


Introduction
Purpose and context of the EFPC position paper on primary care for migrants
The number of immigrants in European countries is growing, migrant patients face challenges in accessing high-quality primary care and primary care professionals encounter difficulties in delivering this care. Therefore, the European Forum for Primary Care (EFPC) has developed this position paper on primary care for migrants. The EFPC is a network organization of primary care professionals, researchers, and policymakers (https://euprimarycare.org/).
In the current paper, the term ‘migrants’ refers to people who move from one country to another. The motives for migration, – and consequently, the health and living circumstances – vary widely between migrant groups, which include students, labour migrants, asylum seekers, refugees among others (see Box 1 for definitions). Currently, in many European countries, a perceived immigration crisis has led to increasingly restrictive policies regarding immigration and targeting certain migrant groups, such as non-EU migrants or those perceived as culturally or ethnically different from the majority population. These policies negatively impact their well-being and, in some cases, access to healthcare. Several scholars have challenged the use of the term ‘crisis’, arguing that it is not justified by actual migration figures and facts (De Haas, Reference De Haas2023).
Definitions (Source: IOM, 2023)
Definitions
Migrant: A person who has left his or her home country to live temporarily or permanently in another country (area). This can be totally voluntary and with individuals who meet the entry requirements of their destination country or to some extent involuntary, where forced migration represents the extreme end of a continuum of migratory motives. According to IOM a migrant is ‘anyone who has moved either across or within state borders away from their usual residence’.
Immigrant: A migrant who has settled in a specific country, in contrast to non-migrants or the majority population in that country.
Forced migration/forcibly displaced: Migration that involves force, compulsion, or coercion, even though the drivers may vary.
Asylum seeker: A person seeking protection from persecution or serious harm in a country other than their own and awaiting a decision on an application for refugee status under international and national laws.
Refugee: A person who, owing to a well-founded fear of being persecuted for reasons of race, religion, nationality, membership of a particular social group or political opinion, is outside the country of which he or she is a national and is unable or, owing to such fear, is unwilling to avail himself or herself of the protection of that country. The United Nations Refugee Convention of 1951 states that ‘a refugee should not be returned to a country where they face serious threats to their life or freedom’. This convention entitles legally recognized refugees to protection in other countries.
Undocumented migrants: Individuals without legal residency status, either because their asylum application was rejected or because they never filed one.
Non-migrants: people who have never migrated
General population: Refers to the entire population, including both migrants and non-migrants.
The aim of this paper is to outline what constitutes good-quality, accessible, affordable primary care for migrants – where affordable refers to low costs that enable people with low income to access services (WHO Regional Office for Europe, 2019a). The paper provides evidence- and practice-based recommendations and guidance for primary care organizations and professionals on how to deliver and facilitate such care. The paper starts with an overview of the impact of migration on health, the accessibility and quality of healthcare for migrants. It then presents our positions and recommendations supported by relevant evidence. This paper complements the EFPC position paper on healthy aging in migrants, published in 2023 (Jacobsen et al., Reference Jacobsen, Glasdam, Schopman, Sodemann, Van den Muijsenbergh and Ågotnes2023).
Migrants in Europe; demographics, displacements and legal status
Over the past decades, international migration has increased. People are forced or choose to leave their country, due to war, natural or other violence, poverty, or for study or family reasons. On January 1 2024, 44.7 million people (9.9%) of the 449.3 million people living in the EU were born outside the EU and 17.9 million people (4.0%) were born in another EU country (Eurostat, 2025). The Russian Federation’s invasion of Ukraine in 2022 resulted in one of the largest and fastest displacements in Europe since the Second World War. By June 2025, Europe – particularly Germany, Poland, and France – hosts over 5 million Ukrainian refugees (UNHCR, 2025).
European border countries such as Greece, Italy, and Turkey face continuous arrivals of migrants. Many of these migrants remain stuck in these countries due to the reluctance of other European nations to accept them. Due to restrictive immigration policies, many migrants are not granted legal residency. This has resulted in an estimated 1.9 to 3.8 million undocumented migrants in the EU, representing about 0.39% to 0.77% of the total population. In most countries, these individuals have limited or no access to social services and healthcare (PICUM, 2023).
The migrant population is aging (WHO, 2018: 1), approximately half of all migrants are women, and 10% are under the age of 18 (McAuliffe and Oucho, Reference McAuliffe and Oucho2024).
Health of migrants
Migration influences health outcomes through complex and interrelated mechanisms that unfold before, during and after displacement. These mechanisms are shaped by socio-economic factors, migration-induced stress, access to and appropriateness of the (healthcare) system, and the individual characteristics of migrants (Abubakar et al., Reference Abubakar, Aldridge, Devakumar, Orcutt, Burns, Barreto, Dhavan, Fouad, Groce, Guo, Hargreaves, Knipper, Miranda, Madise, Kumar, Mosca, McGovern, Rubenstein, Sammonds, Sawyer, Sheikh, Tollman, Spiegel and Zimmerman2018; Zeeb et al., Reference Zeeb, Stronks, Agyemang, Spallek, Ahrens and Pigeot2023). Many migrants experience physical and mental violence in their country of origin or during migration, which evidently impacts their health (Benvenuti et al., Reference Benvenuti, Marshall-Denton and McCann2024).
Although many migrants, refugees and labour migrants alike, are often in good health upon departure from their home countries, their health typically deteriorates after arrival. Over time, they experience worse health outcomes than individuals of similar socio-economic status in the host country or in their country of origin (Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer and Linos2020). Mental health problems (depression, PTSD, anxiety disorders, psychosis), cardiovascular disease, dementia, being overweight, diabetes mellitus, some infectious diseases (hepatitis B/C, HIV, Tuberculosis, parasitic infections), are more prevalent – often at younger ages – among immigrants, compared to non-migrants (WHO, 2021; Chilunga et al., Reference Chilunga, Appelman, van Vugt, Kalverda, Smeele, van Es, Wiersinga, Rostila, Prins, Stronks, Norredam and Agyemang2023; Zeeb et al., Reference Zeeb, Stronks, Agyemang, Spallek, Ahrens and Pigeot2023). Refugee children are especially vulnerable: they suffer more often from mental health problems than other migrant and non-migrant children. For instance, depression is seen in 14% of refugee children globally, compared to 3% of other children (Dangmann et al., Reference Dangmann, Dybdahl and Solberg2022).
Some diseases with a genetic origin like hemoglobinopathies are more prevalent among immigrant populations than in the general population in Europe. Moreover, the prevalence of oral health problems is higher in migrants (Bamihashem et al., Reference Banihashem Rad, Esteves-Oliveira, Maklennan, Douglas, Castiglia and Campus2024). Immigrant women, in particular those with a forced migration background, face higher risks of perinatal mortality and morbidity, stillbirth, preterm birth, and low birthweight in their newborns (Gieles et al., Reference Gieles, Tankink, van Midde, Düker, van der Lans, Wessels and Browne2019; Souza et al., Reference Souza, Day, Rezende-Gomes, Zhang, Mori, Baguiya, Jayaratne, Osoti, Vogel, Campbell, Mugerwa, Lumbiganon, Tunçalp, Cresswell, Say, Moran and Oladapo2023).
Migration is associated with dietary changes, driven by new and different culture and food environments. Dietary acculturation is connected to poorer dietary choices: like diets with high levels of fat and sugar, low in consumption of fruits and vegetables, contributing to overweight (Popovic and Strasser, Reference Popovic-Lipovac and Strasser2015). At the same time, refugees frequently experience limited dietary diversity and insufficient intake of essential nutrients, resulting in undernutrition, vitamin D- and iron deficiencies, and alarmingly low haemoglobin levels among children (Khuri et al., Reference Khuri, Wang, Holden, Fly, Mbogori, Mueller, Kandiah and Zhang2022).
The causes of these adverse health outcomes are multifaceted and interrelated, worsening outcomes in cases where other inequities, like gender inequality, are present (intersectionality). Often, migrants also suffer disproportionately from other social determinants of poor health, including poverty, poor housing, barriers to participating in society, discrimination, and lack of social support (Borrell et al., Reference Borrell, Palència, Bartoll, Ikram and Malmusi2015). Social isolation, particularly among older immigrants, is a significant concern (Jacobsen et al., Reference Jacobsen, Glasdam, Schopman, Sodemann, Van den Muijsenbergh and Ågotnes2023).These stressors can lead to chronic stress, which not only increases the risks for certain diseases like diabetes, depression, and cardiovascular disease (Chilunga et al., Reference Chilunga, Boateng, Henneman, Beune, Requena-Méndez, Meeks, Smeeth, Addo, Bahendeka, Danquah, Schulze, Klipstein-Grobusch, Mannens and Agyemang2019; Guidi et al., Reference Guidi, Lucente, Sonino and Fava2021), but can also undermine health literacy and self-management, further hindering effective prevention and management of diseases (D’ Amico et al., Reference D’Amico, Amestoy and Fiocco2020).
As such, migration can be regarded as an independent social determinant of health. The health disparities between immigrants and non-migrant populations reflect ‘tangible manifestations of persistent inequities in global health and socio-economic development’ (Souza et al., Reference Souza, Day, Rezende-Gomes, Zhang, Mori, Baguiya, Jayaratne, Osoti, Vogel, Campbell, Mugerwa, Lumbiganon, Tunçalp, Cresswell, Say, Moran and Oladapo2023).
Culture shapes our understanding and perception of illness and what constitutes good care (Kleinman et al., Reference Kleinman, Eisenberg and Good1978). When these cultural frameworks differ between healthcare providers and patients, misunderstandings can arise. Too often, these are attributed solely to the ‘culture of migrants’, without acknowledging how providers’ own cultural assumptions influence their beliefs and actions. Moreover, biomedicine itself is not culturally neutral; it is shaped by underlying values and assumptions that inform diagnostic frameworks, treatment protocols, and even definitions of health and illness. Recognizing these cultural dimensions calls for humility and reflexivity in practice, encouraging healthcare professionals to critically examine both their personal beliefs and the systemic norms embedded in medical knowledge and practice.
Access to and quality of healthcare for immigrants
Health care systems themselves are an important social determinant of health (O’Donnell et al., Reference O’Donnell, Burns, Mair, Dowrick, Clissmann, Van den Muijsenbergh, Van Weel-Baumgarten, Lionis, Papadaki, Saridaki, de Brun, O’Reilly de Brun and MacFarlane2016). A lack of access to prevention and care, combined with a lack of cultural-responsive care, contributes to the worse outcomes of care among migrant patients (Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer and Linos2020). Prior healthcare experiences in the country of origin also shape expectations regarding healthcare. As in many countries no strong primary care system exists, this is especially true for primary care. This is particularly evident in the reluctance of many migrants to accept the role of the general practitioner as gatekeeper to the healthcare system, or the role of other primary care professionals such as nurses or midwives (Kroezen et al., Reference Kroezen, Rajan and Richardson2023).
Immigrants encounter various barriers in accessing and receiving appropriate and timely care (Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer and Linos2020; Filler et al., Reference Filler, Jameel and Gagliardi2020; Mudyarabikwa et al., Reference Mudyarabikwa, Regmi, Ouillon and Simmonds2022; Kamran et al., Reference Kamran, Hassan, Ali, Ali, Taj, Mir, Pandya, Steinberg, Jamal and Zaidi2022).
These include:
-
• Structural barriers relating to the health care system, such as limitation of entitlement or lack of health insurance for certain groups. Despite the universal human right to medical care for all, and medical professionals’ obligations to deliver all necessary medical care irrespective of finances or one’s legal status (WMA. 2022), undocumented migrants face substantial financial and administrative barriers in accessing healthcare (de Vito et al., Reference De Vito, de Waure, Specchia and Ricciardi2015). In 2016, among 28 EU countries, only six allowed undocumented migrants full access to emergency, primary, and secondary care free of charge (fundamental rights report, 2016). More recent EU-wide data are scarce, but there is little evidence of substantial improvement since then.
-
• Accessibility barriers of available services, including language barriers, high transportation costs and out of pocket payments, unclear procedures, and inadequate information about the health care system and fear for unknown (financial) consequences. At a provider level, poor communication skills and a lack of cultural competence, as well as lack of knowledge about rights and needs of immigrants and their complex medical and social history, can act as major barriers (WHO, 2024). Moreover, formal interpreters are rarely used in everyday clinical practice, despite evidence supporting their effectiveness (Krystallidou et al., Reference Krystallidou, Langewitz and van den Muijsenbergh2020).
-
• Interaction barriers arising from the patient – provider contact. Immigrants do not always share the same conceptual frameworks or views of illness or solutions for their symptoms as European healthcare professionals. For instance, in case of mental distress they often see this as a logical result of their situation and often prefer informal support from family, religion or community members (Renkens et al., Reference Renkens, Rommes and van den Muijsenbergh2022). Although differences in beliefs and preferences exist between different cultures and religions (e.g., concerning end-of-life issues) bigger individual differences exist between members from the same immigrant community. Therefore, rather than making assumptions, it is important that healthcare professionals ask their patients what beliefs and practices are personally important to them, and be aware of their own beliefs and preferences (WHO, 2018). Past experiences of not being taken seriously by healthcare providers, discrimination and privacy concerns may further discourage seeking care (Borrell et al., Reference Borrell, Palència, Bartoll, Ikram and Malmusi2015).
Due to these barriers, migrants tend to underutilize health services, screening and preventive programmes, and homecare services compared to the majority population, and overall face lower access to care (Lebano et al., Reference Lebano, Hamed, Bradby, Gil-Salmerón, Durá-Ferrandis, Garcés-Ferrer and Linos2020; Behboudi-Gandevani et al., Reference Behboudi-Gandevani, Bidhendi-Yarandi, Panahi, Mardani, Prinds and Vaismoradi2022; WHO, 2024).
Racism, ethnic and religious discrimination in healthcare
Beyond language and cultural barriers, racism, discrimination, and (unconscious) bias based on ethnicity, religion, socio-economic status, and disability persist across all sectors of society, including healthcare (Fitzgerald et al., Reference Fitzgerald and Hurst2017; Gil-Salmerón et al., Reference Gil-Salmerón, Katsas, Riza, Karnaki and Linos2021).
These issues are deeply rooted in a combination of historical legacies, entrenched social structures, and systemic inequities. This negatively affects care delivery and health outcomes and contributes to disparities in health, quality of healthcare and access between migrants, ethnic minoritized groups, and white majority populations (Horton, Reference Horton2017; Ibrahiim et al., Reference Ibrahiim, Agyemang, Adams and Ahmed-Landeryou2023; Gangrova et al., Reference Gangarova, Yildiz and Kabangu2025).
Discrimination can manifest in various ways, including differential treatment, biased clinical decision-making, and unequal access to resources and services. The consequences not only undermine the quality of care but can also erode trust in healthcare, discourage individuals from seeking necessary care, and thus further contribute to poorer health outcomes (Brown and Homan, Reference Brown and Homan2022). Addressing these challenges requires embedding accountability and equity principles within health system governance.
Paucity of data
Despite the above mentioned evidence on existing disparities in health and healthcare, in most countries few data exists specifying health outcomes, healthcare use, and quality of care among migrants. Often migrant patients are not included in studies, with researchers claiming they are ‘hard to reach’ or that research instruments like questionnaires are not validated in different languages. However, it is very well possible to involve migrants in research. Collaborative, co-produced research approaches aimed at advancing health equity can foster meaningful and sustainable change (Atwal and Ibrahiim, Reference Atwal, Ibrahiim and Atwal2022; MacFarlane et al., Reference MacFarlane, Huschke, Marques, Gama, Kinaan, Hassan, Papyan, Phelan, Severoni, Kumar and Dias2024).
Also, sex and gender-disaggregated and income-disaggregated data are not always collected making it difficult to provide a full picture of the intersectional dynamics in migration, for instance gender differences in remittance sending, and to address gender discrimination. Strengthening data collection standards, including disaggregation by migration status, gender, and income, is essential to inform equitable policies.
Methods
All authors of this position paper are members of the EFPC Working Group on Migrant Care, and come from diverse professional backgrounds and countries, including primary care health workers from various disciplines (such as general practitioners, dietitians, and nurses), researchers, and policy makers. All have extensive experience in providing or researching migrant care, including involvement in several European projects focused on primary care for refugees and other migrants, a.o. RESTORE: Communication with Migrants in primary care (www.fp7restore.eu), EUropean Refugees – HUman Movement and Advisory Network – EUR-HUMAN (http://eur-human.uoc.gr/), and Operational Refugee and Migrant Maternal Approach – ORAMMA (https://oramma.eu/the-project/).
Through a purposive search, papers on migrant health and primary care for migrants were reviewed, informing the narrative synthesis of evidence presented in this position paper. The positions and recommendations outlined in this paper are based on scientific literature as well as on the experiences of primary healthcare providers.
The paper was written in a collaborative, iterative process, with contributions from each of the authors based on their specific expertise. Several rounds of revision were conducted, and feedback was documented and incorporated into subsequent drafts. Drafts were circulated among the working group members for feedback, ensuring that diverse perspectives were included. In addition to written feedback, a series of online discussion sessions were held to further refine the positions and recommendations. These sessions allowed for in-depth conversations and collective decision-making, helping to ensure that the paper reflects a broad range of experiences and insights. A wide range of professions, disciplines were involved with substantial geographical, gender, and ethnic diversity among the participants of the working group and authors of this paper, including authors with lived experience as a migrant. However, they all are engaged in primary care research, delivery, organization or planning which could implicate we missed out on the patient perspective. By including studies on patient experiences, we hope to sufficiently acknowledge this perspective.
Subsequently, during a consensus meeting at the 2024 EFPC conference in Ljubljana, the preliminary recommendations were discussed and refined by 30 participants in a plenary format. Interactive tools were used to facilitate discussion and enable participants to indicate agreement or suggest changes through voting. Feedback gathered during this process was integrated into the final version of the paper.
Positions and recommendations
-
1. All migrants should have access to good-quality primary care
Strengthening primary health care (PHC) is a priority of World Health Organization (WHO), as it brings healthcare and social care closer to people’s home, addresses all health needs and has the potential to promote health equity and well-being by addressing root causes and psychosocial determinants of health (Detollenaere et al., Reference Detollenaere, Hanssens, Vyncke, De Maeseneer and Willems2017; WHO-Europe, 2022). The complex health needs of refugees and other migrants require an integrated community-based primary healthcare approach, delivered by an interprofessional team – a key feature of good primary care (McMurray et al., Reference McMurray, Breward, Breward, Alder and Arya2014).
There is substantial evidence supporting the positive effects of person-centred, community-oriented (integrated) primary care on health outcomes, patient and doctor satisfaction as well as costs (Ahmed et al., Reference Ahmed, van den Muijsenbergh and Vrijhoef2022). A person-centred approach builds mutual trust and understanding, which are crucial elements for effective communication. This is of particular importance in migrant populations where negative experiences with professionals and institutions can make it difficult to establish and build a trusting therapeutic relationship (van den Muijsenbergh et al., Reference Van den Muijsenbergh, van Weel-Baumgarten, Burns, O’Donnel, Mair, Spiegel, Liones, Dowrick, O’Reilly, de Brun and MarFarlane2014). Person-centred care involves considering the personal and social context of the patient. Realization of a person-centred approach in migrant populations requires additional knowledge of ethnic and cultural health differences, as well as skills for communicating across linguistic and cultural differences (Seeleman et al., Reference Seeleman, Suurmond and Stronks2009; Seeleman et al., Reference Seeleman2014). However, above all, it requires empathy and an attitude of cultural modesty, awareness of one’s own cultural beliefs, biases and prejudice as well as of systemic racism and bias (Hagiwara et al., Reference Hagiwara, ELston Latafa, Mezuk, Vrana and Fetters2019; Lee and Haskins, Reference Lee and Haskins2022). Healthcare professionals should be aware of their own cultural competencies and limitations, such as cultural values and prejudice (Oxtoby, Reference Oxtoby2020). Another important element is personal continuity of care: patients seeing as much as possible the same healthcare provider. This increases satisfaction, trust and confidence and improves health outcomes (Sandvik, Reference Sandvik2022). Also important is performing a physical examination when patients present physical complaints, to ensure their trust (O’Donnell et al., Reference O’Donnell, Higgins, Chauhan and Mullen2008). Although the benefits of shared decision-making are widely acknowledged, and especially patients with low health literacy benefit from shared decision-making (Durand et al., Reference Durand, Carpenter, Dolan, Bravo, Mann, Bunn and Elwyn2014), many healthcare professionals expect that migrant patients do not wish to participate in shared decision making (Jager et al., Reference Jager, van der Sande, Essink-Bot and van den Muijsenbergh2018), and linguistic and cultural barriers can complicate this process. However, most migrant patients, like everybody else, actually do have a desire to be included in the decision-making process (Schinkel et al., Reference Schinkel, Schouten and van Weert2013).
Migrants’ experiences with PHC in destination countries are not always positive. They often feel they are not taken seriously by the PHC professional, complain about insufficient time allocated for consultations, and experience misunderstandings due to the lack of interpreters (van Loenen et al., Reference Van Loenen, Van den Muijsenbergh, Hofmeester, Dowrick, Ginneken, van, Aggelos Mechili, Angelaki, Ajdukovic, Bakic, Rotar Pavlic, Zelko, Hoffmann, Jirovsky, Mayrhuber, Dückers, Mooren, Gouweloos–Trines, Kolozsvári, Rurik and Lionis2018; Soltani et al., Reference Soltani, Fair, Watson, Raben and Van den Muijsenbergh2018; Jager et al., Reference Jager, van der Sande, Essink-Bot and van den Muijsenbergh2018; Cinar et al., Reference Çinar, de Klein, Renkens, Akkermans, Latify, Walewijn, Van den Muijsenbergh and van Loenen2025). Primary care providers mention lack of awareness of the healthcare system, stigma, competing priorities, shortage of family physicians and direct costs as some of the barriers to access primary care (Sundareswaran et al., Reference Sundareswaran, Martignetti and Purkey2024). Migrants in the UK, for example, were already less likely to use primary care compared to non-migrants before the COVID-19 pandemic, and this disparity worsened due to the rise of remote and hybrid service delivery models during the pandemic (Zhang et al., Reference Zhang, Boukari, Pathak, Mathur, Katikireddi, Patel, Campos-Matos, Lewer, Nguyen, Hugenholtz, Burns, Mulick, Henderson and Aldridge2022).
To ensure equitable access to good primary care for all migrants, structural barriers must be eliminated. These barriers, often created by government policies, health insurance or others systemic factors, include limitations on the availability of interpreter services and sufficient time allocated for consultation with professionals (McFarlane et al., Reference MacFarlane, Dowrick, Gravenhorst, O’Reilly-de Brún, de Brún, van den Muijsenbergh, van Weel Baumgarten, Lionis and Papadakaki2021). Addressing these issues require advocacy for policy changes that support the integration of comprehensive support services into primary care.
Collaboration with local migrant communities, actively involving them in co-designing practice organization as well as health promotion campaigns is mandatory to tailor the information and services to their specific needs (O’Reilly-deBrún et al., Reference O’Reilly-de Brún, De Brún, O’Donnell, Papadakaki, Saridaki, Lionis, Burns, Dowrick, Gravenhorst, Spiegel, Van Weel, Van Weel-Baumgarten, Van den Muijsenbergh and MacFarlane2017; WHO, 2018; McFarlane et al., Reference MacFarlane, Dowrick, Gravenhorst, O’Reilly-de Brún, de Brún, van den Muijsenbergh, van Weel Baumgarten, Lionis and Papadakaki2021). To provide diversity-sensitive person-centred care, healthcare professionals will need sufficient time and training, as emphasized by WHO (WHO, 2021a, b, c).
-
2. Training in diversity-sensitive person-centred care should be integrated in under- and postgraduate training for all primary care professionals
As the health experiences and outcomes of migrant patients often are influenced by more factors than culture, we prefer to refer to this approach as diversity-sensitive person-centred care rather than culturally-sensitive care. Being able to address all issues relevant for a person, including his social circumstances, requires from health care providers to possess structural competency (Neff et al., Reference Neff, Holmes, Knight, Strong, Thompson-Lastad, McGuinness, Duncan, Saxena, Harvey, Langford, Carey-Simms, Minahan, Satterwhite, Ruppel, Lee, Walkover, De Avila, Lewis, Matthews and Nelson2020). This means they must understand the social determinants of health, be able to discuss these topics that often are felt to be shameful, and to forge interprofessional collaborations with professionals and organizations that can support patients in their social needs (Metzl and Hansen, Reference Metzl and Hansen2014).
Primary care professionals, such as physicians, nurses, allied health professionals, dieticians, midwives, social workers – experience challenges in providing the same level of quality care for migrants, due to language and cultural differences, lack of competences as well as time constraints. Many of them report a need for training in this field (Suphanchaimat et al., Reference Suphanchaimat, Kantamaturapoj, Putthasri and Prakongsai2015; Jager et al., Reference Jager, Den Boeft, Leij-Halfwerk, Van der Sanden and Van den Muijsenbergh2020; Fair et al., Reference Fair, Soltani, Raben, van Streun, Sioti, Papadakaki, Burke, Watson, Jokinen, Shaw, Triantafyllou, van den Muijsenbergh and Vivilaki2021; Ibrahiim et al., Reference Ibrahiim, Agyemang, Adams and Ahmed-Landeryou2023; Oehri et al Reference Oehri, Chernet, Merten, Sydow and Paris2023).
Evidence suggests that these challenges contribute to substandard quality of care. For example, general practitioners often fail to discuss sensitive topics, such as mental health or reproductive health, with refugees, leading to underdiagnosis of health needs in these respects (Raben and van den Muijsenbergh, Reference Raben and van den Muijsenbergh2018; Cinar et al., Reference Çinar, de Klein, Renkens, Akkermans, Latify, Walewijn, Van den Muijsenbergh and van Loenen2025).
Social justice, equity, racism or bias are not always sufficiently addressed in medical curricula, which leaves healthcare professionals and trainees unprepared and lacking the knowledge necessary to address social, cultural, and public health issues, or to recognize and deal with racism in practice. The lack of preparation reduces their confidence in confronting the systems that sustain health disparities (Papadaki et al., Reference Papadakaki, Lionis, Saridaki, Dowrick, De Brún, O’Reilly-de Brún, O’Donnell, Burns, Van Weel-Baumgarten, Van den Muijsenbergh, Spiegel and MacFarlane2017; Oehri et al., Reference Oehri, Chernet, Merten, Sydow and Paris2023; Verschuuren et al., Reference Verschuuren, Tankink, Franx, van der Lans, Erwich, Jong and de Graaf2023).
Evidence is growing that diversity-sensitive person-centred care, including awareness of one’s bias, can be taught (Suurmond et al., Reference Suurmond, Lantinga, de Voogd, Oueslati, Boland and van den Muijsenbergh2020; Fair et al., Reference Fair, Soltani, Raben, van Streun, Sioti, Papadakaki, Burke, Watson, Jokinen, Shaw, Triantafyllou, van den Muijsenbergh and Vivilaki2021; Jager et al., Reference Jager, Leij-Halfwerk, Akkermans, van der Sande and van den Muijsenbergh2024). Although on-line courses have their merits and are easily used, training is most fruitful when migrants with lived experience are co-trainers, when it includes practical exercises in cross-cultural communication and when there is a booster training to discuss experiences in daily practice (Jager et al., Reference Jager, Leij-Halfwerk, Akkermans, van der Sande and van den Muijsenbergh2024).
A review shows that most interventions to improve primary are for refugees primarily focus on upskilling physicians, with a paucity of research exploring the involvement of other health care professionals (Iqbal et al., Reference Iqbal, Walpola, Harris-Roxas, Li, Mears, Hall and Harrison2022). Future interventions should incorporate other healthcare professionals and foster interprofessional collaboration (Iqbal et al., Reference Iqbal, Walpola, Harris-Roxas, Li, Mears, Hall and Harrison2022). National and European health workforce strategies must prioritize interprofessional education and collaborative care models to ensure support for migrant patients. Participation of students and trainers in international exchange programmes on diversity-sensitive care can contribute to intercultural communication and empathy skills (Guner et al., Reference Guner, Ocak Akturk, Oner Aydın and Karaca Saydam2022), as could diversification of the workforce. However, at this moment healthcare professionals of migrant background are underrepresented, and trainees from ethnic minority background face more challenges than others. This calls for more inclusive training of primary care professionals (Van Moppes, Reference Van Moppes2025).
-
3. Good, effective primary care for migrants requires strong interprofessional collaboration
Effective primary care for migrants hinges on robust interprofessional collaboration. Healthcare providers must not only be knowledgeable about social determinants of health but also actively engage with professionals from different disciplines to address the diverse needs of migrant populations. This collaborative approach ensures that all aspects of a migrant’s health – both physical, mental and social – are considered (Metzl and Hansen, Reference Metzl and Hansen2014). Faith communities and volunteer organizations are important sources of emotional and practical support (WHO, 2018). Knowing where to find and how to refer to them, to social care, welfare and specialized services for particularly vulnerable subgroups like older people can help to realize their needs. Supporting migrants’ wellbeing and health and enabling their full participation in society on equal terms also requires access to essential resources such as affordable, nutritious, and culturally appropriate food. This can be achieved through coordinated efforts with local food banks, community organizations, and governmental agencies (WHO, 2021; Gingell et al., Reference Gingell, Murray, Correa-Velez and Gallegos2022). Dietitians can play an important role in this (Khur et al., Reference Khuri, Wang, Holden, Fly, Mbogori, Mueller, Kandiah and Zhang2022; Ramsahoi et al., Reference Ramsahoi, Sonny and Monk2022).
-
4. Language differences in healthcare require the consistent availability of Professional interpretation services
Professional interpreter services should be consistently available in all primary care practices. Involving professional interpreters is essential in migrant healthcare, particularly when addressing sensitive topics like mental health or trauma. Interpreters ensure accurate communication, improve patient-clinician interactions, and enhance the effectiveness of treatments, especially in psychological care (Krystallidou et al., Reference Krystallidou, Langewitz and van den Muijsenbergh2020). Relying on family members for translation is not recommended due to potential misunderstandings, especially regarding sensitive information.
Cultural mediators, who are familiar with both the local healthcare system and the cultural background of migrants, can support patients in navigating the system. Their role is particularly effective when they are consistent throughout the treatment process, helping to build trust and continuity (WHO, 2018).
Many telehealth platforms incorporate real-time interpretation services. While telephone or online interpretation can be cost-effective, in-person professional interpretation should be prioritized for complex or sensitive cases to ensure high-quality communication.
Consensus on recommendations
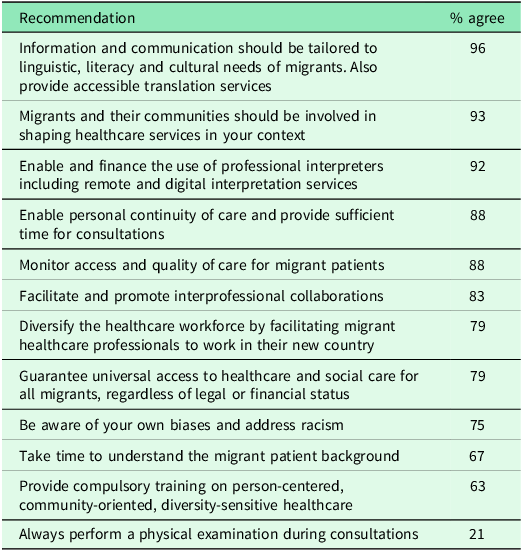
Based on the above, we formulated recommendations (see Box 2) to improve access to and quality of primary care for migrants. These were discussed within the EFPC working group on migrant care and during the workshop at the annual EFPC conference 2024 (see Table 1). A vast majority of the participants supported enabling personal continuity of care and providing sufficient time for consultations (88%), as well as promoting interprofessional collaboration (83%). There was also agreement on the importance of addressing personal bias and racism in healthcare (75%), and monitoring access and quality of care for migrant patients (88%). Significant support was shown for using professional interpreters (92%), and involving migrant communities in shaping healthcare services (93%). Tailoring communication to the linguistic and cultural needs of migrants also received broad approval (96%).
Recommendations to improve access and quality of primary care for migrants
-
A. Recommendations for healthcare and research policies
-
• Ensure the universal human right to health for all migrants, regardless of legal status, to have access to healthcare, nutritional care, and social care. Provide clear information to migrants about their rights and entitlements within the healthcare system.
-
• Include into quality assessment of care topics to assess the access and quality of care for migrant patients
-
• Promote and fund inclusive research: scientific research that includes migrant populations, ensuring the collection and availability of data on their health outcomes, healthcare access, and use.
-
• Integrate diversity-sensitive care by incorporating teaching diversity-sensitive, person-centred care into professional education, and support the delivery of this care by national and international laws and policies.
-
• Ensure access to professional interpreter services by establishing regulations and financial mechanisms to ensure the availability and use of professional interpreters in healthcare consultations to ensure clear communication and effective care.
-
-
B. Recommendations for education and training
-
• Start early and continue throughout career
-
• Focus on awareness of bias, and cultural norms of the patient as well as of the professional, communication, and potential barriers to care.
-
• Incorporate practical training and lived experiences: involve migrants with lived experience as co-trainers for practical exercises in cross-cultural communication
-
• Encourage international exchange programmes
-
-
C. Recommendations for healthcare organizations
-
• Engage with migrant communities to tailor information, health promotion, and services to their specific needs.
-
• Encourage and support the employment of migrant and ethnic minority health care professionals
-
• Enable diversity-sensitive person-centred care by facilitating personal continuity of care, securing enough time per consultation, facilitating the use of interpreters and of relevant training
-
• Ensure effective communication by facilitating the use of professional interpreters and cultural mediators
-
• Foster interprofessional and cross-sectoral collaboration by integrating social workers, dieticians, community health workers etc., into primary care teams.
-
• Provide accessible easy to understand Health Information in multiple languages – e.g. short movies in the waiting room – on practice procedures and health promotion
-
-
D. recommendations for healthcare professionals
-
• Develop self-awareness of cultural competencies and limitations
-
• Provide Diversity sensitive person-centred care and involve also migrants in shared decision-making
-
• Explore the broader context of the patients’ life, assessing all social determinants of health and risk factors that might influence the health of your migrant patient
-
• Foster collaboration with community organizations and support networks that address the social determinants of health can further enhance care.
-
• Don’t assume but ask your patient about their beliefs and preferences.
-
• Involve professional interpreters and cultural mediators.
-
• Adjust your communication to the literacy level and preferences of the patient. It is important to assess the level of literacy of your patient and to adjust your information to this level. Discuss if, and if so, the patients prefer a family member or other trusted person to be present during the consultation, and to what extent he wants to be informed.
-
• Always perform a physical examination in case of physical complaints.
-
• Assess nutritional risks
-
• Collaborate with other professionals across healthcare and social care as well as with migrant communities.
-
Overview of the agreement on recommendations at the EFPC conference

Moderate support was noted for diversifying the healthcare workforce (79%), providing compulsory training on diversity-sensitive care (63%), and taking more time to understand the background of migrant patients (67%). Guaranteeing universal access to healthcare for all migrants regardless of legal or financial status was agreed upon by 79%. However, opinions were more divided on always performing physical examinations during consultations, with only 21% (strongly) of respondents agreeing and a notable proportion remaining neutral or disagreeing.
Conclusion
Overall, this position paper highlights the need for strong communication, effective collaboration, and structural reform as cornerstones of diversity-sensitive primary care. This is particularly relevant in an increasingly diverse Europe, where migration is no longer a new phenomenon, and the complexity of migrants’ living conditions is familiar to many healthcare professionals. This position paper highlights the urgent need to improve access to and the quality of primary care for refugees and other migrants, in particular those who are undocumented, through a structural, person-centred, and diversity-sensitive care approach. Box 3 shows an example from daily GP practice what such an approach can entail.
Case-example for illustrating person-centred-diversity sensitive primary care (adaption of example in Van den Muijsenbergh, Reference Van den Muijsenbergh and Dowrick2019).
On a busy Monday morning Naima enters your consultation room. You know her quite well. She is a young North African woman, very active in her community. Consultations with her are always easy. But today, she is not alone. With her comes a girl you have never seen before. She looks to the floor and gives a very weak handshake; she does not say a word. She looks very sad. Naima tells you her name is Latifa, she is 20 years old and she is not feeling at all well. Naima did not know who to turn to as Latifa has just arrived in your city. Originally she is from Egypt, Naima thinks; they met at the Mosque, where Latifa was brought by her aunt. Naima had tried to speak with Latifa, but got the impression that she was very afraid and ill. She does not know if Latifa has health insurance, but she does know that the girl needs help, right now.
If Latifa does not have health insurance, are you obliged to help her?
Yes. According to medical ethics, we must help all patients regardless of their background or financial status.
It is Monday morning, your waiting room is filled with patients. You clearly have very limited time now to handle this.
What would be the best strategy?
You understand this is an urgent problem, but you will need time to explore what is going on. Therefore, you ask Naima if she and Latifa can come back at lunchtime, to have more time for the consultation. They agree and come back a few hours later.
As migrants often feel rejected, and Latifa clearly needs help, it is important you let her feel you want to help. A therapeutic relationship requires trust to be built. In order to make sure she and Naima understand this, and that you have a mutual understanding of the procedure, you should be very specific about the new appointment, and make sure it fits their schedule as well as yours.
Latifa will probably not speak your language, as she has just arrived from Egypt. Naima probably does.
What would be the best strategy to handle this?
The best option is to request a professional interpreter and ask through this interpreter whether Latifa wishes for Naima to stay. Often this is the case as the patient will feel supported and advocated for by the presence of a compatriot who also understands the language and culture of the host country. With a male Arabic interpreter on the phone you start your conversation with Latifa.
Could the interpreter be a problem?
If Latifa has problems that are related to sexual or reproductive health, she may find this hard to share with a male interpreter. If you do not know a patient, then try to find a gender congruent interpreter.
Latifa explains that she does not feel well, her belly aches, she cannot eat, she has lost her appetite, and she is very tired. This started when she arrived in your country. She thinks she might have caught a local disease. All your further questions do not reveal any indication for a gastro intestinal or gynaecological disease. You are increasingly convinced that Latifa is suffering from a mental health problem.
To convince Latifa that she does not have a physical illness, and to give her the feeling you have taken her seriously, you examine her abdomen and undertake appropriate investigations e.g. blood pressure. Only after specific reassurance that her body is healthy, you are able to explain that sometimes the body feels ill because of stress or other problems, and continue with questions related to stress and mental health.
To your surprise, when asking Latifa if she feels depressed, she says no, although she looks very depressed.
How can you explain this?
There are several possibilities: Maybe she is not depressed and your impression has been influenced by your implicit bias, thinking women who will not look you in the face and smile will have to be depressed. It is also possible that she does not know the word depressed, not even in her own language. Or she might feel ashamed about her ‘wrong’ feelings and she does not want Naima to know this, for fear of the stigma of mental health problems in the community or on the contrary she would prefer to discuss these issues with someone from her religion or community. These could all be true. Therefor you ask more questions, after asking Naima to leave the room, to get a deeper understanding of her problems. You remember that it is always important to get to know the context of the patient and asks her about her life circumstances and her life in Egypt. Latifa tells you she had a ‘bad’ experience in Egypt with a man, and her family had sent her away to stay with her aunt in your country. Since this experience she does not sleep, even though she is very tired, she is easily startled by noise and loses her temper very quickly. She overheard her aunt say to the Imam that it is the work of a Djinn.
How should you react to this information?
It would be best to ask Latifa about the Djinn. Ignoring or rejecting the existence of Djinns will probably harm the confidence Latifa will have in you, preventing you from gaining further information on what they are going to do about the Djinn, and will probably form a barrier against effective help. Stating that you know about Djinns may seem like a means of building trust, however doing so assumes you know what Latifa has experienced. It is always best to ask the patient what they think about culturally influenced health beliefs. After a lengthy conversation, Latifa begins to speak more and makes some eye contact. She tells you she also worries about the lack of money and about finding housing, as her aunt does not have money and is not allowed to host people in her rented rooms. She has a lot of stress. You are convinced she suffers from chronic stress and probably of PTSD and you suspect sexual violence. You do not wish to ask about this in a first consultation. You want to refer her to a social worker and a mental health nurse with expertise on migrant women and sexual violence.
How can you refer her?
Your standard practice, would be to make an electronic referral to these services, and tell Latifa that she will receive an invitation for an appointment with them within the next weeks. However, in this case this isn’t a good way to refer. The chances are high that Latifa will never arrive, or the therapy will not start properly. The appointment letter may not reach her as she may change address or may not have anyone in the house able to read the letter. She will not know where to go, or may not have enough money for public transport. She also may not trust these unknown persons. Ideally, for a vulnerable migrant like Latifa you arrange a ‘warm’ referral. This is easy when social workers and mental health nurses are members of your primary care team and located in the same building. Anyhow, you should make a personal appointment, if possible while Latifa is still in your room, so she hears what you discusses. It would be even better to involve a ‘peer supporter’, a migrant speaking her mother tongue who can act as a navigator through the system, and accompany her to appointments. Check if the appointment fits in with her agenda, if an interpreter will be available, and if Latifa understands where and when she has to go, and if she is able to do so. Make a follow-up appointment to get to know her better, and to check how she is doing. During that appointment, you could ask about her medical history, and include in this the question about if she has had a bad sexual experience. To introduce this delicate issue, it is important to ‘normalize’ it, for instance by saying ‘As I know that many women have suffered from bad sexual experiences, and that these experiences can damage your health, I always ask new patients if they have ever suffered from a bad sexual experience, for instance being touched by a man you did not want, or have sex without protection’. If sexual violence has taken place, do not forget to ask about symptoms of sexually transmitted infections and possible pregnancy. Explain to Latifa what PTSD is, and why she is experiencing the nasty things she feels.
Despite existing evidence on health inequities, persistent barriers, ranging from legal and financial constraints to lack of professional training and interpreter services, continue to impede equitable healthcare provision.
EFPC stresses the point that besides the required medical knowledge, intersectoral collaboration to address social determinants, the use of interpreters and above all empathy and compassion are essential elements of care which should be strengthened to provide a more inclusive healthcare across Europe and beyond. A transition towards truly inclusive primary care systems requires commitment at all levels, policy, education, practice, and research.
Person-centred diversity-sensitive primary care must become the guiding principle in the design and delivery of services for migrant populations. This entails recognizing the individuality of each patient, being responsive to their cultural, linguistic, and social backgrounds, and addressing broader determinants of health. Such an approach not only enhances trust and communication but also leads to better health outcomes, greater patient and provider satisfaction, and more sustainable healthcare systems. Only by embedding the principles in primary care systems can equitable access, continuity of care, and improved health outcomes for migrant populations be ensured. Ultimately, strengthening diversity-sensitive primary care not only benefits migrants, but also contributes to more resilient, cohesive, and inclusive health systems for all, enhancing preparedness for demographic changes and public health crises.
Data availability statement
No new data were generated or analyzed in support of this research.
Acknowledgements
We thank the Migrant Health Working group members as well as all participants of the Ljubljana EFPC conference workshop for their input and expertise
Author contributions
Conceptualization: T.vL., M.P.C., S.W., Z.T., O.K., I.M., P.G., K.I., Se.G., St.G., S.A., M.U. and M.vdM. Management T.vL., S.A., M.vdM. Writing – original draft: T.vL and M.vdM. Writing – review & editing: T.vL., M.P.C., S.W., Z.T., O.K., I.M., P.G., K.I., Se.G., St.G., S.A., M.U. and M.vdM. All authors contributed to discussion on content, active participation in the workshops and helped in revising and making substantial contributions to the manuscript, and also read an approved the final manuscript.
Financial statement
No funding.
Open access funding provided by Radboud University Medical Center.
Competing interests
None.
Ethical standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional guidelines and with the Helsinki Declaration of 1975, as revised in 2008.

 Open access
Open access