness of minority stress and identity-specific barriers within DBT/CBT intervention delivery, case formulation, and supervision. This is pertinent given the high representation of SGM people in DBT services and studies and the potential for some inequality in outcomes, as well as this being recommended in the wider literature.
Data availability statement
This systematic review is a secondary analysis of existing published research, thus data availability for the original studies will vary.
Acknowledgements
We would like to acknowledge the work of Ashleigh-Jane Woodrup, an expert-by-experience young person, who took the time to read over this manuscript to provide feedback on wording and content.
Author contributions
Jake Camp: Conceptualization (lead), Data curation (equal), Formal analysis (lead), Funding acquisition (lead), Investigation (lead), Methodology (lead), Project administration (lead), Resources (lead), Software (lead), Supervision (equal), Validation (lead), Visualization (lead), Writing - original draft (lead), Writing - review & editing (lead); Mara Bodea: Conceptualization (supporting), Data curation (equal), Formal analysis (equal), Investigation (supporting), Methodology (supporting), Project administration (supporting), Validation (equal), Writing - original draft (supporting), Writing - review & editing (supporting): Kim Skerven: Conceptualization (supporting), Data curation (supporting), Formal analysis (supporting), Methodology (equal), Project administration (supporting), Validation (equal), Visualization (supporting), Writing - review & editing (supporting); Stan Papoulias: Conceptualization (supporting), Investigation (supporting), Methodology (supporting), Project administration (supporting), Supervision (equal), Writing - review & editing (supporting); Michaela Anne Swales: Conceptualization (supporting), Formal analysis (supporting), Funding acquisition (supporting), Investigation (supporting), Methodology (supporting), Project administration (supporting), Supervision (equal), Writing - review & editing (supporting); Patrick Smith: Conceptualization (supporting), Formal analysis (supporting), Funding acquisition (supporting), Investigation (supporting), Methodology (supporting), Project administration (supporting), Supervision (equal), Writing - review & editing (supporting).
Financial support
Jake Camp, via the NIHR Doctoral Clinical and Practitioner Academic Fellowship Scheme, is funded by the National Institute for Health and Care Research (NIHR) for this research project (ref: NIHR304071). The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, NHS, or the UK Department of Health and Social Care.
Competing interests
Jake Camp is an Associate Editor of the Cognitive Behaviour Therapist. They were not involved in the review or editorial process for this paper, on which they are listed as an author. Jake Camp also receives payment for providing training in DBT.
Michaela Swales provides training in DBT, receives royalties from books and training materials and her husband is the Chair of the Board and major shareholder in a company delivering training in DBT. No other authors declare competing interests.
Ethical standards
This study abides by the Ethical Principles of Psychology and Code of Conduct set out by the BABCP and BPS. This systematic review was a secondary analysis of published data and thus did not require ethical approval. The protocol for this review was published a priori via PROSPERO (ref: CRD42025609288).
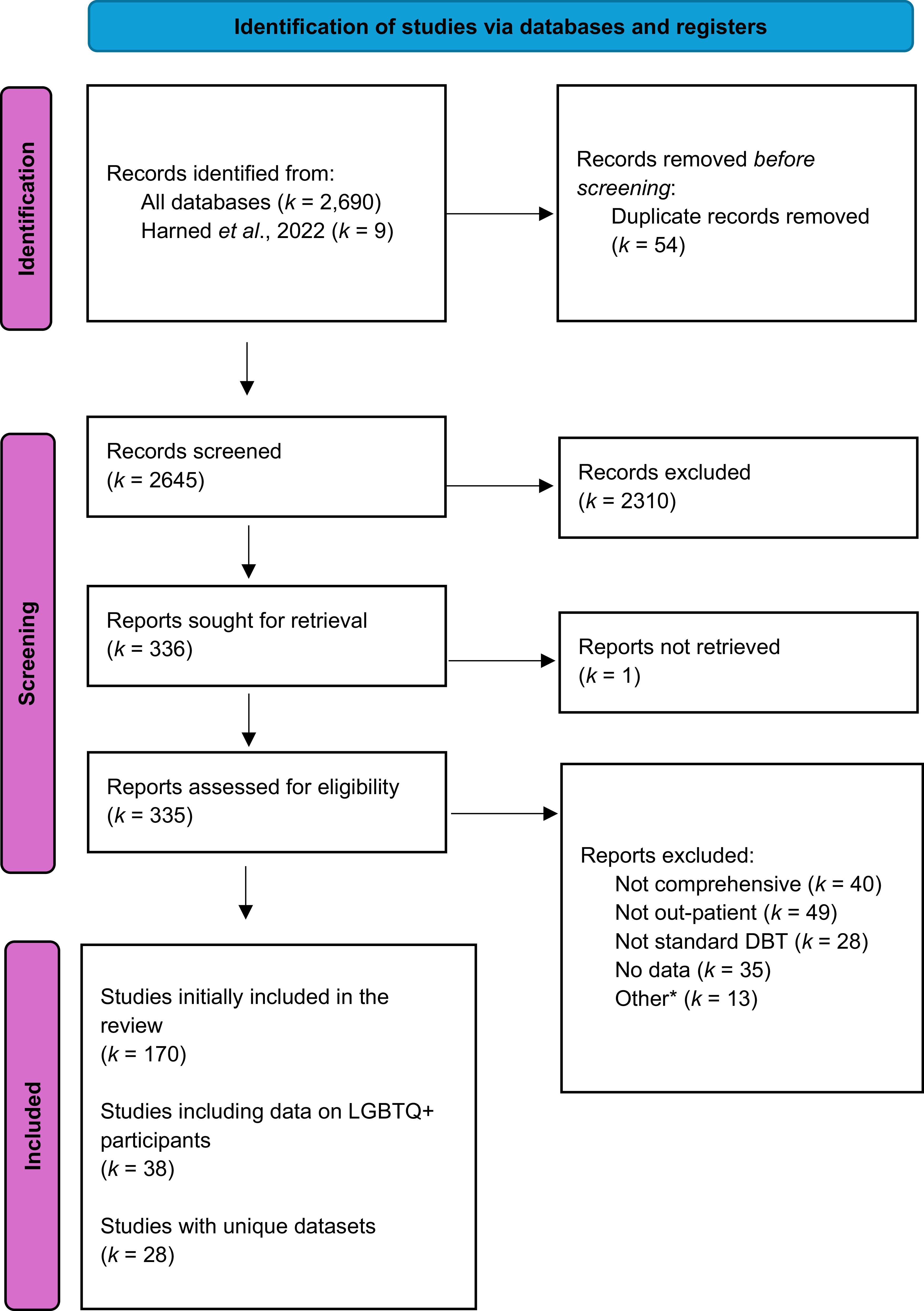

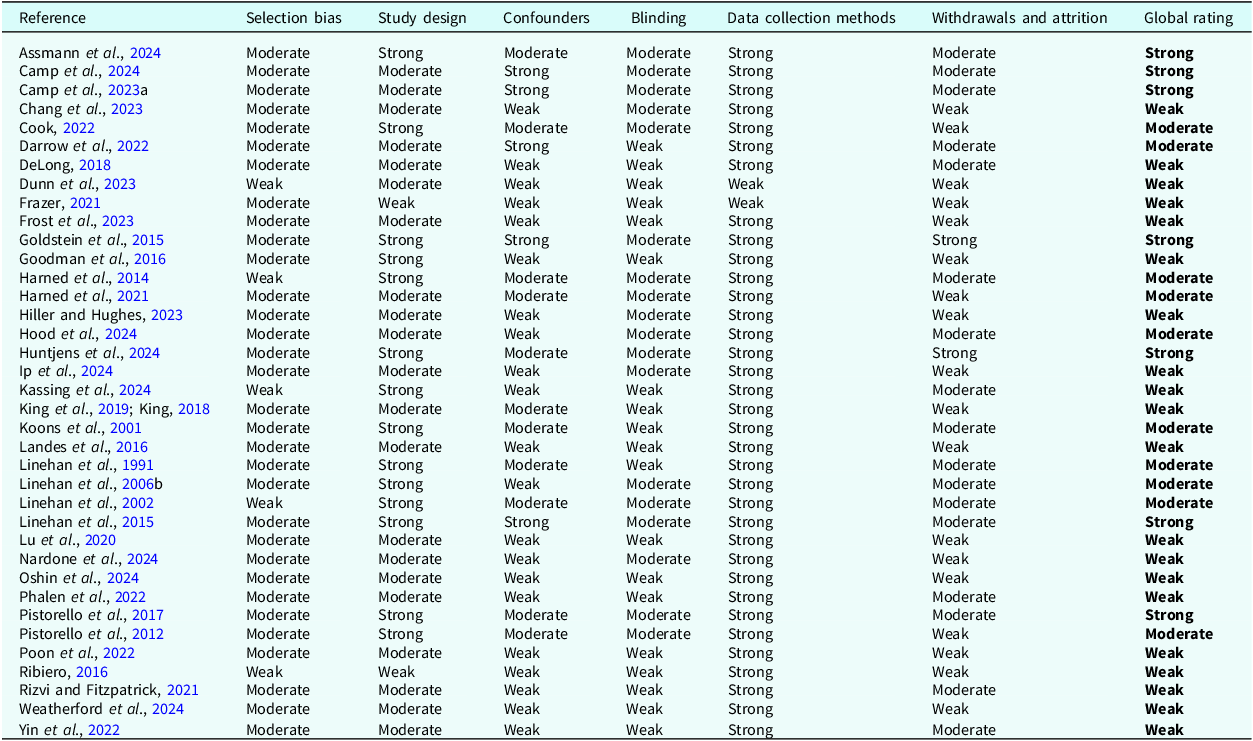
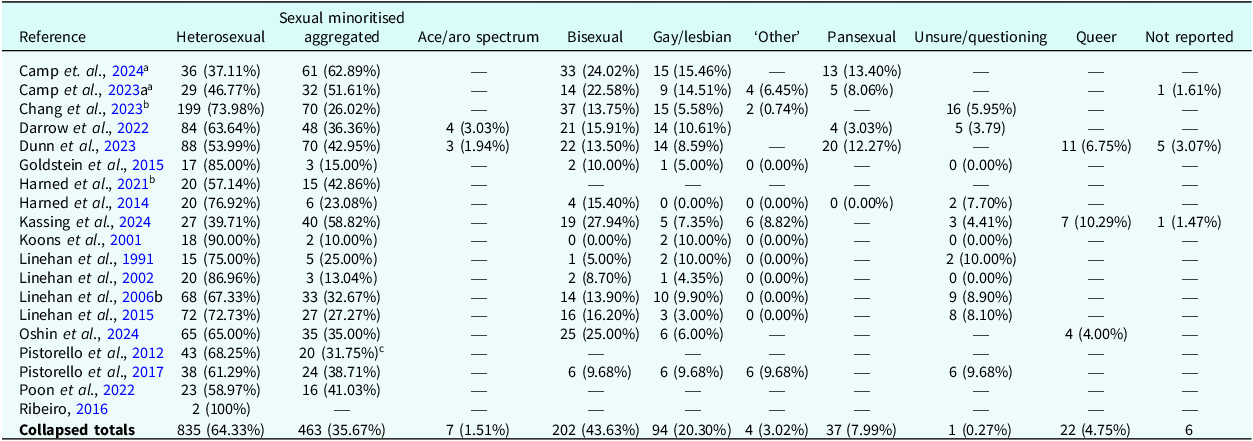
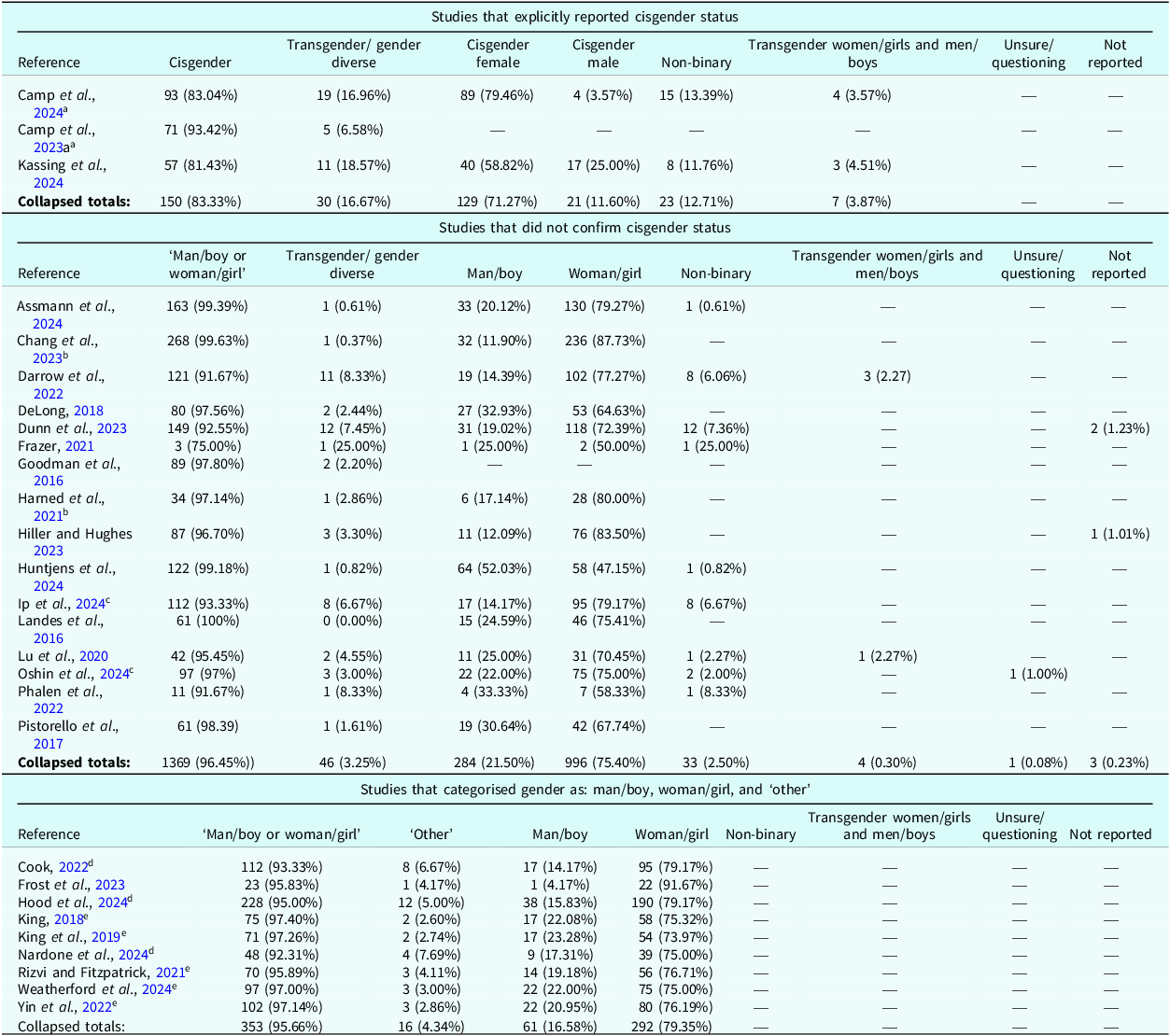









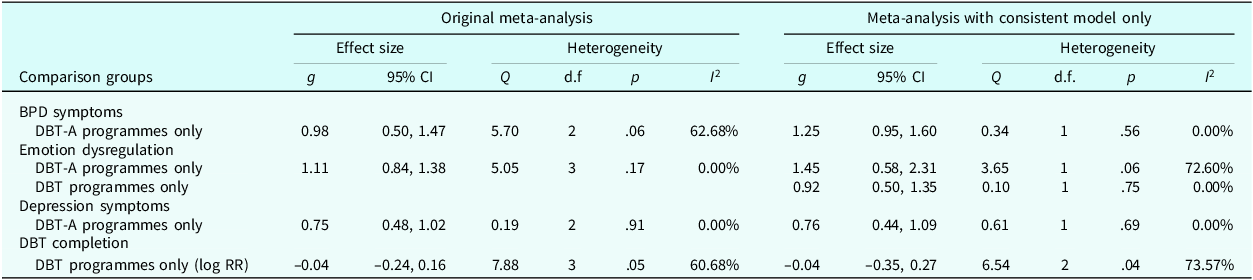

 Open access
Open access
Comments
No Comments have been published for this article.