



Significant outcomes
-
• The IFN-γ/NGF ratio achieved an excellent Area Under the Curve (AUC) of 0.858 for distinguishing DD patients from healthy controls, with high sensitivity (82.20%) and specificity (77.50%). Its diagnostic efficacy significantly outperformed the use of IFN-γ or NGF alone.
-
• The results confirm a significant immune-neuroendocrine disturbance in DD patients, characterised by downregulated IFN-γ and upregulated NGF levels, providing crucial new insights into the disorder’s biology.
Limitations
-
• The case-control design cannot determine whether the observed biomarker alterations are a cause or a consequence of depressive disorder. Additionally, the one-week medication washout period may not fully eliminate residual pharmacological effects on biomarker levels; future studies in drug-naïve populations are warranted.
Introduction
Depressive disorder (DD) is one of the most prevalent mental health conditions globally, affecting over 280 million people and contributing significantly to the global burden of disease (Marx et al., Reference Marx, Penninx, Solmi, Furukawa, Firth, Carvalho and Berk2023). Characterised by persistent sadness, anhedonia, cognitive impairments, and functional disability, DD is not only a leading cause of years lived with disability (YLDs) but also a major contributor to premature mortality through suicide and comorbid medical illnesses (Cui et al., Reference Cui, Li, Wang, Wu, Liu, Yu, Wang, Tang, Xia and Li2024). Despite the widespread use of standardised diagnostic criteria such as the DSM-5 and structured clinical interviews, diagnosis remains largely reliant on subjective assessments of mood and behaviour, which can be inconsistent, prone to bias, and limited in predictive value (Khan et al., Reference Khan, Yahya, Kamel and Faye2021; Marx et al., Reference Marx, Penninx, Solmi, Furukawa, Firth, Carvalho and Berk2023; Spytska, Reference Spytska2024).
A critical clinical gap lies in the absence of objective, reliable, and reproducible biological markers for the diagnosis and stratification of depression. This lack of biomarkers impairs early detection, delays effective intervention, and hinders efforts to personalise treatment strategies (Malik et al., Reference Malik, Singh, Arora, Dangol and Goyal2021; Winter et al., Reference Winter, Blanke, Leenings, Ernsting, Fisch, Sarink, Barkhau, Emden, Thiel, Flinkenflügel, Winter, Goltermann, Meinert, Dohm, Repple, Gruber, Leehr, Opel, Grotegerd, Redlich, Nitsch, Bauer, Heindel, Gross, Risse, Andlauer, Forstner, Nöthen, Rietschel, Hofmann, Pfarr, Teutenberg, Usemann, Thomas-Odenthal, Wroblewski, Brosch, Stein, Jansen, Jamalabadi, Alexander, Straube, Nenadić, Kircher, Dannlowski and Hahn2024). Patients often experience prolonged periods of untreated or inadequately treated illness, which is associated with poorer long-term outcomes, greater risk of relapse, and increased healthcare costs (Kuchimova, Reference Kuchimova2021). Moreover, existing diagnostic tools offer limited ability to differentiate depression from other neuropsychiatric or somatic conditions with overlapping symptoms, such as anxiety disorders, chronic fatigue, or thyroid dysfunction (Dubovsky et al., Reference Dubovsky, Ghosh, Serotte and Cranwell2021).
Emerging research has highlighted the role of immune and neurotrophic dysregulation in the aetiology of depression. Proinflammatory cytokines such as interferon-gamma (IFN-γ) have been shown to disrupt neurotransmitter metabolism, neuroendocrine function, and neuroplasticity, contributing to the onset and persistence of depressive symptoms (Lai et al., Reference Lai, Ho, Kow, Liang, Tham, Ho and Lee2023). Conversely, neurotrophic factors such as nerve growth factor (NGF) play a vital role in maintaining neuronal health, and their deficiency has been linked to neurodegenerative changes observed in depression (Jaiswal et al., Reference Jaiswal, Shreekantiah and Goyal2023; Salsabil et al., Reference Salsabil, Shahriar, Islam, Bhuiyan, Qusar and Islam2023). However, these findings are often reported in isolation and have not been adequately translated into diagnostic frameworks.
Importantly, there is an urgent need to integrate immune and neurotrophic markers into a composite diagnostic model. The IFN-γ/NGF ratio may serve as a promising index that captures the balance between systemic inflammation and neuroprotective capacity. Additionally, other serum indicators such as thyroid peroxidase antibody (TPOAb) (Yang et al., Reference Yang, Qu, Jiang, Lang and Zhang2023) and glial fibrillary acidic protein (GFAP) (Michel et al., Reference Michel, Fiebich, Kuzior, Meixensberger, Berger, Maier, Nickel, Runge, Denzel, Pankratz, Schiele, Domschke, van Elst and Endres2021), markers of autoimmune and glial dysfunction respectively, may provide further insight into the heterogeneity of depressive pathology.
This study was undertaken to address the pressing need for objective biomarkers in the diagnosis of depressive disorders. By comparing serum IFN-γ, NGF, TPOAb, and GFAP levels in patients with depressive disorders and matched healthy controls, and evaluating their diagnostic performance – individually and in combination – this work aims to establish a foundation for biologically informed clinical tools. Such tools have the potential to improve early detection, reduce diagnostic uncertainty, and ultimately enhance treatment outcomes for individuals affected by depression.
Methods
Study design and participant recruitment
This case-control study aimed to investigate immunological and neurotrophic biomarkers in patients with DD compared to healthy individuals. In this study, all patients with depression had experienced depressive symptoms for at least two weeks. The exclusion criteria were as follows: a history of alcohol or illegal drug abuse or substance dependence within the past 6 months, kidney disease or inflammatory disease, heart disease, and acute/chronic infection. Since antidepressants and antipsychotics can affect the levels of various substances in the body, all participants were required to discontinue the use of these medications for at least one week prior to the test. This study involved DD patients and sex- and age-matched healthy controls. Compliance with the washout requirement was confirmed through participant self-report and review of medical records where available.
Prior to the initiation of the trial, each participant was evaluated by a qualified psychiatrist. The screening procedures included psychiatric interviews; standardised diagnostic consultations based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5); assessment of depression severity using the Hamilton Depression Rating Scale (HAM-D); evaluation of past mental health issues; and collection of sociodemographic information via pre-designed questionnaires.
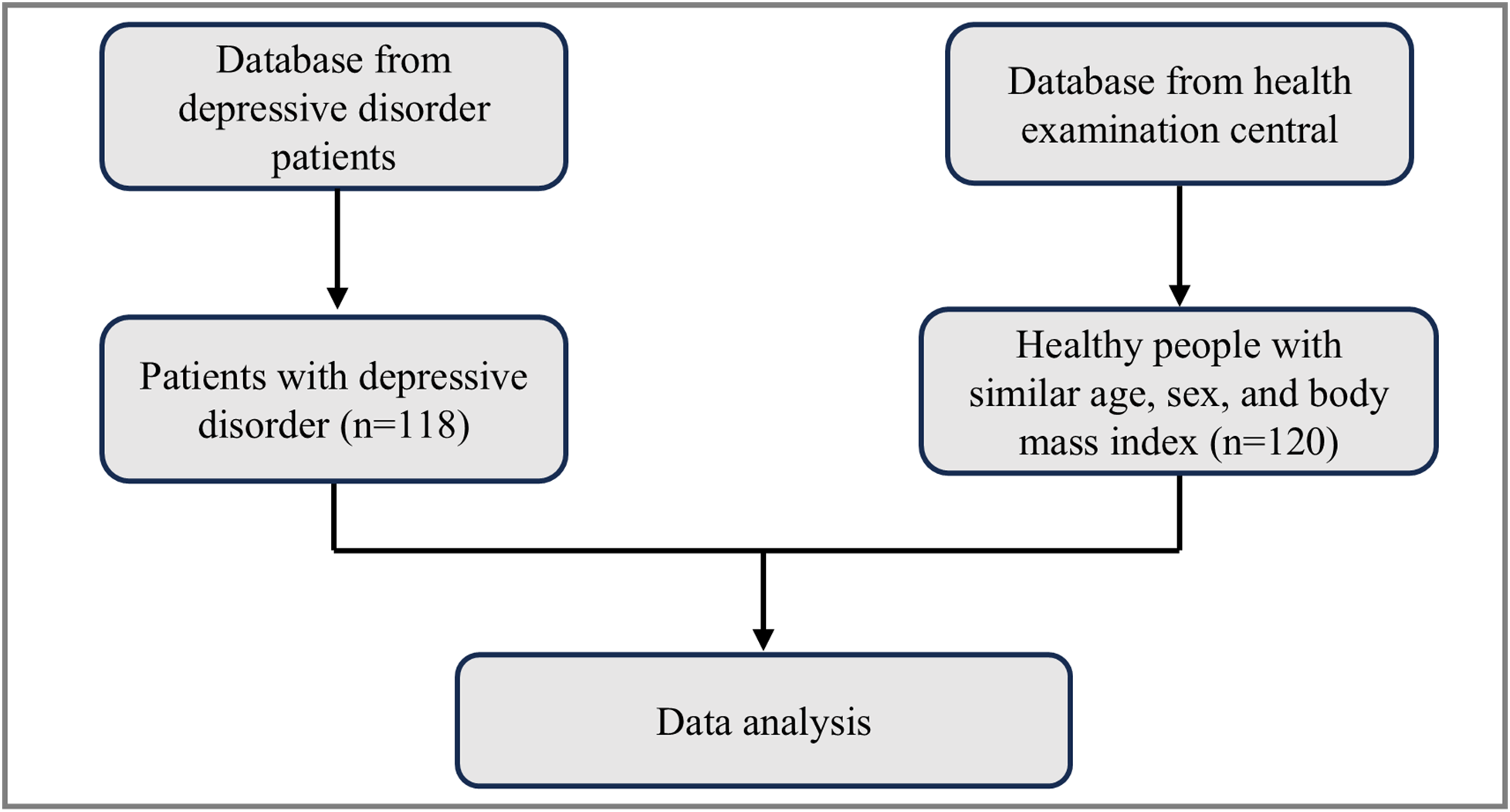
Participants were recruited from two independent sources: individuals with clinically diagnosed depressive disorders were identified through a psychiatric outpatient clinic database, while healthy controls were selected from the health examination centre of the same institution. The flow of participant inclusion is illustrated in Figure 1.
Flow chart of the study participants.

Inclusion criteria for the DD group included: (1) diagnosis of major depressive disorder in accordance with DSM-5 criteria, (2) age between 18 and 60 years, and (3) no major physical or neurological illness. Healthy controls were matched for age and sex, with no history of psychiatric disorders.
The study was approved by Qingdao Mental Health Center (#2023-V82-03). This study was conducted in accordance with the Declaration of Helsinki. We provided each participant with a detailed explanation of the study’s purpose and objectives and obtained their written informed consent prior to their participation. If a participant was found to have an intellectual disability, consent was obtained from their legal guardian. Furthermore, the detailed information of all patients was de-identified to ensure that they could not be identified in any manner.
Sociodemographic and clinical data collection
Sociodemographic data such as age, sex, marital status, education level, smoking status, economic status, area of residence, and BMI were collected through structured interviews and medical records. Clinical history regarding previous or familial depressive disorders was also documented. Depression severity was assessed using the DSM-5 criteria and Hamilton Depression Rating Scale (HAM-D) (Renemane & Vrublevska, Reference Renemane and Vrublevska2021).
Blood sample collection and biomarker analysis
Venous blood samples were collected from all participants between 8:00 and 10:00 AM after an overnight fast. Serum was separated and stored at −80°C until analysis. Concentrations of interferon-gamma (IFN-γ), NGF, TPOAb, and GFAP were quantified using enzyme-linked immunosorbent assay (ELISA) kits following the manufacturer’s instructions.
Statistical analysis
Data were processed and examined using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard error of the mean (SEM), and categorical variables as frequencies and percentages. Comparisons between groups were performed using the Student’s t-test for continuous variables and the chi-square test for categorical variables. ROC curve analysis was conducted to evaluate the diagnostic performance of IFN-γ, NGF, and their ratio. A p-value of less than 0.05 was considered statistically significant.
Results
Participant recruitment and demographics
A total of 238 participants were included in the final analysis, with 118 individuals diagnosed with DD and 120 healthy controls. Figure 1 depicts the recruitment flowchart detailing inclusion from respective databases.
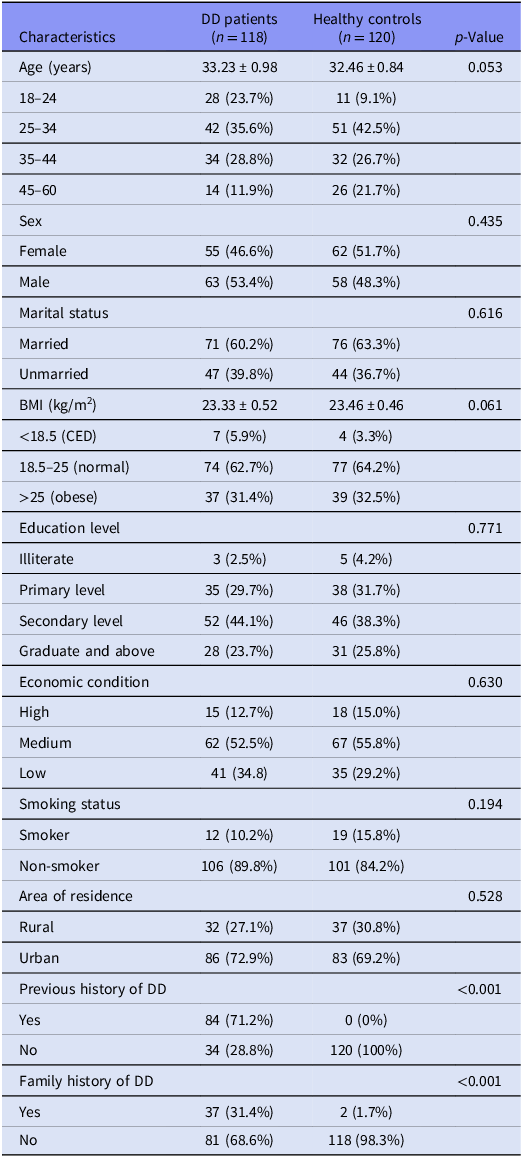
As shown in Table 1, there were no statistically significant differences in age (33.23 ± 0.98 vs. 32.46 ± 0.84 years, p = 0.053), sex distribution (p = 0.435), marital status (p = 0.616), BMI (p = 0.061), education level (p = 0.771), economic condition (p = 0.630), smoking status (p = 0.194), or area of residence (p = 0.528) between the two groups. However, prior personal history of depression (71.2% vs. 0%, p < 0.001) and family history of depressive disorders (31.4% vs. 1.7%, p < 0.001) were significantly more common in the DD group.
Sociodemographic characteristics of the study population

Data are presented as mean ± SD or n (%). Values of p < 0.05 were considered statistically significant. BMI, body mass index; CED, chronic energy deficiency; DD, depressive disorder.
Altered immune and neurotrophic biomarkers in depressive disorder
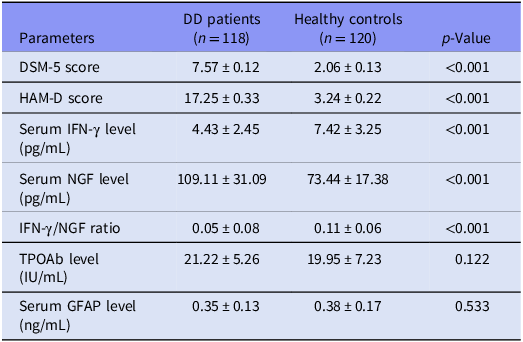
Table 2 summarises the clinical features and laboratory parameters for both groups. DD patients exhibited significantly elevated scores on both the DSM-5 (7.57 ± 0.12 vs. 2.06 ± 0.13, p < 0.001) and HAM-D (17.25 ± 0.33 vs. 3.24 ± 0.22, p < 0.001) scales compared to controls.
Clinical features and laboratory findings of study participants
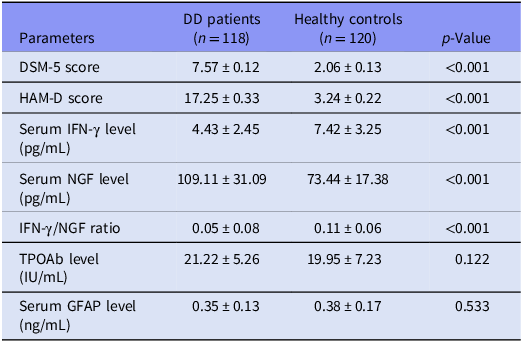
Data are presented as mean ± SD. Values of p < 0.05 were considered statistically significant.
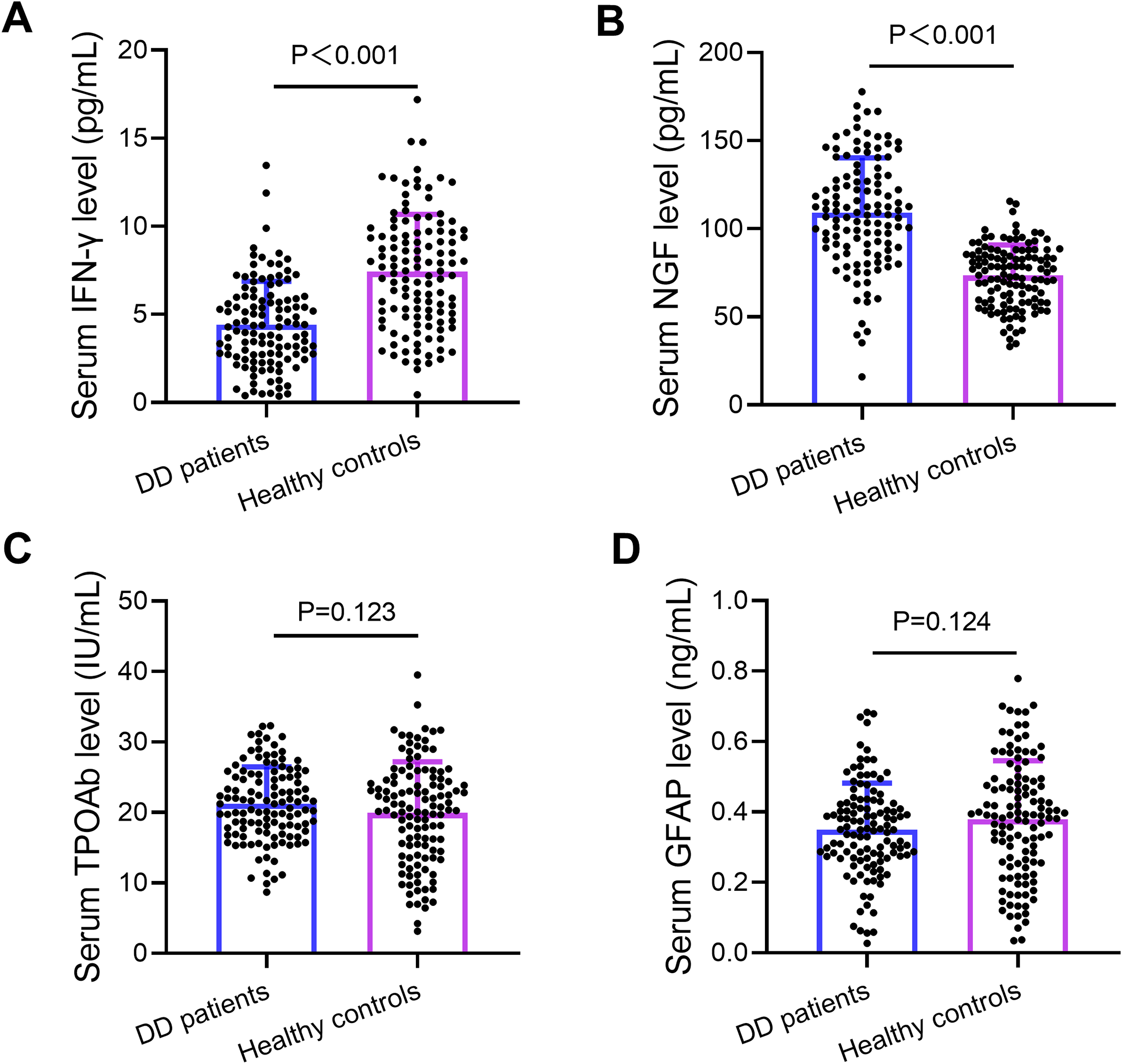
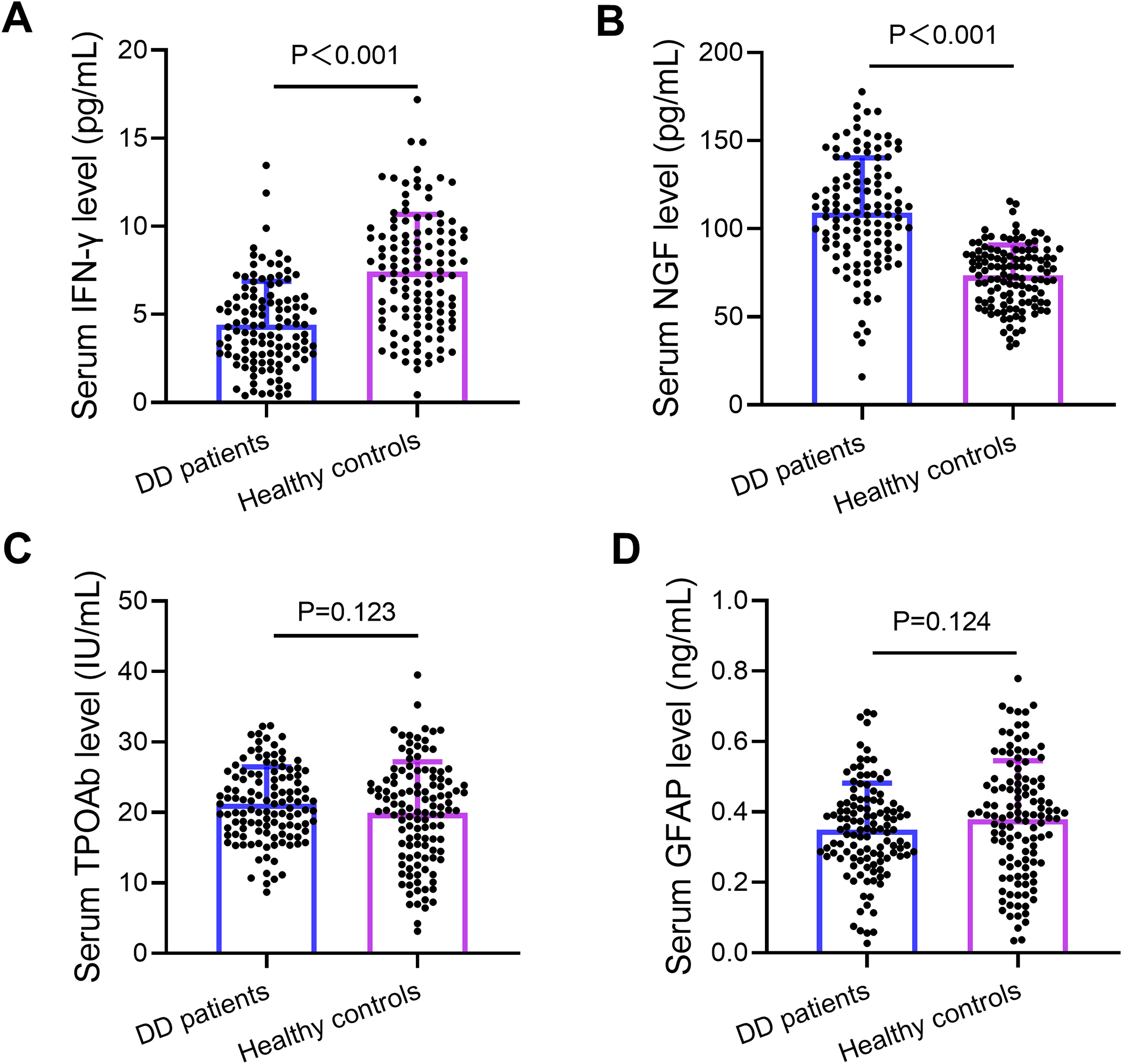
Notably, IFN-γ levels were significantly decreased in DD patients (4.43 ± 2.45 pg/mL) versus healthy individuals (7.42 ± 3.52 pg/mL, p < 0.001), whereas NGF levels were significantly elevated (109.11 ± 31.09 pg/mL vs. 73.44 ± 17.38 pg/mL, p < 0.001). Consequently, the IFN-γ/NGF ratio was significantly lower in the DD group (0.05 ± 0.08) than in controls (0.11 ± 0.06, p < 0.001). There were no significant group differences in TPOAb or GFAP levels (both p > 0.1). Figure 2A–2D illustrates these biomarker variations graphically.
Variations of serum IFN-γ (A), NGF (B), TPOAb (C) and GFAP (D) among the study population.
IFN-γ/NGF ratio demonstrates high diagnostic accuracy for depressive disorder
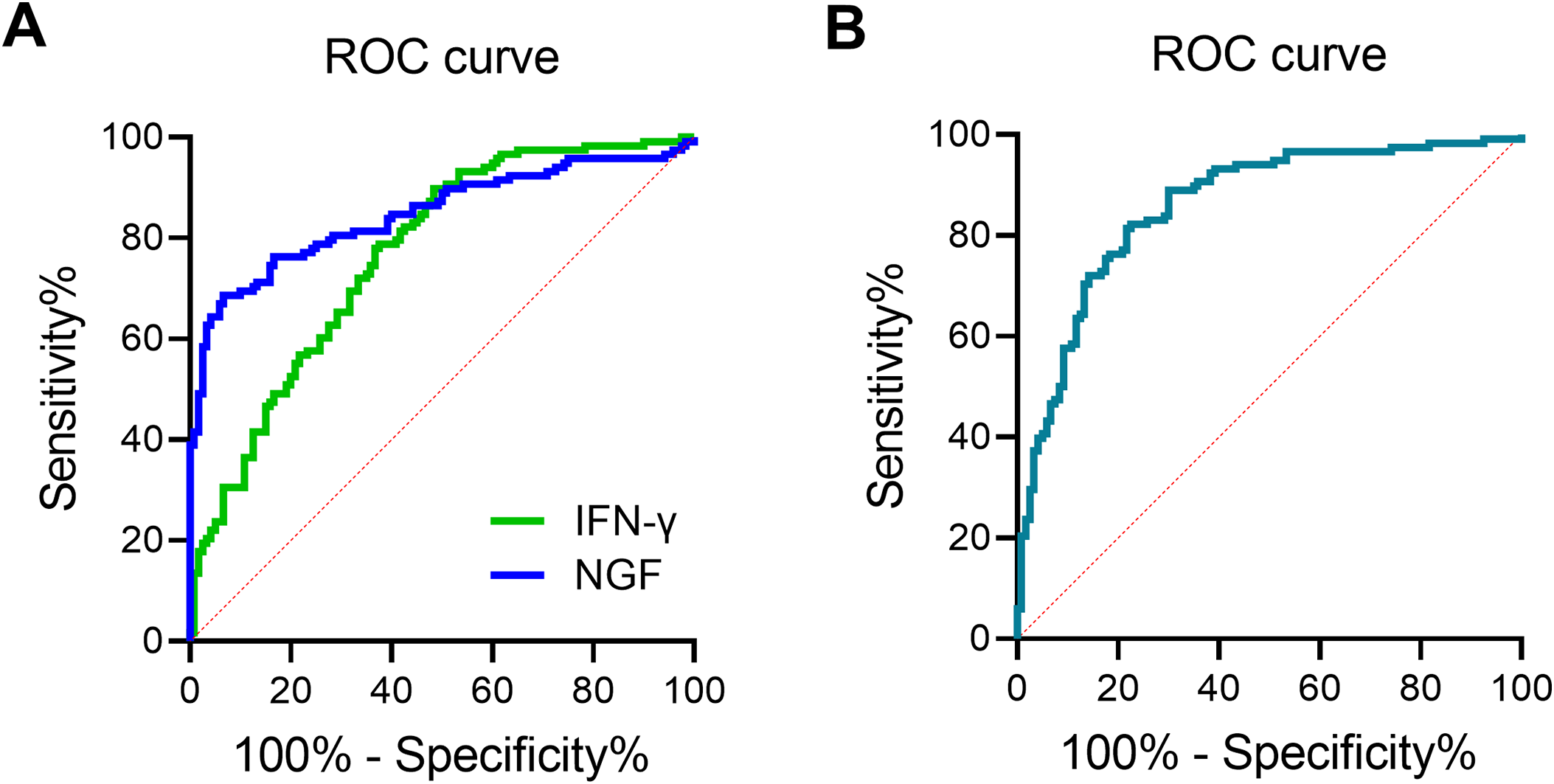
Receiver operating characteristic (ROC) analysis was performed to evaluate the diagnostic performance of individual and combined biomarkers (Figure 3). IFN-γ alone yielded an AUC of 0.766 (95% CI: 0.707–0.818, p < 0.001) with a sensitivity of 89.83% and specificity of 51.67% at a cut-off value of 7.27 pg/mL (Figure 3A). NGF also demonstrated strong diagnostic performance (AUC = 0.848, 95% CI: 0.796–0.891, p < 0.001) with a sensitivity of 68.64% and specificity of 93.33% at a cut-off of 95.56 pg/mL (Figure 3A).
ROC curves for the healthy controls group and the DD patient group and the combined auxiliary diagnostic models. (A) ROC curves for IFN-γ and NGF. (B) ROC curve for IFN-γ/NGF ratio. The model was established based on the IFN-γ/NGF ratio of each sample and whether the subject was a DD patient.

In contrast, the IFN-γ/NGF ratio demonstrated the highest diagnostic performance, with an AUC of 0.858 (95% CI: 0.808–0.900, p < 0.001), sensitivity of 82.20%, and specificity of 77.50% at a cut-off of 0.06 (Figure 3B). These findings underscore the ratio’s potential as a robust auxiliary marker for the clinical assessment of depressive disorder.
Discussion
This study provides novel evidence that immune and neurotrophic biomarkers – particularly the IFN-γ/NGF ratio – may serve as valuable adjuncts to the clinical diagnosis of DD. Compared to healthy controls, individuals with DD exhibited significantly lower levels of IFN-γ and elevated levels of NGF, resulting in a markedly reduced IFN-γ/NGF ratio. Among all tested parameters, this ratio demonstrated the highest diagnostic accuracy, with strong sensitivity and specificity, underscoring its potential clinical relevance.
Our findings both align with and expand upon prior work examining cytokine and neurotrophic factor alterations in depression (Gadad et al., Reference Gadad, Vargas-Medrano, Ramos, Najera, Fagan, Forero and Thompson2021; Horita et al., Reference Horita, da Silva, Ferrari, Vieira, Moreira, de Oliveira and Reis2021). The observed reduction in IFN-γ may reflect a state of immune suppression often seen in chronic or recurrent depressive states. This phenomenon may be linked to chronic stress, dysregulation of the HPA axis, and impaired cellular immune responses (Lei et al., Reference Lei, Phang, Lee, Kow, Tham, Ho and Lee2025). The elevated NGF levels observed in the DD group may represent a compensatory neurotrophic response to neuronal stress or damage. Our findings are consistent with models suggesting that neurotrophic systems may upregulate in response to prolonged pathological changes as a form of endogenous neuroprotection (Valencia-Sanchez et al., Reference Valencia-Sanchez, Pittock, Mead-Harvey, Dubey, Flanagan, Lopez-Chiriboga, Trenerry, Zalewski, Zekeridou and McKeon2021). This finding appears to contrast with the widely reported inflammatory hypothesis of depression, which typically associates IFN-γ with elevated pro-inflammatory activity; however, several explanations may account for this discrepancy. First, illness stage appears critical: while acute or early-stage depression may involve heightened immune activation, chronic or recurrent illness may lead to immune exhaustion and paradoxical cytokine suppression. Second, although a one-week washout was implemented, residual immunomodulatory effects of prior pharmacotherapy cannot be entirely excluded, as certain antidepressants can durably alter cytokine profiles beyond the washout window. Third, the findings may reflect a Th1-to-Th2 immune shift, in which declining Th1-driven IFN-γ production accompanies a relative rise in Th2-mediated responses – a pattern documented in specific subsets of depressed patients in prior research. Notably, similar IFN-γ reductions have been reported in patients with recurrent or treatment-resistant depression, suggesting that the present results may represent a biologically distinct depression phenotype rather than a contradiction of the inflammatory model. It is important to acknowledge, however, that NGF findings in the depression literature are heterogeneous: while the present study and certain prior reports observe elevated NGF, other studies have found decreased or unchanged levels in depressed populations (Jaiswal et al., Reference Jaiswal, Shreekantiah and Goyal2023; Salsabil et al., Reference Salsabil, Shahriar, Islam, Bhuiyan, Qusar and Islam2023). These divergent findings may reflect differences in illness stage, depression subtype, medication history, and the degree or chronicity of neuronal stress. For instance, early or mild depression may be associated with NGF suppression, whereas chronic or severe illness may trigger compensatory neurotrophic upregulation. Depression subtypes – such as melancholic or treatment-resistant forms – may also display distinct neurotrophic profiles. Future studies with clearly stratified patient subgroups will be necessary to resolve these inconsistencies and better characterise the directionality of NGF changes across the depressive spectrum.
One important contribution of our study is the evaluation of the IFN-γ/NGF ratio as a combined marker, rather than interpreting these biomarkers independently. This integrative and novel approach captures the dynamic interaction between inflammatory and neurotrophic pathways, providing a more comprehensive biological signal that is more diagnostically robust than either marker alone. The strong discriminative performance of this ratio suggests it could be a reliable auxiliary diagnostic tool in clinical psychiatry.
In contrast, serum levels of TPOAb and GFAP did not significantly differ between groups. These findings suggest that autoimmune thyroid dysfunction and astrocytic activation may not be central to the pathophysiology of depression in this specific cohort, which has recently been an active research area (Sawicka-Gutaj et al., Reference Sawicka-Gutaj, Zawalna, Gut and Ruchała2022; Lekurwale et al., Reference Lekurwale, Acharya, Shukla and Kumar2023). It is also possible that these markers are only altered in specific subtypes or severities of depression not represented here.
The clinical implications of these results are significant. The integration of objective, blood-based biomarkers into routine psychiatric assessment could reduce reliance on subjective symptom reporting, decrease diagnostic uncertainty, and improve early intervention. Particularly in primary care or resource-limited settings, such biomarkers could serve as accessible and efficient tools for identifying at-risk individuals and guiding personalised treatment decisions.
Nonetheless, several limitations should be noted. The cross-sectional nature of the study precludes causal interpretation and limits the ability to assess biomarker changes over time. The relatively homogeneous demographic characteristics of the sample may also restrict generalisability. Furthermore, factors such as medication use, dietary habits, sleep quality, and comorbid physical conditions were not exhaustively controlled, and these may influence biomarker levels. Moreover, the one-week medication washout period, while intended to reduce pharmacological confounding, may not fully eliminate residual biological effects of prior antidepressant or antipsychotic treatment, particularly for agents with extended half-lives or sustained immunomodulatory properties. Future investigations employing drug-naïve patient cohorts would be valuable to confirm these biomarker findings in a fully unmedicated state.
Future research should employ longitudinal study designs to evaluate biomarker dynamics across different phases of illness and treatment. Investigations that include larger, more diverse populations and incorporate additional biological and imaging markers could further enhance the diagnostic specificity and mechanistic understanding of depression. Exploring the utility of the IFN-γ/NGF ratio in differentiating depression from other neuropsychiatric or inflammatory conditions may also extend its clinical utility.
Conclusion
In summary, this study highlights the IFN-γ/NGF ratio as a promising biomarker with high diagnostic performance in depressive disorder. By reflecting the interplay between immune and neurotrophic processes, this ratio offers a biologically meaningful tool that could facilitate earlier and more precise identification of individuals with depression, ultimately improving clinical outcomes and supporting personalised mental health care.
Data availability statement
The data used to support the findings of this study are available from the corresponding author upon request.
Author contributions
Data collection: Lei Yi, Chuanqin Liu, Wei Lin and Ni Duan; design of the study: Ni Duan; statistical analysis: Lei Yi; analysis and interpretation of the data: Lei Yi, Chuanqin Liu, Wei Lin and Ni Duan; drafting the manuscript: Lei Yi, Chuanqin Liu, Wei Lin and Ni Duan; critical revision of the manuscript: Ni Duan.
Funding statement
None.
Competing interests
The authors declare they have no conflict of interest regarding this research study.
Ethical standards
The study was approved by Qingdao Mental Health Center (#2023-V82-03). Informed written consent was obtained from the participants. The study was performed in strict accordance with the Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects.
Informed consent
All patients signed the informed consent.
Consent for publication
Not applicable.

 Open access
Open access