


Introduction
Spirituality remains ontologically exclusively undefined. Large individual variety in comprehension and experience of spirituality, the relational nature, and sensitivity to time and cultural differences has been claimed for that (Saarelainen et al. Reference Saarelainen, Vähäkangas and Anttonen2020; Nissen et al. Reference Nissen, Viftrup and Hvidt2021; Dorenbaum- Fastlicht et al. Reference Dorenbaum- Fastlicht, Castañeda and Guevara-López2025), which makes an exclusive definition of spiritual care challenging, too. The WHO considers, however, spiritual care as an inseparable part of palliative care which supports patients in reconnecting with their beliefs, values, and practices that give them meaning and strength. In practice, spiritual care often involves interventions facilitating listening to patients’ fears, hopes, and concerns, while fostering opportunities to find meaning and purpose in illness (Büssing Reference Büssing2021; WHO 2025).
In this context, spirituality is understood broadly and is not limited to religious affiliation. While religion refers to institutionalized beliefs and practices, spirituality encompasses how individuals relate to questions of meaning, purpose, connection, and coherence in life, including but not restricted to religious frameworks (Selman et al. Reference Selman, Harding and Beynon2007; Büssing et al. Reference Büssing, Zhai and Peng2013b; Wierstra et al. Reference Wierstra, Liefbroer and Post2023). Accordingly, spiritual needs may be present regardless of whether individuals identify as religious, spiritual, both, or neither (Nolan et al. Reference Nolan, Saltmarsh and Leget2011).
Furthermore, spiritual care may include presence, awareness, respect, empathy, compassion, and commitment (Edwards et al. Reference Edwards, Pang and Shiu2010; Walker and Waterworth Reference Walker and Waterworth2017; Morland et al. Reference Morland, McSherry and Rykkje2022) expressed through communication and sustained support (Vivat Reference Vivat2008; Minton et al. Reference Minton, Isaacson and Varilek2018; Moudatsou et al. Reference Moudatsou, Stavropoulou and Philalithis2020).
Spiritual needs can be considered as multidimensional concerns through which individuals seek meaning, purpose, connection, coherence, and inner peace (Bradford Reference Bradford2023; Wei et al. Reference Wei, Zhang and Zh2025). They include existential questions about identity, suffering, hope, and values, as well as relationships; for some individuals, religious beliefs and practices are also part of these needs (Büssing et al. Reference Büssing, Kloke and Gerundt2025). Spiritual needs may also be related to being recognized as a unique person, seeking forgiveness, or expressing love (Hermann Reference Hermann2006; Lunder et al. Reference Lunder, Furlan and Simonic2011; Bermejo Higuera et al. Reference Bermejo Higuera, Lozano González and Villacieros Durbán2013). Unlike physical, psychological, or social needs, spiritual needs address the worldview through which people interpret life, illness, and relationships (Büssing et al. 2021).
Spiritual needs often emerge in everyday interactions between patients and healthcare professionals (Cobb et al. Reference Cobb, Dowrick and Lloyd-Williams2012; Best et al. Reference Best, Butow and Olver2015). There is also a considerable amount of overlapping between spiritual and social needs (Lormans et al. Reference Lormans, de Graaf and van de Geer2021). As an example, meaningfulness in daily life: the home care personnel, outdoor activities and green spaces greatly influenced on the meaningfulness of life in a recent study examining elderly Finnish frail patients cared at home (Hemberg et al. Reference Hemberg, Näsman and Nyqvist2022).
Addressing patients´ spiritual needs may relieve distress, foster resilience, enhance the quality of life at the end of life (Balboni et al. Reference Balboni, Vanderwerker and Block2007; Puchalski et al. Reference Puchalski, Ferrell and Virani2009; Phelps et al. Reference Phelps, Lauderdale and Alcorn2012; Sinclair et al. Reference Sinclair, McConnell and Raffin Bouchal2015), and promote holistic care (Baldacchino Reference Baldacchino2015). Even the families of the patients facing life-threatening illness can experience consolidation when their closest ones´ spiritual needs are met in the care (Gijsberts Reference Gijsberts2022).
By contrast, unfulfilled spiritual needs are associated with distress and depression, hopelessness, loneliness, guiltiness (Schultz et al. Reference Schultz, Meged-Book and Mashiach2017; Ordons et al. Reference Ordons, Sinuff and Stelfox2018), reduced physical well-being (Hui et al. Reference Hui, de la Cruz and Thorney2011; Caldeira et al. Reference Caldeira, Carvalho and Vieira2013) and diminished quality of life (Winkelman et al. Reference Winkelman, Lauderdale and Balboni2011) and satisfaction with care (Riklikienė et al. Reference Riklikienė, Tomkevičiūtė and Spirgienė2020).
Although clinical studies and systematic reviews have suggested many successful interventions for improving spiritual care (Hvidt et al. Reference Hvidt, Hansen and Ammentorp2017; Pérez-Eizaguirre and Vergara-Moragues Reference Pérez-Eizaguirre and Vergara-Moragues2021; Warth et al. Reference Warth, Koehler and Brehmen2021; Huda et al. Reference Huda, Banda and Liu2023; Valero-Cantero et al. Reference Valero-Cantero, Vázquez-Sánchez and Casals-Sánchez2024; Brungardt et al. Reference Brungardt, Wibben A and Shanbhag2024; Nassehi et al. Reference Nassehi, Saake and Breitsameter2024), unfortunately spiritual needs are rarely addressed in clinical practice (Gijsberts et al. Reference Gijsberts, Liefbroer and Otten2019; Varner-Perez et al. Reference Varner-Perez, Comer and Fitchett2024). Barriers for health-care professionals to recognizing spiritual needs include different concepts of spirituality, absence of spiritual care guidelines; shortage of time; and insufficient training and education on spiritual issues, shame of approaching spirituality and lacking spiritual or religious literacy (Rushton Reference Rushton2014; Hvidt et al. Reference Hvidt, Hansen and Ammentorp2017; Dellenborg and Enstedt Reference Dellenborg and Enstedt2023; Laranjeira et al. Reference Laranjeira, Dixe and Querido2023; Costeira et al. Reference Costeira, Querido and Ventura2024).
In the Nordic countries spiritual issues have been traditionally considered very individual matters, which seldom are discussed in care settings and remain poorly anchored in public health care (Viftrup et al. Reference Viftrup, Nissen and Søndergaard2021). As an example, retrospective studies from Norway and Sweden have observed very few mentions about spiritual needs and care in nursing reports in palliative care (Gunhardsson et al. Reference Gunhardsson, Svensson and Berterö2008; Hynnekleiv et al. Reference Hynnekleiv, Giske and Heggdal2024). Yet a recent large population-based questionnaire survey including 104,137 Danish adults observed that over 80% of responders had experienced spiritual needs (Stripp et al. Reference Stripp, Wehberg and Büssing2023).
Contemporary qualitative research has provided insight for detecting patients´ spirituality and spiritual issues nonverbally in behavioral patterns and care facilities (Toivonen et al. Reference Toivonen, Charalambous and Suhonen2018; Penman Reference Penman2021; Voetmann et al. Reference Voetmann, Hvidt and Viftrup2022). Health-care professionals´ communication with patients about the spirituality can importantly be facilitated with specific questionnaires such as the Spiritual Needs Questionnaire (SpNQ) (Büssing et al. Reference Büssing, Balzat and Heusser2010) and the Spiritual Needs Assessment for Patients (SNAP; Sharma Reference Sharma, Astrow and Texeira2012) developed for assessment of needs in palliative care. Their use requires naturally that patients are able to communicate verbally (Büssing et al. Reference Büssing, Zhai and Peng2013b; Moeini et al. Reference Moeini, Zamanian and Taheri-Kharameh2018; Zhao et al. Reference Zhao, Wang and Yao2019; Brandstötter et al. Reference Brandstötter, Büssing and Eham2025; Hagelin et al. Reference Hagelin, Holm and Axelsson2025). Also, these questionnaires must be culturally adapted.
Although SpNQ was recently validated in Danish (Stripp et al. Reference Stripp, Büssing and Wehberg2022), a nationally designed instrument for palliative care has not been developed in the Nordic context (Benzein and Berg Reference Benzein and Berg2004; Asgeirsdottir et al. Reference Asgeirsdottir, Sigurdardottir and Gunnarsdottir2017; Stripp et al. Reference Stripp, Wehberg and Büssing2023). Spirituality has been overall studied very little in Finnish palliative care, but the previous Finnish qualitative studies have detected insufficient spiritual care in palliative units. Spiritual issues are not met enough well and that spiritual care skills of the nurses are not sufficient in palliative care (Lammi et al. Reference Lammi, Kosunen and Kellokumpu-Lehtinen2001; Selman et al. Reference Selman, Brighton and Sinclair2018; Toivonen et al. Reference Toivonen, Charalambous and Suhonen2018). Yet the importance of spirituality and the relationship of higher spiritual well-being and general quality of life and psychological well-being has been documented also among Finnish patients (Norberg et al. Reference Norberg, Lundman and Gustafson2015; Saarelainen et al. Reference Saarelainen, Vähäkangas and Anttonen2020; Goyarrola et al. Reference Goyarrola, Lamminmäki and Sipola2024). Clearly, there is a need for a culturally grounded tool for palliative care professionals to better identify and address patients’ spiritual needs, thereby strengthening the provision of truly holistic care.
Methods
Aim
The study aimed to develop a novel instrument for assessing the spiritual needs of palliative care patients. The finalized questionnaire was created in Finnish, with an official English translation to support broader applicability and cross-cultural use.
Study design for elaboration and validation
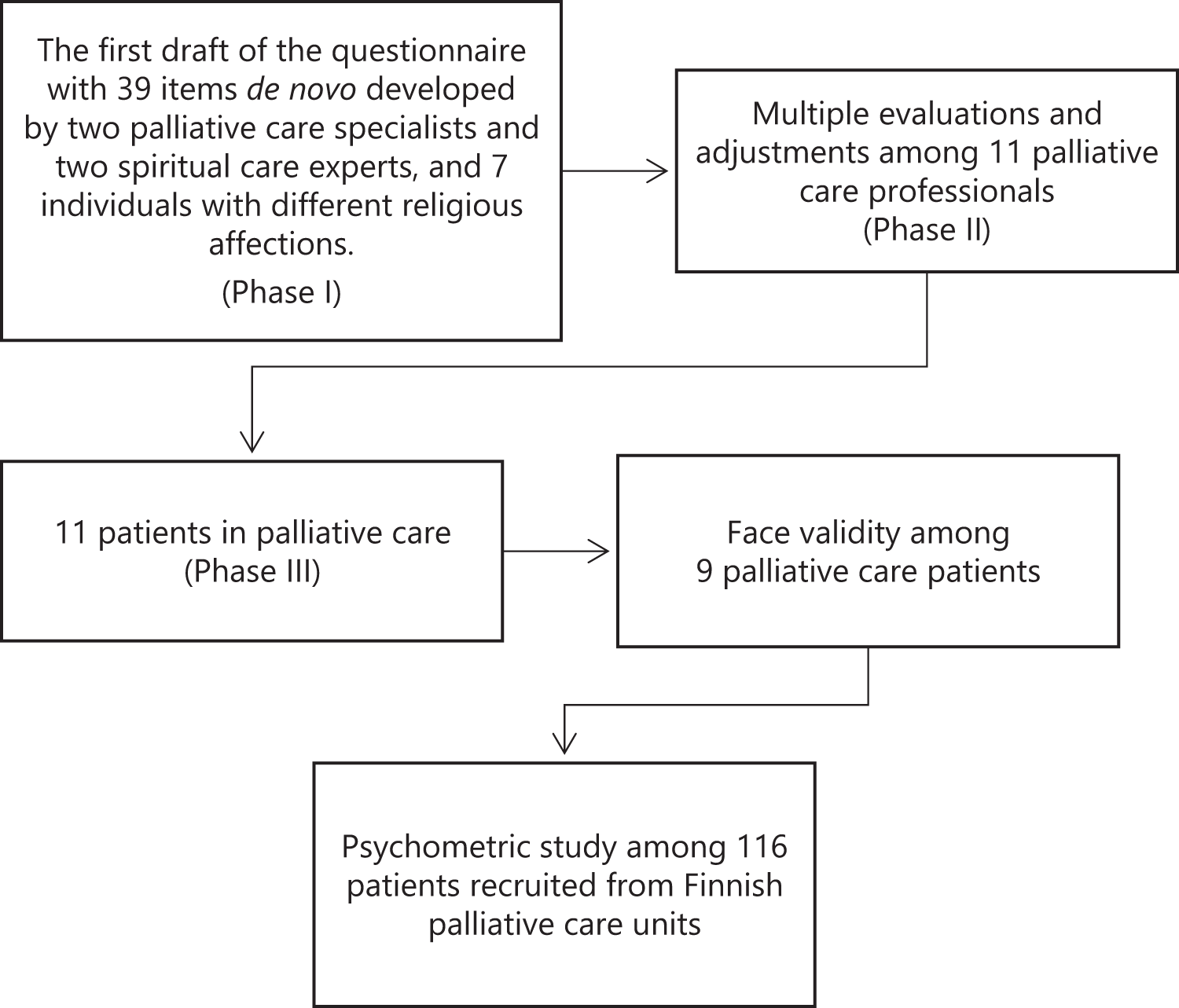
The questionnaire was developed, pre-tested, and validated using a prospective study design. Development began in 2020 and proceeded in three phases (Fig. 1). Throughout the process, the core research expert team (RG, AL, SS, RP) the expert team held monthly online meetings to refine the questionnaire. Thus, the role of the expert research team was vital during the entire development process.
Flow chart of the developmental process of the Finnish questionnaire of spiritual needs. → = “leading to”.

Questionnaire development
Phase 1
An initial pool of 39 items representing spiritual needs was developed by the research main group of two palliative care physicians and two spiritual care experts, on the basis of previous international studies (Bussing 2010; Sharma Reference Sharma, Astrow and Texeira2012), a recent Finnish qualitative study (Saarelainen et al. Reference Saarelainen, Vähäkangas and Anttonen2020) and their long-time experience in discussions with palliative care patients. Items were grouped into psychological (n = 14), existential/spiritual (n = 17), and religious (n = 8) domains. After refinement with input from 3 additional medical professionals, the questionnaire was revised to 36 items, evenly divided into psychological, existential, and religious needs (12 items in each). The structure, designed to assess both met and unfulfilled needs, was reviewed by representatives of 6 religious traditions in Finland and 1 non-affiliated individual (n = 7). Using a 0–5 rating scale, participants evaluated each need’s importance and could mark indisputable items. A cut-off score of 21 (≥60% of maximum 35 points) determined item acceptance. Participants were also asked to select their prioritized items.
Phase 2
The revised questionnaire was evaluated by 11 health-care professionals experienced in palliative or long-term care, who assessed its content and structure using the same Likert-type scale as in the first phase. Content validity was measured with the Content Validity Index (CVI), calculated as the proportion of essential ratings (Yusoff Reference Yusoff2019). Items with a CVI of 0.6–0.8 were reconsidered after discussion, while those below 0.6 were excluded. Participants could also suggest new items and provide qualitative feedback on clarity, wording, and response format. Based on this review, the Finnish version was revised and expanded to 27 items.
Phase 3
The questionnaire was pilot tested with 11 patients through individual pre- and post-completion interviews. Interviews explored clarity, comprehensibility, and sensitivity, asking whether any text was difficult, confusing, offensive, or distressing. Participants were also invited to suggest modifications to improve clarity and acceptability. Four team members re-evaluated the final questionnaire.
Validation of the final questionnaire
The final Spiritual Needs in Palliative Care (SNPC) questionnaire comprises 28 items on a 5-point verbal rating scale that assess both the importance (“How important is this need to you?”: 0 = I cannot say. 1 = Not at all important. 2 = Somewhat important. 3 = Fairly important. 4 = Very important), and fulfilment (“How is this need being met for you at the moment?”: 0 = I cannot say. 1 = Not at all. 2 = To some extent. 3 = Fairly well. 4 = Very well). Items were reorganized using an online pseudorandom number generator. For each need, participants rated its importance and the extent to which it was satisfied and were additionally asked to indicate any other needs.
Face validity
Face validity of the final SNPC questionnaire was assessed with 9 palliative care patients. Each of them received an explanation of the questionnaire beforehand, and was interviewed afterward to evaluate its comprehensibility, relevance, and acceptability.
Testing and the population
The final questionnaire was administered to 135 patients from palliative care units across Northern, Eastern, Western, and Southern Finland. Eligibility required adequate cognitive and linguistic ability in Finnish and diagnosis of serious, incurable life-limiting and progressive disease and receiving or being eligible for receiving palliative care. The eligibility refers to such patients who didn´t yet have a formal palliative care decision but were consulted for a palliative care specialist because of approaching palliative care at the time of filling of the questionnaire. Alongside spiritual needs, the instrument assessed demographics (age, gender), clinical status (diagnosis, palliative care status, past-week health), quality of life, functional capacity, and religious or spiritual affiliation.
Validity and internal consistency
Construct validity and internal consistency were studied using exploratory factor analysis (EFA; Mvududu and Sink Reference Mvududu and Sink2013).
For Convergent/divergent validity associations between SNPC scores, spiritual well-being, quality of life, and symptom burden were examined using the Spiritual Well-Being Questionnaire (EORTC-SWB32) (Vivat et al. Reference Vivat, Young and Winstanley2017), the Edmonton Symptom Assessment System (ESAS; Hui and Bruera Reference Hui and Bruera2017), and the WHO Performance Status Scale (Zubrod et al. Reference Zubrod, Schneiderman and Frei1960). The SWB32 is a 32-item, cross-culturally validated tool measuring five dimensions of spiritual well-being (self, others, something greater, existential concerns, God); its Finnish version has been recently validated (Goyarrola et al. Reference Goyarrola, Lipsanen and Saarelainen2023). The ESAS rates 13 common symptoms in advanced illness on a 0–10 scale, while quality of life and perceived health are assessed on a 7-point scale (1 = very poor, 7 = excellent). The WHO Performance Status Scale evaluates daily functioning from 0 (fully active) to 4 (bedbound) and is widely used in oncology and palliative care.
Data collection and statistical analysis
Data collection, anonymization, and digitalization took place in 2024–2025. Descriptive results are reported as means with standard deviations (SD) or percentages. Statistical analyses included Pearson’s correlation coefficients, independent samples t-tests. Correlation strength was defined as >0.5 strong, 0.3–0.5 moderate, 0.2–0.29 weak, and <0.2 negligible.
EFA was performed using principal axis factoring with varimax rotation to assess construct validity (Fabrigar et al. Reference Fabrigar, Wegener and MacCallum1999; Costello and Osborne Reference Costello and Osborne2005). Suitability for factor analysis was confirmed with the Kaiser–Meyer–Olkin (KMO) measure and Bartlett’s test of sphericity (Kaiser Reference Kaiser1974). Internal consistency was evaluated using Cronbach’s alpha.
Statistical significance was set at p < 0.05 (*) and p < 0.01 (**). All analyses, including factor analyses, were performed using IBM SPSS Statistics version 27.0.1 (Armonk, NY: IBM Corp.).
Results
Questionnaire development
Phase 1
In the preliminary 39-item questionnaire, 1 item (“to be complete and safe”) was removed, and 4 were consolidated into 2, yielding 36 items. The mean ranking (SD) was 27 (3.8).
The highest-ranked needs (31–35) emphasized both existential and relational dimensions, such as peace of mind, participation in care decisions in line with personal convictions, and sharing thoughts and experiences with loved ones. Needs related to explicitly religious practices, such as funeral rites or finding one’s relationship with God or something higher, were also among the most valued.
The lowest-ranked needs (10–21) included To dive into the beauty of nature, To keep in touch with other patients suffering from similar illnesses, To find meaning in the experience of illness, To know how to relax and manage stress, To overcome feelings of rejection, vulnerability, or isolation, and To create reconciliation of old disputes, hurts, or resentments with family or friends.
Some elements of these items were merged into others, and further consolidation reduced the questionnaire to 25 items, with revised wording. Figure 1 summarizes the development process.
Phase 2
The lowest-rated items were Finding meaning in my illness, Participating in care decisions according to my beliefs, Experiencing the beauty of nature, Planning my own funeral, and Being free from shame or guilt (ratings 2.93–4). Content CVI values ranged from 0.2 to 1, leading to the exclusion of Finding meaning in the disease (CVI = 0.2). In the second phase, the Finnish wording of all items was refined. Based on this feedback, two physicians and two humanities experts finalized a 27-item instrument. The questionnaire’s structure was rated entirely appropriate (CVI = 1); it includes two columns – one for the importance of each SN and another for its fulfilment – plus an open column for respondents to add other needs and descriptions.
Phase 3
One participant noted difficulty understanding items on freedom from shame, guilt, and meaning in life. Most needs were rated rather or very important (scores ≥3–4) in 88% of responses. Discussing death, freedom from shame, and freedom from guilt were rated moderately important (score = 2) in 10% of responses, while prayer and meeting a faith leader were considered unimportant by 2%. No new needs were suggested, and no items were reported as confusing, offensive, or distressing; no modifications were proposed. Based on expert team´s consensus, a new item – Finding comfort in the arts (e.g., films, books, music) – was added, yielding the final 28-item SNPC questionnaire.
Validity and reliability of the final questionnaire
The nine patients confirmed the face validity of the questionnaire, reporting that it was comprehensible, relevant, and acceptable, with no difficulties encountered.
Participants
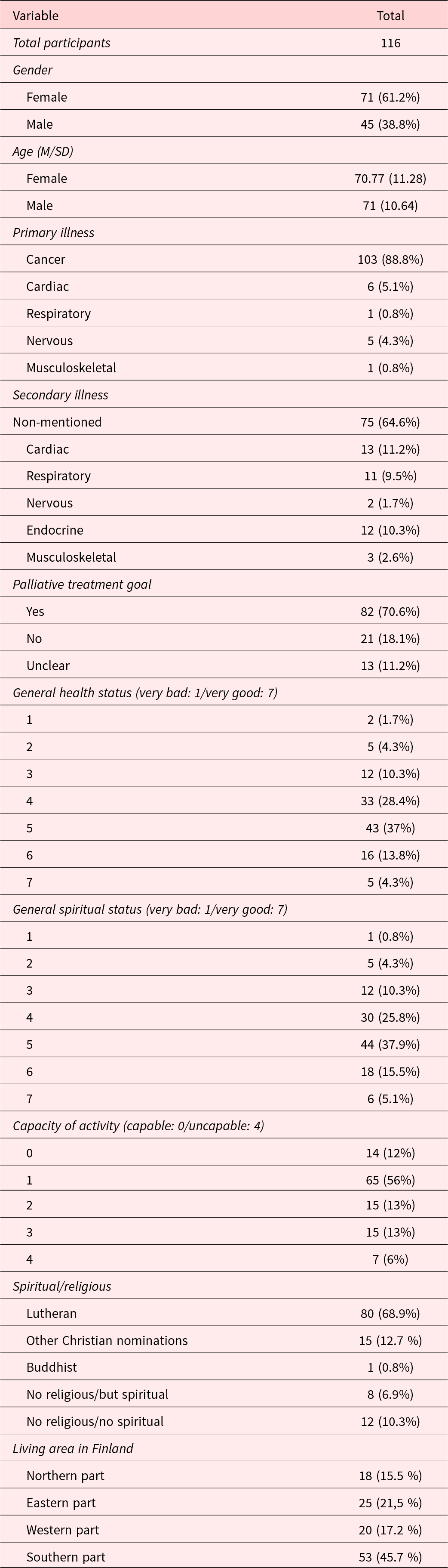
Table 1 summarizes Participants’ demographic and clinical characteristics. Most of the patients had cancer diagnosis (88.8%), and 70.6% had a palliative treatment plan. The quality of life and spiritual well-being were rated as moderate to good, and more than half reported moderate functional capacity.
The characteristics of the participants in the final validation part

M = mean, SD = standard deviation.
Content validity
A total of 116 patients completed the finalized SNPC questionnaire; nine questionnaires with substantial missing data were excluded. Figure 2 shows the perceived importance and fulfilment of SNs, ranked from highest to lowest importance. The most highly rated needs for importance were To feel safe in care (18), Peace of mind (5), and To participate in care decisions (15). The lowest-rated needs were Participation in religious ceremonies (24), Meeting with a priest or another member of my faith community (23), and The experience that suffering has a purpose/meaning (11). For fulfilment, the highest-rated needs were To feel safe in care (18) and To be accepted and loved as I am (1), while the lowest were Participation in religious ceremonies (24) and The experience that suffering has a purpose/meaning (11). Significant discrepancies between importance and fulfilment were observed for To be heard and understood (2), Peace of mind (5), Hope (12), and To experience the presence and support of my loved ones as death approaches (26).
Means of Likert scales of importance (“How important is this need to you?”: 0 = I cannot say. 1 = Not at all important. 2 = Somewhat important. 3 = Fairly important. 4 = Very important), and fulfilment (“How is this need being met for you at the moment?”: 0 = I cannot say. 1 = Not at all. 2 = To some extent. 3 = Fairly well. 4 = Very well).

Construct validity and internal consistency
Quantitative analysis (Table 2) provided descriptive statistics and response distributions for all items. Item-level analysis assessed ceiling and floor effects, defined as >95% of responses in two categories or <5% in any category. The number of factors was guided by statistical calculations and confirmatory graphs, with parallel analysis confirming the optimal latent constructs. They were named according to our primary theoretical conceptualization. Internal consistency was high across eight categories, with Cronbach’s alpha coefficients ranging from 0.627 to 0.927. The overall Cronbach’s alpha for the SNPC scale was 0.714.
Exploratory Factor Analysis SNPC “Importance of the Needs” (Range 1–4). Com: Communalities; Rot: Varimax rotated factor matrix. Extraction Method: Principal Axis Factoring. Rotation Method: Varimax with Kaiser Normalization Kaiser–Meyer–Olkin Measure of Sampling Adequacy: 0.779. Bartlett’s Test of Sphericity p-value: 0.000. Bartlett’s Test of Sphericity Approx. Chi-Square: 1703.082; df 378; Sig. < 0.001. Those 8 factors: % of Variance Cumulative 70.997%

Convergent/divergent validity of SNPC
Association of needs, SWB32, and ESAS are shown in Table 3. Existential, emotional, and religious needs were each significantly associated with their corresponding aspects of spiritual well-being in SWB32. In contrast, spiritual distress was linked to lower overall well-being. These associations remained independent of physical symptoms, including pain in ESAS, which showed no significant correlations with spiritual or emotional factors. We also found several significant associations between quality of life, WHO performance status, and SWB32 (Table 4). In contrast, correlations between the spiritual needs’ factors and overall symptom burden, as measured by ESAS were consistently low and non-significant across all dimensions.
Correlations SNPC factors/SWB32/ESAS (SN.Exi: Existential dimension of spiritual needs; SN.Emo: Emotional and esthetic dimension of SN; SN.Rel: Religious dimension of SN; SWB32. Exi: Existential items; SWB32. Emo: Emotional items; SWB32.Rel: Religious items; SWB32: item 32: Spiritual well-being; ESAS.WB: Over-all well-being)

** Correlation is significant at the 0.01 level (2-tailed).
* Correlation is significant at the 0.05 level (2-tailed).
Correlations between spiritual well-being (SWB32), general condition (ESAS), functional status (WHO), and patient´s appreciation on own health state and quality of life. SWB32: Spiritual Well-Being Questionnaire; ESAS: Edmonton Symptom Assessment System; WHO: Performance Status Scale

** Correlation is significant at the 0.01 level (2-tailed).
Discussion
This study describes the development and validation of the SNPC questionnaire, the first culturally adapted tool for assessing spiritual needs in Finnish palliative care patients. The SNPC demonstrated satisfactory content and construct validity, good internal consistency, and convergent validity with the EORTC-SWB32, as well as divergent validity with the ESAS. Strong correlations with the SWB32 indicate that the SNPC effectively captures key aspects of spiritual well-being. At the same time, the lack of association with symptom burden (ESAS) highlights that spiritual needs are distinct from physical and psychological symptoms.
Main findings
Exploratory factor analysis identified eight domains encompassing existential, emotional-aesthetic, religious, and distress-related needs, reflecting the multifaceted nature of spirituality in palliative care (Selman et al. Reference Selman, Brighton and Sinclair2018), including meaning, connection, inner peace, and reconciliation (Puchalski et al. Reference Puchalski, Ferrell and Virani2009; Vilalta et al. Reference Vilalta, Valls and Porta2014). Notably, “Emotional and Inner Peace” and “Freedom from Guilt and Shame” emerged as distinct factors, capturing key psychological and existential dimensions (McClain et al. Reference McClain, Rosenfeld and Breitbart2003; Cheng et al. Reference Cheng, Chen and Lin2023). Consistent with prior research, patients prioritized existential and emotional needs – such as hope, being heard, and the presence of loved ones – over formal religious practices (Balboni Reference Balboni, Sullivan and Amobi2013). Needs related to rituals, clergy visits, or finding meaning in suffering were rated lowest, highlighting that some patients experience spirituality outside formal religious frameworks (Steinhauser et al. Reference Steinhauser, Christakis and Clipp2000; Büssing et al. Reference Büssing, Janko and Baumann2013a).
Strong correlations but low mean scores in items reflecting traditional spirituality and religion (e.g., praying together, meeting a priest) suggested that while fulfilment is linked to the expression of these needs, they are not widely prioritized by all patients. Although less prominent overall, religious needs remained important for a substantial subgroup, highlighting the diversity of spiritual needs. These findings indicate a cultural shift in spiritual care toward relational, emotional, and meaning-centered domains in secularized societies such as Finland, consistent with international research (Büssing et al. Reference Büssing, Balzat and Heusser2010; Nygaard et al. Reference Nygaard, Austad and Sørensen2022).
Emotional distress is common among patients with advanced cancer, and prior studies often show moderate correlations between symptom burden and psychological distress (Ferrell et al. Reference Ferrell, Temel and Temin2017; Ascencio-Huertas et al. Reference Ascencio-Huertas, Allende-Pérez and Pastrana2021). In our study, however, ESAS scores did not correlate significantly with distress measures. Distress may arise from psychosocial or spiritual factors beyond physical symptoms, and symptom control can reveal underlying needs that require attention to improve quality of life (Ostwal et al. Reference Ostwal, Singh and Sanghavi2021). Evidence suggests that spiritual care may support coping with pain rather than reducing its intensity (Hindmarch et al. Reference Hindmarch, Dalrymple and Smith2022). Our findings highlight the distinct yet potentially overlapping nature of pain, spiritual distress, and emotional well-being. More comprehensive psychometric assessments and advanced analyses may reveal subtle or context-specific relationships that simple correlations cannot detect (Gonçalves et al. Reference Gonçalves, Gaudêncio and Paiva2024).
In this study, we observed a gap between the high importance patients place on existential and emotional needs and their lower reported fulfilment. This underscores a persistent challenge in palliative care: although spiritual needs are widely recognized as essential, they are often inadequately addressed in practice (Koper et al. Reference Koper, Pasman and Schweitzer2019; Jones et al. Reference Jones, Paal and Symons2021). Provision of spiritual care in medical settings is consistently limited, even though patients – particularly those at the end of life – express a strong desire for holistic recognition of these needs (Ripamonti et al. Reference Ripamonti, Giuntoli and Gonella2018).
In our study, unmet needs related to reconciliation, forgiveness, guilt, and existential suffering were particularly concerning, as they can exacerbate anxiety, depression, and hopelessness (Büssing Reference Büssing2021). Addressing these sources of spiritual distress is essential, and health-care professionals should be able to recognize both religious and non-religious forms of spirituality and respond flexibly to individual concerns (Batzler et al. Reference Batzler, Stricker and Bakus2024). Some clinicians also reported discomfort or lack of confidence in addressing existential or religious issues, sometimes leaving patients to manage these concerns alone (Prieto-Crespo et al. Reference Prieto-Crespo, Arevalo-Buitrago and Olivares-Luque2024). This is not an exception (Taylor Reference Taylor2021). Barriers included staff shortages, inadequate training (O’Brien et al. Reference O’Brien, Kinloch and Groves2019), and the perception that spirituality is too personal or falls beyond of the scope of professional responsibility (Vivat et al. Reference Vivat, Lodwick and Garcia-Baquero Merino2023). There is a clear need for professional skills and training to identify and address patients’ spiritual needs effectively (Batstone et al. Reference Batstone, Bailey and Hallett2020; Büssing et al. Reference Büssing, Kloke and Gerundt2025).
Significant gender differences were observed in existential and religious factors, with females scoring higher than males (existential: M = 61.08 vs. 46.80; religious: M = 62.55 vs. 46.79), indicating greater concern in these domains among women. No significant differences were found for emotional factors (females: M = 58.28; males: M = 49.77) or spiritual distress (females: M = 52.72; males: M = 57.20). These findings are consistent with previous reports that women more frequently express spiritual and existential concerns (Hermann Reference Hermann2007) and highlight the importance of individualized approaches considering demographic and cultural factors in spiritual care (Steinhauser et al. Reference Steinhauser, Fitchett and Handzo2017).
Strengths and limitations
This study has several strengths, including rigorous psychometric development, multicenter recruitment, and the involvement of both patients and professionals in validation and thorough psychometric analysis. The SNPC demonstrated strong internal consistency across most subscales and robust construct validity.
To our knowledge, it is the first validated tool for assessing spiritual needs in Finnish palliative care. These findings support the SNPC’s utility as a clinical and research instrument, addressing a previously noted barrier to culturally appropriate spiritual care in Finland and beyond. A major strength of the SNPC is its ability to adapt to cultural contexts. Unlike existing instruments such as the Spiritual Needs Questionnaire (SpNQ) (Büssing Reference Büssing2021), the SNAP (Sharma et al. Reference Sharma, Astrow and Texeira2012), and the Spiritual Concerns Checklist (SCC) (Michael et al. Reference Michael, Bobevski and Georgousopoulou2023), the SNPC was explicitly developed for the Finnish palliative context. Evidence from other cultural adaptations – e.g., SNAP in Chinese populations (Astrow et al. Reference Astrow, Sharma and Huang2012) and SpNQ in Chinese (Büssing et al. Reference Büssing, Zhai and Peng2013b) and Brazilian populations (Valente et al. Reference Valente, Cavalcanti and Büssing2018) – demonstrates that conceptualizations of spirituality vary widely across cultures, highlighting the importance of context-specific tools (Chen et al. Reference Chen, Lin and Yan2018). However, it would be interesting to find out, how our new questionnaire would fit in another culture.
Our questionnaire has rather similar number of items as the most of the previous English ones (Galek et al. Reference Galek, Flannelly and Vane2005; Büssing et al. Reference Büssing, Balzat and Heusser2010, Vilalta et al. Reference Vilalta, Valls and Porta2014). A unique difference is that we have focused both on the importance and fulfilment of the needs.
We believe that the new Finnish questionnaire could serve as a screening tool, as a discussion aid for those palliative care professionals who do not feel comfortable with spiritual issues, as a research instrument and as a bench-marking tool in palliative care.
A strength of the current study is that this new tool complements well with our Finnish translation of the EORTC-SWB32 (Goyarrola et al. Reference Goyarrola, Lipsanen and Saarelainen2023), which lacks detailed inquiry of spiritual needs but rather assesses the spiritual wellbeing of a patient.
Several limitations should be noted. Our questionnaire was tested mostly among primarily older cancer patients with Finnish Lutheran background, which may limit its use for patients with other diagnoses, cultures, or spiritual affiliations. Furthermore, as researchers with variable but mainly Christian backgrounds, we acknowledge that our professional experiences and personal beliefs may influence how we interpret data. The team engaged in regular discussions and reflexions to critically examine the interpretations. Divergent viewpoints within the team were discussed and integrated to minimize individual bias. Some subscales, such as Artistic and Quiet Comfort, showed lower internal consistency, indicating a need for refinement. Further qualitative studies on lived religion show, religiosity and spirituality are inherently situational, embodied, relational, and contextual; therefore, the operationalization of the scale may have captured only a partial representation of the lived realities of SNPC(McGuire Reference McGuire2008; Ammerman Reference Ammerman2014).
We did not formally assess the education levels of the responders, but in the preliminary assessments all participants had a professional education and the patients in the validation part represented well general well-educated Finnish population. No signs of difficulties in understanding the wordings were observed. The cross-sectional design precludes assessment of how spiritual needs change over time. Future longitudinal studies should evaluate the SNPC’s sensitivity to change and its predictive value for patient outcomes. We acknowledge as a limitation, that patients with cognitive decline, severe deterioration or fragility may not be able to respond to the whole questionnaire or even any part of it. Even in the care such patients, the questionnaire putatively might help palliative care staff or used only partly.
Implications for practice and research
Clinically, these findings highlight the ethical and practical imperative to integrate spiritual assessment into routine palliative care. Addressing spiritual needs can enhance patient satisfaction and has been associated with improved emotional functioning, coping, and quality of life at the end of life. We believe that the new questionnaire could be used both in the clinics and studies of palliative care. We think that this questionnaire would be particularly useful to help the palliative care staff to acknowledge spiritual issues in clinical practice those palliative care professionals, who express difficulties regarding existential, spiritual and religious issues. The SPNC could be used both as a written document by the patient or a nurse or a physician as an aid for the professionals during the discussions with the patients. The questionnaire could also serve as a bench-marking tool for palliative care, too.
Future research should validate the SNPC in more diverse populations (e.g., non-cancer patients, younger individuals, and different cultural or religious groups), conduct longitudinal studies to track changes in needs over the illness trajectory, and explore implementation strategies to integrate the SNPC into routine care while evaluating its impact on patient well-being, care satisfaction, and health system outcomes. We also think that further studies should be carried using qualitative methodology about spiritual and existential issues among younger patients in palliative care. This might widen the conceptualization and understanding the true spirituality from more narrow view using predefined items only.
Conclusion
The SNPC is a valid and culturally sensitive instrument that captures the multifaceted spiritual needs of Finnish palliative care patients. By bridging the gap between patient-reported needs and clinical practice, it offers a practical tool for advancing holistic, patient-centered care. Future research should evaluate its longitudinal impact on outcomes and explore its integration into professional training and health-care systems.
Supplementary material
The supplementary material for this article can be found at https://doi.org/10.1017/S1478951526102168.
Acknowledgments
Minna Hökkä (Oulu), Leena Surakka (Joensuu), Florence Schmitt (Turku), Taina Toivanen (Helsinki), Tiina Tiirikainen (Mikkeli), Elina Vogel (Lahti), and Anu Usvasalo (Rovaniemi) assisted with distributing the questionnaires.
Author contributions
RG, AL, SMS, and RP conceived and designed the research. RG had complete access to the study data. SMS, AL, and RP facilitated the translation process. RG, AL, and RP assisted with research permits and questionnaire distribution. RG conducted Statistical analysis. RG and RP drafted the manuscript. AL and SMS commented and edited manuscript. ER, KR, SM, KTK, and MH have asked for the permission in their respective hospitals and units and shared the questionnaires. All authors interpreted the data, critically revised the manuscript for important intellectual content, and approved the final version for submission.
Funding
This research received no specific grant from any funding agency, commercial or not-for-profit sectors.
Competing interests
The authors declare that they have no conflicts of interest.
Ethical approval
Ethical approval was granted by the Helsinki University Ethics committee. All participants in the content validity phase were adults with sufficient cognitive and linguistic abilities, and they gave the informed consent to participate to the study.







 Open access
Open access