


Introduction
Induced abortion (IA) is a crucial component of sexual and reproductive health and a significant factor in fertility behaviour. Together with contraception and sexual abstinence, IA allows for the control of the timing of motherhood and the number of children, contributing to the exercise of reproductive autonomy (Ferrer Serret and Solsona Pairó, Reference Ferrer Serret and Solsona Pairó2018a). Although abortion is a phenomenon present across all social strata, the probability of resorting to it increases under specific conditions (Rossier et al., Reference Rossier, Michelot and Bajos2007; Coast et al., Reference Coast, Norris, Moore and Freeman2018; Väisänen and Batyra, Reference Väisänen and Batyra2022).
Among the various factors associated with unintended pregnancies and, consequently, abortion, age emerges as one of the most robust and consistent predictors. However, this association is not linear. Empirical evidence reveals a characteristic pattern: unintended pregnancies ending in abortion rates peak among women aged 20–24 years, decline progressively during the late twenties and early thirties – when childbearing tends to be intentional – and increase again at older reproductive ages (Pérez et al., Reference Pérez, Ruiz-Munoz, Gotsens, Cases and Rodriguez-Sanz2014; Llorente-Marrón et al., Reference Llorente-Marrón, Díaz-Fernández and Méndez-Rodríguez2016; Ferrer Serret and Solsona Pairó, Reference Ferrer Serret and Solsona Pairó2018b; MS, 2021). These age-specific patterns suggest that reproductive intentions are not static; rather, they evolve over time, shaped by a combination of personal conditions, life transitions, and broader structural conditions (Helfferich et al., Reference Helfferich, Hessling, Klindworth and Wlosnewski2014; Kuhnt et al., Reference Kuhnt, Minkus and Buhr2021).
The motivations underlying abortion decisions are closely linked to the age at which a pregnancy occurs. Young women, particularly those who are single and childless, are more likely to seek abortion as a means of avoiding early motherhood and its potential interference with educational trajectories and labour market integration (Bankole et al., Reference Bankole, Singh and Haas1999; Ferrer Serret and Solsona Pairó, Reference Ferrer Serret and Solsona Pairó2018b). Conversely, in later stages of the reproductive cycle, abortion may be used to limit or suspend further childbearing, often in the context of having already achieved the desired family size or facing work–family conflicts (Chae et al., Reference Chae, Desai, Crowell and Sedgh2017; Ferrer Serret and Solsona Pairó, Reference Ferrer Serret and Solsona Pairó2018b). In some cases, however, women without children nearing the end of their reproductive years may be more inclined to continue a pregnancy despite adverse conditions, given the increasing weight of biological constraints and the salience of motherhood aspirations (Helfferich et al., Reference Helfferich, Hessling, Klindworth and Wlosnewski2014).
However, age does not operate in isolation but interacts dynamically with a range of individual and contextual variables (Minkus and Drobnič, Reference Minkus and Drobnič2021). Several studies have shown that the influence of factors such as partnership status, parity, and socio-economic position is mediated by the age in which a woman finds herself (Bankole et al., Reference Bankole, Singh and Haas1999; Sihvo et al., Reference Sihvo, Bajos, Ducot and Kaminski2003; Santelli et al., Reference Santelli, Speizer, Avery and Kendall2006; Rossier et al., Reference Rossier, Michelot and Bajos2007). Recent studies showed that having dependent children, living without a stable partner, lower educational attainment, and unemployment are strongly associated with abortion decisions, and these associations vary significantly across age groups (Senso et al., Reference Senso, Rodríguez and Rodríguez-Arenas2022; Requena and Stanek, Reference Requena and Stanek2024). In this sense, the same condition – such as unemployment or the absence of a stable partner – may carry different implications depending on whether a woman is at the beginning or at a more advanced stage of her reproductive trajectory. In other words, age shapes how educational level, employment status, and access to economic resources influence the perception of pregnancy and the acceptability of its continuation (Kuhnt et al., Reference Kuhnt, Minkus and Buhr2021; Requena and Stanek, Reference Requena and Stanek2025).
Spain legalised abortion in 1985, establishing provisions that permitted the procedure within specific gestational limits. In 2010, a law was enacted allowing unrestricted abortion until the 14th week and up to the 22nd week in certain circumstances such as serious risks to the pregnant woman’s life or health or severe foetal abnormalities. Between 2002 and 2011, the abortion rate per 1,000 women steadily increased from 8.4 to 12.4 (MS, 2011; Senso et al., Reference Senso, Rodríguez and Rodríguez-Arenas2022). However, from that point onwards, it began to decrease and reached 10.7 in 2021 (MS, 2021). According to estimates made by Bearak et al. Reference Bearak, Popinchalk, Beavin, Ganatra, Moller, Tunçalp and Alkema(2022), in Spain, in 2015–2019, 36% of all pregnancies were unintended, of which 43% ended in abortion. In other words, 15.5% of all pregnancies ended in IA.
Although abortion patterns and correlates in Spain have attracted considerable attention, research has primarily focused on their association with social and demographic characteristics – such as educational attainment and migratory background (Malmusi and Pérez, Reference Malmusi and Pérez2009; Zurriaga et al., Reference Zurriaga, Martínez-Beneito, Galmés Truyols, Torne, Bosch, Bosser and Portell Arbona2009; Rodríguez-Álvarez et al., Reference Rodriguez-Alvarez, Borrell, González-Rábago, Martín and Lanborena2016; González-Rábago et al., Reference González-Rábago, Rodriguez-Alvarez, Borrell and Martín2017; Senso et al., Reference Senso, Rodríguez and Rodríguez-Arenas2022; Requena and Stanek, Reference Requena and Stanek2024) – as well as on socio-economic inequalities (Font-Ribera et al., Reference Font-Ribera, Pérez, Salvador and Borrell2008; Pérez et al., Reference Pérez, Ruiz-Munoz, Gotsens, Cases and Rodriguez-Sanz2014) and the effects of the economic crisis (Pérez et al., Reference Pérez, Gotsens, Cevallos-García and Domínguez-Berjón2019). To date, no study has systematically examined how age patterns vary across sociodemographic subgroups or how age interacts with other determinants in shaping the likelihood of IA in Spain. Most studies treat age merely as a control variable (Font-Ribera et al., Reference Font-Ribera, Pérez, Salvador and Borrell2008; Pérez et al., Reference Pérez, Ruiz-Munoz, Gotsens, Cases and Rodriguez-Sanz2014). Others focused on a specific life stage, for example, young adults aged 25–34 years (Ferrer Serret and Solsona Pairó, Reference Ferrer Serret and Solsona Pairó2018b), taking into account various control variables such as country/region of origin (Zurriaga et al., Reference Zurriaga, Martínez-Beneito, Galmés Truyols, Torne, Bosch, Bosser and Portell Arbona2009; González-Rábago et al., Reference González-Rábago, Rodriguez-Alvarez, Borrell and Martín2017; Senso et al., Reference Senso, Rodríguez and Rodríguez-Arenas2022), socio-economic status (Font-Ribera et al., Reference Font-Ribera, Pérez, Salvador and Borrell2008), and education level (Rodriguez-Alvarez et al., Reference Rodriguez-Alvarez, Borrell, González-Rábago, Martín and Lanborena2016; González-Rábago et al., Reference González-Rábago, Rodriguez-Alvarez, Borrell and Martín2017). To address this gap, this study aimed to explore the likelihood of a pregnancy ending in IA, with particular attention to age patterns and their interactions with partnership status, the number of children, and employment status.
Methods
This study was based on the quantitative analysis of data merged from two registries: the Voluntary Termination of Pregnancy Statistics (from 2011 to 2022) and the Vital Statistics (Movimiento Natural de la Población, MNP) (from 2011 to 2022). The Voluntary Termination of Pregnancy Statistics is a data source maintained and managed by the Spanish Ministry of Health, based on information obtained from the Autonomous Communities. It contains data records of IA procedures performed in healthcare centres (both hospital and non-hospital settings, public and private) for both resident and non-resident women in Spain. The Vital Statistics data – a registry produced and managed by the Spanish National Statistics Institute (Instituto Nacional de Estadística, INE) – included registrations of births (live and stillborn) and late foetal deaths (LFDs). An LFD is defined as the ‘death, before its complete expulsion or extraction from the mother’s body, of a viable conception product’ with viability currently determined by a weight of 500 g or more or gestational age of 22 weeks or more.
The objective of combining these databases was an estimate as comprehensive as possible of the annual number of pregnancies (denominator) and the possible outcomes of conception: live birth or stillbirth, foetal death, and IA. The only outcome that is not monitored is miscarriages (natural abortions), since in Spain, data on miscarriages are not systematically recorded nor regularly published by health authorities, which means that approximately 15–20% of potential pregnancy outcomes are not captured. This is because miscarriages that occur before 22 weeks or involve a foetus weighing less than 500 g are not systematically monitored and, in some cases, go unnoticed by the women herself (Sánchez Ortiz et al., Reference Sánchez Ortiz, Huerta, Llorente-García, Ortega, Astasio and Cea-Soriano2021).
The unified database comprises all pregnancy records between 2011 and 2022. First, pregnancies conceived in 2010 and 2022 were removed due to incomplete data, which could otherwise introduce bias (N = 4,837,275). Then, only women in the fertile age range, that is, aged between 15 and 44 years, were selected, in line with the age definition used by the Spanish Ministry of Health in its official statistics on voluntary terminations of pregnancy. Afterwards, cases with women residing abroad were excluded. Lastly, all lost values were removed. Consequently, the dataset was reduced to 4,404,902 cases (Figure 1). Of these total cases, 76.3% were live births, 0.2% were LFDs, 1.9% were abortions performed for medical reasons, such as foetal anomalies or risks to the woman’s health, and 21.6% were IAs, those performed in the first 14 weeks of pregnancy.
Selection flow and study population.

The dependent variable in the analysis was the pregnancy outcome, which was divided into two categories: (i) IAs performed until the 14th week of gestation and (ii) all other recorded pregnancy outcomes: abortions performed after 14 weeks due to medical indications (risks to the pregnant woman’s life or foetal anomalies), live births, stillbirths, and LFDs. The main independent variables were age, the number of children, having or not having a partner, and employment status (divided into employed and not employed women: inactive and unemployed) as these are the most relevant factors when a woman decides to terminate a pregnancy (Minkus and Drobnič, Reference Minkus and Drobnič2021). Other adjustment variables were included, namely educational level, ratio of centres per 100,000 women of reproductive ageFootnote 1 , country of birth, and year of conception (the conception date was calculated by subtracting the gestational age from the event date).
Age has been grouped into four broad categories: 15–19, 20–29, 30–39, and 40–44 years – categories that align with those widely used in studies on abortion (Shah and Ahman, Reference Shah and Ahman2004; Sedgh et al., Reference Sedgh, Bankole, Singh and Eilers2013; Jones, Reference Jones2024). This classification enables comparison across women at different age and allows for a clearer interpretation of the results in relation to their social and reproductive circumstances. The 15–19 group corresponds to adolescence – a period in which motherhood tends to be less common and more shaped by structural conditions. The 20–29 group represents a stage of transition to adulthood, while the 30–39 group includes, on average, the core years of motherhood and family formation in the Spanish context. Finally, the 40–44 age range marks the final phase of reproductive age, in which pregnancies are less frequent and often more planned or linked to specific circumstances.
The analysis was carried out in three stages. In the first stage, descriptive analysis was performed to examine the association between each independent variable and the dependent variable. In the second stage, log binomial regression was used to calculate the odds ratios (ORs) and corresponding 95% confidence intervals (CIs) for the associations of the number of children, having or not having a partner, and age with each dependent variable before and after controlling for educational level, employment status, place of residence, country of woman’s birth, and year of conception. For the final models, the associations between partnership status, number of children, and employment status with the likelihood of an IA were examined by incorporating interaction terms with age group. This approach allows the models to capture how the predictive effect of these social determinants varies across different age categories. The results of these interactions are presented as adjusted predicted probabilities. All models were further adjusted for educational level, the ratio of centres per 100,000 women of reproductive age, country of birth, and year of conception. All statistical analyses were conducted using the Stata software for Windows, version 17.0.
Results
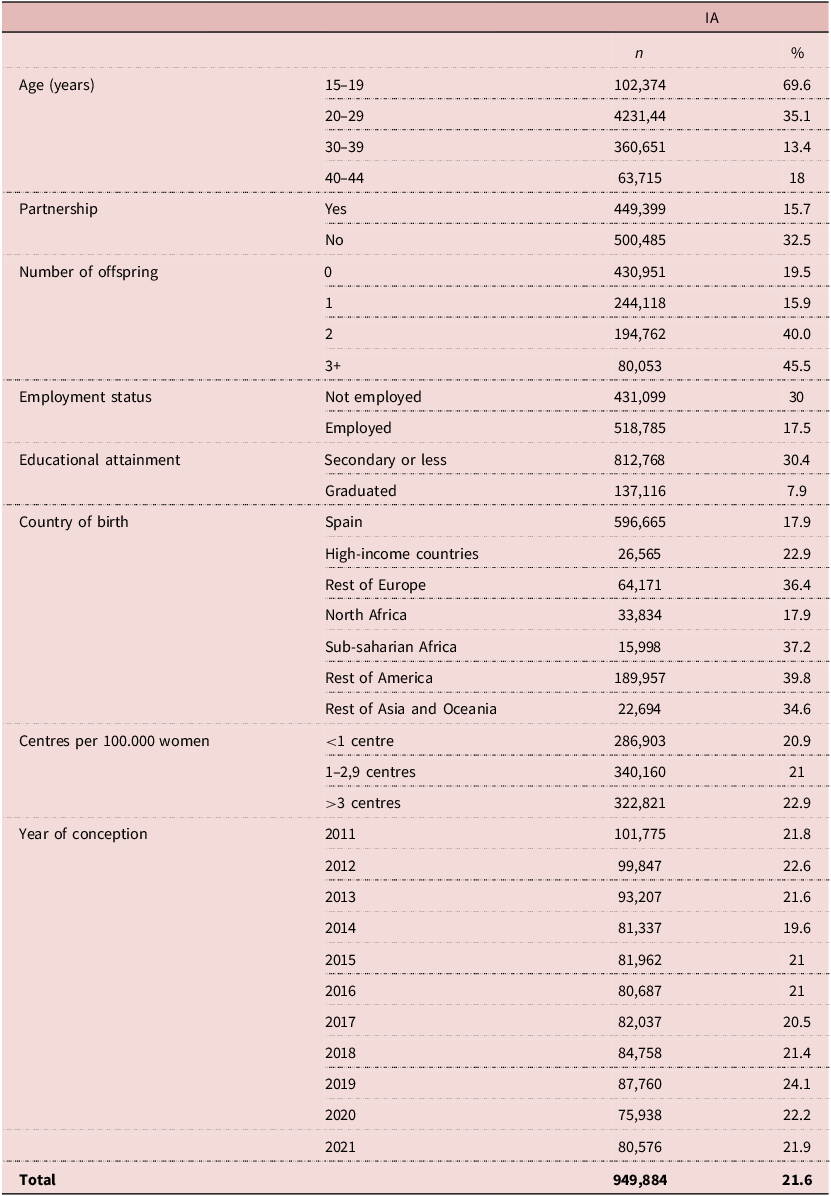
Table 1 shows the percentage of pregnancies ending in IA compared to other outcomes (births, LFDs, or abortions due to risk to the woman or foetus) according to the selected independent variables and their respective values. All variables showed significant chi-square results, indicating significant differences for each variable.
Descriptive statistics for the studied population

Table 1 Long description
A table showing descriptive statistics for a studied population. The table has 12 rows and 3 columns. The columns are labeled 'Age (years)', 'n', and '%'. The rows are grouped by age ranges, partnership status, number of offspring, employment status, educational attainment, country of birth, centers per 100,000 women, and year of conception. Each row provides the count (n) and percentage (%) for each category. For example, the age group 15-19 has 102,374 individuals, representing 69.6 percent of the population. The table includes detailed data points for each category, such as employment status with 431,099 not employed and 518,785 employed, and educational attainment with 812,768 having secondary or less education and 137,116 being graduated.
Source: Authors’ calculations using the Voluntary Termination of Pregnancy and The Vital Statistisc registered between January 2011 and December 2022.
The association between age and the percentage of IA was not linear, with the highest proportion reported in adolescent women aged 15–19 years (69.6%) and the lowest among women aged 30–39 years (1.4%). Furthermore, the absence of a partner resulted in a larger percentage of pregnancies ending in IAs than the presence of one (32.5% vs. 15.7%). The percentage of women opting for IAs increased as the number of children increased, ranging from 19.5% for women with no children to 45.5% for those with three or more children. Employment status showed clear differences: non-employed women had a higher incidence of IA (30%) than employed women (17.5%). Similarly, educational attainment was inversely associated with IA: women with secondary education or less had a higher percentage (30.4%) compared with university graduates (7.9%).
Differences were also observed by country of birth. Women from Spain and North Africa had similar proportions of IA (17.9%), while women from other regions showed higher rates, particularly those from sub-Saharan Africa (37.2%), the rest of Europe (36.4%), the rest of America (39.8%), and the rest of Asia and Oceania (34.6%). Women from high-income countries had a rate of 22.9%. The availability of healthcare centres showed a modest gradient: in areas with fewer than one centre per 100,000 women, 20.9% of pregnancies ended in IA, compared with 21% in areas with 1–2.9 centres and 22.9% in areas with more than three centres per 100,000 women. Finally, the year of conception also influenced the proportion of IVE, with the lowest rates in 2014 (19.6%) and the highest in 2019 (24.1%). Overall, 21.6% of pregnancies ended in IA during the study period.
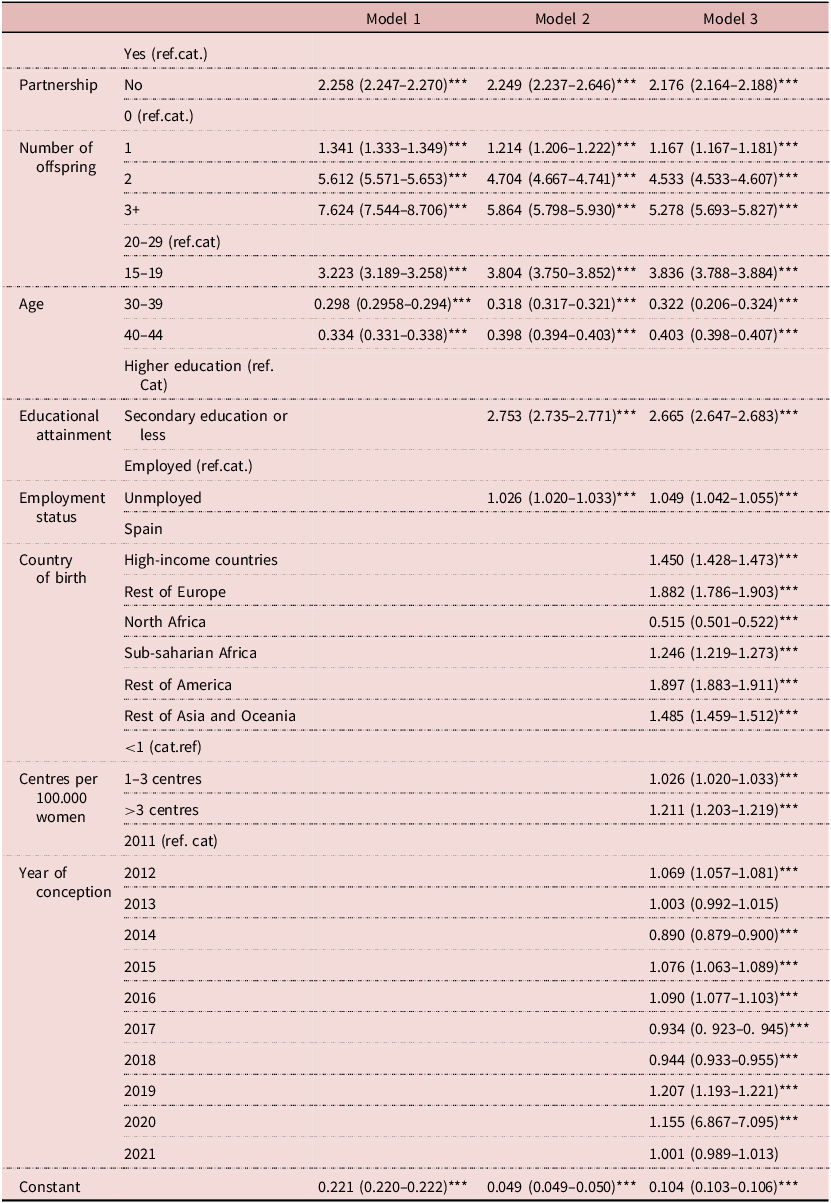
The results of the logistic regression analysis shown in Table 2 reveal a highly stable set of predictors for IA, where age emerges as a central factor. Using women aged 20–29 years as the reference category, adolescents consistently show higher odds of IA, while women aged 30–39 years and 40–44 years display markedly lower odds – a pattern that remains consistent across all adjusted models. Notably, the 30–39 age group presents the lowest probability of IA compared to all other cohorts, a finding that aligns with the concentration of maternal intentionality and birth rates in this group of age.
Odds ratios for induced abortion

Table 2 Long description
The table presents odds ratios for induced abortion across different models. It includes rows for partnership status, number of offspring, age groups, educational attainment, employment status, country of birth, centers per 100,000 women, and year of conception. Each row lists the odds ratios for three models, with confidence intervals. For example, the odds ratio for no partnership is 2.258 in Model 1, 2.249 in Model 2, and 2.176 in Model 3. The table also includes a constant value for each model. The data highlights how different factors influence the likelihood of induced abortion.
Source: *** → P < 0,001.
Partnership status, parity, and employment display consistent associations with the likelihood of IA. Partnership status, in particular, remains a strong correlate; although the magnitude of the effect attenuates slightly across models – from 2.258 in Model 1 to 2.176 in Model 3 – the association remains stable, with women without a partner consistently exhibiting higher odds of IA. Parity also shows a clear gradient, as the odds of IA increase progressively with the number of children, reaching an OR of 5.278 among women with three or more children in the fully adjusted model. Employment status follows the same pattern, with inactive or unemployed women displaying a modest but consistent elevation in the odds of IA.
The inclusion of additional socio-economic and contextual controls in Model 3 provides a broader view of the factors associated with IA likelihood. Women with secondary education or less show higher odds of IA than those with higher education (OR = 2.665). Regarding migration status, most immigrant groups exhibit higher odds of IA compared to women born in Spain – peaking among those from the Rest of America (OR = 1.897) – while women from North Africa show a lower likelihood (OR = 0.515). A higher viability of healthcare centres providing abortion is positively associated with IA. Finally, pregnancies conceived in 2015, 2016, and 2019 show higher odds relative to the 2011 baseline, despite some annual fluctuations.
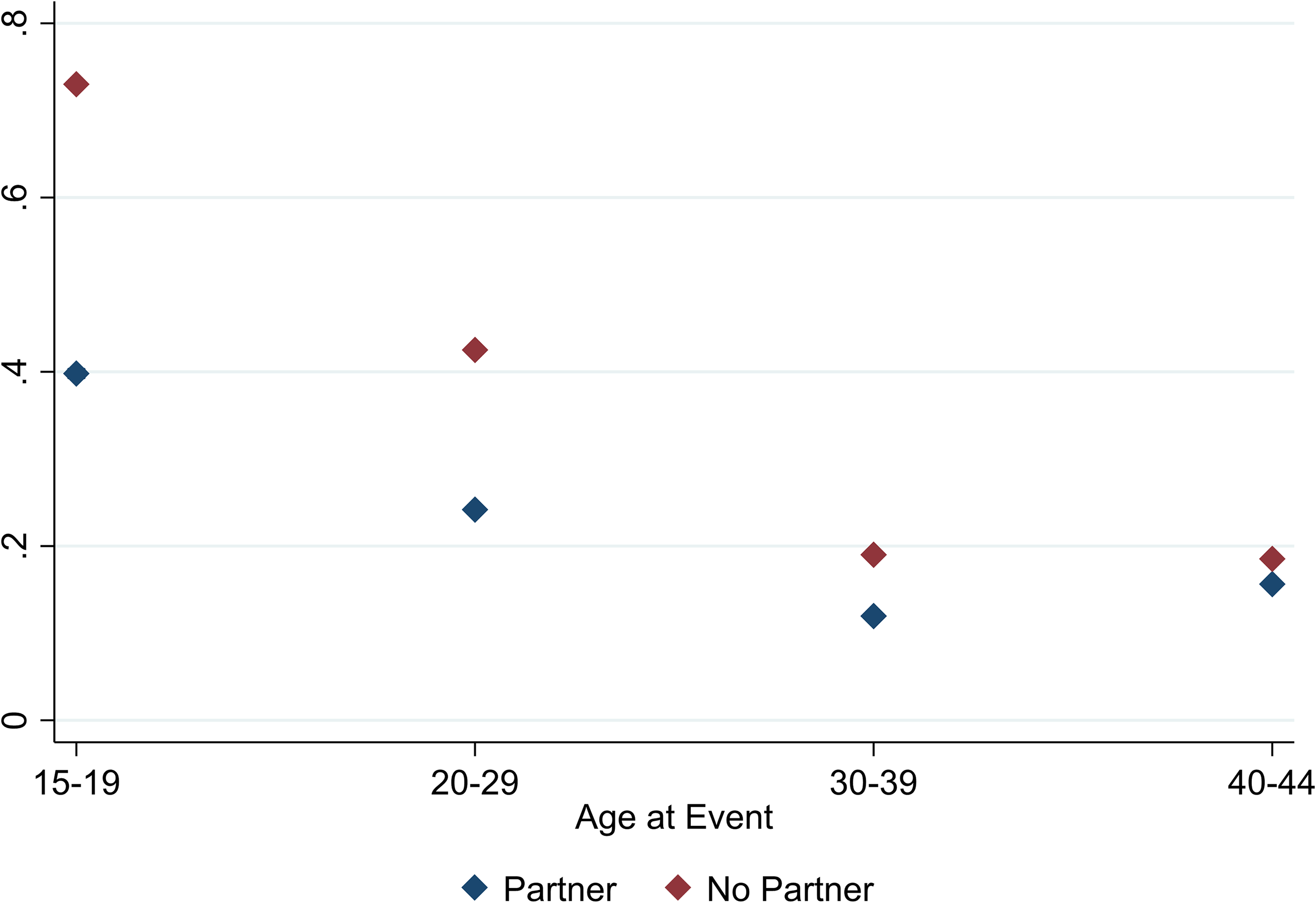
Figures 2–4 present the results of the probabilistic models predicting the likelihood of a pregnancy ending in an IA, incorporating an interaction term between the main predictors and age group. As shown in Figure 2, the effect of partnership status varies markedly by age and is strongest at younger ages. Among women aged 15–19 years, the predicted probability of an IA is substantially higher for those without a partner (73.0%) than for those with a partner (39.8%). This gap narrows progressively with age – 42.5% versus 24.2% at ages 20–29 years, and 19.0% versus 12.0% at ages 30–39 years, the lowest probabilities observed. By ages 40–44 years, predicted probabilities converge further (18.5% without a partner; 15.6% with a partner), indicating a diminished role of partnership status in late reproductive years.
Predicted probabilities of induced abortion by partnership and age.

The model including an interaction between parity and age group shows that parity is a strong and consistent predictor of IA across different ages (Figure 3). In all age categories, the predicted probability of IA increases steadily with the number of existing children. The highest probability in the study is observed among women aged 15–19 years with three or more children (88%). Although predicted probabilities decline with age, the gap by parity remains substantial. For example, among women aged 30–39 years, the probability is lowest for those with no children (8%) and remains markedly higher for those with three or more children (36%). In the oldest group (40–44 years of age), the likelihood of IA remains elevated among women with two or more children, indicating that once a desired family size is reached or exceeded, parity continues to shape abortion decisions irrespective of age.
Predicted probabilities of induced abortion by number of offspring and age.

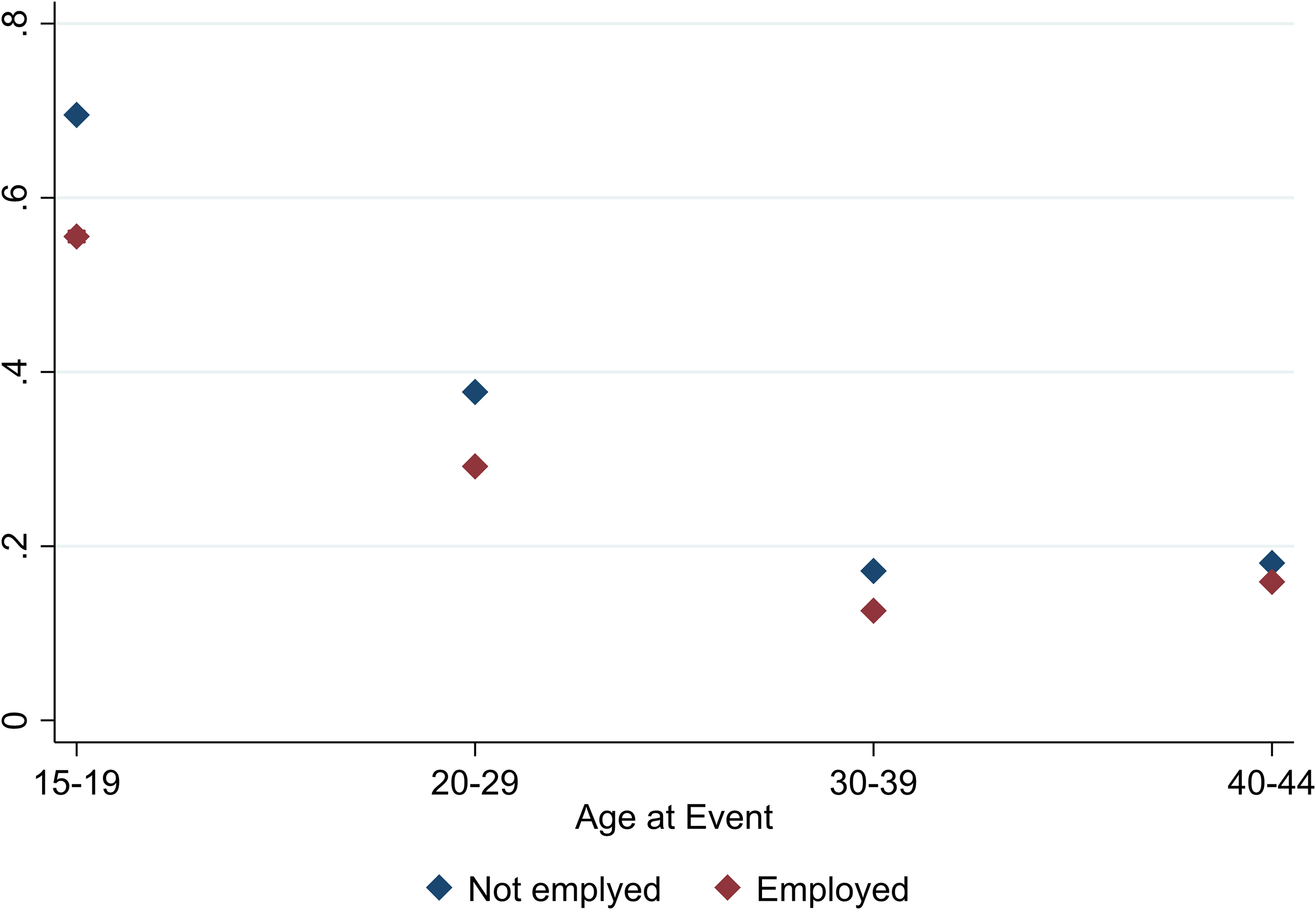
The model incorporating an interaction between employment status and age shows that being outside the labour market is associated with a higher likelihood of IA, although the magnitude of this effect varies across nearly all age groups (Figure 4). Among the youngest (15–19 years of age), non-employed women have a predicted probability of 70%, compared to 55.7% for employed peers – the largest gap observed. With increasing age, predicted probabilities decline for both groups, and the disparity narrows: 8.6 percentage points in the 20–29 age group and 4.5 in the 30–39 age group, with non-employed women remaining more likely to have an IA. In the 40–44 age group, the difference is no longer significant.
Predicted probabilities of induced abortion by employment status and age.

Discussion
This study confirmed the importance of a woman’s age in determining whether a pregnancy ends in IA or not (Sihvo et al., Reference Sihvo, Bajos, Ducot and Kaminski2003; Santelli et al., Reference Santelli, Speizer, Avery and Kendall2006). Not only do the descriptive data show a higher percentage in younger age groups, but this is also confirmed by the results of the multivariate analysis. This finding is consistent with previous research showing that adolescents and young women are more likely to opt for an abortion due to lower levels of economic independence, educational and employment aspirations, and social stigma around early motherhood (Bankole et al., Reference Bankole, Singh and Haas1998; Santelli et al., Reference Santelli, Speizer, Avery and Kendall2006). In addition, these results may be also attributed to an increase in sexual activity, an earlier age of sexual initiation, and a larger number of sexual partners (de Sanjose et al., Reference de Sanjose, Cortés, Méndez, Puig-Tintore, Torné, Roura, Bosch and Castellsague2008).
The likelihood of IA was also increased among women who are older and closer to the end of their reproductive years, which is consistent with other studies that have associated it with different reasons such as not wanting to have more children, being unable to afford to have a child, being too old, or the work situation (Santelli et al., Reference Santelli, Speizer, Avery and Kendall2006; Zurriaga et al., Reference Zurriaga, Martínez-Beneito, Galmés Truyols, Torne, Bosch, Bosser and Portell Arbona2009; Chae et al., Reference Chae, Desai, Crowell and Sedgh2017). Notably, the probability of undergoing an IA was lower in the 30–39 age group than in the other age groups. Women commonly choose to be mothers in this stage of life, and the largest number of births occur in this age group (INE, 2022). The results reinforce the idea, highlighted by Seiz et al. Reference Seiz, Castro-Martín, Cordero-Coma and Martín-García(2022) that this age range reflects not only biological optimality but also social expectations and economic planning regarding motherhood.
However, the most salient finding is the age-dependent nature of sociodemographic effects. Although the absence of a partner is associated with a higher likelihood of IA at all ages – consistent with previous research (Sihvo et al., Reference Sihvo, Bajos, Ducot and Kaminski2003; Chibber et al., Reference Chibber, Biggs, Roberts and Foster2014) – this effect is strongest during adolescence. Among women aged 15–19 years, the absolute difference in predicted probabilities reaches 33.2 percentage points. With increasing age, both the gap between groups and the overall probability of IA decline, becoming realtively small although still statistically significant in the 40–44 age group.
The number of prior children is a key determinant of IA likelihood, generally increasing the predicted probability as parity rises. However, its effect varies by age. Women aged 30–39 years with zero or one child show the lowest probabilities, possibly reflecting that they have not yet reached their desired family size or maternal goals (Väisänen and Batyra, Reference Väisänen and Batyra2022). In contrast, among women aged 40–44 years, the likelihood rises sharply from the second child, suggesting a desire to conclude childbearing after achieving the culturally typical family size of two in Spain (Castro et al., Reference Castro Martín, Martín García, Cordero and Seiz2020). The highest probability occurs among adolescents (15–19 years of age) with three or more children (≈88%). These results confirm that parity strongly predicts IA decisions, though its meaning shifts across life stages.
Finally, employment status also influences the likelihood of a pregnancy ending in IA, with this relationship clearly varying by age. Among younger women, those who are inactive or outside the labour market are more likely to have an abortion than those who work. This disparity likely reflects that, for adolescents and women in their twenties, being non-employed often coincides with full-time education or economic instability. Finer et al. (Reference Finer, Frohwirth, Dauphinee, Singh and Moore2005) highlight that the desire to complete education and the perception of being unprepared for the financial demands of motherhood are key drivers of IA, making the lack of a stable income a critical barrier to childbearing. In addition, among older women, being outside the labour market makes little difference in the likelihood of abortion compared to those who are employed. This pattern is consistent with findings from Helfferich et al. (Reference Helfferich, Hessling, Klindworth and Wlosnewski2014), who highlight that older women may prioritise motherhood despite adverse economic conditions, driven by the perception that their reproductive window is closing. Therefore, the biological limitations to fertility play an important role, in the sense of ‘now-or-never’, which overrides the subjective impact of unfavourable circumstances.
Limitations
The present study has several limitations that are important to note. The main limitation is that, despite the overall aim of the source databases to cover all conceptions, this aim was often not fulfilled due to the exclusion of miscarriages. Not only are miscarriage events not recorded when they occur before week 22 or 500 g of weight, but they also often go unnoticed by the women themselves. Moreover, in the process of merging multiple records, certain variables, such as marital status or employment status, lose quality in the description because they were not originally coded with the same labels.
Another aspect to bear in mind is that, despite having all the pregnancies recorded, information that would tell whether the pregnancy was intended or unintended is lacking. It is assumed that all those that ended in IA were, but it is not known which of those that ended in another term were.
Additionally, information on the women’s socio-economic status – such as their social class – was not available. As a result, educational level was used as a proxy indicator of socio-economic status. This is a common approach in research, as education is generally stable over time and less affected by variables such as age or employment status. However, the Voluntary Termination of Pregnancy Statistics database does not collect information on the women’s partners, including their employment status, income, or educational attainment. This lack of data limited the ability to examine the potential influence of these partner-related factors.
Conclusions
This is the first Spanish study that examines abortion, in comparison to other pregnancies, placing the focus on the age of women. The results show that sociodemographic characteristics play a very important role in whether a pregnancy ends in IA, and that these vary according to the woman’s age. The findings of this study provide a critical empirical basis for refining sexual and reproductive health policies in Spain.
First, the analysis indicates that among younger women, the absence of a partner and economic inactivity are strongly associated with IA. In the Spanish context – characterised by high labour market instability among youth and comparatively late residential emancipation – a pregnancy may coincide with ongoing educational and early career trajectories (Alderotti et al., Reference Alderotti, Vignoli, Baccini and Matysiak2021; Del Rey et al., Reference Del Rey, Stanek and García-Gómez2023). From a policy perspective, this suggests that strategies should extend beyond clinical access to include comprehensive sex education and guidance related to the transition to independent adulthood. Expanding access to free Long-Acting Reversible Contraception (LARC) for this age group may also be particularly relevant, given that the results point to a wider gap in IA probability between women with more and less stable socio-economic circumstances during these years.
Second, a significant finding is that among women over 40 years of age, IA is less associated with partnership status and more with prior parity. The sharp increase in IA probability among women with two or more children suggests that IA may function as a mechanism for managing reproductive goals once the culturally prevalent two-child norm in Spain has been reached (Brinton et al., Reference Brinton, Bueno, Oláh and Hellum2018). Accordingly, public health interventions for this group could shift from general pregnancy prevention to family-size management, including targeted postpartum or post-abortion counselling for women over 35 years of age and ensuring access to permanent or highly effective contraceptive methods to reduce unintended pregnancies after family goals are fulfilled.
Finally, while this study identifies the sociodemographic profiles associated with IA, further investigation is needed to delve into the subjective reasons behind these decisions. The multidimensional nature of termination – which often involves a complex combination of economic, relational, and personal factors – suggests that future research should incorporate the role of the partner and the duration of the relationship. Qualitative studies are necessary to complement these quantitative findings and provide a deeper understanding of the decision-making process across different ages, ensuring that reproductive health services remain responsive to the diverse realities of women in Spain.
Financial support
This publication is part of the R&D&I project PID2021-128108OB-I00, funded by MCIN/AEI/10.13039/501100011033/ and FEDER, ‘A way to make Europe’.
Competing interests
The authors report there are no competing interests to declare.
Ethical standard
The protocol of this research was reviewed and approved by the Research Ethics Committee of the University of Salamanca and complied with the ethical requirements necessary for its execution (registration number 919; February 14, 2023).



 Open access
Open access