


Background
Out-of-hospital cardiac arrest (OHCA) is a major public health problem and remains one of the leading causes of death world-wide. According to data from the European Resuscitation Council (ERC; Niel, Belgium), the overall survival rate for OHCA cases is reported to be approximately 7.5%. Reference Baldi, Wnent and Caputo1 Similarly to Europe, in the United States, the overall survival rate after OHCA has been reported to be 10.5%, with favorable neurological survival documented in 8.2%. Reference Del Rios, Bartos and Panchal2 In witnessed OHCA cases, early initiation of cardiopulmonary resuscitation (CPR) incorporating high-quality chest compressions is a key determinant of survival. Reference Kragholm, Wissenberg and Mortensen3 Large-scale studies such as the European Registry of Cardiac Arrest (EuReCa) have demonstrated that a substantial proportion of OHCA events are witnessed by untrained laypersons. Nevertheless, these studies emphasize that bystander CPR rates in witnessed cases remain below the aimed level. Reference Gräsner, Wnent and Herlitz4–Reference Wnent, Masterson and Maurer6 As in Europe, the rates of CPR initiation at the scene in the United States remain well below the aimed levels (58% versus 41.7%). One of the primary underlying reasons for this disparity is insufficient knowledge among bystanders. Reference Baldi, Wnent and Caputo1,Reference Del Rios, Bartos and Panchal2
In witnessed OHCA cases, lay rescuers activate the Emergency Medical Services (EMS) by contacting the emergency dispatch center. Telephone-assisted cardiopulmonary resuscitation (T-CPR), defined as the provision of CPR guided by verbal instructions from the dispatcher after recognition of cardiac arrest, has been shown in numerous studies to increase bystander CPR rates and to have a positive impact on survival outcomes. Reference Dezfulian, Cabañas and Buckley7–Reference Ringh, Rosenqvist and Hollenberg10 However, T-CPR has certain operational difficulties naturally. The dispatcher provides guidance based solely on auditory feedback and is therefore unable to directly assess key quality indicators of chest compressions, such as depth, rate, and complete chest recoil. Reference Dezfulian, Cabañas and Buckley7,Reference Plata, Nowack and Loeser8,Reference Szöllősi, Horváth and Németh11
These limitations have led to increasing interest in integrating visual communication technologies into emergency dispatch systems in recent years. In this context, video-assisted cardiopulmonary resuscitation (V-CPR) enables dispatchers to visually assess the rescuer’s performance and provide real-time corrective feedback. Reference Dezfulian, Cabañas and Buckley7,Reference Szöllősi, Horváth and Németh11 Recent studies suggest that V-CPR may improve chest compression quality and potentially lead to better clinical outcomes. Therefore, V-CPR systems are considered a more advanced model of remote guidance compared with conventional T-CPR. Reference Lin, Chiang and Hsieh12–Reference Bielski, Böttiger and Pruc14
Data regarding how effectively real-time video guidance can improve CPR performance in completely untrained individuals remain limited. In particular, the impact of visual guidance on key quantitative CPR quality parameters—such as compression rate, total number of compressions, and adherence to guideline-recommended targets—has not yet been clearly established. Reference Lin, Chiang and Hsieh12–Reference Bielski, Böttiger and Pruc14
The primary rationale for conducting this study was to provide untrained lay rescuers with a functional, low-barrier, real-time skill transfer during the critical early minutes of CPR, conceptualized as just-in-time guidance. Although community-based CPR training programs represent a sustainable long-term solution, their real-world effectiveness is limited by restricted training coverage and inconsistent participation in refresher courses. Even among trained individuals, confidence may decline over time, leading to increased hesitation to initiate resuscitative efforts.
Within this framework, the present study aimed to objectively evaluate the effect of real-time video guidance on CPR performance quality in untrained individuals using measurable performance metrics. In this model, the dispatcher provides live visual guidance by simultaneously performing CPR on a manikin during the video call, allowing immediate observational transfer of correct procedural steps and facilitating real-time corrective feedback.
The primary hypothesis of this study is that real-time visual guidance will enable a higher proportion of chest compression rates and total compression counts to fall within guideline-recommended ranges, thereby significantly improving overall CPR quality parameters. This study specifically evaluates a live, bidirectional video guidance model in which the dispatcher simultaneously demonstrates CPR on a manikin, unlike previous studies that relied solely on verbal or passive visual instruction. In this regard, the study aims to fill a critical gap in the literature on remote-guided CPR applications by examining the effect of video-guided guidance systems on untrained rescuers through quantitative quality indicators.
Methods
Study Design and Ethical Approval
This study was designed as a prospective, randomized, controlled, single-blind manikin-based trial. The study protocol was approved by the Ordu University (Ordu, Turkey) Faculty of Medicine Clinical Research Ethics Committee (Decision No: 2024/159, dated November 8, 2024). The study was conducted from April 2025 through May 2025 and was performed in accordance with the principles of the Declaration of Helsinki and the Good Clinical Practice guidelines.
Participants and Group Assignment
Volunteer university students aged 18 years and older with no prior training in Basic Life Support (BLS) or Advanced Life Support (ALS) were enrolled in the study. Written informed consent was obtained from all participants.
The exclusion criteria were prior CPR/BLS/ALS training, the presence of musculoskeletal conditions that could limit the performance of chest compressions, and withdrawal from the study.
Equipment and Technical Infrastructure
All call guidance was provided by a single dispatcher. A standardized smartphone model was used for both the dispatcher and all participants: iPhone 15 (Apple Inc.; Cupertino, California USA, 2024; iOS version 18.4.1). For both the voice call and video call groups, the audio and video calling features of the FaceTime application (Apple Inc.) were utilized.
Smartphone Positioning
The smartphone was placed on a small, inclined wooden stand positioned adjacent to the participant, who knelt beside the CPR manikin. In both groups, the smartphone was mounted on a fixed stand and handheld use was not permitted. The stand was oriented to provide a clear view of the chest compression area and hand placement during CPR performance.
Study Protocol and Intervention
Participants were presented with a witnessed adult OHCA scenario, and the study protocol commenced at the stage of contacting the emergency call center, which is a key step in the BLS algorithm. The dispatcher’s phone number was pre-registered on all participants’ smartphones as “EMS” and call initiation was standardized to a single-touch action. The start time of the study was defined as the moment the emergency call button was pressed.
The protocol applied in the voice call and video call groups was identical except for the mode of communication. The duration of CPR was standardized to five minutes in both groups, and all participants performed hands-only CPR.
In the T-CPR group, the dispatcher guided the participants exclusively through verbal instructions. Participants were instructed sequentially to:
-
Place the thenar eminence of the dominant hand on the lower half of the sternum along the midline;
-
Place the other hand on top of the first hand with fingers interlocked;
-
Keep the arms straight and perpendicular to the chest;
-
Perform chest compressions at a depth of five-to-six centimeters and a rate of 100-120 compressions per minute; and
-
Continue compressions without removing the hands from the chest.
In the V-CPR group, the dispatcher visually observed the participant via the FaceTime application and simultaneously performed CPR on a manikin positioned in front of the dispatcher, in real time and in synchrony with the participant. During this process, the dispatcher provided the same verbal instructions as in the T-CPR group and additionally demonstrated these instructions visually on the manikin. Real-time visual feedback was provided by simultaneously demonstrating:
-
Correct hand placement;
-
Appropriate body positioning; and
-
Adequate compression depth and rate.
In both groups, the CPR technique—including chest compression location, depth (five-to-six centimeters), rate (100-120 compressions per minute), and body positioning—was standardized in accordance with the adult BLS guidelines of the ERC and the American Heart Association (AHA; Dallas, Texas USA). Reference Olasveengen, Semeraro and Ristagno15,Reference Panchal, Bartos and Cabañas16
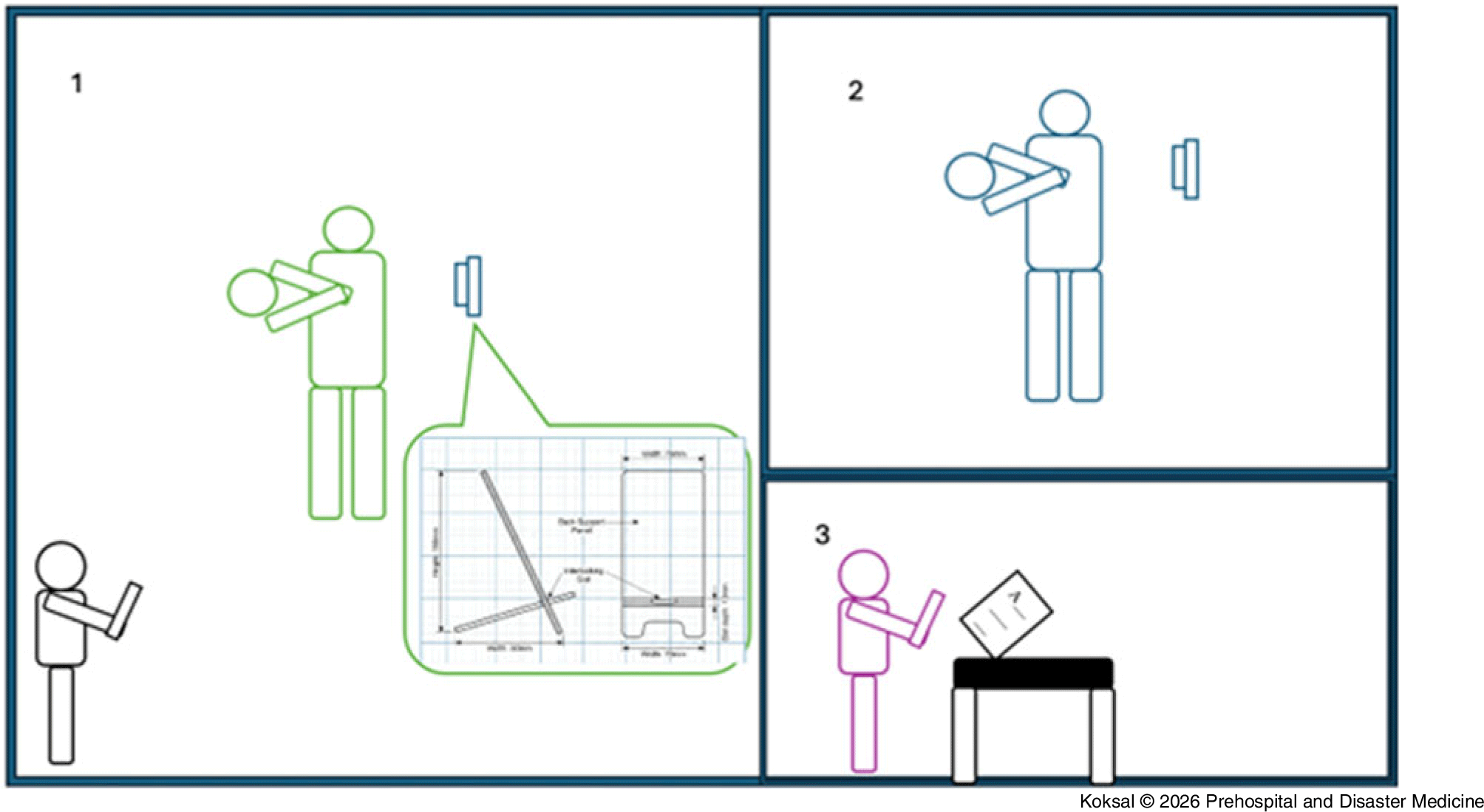
A schematic overview of the study workflow and participant-observer configuration is presented in Figure 1.
Study Workflow and Participant-Observer Configuration.
Note: The schematic illustrates the stepwise study workflow. A lay participant kneels beside the CPR manikin and initiates the emergency call using a smartphone placed on a fixed, inclined stand positioned to visualize the chest compression area and hand placement. A single dispatcher provides standardized guidance via the same smartphone model; participants receive either voice-only instructions or real-time video guidance. In the video-guided arm, the dispatcher visually observes the participant and delivers corrective feedback during CPR. Data from CPR performance are automatically recorded by the manikin’s integrated feedback system and independently extracted by a third investigator located in a separate room, who is blinded to group allocation.
Abbreviation: CPR, cardiopulmonary resuscitation.

CPR Simulation Equipment
Participant CPR performance was conducted using a Laerdal Resusci Anne Advanced Skill Trainer manikin (Laerdal Medical; Stavanger, Norway). The manikin was equipped with an integrated feedback system capable of measuring chest compression rate, depth, accuracy of hand placement, and overall CPR quality parameters. Data were recorded via the manufacturer-provided integrated tablet/feedback module (SimPad PLUS; Laerdal Medical AS, manufactured in Taiwan, 2015; software version 6.3.2.51-Plus).
Dispatcher CPR performance was also conducted on a Laerdal Resusci Anne Advanced Skill Trainer manikin (Laerdal Medical).
Instructions and Data Collection
The research team consisted of three investigators. The first investigator was positioned next to the participant and was responsible for issuing the start command and recording two separate time intervals: the time from the start command to initiation of the EMS call, and the time from EMS connection to the initiation of chest compressions.
The second investigator, who served as the dispatcher, delivered the CPR instructions to both the voice call and video call groups using a standardized instruction form. For the video call group, additional visual guidance was provided by simultaneously performing CPR on a separate manikin positioned in front of the dispatcher. Visual support focused on correct hand placement; alignment of the hands, elbows, and shoulders; chest compression rate, chest compression depth, and allowance for adequate chest wall recoil.
The third investigator, located in a separate room and blinded to group allocation, recorded the data obtained from the CPR manikin’s data logging system.
Outcomes
The primary outcome of this study was the CPR Quality Score, a composite measure automatically generated by the manikin system. This score integrates multiple dimensions of resuscitation performance, including compression depth, compression rate, correct hand positioning, full chest recoil, and minimization of interruptions. The CPR Quality Score was pre-specified as the main outcome, as it reflects overall CPR quality in alignment with current resuscitation guidelines.
Secondary exploratory outcomes were defined as: Time from case recognition to EMS call; Time from EMS call to initiation of CPR; Total number of compressions; Duration of CPR (min); Mean compression rate (compressions/min); Proportion of compressions at correct rate (%); Mean compression depth (mm); Proportion of compressions with full chest recoil (%); Proportion of compressions with adequate depth (%); Correct hand position; and Mean interruption time between compressions (s). These variables were considered exploratory and hypothesis-generating.
Statistical Analysis
Statistical Sim Pad analyses were performed using SPSS (version 30; IBM Corp.; Armonk, New York USA) and R (version 4.5.0; R Foundation for Statistical Computing; Vienna, Austria). Continuous variables were summarized as mean (standard deviation [SD]) or median (interquartile range [IQR]), depending on distribution, and categorical variables as frequencies and percentages (%).
Normality of continuous variables was assessed using the Shapiro-Wilk test (Supplementary Table 1). For comparisons between the T-CPR and V-CPR groups, normally distributed variables were analyzed using the independent-samples t test, and non-normally distributed variables were analyzed using the Mann-Whitney U test.
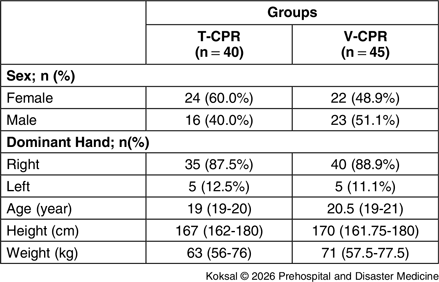
Demographic Data

Abbreviations: CPR, cardiopulmonary resuscitation; T-CPR, telephone-assisted CPR; V-CPR, video-assisted CPR.
The primary outcome, CPR Quality Score, and secondary CPR-related performance variables were compared between groups using two-sided tests at an α level of 0.05. Results of group comparisons are presented as mean differences or Hodges-Lehmann median differences with corresponding 95% confidence intervals.
To examine whether group allocation was independently associated with CPR performance, multivariate robust regression analysis with heteroscedasticity-consistent standard errors (HC3) was performed. Multivariate robust regression analysis was performed separately for each CPR performance outcome to evaluate the independent association between group allocation and outcome measures while adjusting for age, sex, dominant hand, height, and weight. Regression results are reported as coefficients (β), standard errors (SE), and 95% confidence intervals.
No adjustment for multiple comparisons was performed for exploratory secondary outcomes; therefore, confidence intervals for these outcomes are unadjusted.
Power analysis revealed that to detect a large effect size (Cohen’s effect size = 0.68) with α = 0.05 and 1-β = 0.91 power, a minimum of 40 participants per group was required for the study comparing T-CPR and V-CPR groups. This assumed effect size was informed by prior simulation-based research indicating substantial performance differences between video- and telephone-assisted CPR modalities. Reference Szöllősi, Horváth and Németh11
Results
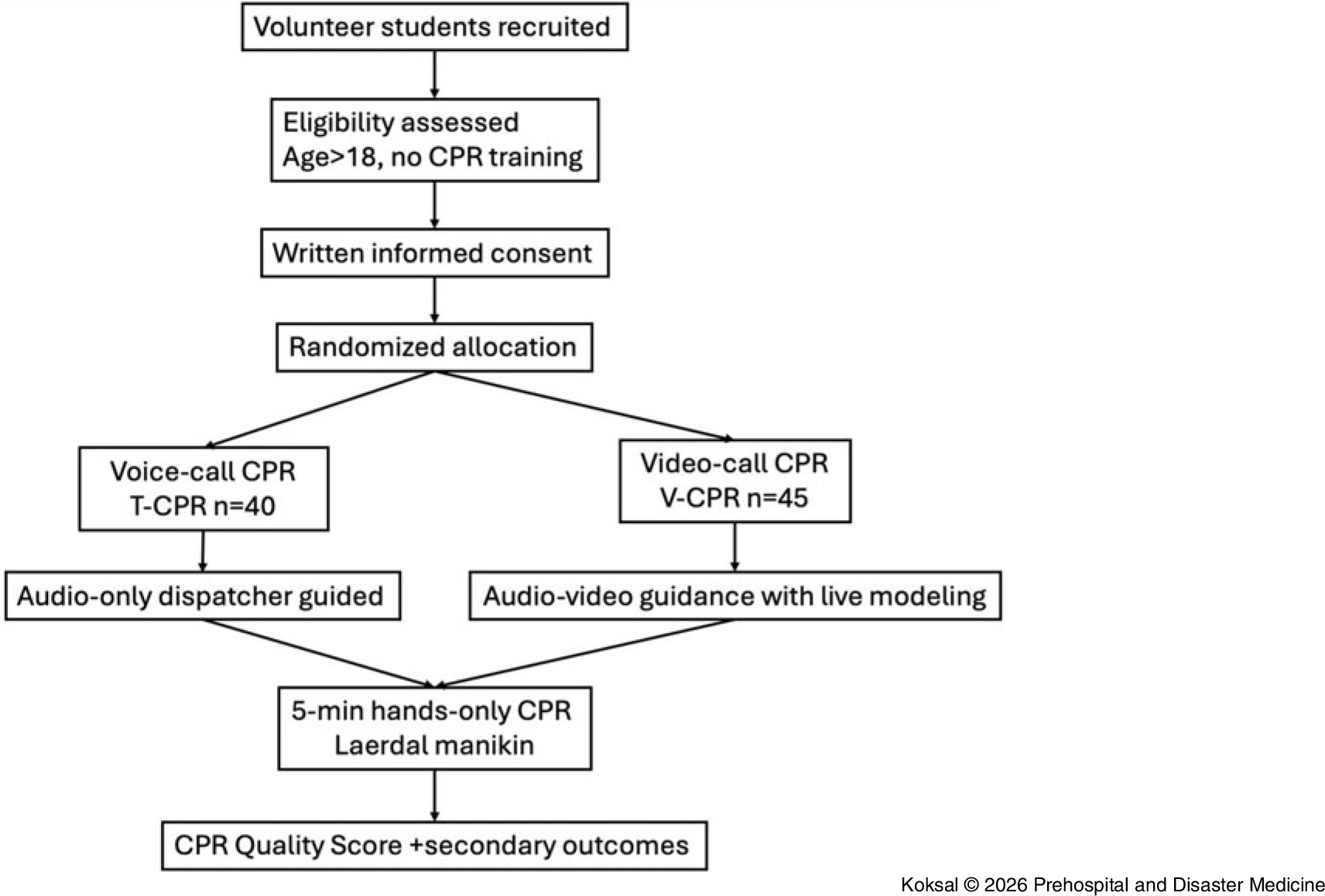
A total of 85 participants were included in the study, with 40 in the T-CPR group and 45 in the V-CPR group. The mean age of participants was 20.13 (SD = 1.81) years, and 54.1% were female. Demographic characteristics were similar between groups. The demographic profile of the study sample is summarized in Table 1. A flowchart of the study process is presented in Figure 2.
Study Flowchart.
Abbreviation: CPR, cardiopulmonary resuscitation.

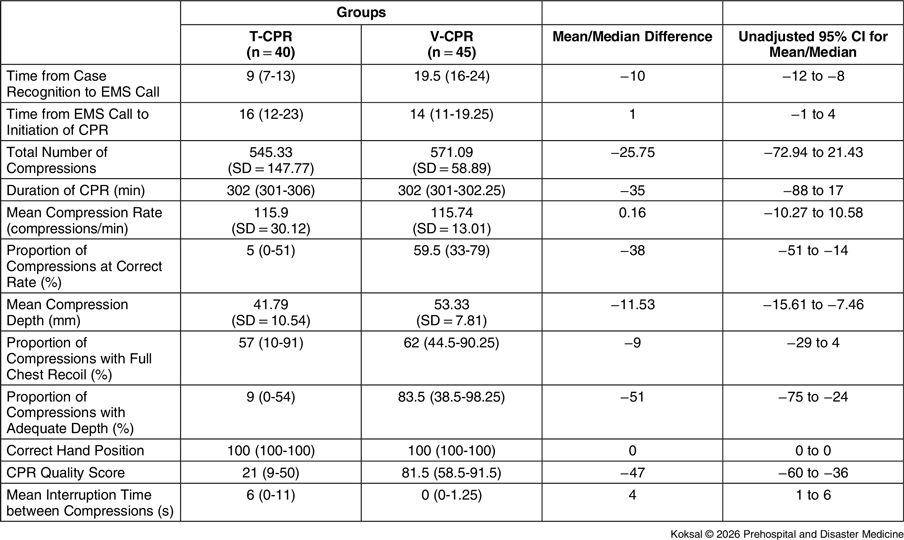
The pre-specified primary outcome, CPR Quality Score, was significantly higher in the V-CPR group than in the T-CPR group (median difference −47; 95% CI, −60 to −36; P < .001).
Among CPR performance measures, the V-CPR group demonstrated significantly greater mean compression depth (mean difference −11.53 mm; 95% CI, −15.61 to −7.46); higher proportions of compressions at the correct rate (median difference -38; 95% CI, -51 to -14); and higher proportions of compressions performed at adequate depth (median difference −51; 95% CI, −75 to −24).
In addition, interruption time between compressions was shorter in the V-CPR group (median difference four seconds; 95% CI, 1 to 6). The T-CPR group demonstrated shorter time from case recognition to EMS call (median difference −10; 95% CI, −12 to −8).
No statistically significant differences were observed between groups for time from EMS call to CPR initiation, total number of compressions, total CPR duration, mean compression rate, proportion of compressions with full chest recoil, or correct hand position. The relationships between CPR-related variables across different groups are summarized in Table 2.
Relationships between CPR-Related Variables Across Groups

Note: Values are presented as mean (SD), median (IQR), or n (%). The widths of the confidence intervals have not been adjusted for multiplicity, and they should not be used in place of hypothesis testing.
Abbreviations: CPR, cardiopulmonary resuscitation; EMS, Emergency Medical Services; IQR, interquartile range; SD, standard deviation; T-CPR, telephone assisted CPR; V-CPR, video assisted CPR.
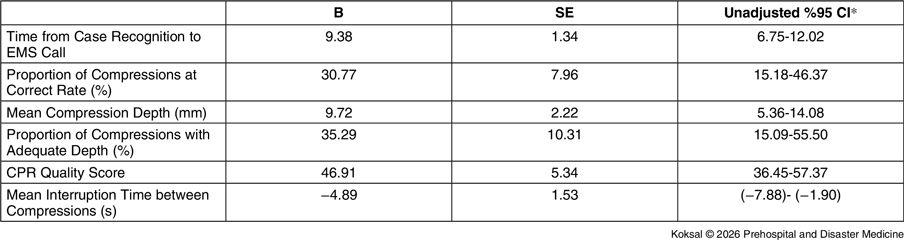
Multivariate robust regression analysis confirmed that allocation to the V-CPR group remained independently associated with higher CPR Quality Score, greater compression depth, higher proportions of compressions at the correct rate and adequate depth, and shorter interruption times between compressions after adjustment for age, sex, dominant hand, height, and weight. The results of the multivariate robust regression analysis are presented in Table 3.
Multivariate Robust Regression Analysis

Note: The widths of the 95% confidence intervals have not been adjusted for multiplicity, and they should not be used in place of hypothesis testing.
Abbreviations: B, regression coefficient; CI, confidence interval; CPR, cardiopulmonary resuscitation; EMS, Emergency Medical Services; SE, standard error.
Discussion
In this randomized, single-blind simulation study, V-CPR was associated with a significantly higher CPR Quality Score in untrained participants compared with T-CPR, the primary outcome of the study (median difference −47; 95% CI, −60 to −36; P < .001). The CPR Quality Score uses a deductive (subtractive) algorithm that integrates compression depth, compression rate, complete chest recoil, hand position, and compression fraction into a single percentage-based score, with deviations from target parameters resulting in score reductions. Reference Arif, Arif and Fasciglione17 The quality scores derived from the manikin’s built-in performance assessment system, which are based on CPR performance parameters, have been widely and reliably used in educational research and are grounded in guideline-defined targets for compression depth and rate. Reference Molinari, Galimberti and da Silva18–Reference Starks, Blewer and Chow20 In the literature, studies comparing video call-assisted and voice call-assisted CPR, similar to the current study design, have reported higher CPR quality scores in the video call group compared with the voice call group. Reference Ecker, Wingen and Hamacher21
A review of the literature indicates that, compared with the V-CPR group, the T-CPR group has a shorter interval from call initiation to the start of CPR. Accordingly, T-CPR has been reported to be associated with earlier initiation of CPR, with this time difference being statistically significant. Reference Lin, Chiang and Hsieh12,Reference Bolle, Scholl and Gilbert22–Reference Stipulante, Delfosse and Donneau24 Review of the methodologies of existing studies shows that the interval from call initiation to the start of CPR has generally been evaluated as a single composite time period. In contrast, in this study, this interval was divided into two distinct phases: first, the time from call initiation to call connection by the dispatcher, and second, the time from call connection to the initiation of CPR. The primary rationale for separating this interval into two components was the hypothesis that delays in the total time to CPR initiation might predominantly be attributable to the call connection phase. The literature suggests that faster call connection in voice calls is closely related to bandwidth availability and telecommunication speed, and that operational delays exist between voice and video calls. Reference Kuhn, Mamede and van den Berg25 In the present study, analysis of the time intervals to reach the EMS demonstrated that call connection times were shorter in the voice call group, and this difference was statistically significant. However, when the interval from the initial establishment of communication—whether by voice or video—until the initiation of CPR was examined, no statistically significant difference was observed between the two groups. As highlighted in previous studies, Reference Lin, Chiang and Hsieh12,Reference Bolle, Scholl and Gilbert22–Reference Kuhn, Mamede and van den Berg25 combining these time intervals between two parts may be misleading. Moreover, it is anticipated that with on-going technological advancements, the access-related delays between video and voice calls will continue to decrease, and that improvements in communication infrastructure will likely eliminate this gap in the foreseeable future, enabling faster and more efficient connectivity.
In this study, no statistically significant difference was observed between the two groups in terms of the total number of chest compressions. However, analysis of mean compression depth and the proportion of compressions performed at an adequate depth demonstrated superior performance in the V-CPR group. Although the findings share several similarities with those reported in previous studies, some notable differences are evident in the literature. Prior investigations have shown that the video call group demonstrates a modest advantage over the voice call group in terms of mean compression depth and the proportion of compressions performed at an adequate depth. Reference Szöllősi, Horváth and Németh11,Reference Lin, Chiang and Hsieh12,Reference Bielski, Böttiger and Pruc14,Reference Pan, Li and Ji26 Consistent with these reports, the current study likewise demonstrated that these parameters were statistically superior in the V-CPR group. The primary reason for this difference may be attributed to a key methodological distinction of the study: unlike previous investigations, the dispatcher simultaneously performed CPR on a manikin together with the rescuer. The main advantage of this approach is that it allows real-time correction of chest compression technique through direct visual demonstration. In the current study, analysis of the proportion of chest compressions delivered at the correct rate demonstrated superior performance in the V-CPR group. Consistent with previous studies, the V-CPR group demonstrated a significantly higher proportion of chest compressions performed at the correct rate. Reference Szöllősi, Horváth and Németh11,Reference Bielski, Böttiger and Pruc14,Reference Pan, Li and Ji26,Reference Kim, Kim and Park27 Additionally, analysis of interruption times between chest compressions revealed that the V-CPR group had shorter pause durations, with the difference being statistically significant. Previous studies have reported that compression interruptions are less frequent in the V-CPR group, demonstrating superiority over the voice call group, Reference Lee, Jeon and Ahn23,Reference Pan, Li and Ji26–Reference Li, Yang and Chang28 similarly to the results of the present study. In contrast, some studies have also reported longer CPR interruption durations in the V-CPR groups. Reference Szöllősi, Horváth and Németh11,Reference Lin, Chiang and Hsieh12,Reference Yang, Wang and Chiang29 The heterogeneity in the findings reported in the literature may be explained by the additional cognitive load imposed by standard video-guided CPR, including tasks such as camera placement, smartphone positioning, visual adjustment, and interpretation of instructions, all of which may prolong no-flow time. No complications were observed during the course of the study (eg, no call drops, video freezes, or audio disruptions during the simulation sessions). In this way, in the proposed model, the instructor continuously maintained the compression pattern on a manikin without interruption, thereby providing rhythm synchronization that helped prevent pauses by the participant. Accordingly, the findings suggest that the benefit of video technology lies not merely in the presence of visual input, but in its integration within a structured and operationally optimized guidance protocol. Although some studies have reported superior correct hand positioning in the V-CPR group compared with the T-CPR group, Reference Lee, Jeon and Ahn23,Reference Ecker, Lindacher and Adams30 the study did not demonstrate a statistically significant difference between the two groups. This finding is likely attributable to the fact that participants in both groups achieved accurate hand placement, resulting in no relative advantage for either intervention.
To improve survival rates in OHCA and enhance resuscitation quality delivered by lay rescuers, the integration of wearable technologies into dispatcher-assisted BLS has been increasingly considered. Pilot studies have demonstrated that video streaming via smart glasses may improve bystander performance compared with telephone-based instructions. Reference Aranda-García, Barrio-Cortes and Fernández-Méndez31,Reference Barcala-Furelos, Aranda-García and Otero-Agra32 Smart glasses may be particularly advantageous for V-CPR by eliminating the need to hold a camera device. Their hands-free functionality allows rescuers to focus on chest compression technique while simultaneously transmitting a real-time first-person visual feed to the dispatcher, potentially reducing common smartphone-related issues such as loss of camera angle, device displacement, and inadequate visualization of the CPR area. Reference Kebapci, Ozkaynak and Bowler33,Reference Aranda-García, Otero-Agra and Fernández-Méndez34 Beyond CPR, smart glasses have also been explored as a communication tool within EMS systems, including applications such as ambulance-to-hospital coordination. Reference Apiratwarakul, Cheung and Ienghong35,Reference Zhang, Bai and Xu36 However, widespread implementation is currently limited by factors such as cost, device accessibility, battery sustainability, and user familiarity. Given the higher prevalence of smartphone use in the general population, smartphones are likely to remain the primary platform for video-assisted guidance in the near term. Nevertheless, as wearable technologies become more widespread—particularly in outdoor and resource-limited settings—smart glasses may become a viable alternative. In this context, the “simultaneous applied visual model” used in this study could be adapted to smart glass-based systems, potentially enabling a more ergonomic and less interruption-prone dispatcher-assisted CPR protocol. For widespread practical implementation, factors such as accessible connectivity, user acceptance, and integration into emergency dispatch workflows are critical. Looking ahead, the establishment of trained dispatcher teams, continued advances in telecommunication technologies, and integration of wearable devices may further enhance the effectiveness of dispatcher-assisted CPR systems and lead to improved outcomes.
The unique contribution of this study lies in moving beyond video communication as a passive visual observation tool and introducing a live “visual modeling” approach, in which the dispatcher simultaneously performs CPR on a manikin during guidance. Through this method, video guidance combined with real-time demonstration transforms the abstract verbal description of “correct chest compressions” into a concrete motor model for untrained rescuers, with the potential to improve the two most critical CPR parameters: compression depth and rate. It is proposed that this approach should not be viewed as an alternative to formal CPR training programs, but rather as a complementary tool that partially bridges training gaps in situations where prior education is unavailable and may increase the likelihood of early bystander intervention in real-world settings. This model directly targets two common limitations of conventional T-CPR: (1) the difficulty untrained rescuers experience in mentally conceptualizing rhythm and depth, and (2) challenges in correctly sequencing and executing verbal commands under stress. By functioning as a visual template of correct movement and providing a metronome-like effect, simultaneous demonstration may stabilize compression rate while offering improved motor feedback for adequate compression depth. The observed increase in the proportion of compressions delivered at adequate depth and correct rate in the V-CPR group is consistent with this proposed mechanism.
Limitations and Strengths
This study has several methodological strengths, including its randomized controlled, single-blind design, which reduces the risk of bias; the objective and multidimensional recording of performance metrics using an advanced manikin-based system; and the adjustment of outcomes for potential confounders through robust regression analysis. In addition, the inclusion of a “simultaneous demonstration” component within the video intervention represents an innovative design that distinguishes this study from many previously reported video-guided CPR protocols.
Several methodological limitations should be considered when interpreting these findings. First, the study population consisted exclusively of young, healthy university students, which may limit the generalizability of the results to older individuals, patients with comorbidities, or populations with reduced physical capacity. In addition, this was a manikin-based simulation study, and therefore may not fully capture the environmental complexity of real-world OHCA scenarios, including confined spaces, ambient noise, crowd presence, emotional stress, and scene safety concerns.
Conducting the study in a controlled and quiet environment with fixed smartphone positioning may have reduced cognitive and operational load, particularly in the video-guided group. In real-world settings, however, factors such as handheld device use, maintenance of camera angle, and variability in connection quality may limit the effectiveness of video-assisted guidance. In addition, although no issues related to mobile network infrastructure, connection delays, or technical disruptions were observed in this study, such factors may play a significant role under field conditions.
Furthermore, limiting CPR performance to a five-minute duration precludes assessment of the effects of fatigue over time. In real-world scenarios, bystander CPR may be required for longer periods, during which performance degradation may be more pronounced. Therefore, to enhance the clinical applicability of these findings, future studies involving diverse age groups and real-world settings, preferably focusing on clinical outcomes, are warranted.
Finally, the study involved multiple comparisons across several CPR-related outcomes. As such, the reported confidence intervals were not adjusted for multiplicity. This may increase the risk of Type I error. Reference Harrington, D’Agostino and Gatsonis37 Therefore, these results should be interpreted as exploratory and hypothesis-generating rather than confirmatory.
Conclusion
The findings demonstrate that video call-assisted dispatcher guidance significantly improved CPR quality in untrained lay rescuers, particularly when combined with a simultaneous, application-based visual support model. Despite previous reports of prolonged interruption times in video-guided CPR, the reduction in compression pauses observed in the current study suggests that the effectiveness of video technology depends less on the mere presence of visual input and more on its operational design, including real-time modeling, rhythm anchoring, and reduction of cognitive load.
This specific visual model enhances care by providing real-time, concrete motor feedback that optimizes compression depth and rate, thereby potentially improving resuscitation quality in lay-rescuer scenarios.
Supplementary Materials
To view supplementary material for this article, please visit https://doi.org/10.1017/S1049023X26108875
Author Contributions
Adem Koksal: Substantial contributions to the conception, design, and methodology of the study; supervision; drafting of the manuscript; and final approval of the version to be published.
Mehmet S. Saribas: Contributions to methodology, data acquisition, statistical analysis, critical revision for important intellectual content, and final approval of the manuscript.
Mesut Tomakin: Involved in interpretation of data, critical review of the manuscript, and final approval of the version to be published.
Yusuf B. Kalafat: Participated in data acquisition, manuscript editing, and approval of the final version.
Ibrahim Caltekin: Contributed to study design and intellectual content revision; provided critical supervision and approved the final version of the manuscript.
Ali Aygun: Provided overall study supervision and methodological support; participated in interpretation of results, critical review, and final approval of the manuscript.
Note: All authors meet the ICJME authorship criteria.
Use of AI Technology: Artificial Intelligence (AI) tools were not used in the design of the study, data collection, statistical analysis, or interpretation of the results. However, OpenAI’s ChatGPT-4o model (OpenAI; San Francisco, California USA) was employed solely for the purpose of editing the English version of the manuscript, specifically to enhance grammar, clarity, and academic phrasing. The authors take full responsibility for the integrity, accuracy, and final content of the manuscript.
Conflicts of interest
Adem Koksal declare that he has no competing interests. Mehmet S. Saribas declare that he has no competing interests. Mesut Tomakin declare that he has no competing interests. Yusuf B. Kalafat declare that he has no competing interests. Ibrahim Caltekin declare that he has no competing interests. Ali Aygun declare that he has no competing interests.



 Open access
Open access